Community-Based
Reporting Template
2014-2015
TABLE OF CONTENTS
General Instructions ... 1
Introduction ... 1
Before You Begin... ... 1
Other Types of Program Reporting ... 2
Part 1 – Identification Information ... 3
Part 2 – Common Information ... 4
1. Programs and Services Delivered ... 4
2. Health Team ... 5
Part 3 – Program Component Reporting ... 6
A. Healthy Child Development ... 10
B. Mental Wellness ... 19
C. Healthy Living ... 25
D. Communicable Disease Control and Management (CDCM) ... 30
E. Home and Community Care ... 37
General Instructions
IntroductionThis Community-based Reporting Template was designed to support the work of Health Funding Agreement recipients in meeting the reporting requirements of their Agreements. As you complete each section of this template, be sure to use the supporting
resource, Community-based Reporting: A Guide for BC First Nations Health Service
Providers. The Guide provides detailed instructions, definitions, examples of answers, and lists of acronyms to assist you in completing the Reporting Template.
For assistance, please contact us at [email protected]. Before You Begin...
• This template is for reporting on performance of health programs and services. This template is not for reporting financial and audit information. For information on financial and audit reporting requirements, refer to your Health Funding Agreement. • Collection and analysis of program performance information should be on-going to
support your program management and reviews, and in order to submit the completed Community-based Reporting Template by the due date specified in your Health Funding Agreement.
• Performance reporting using this Community-based Reporting Template is required for all types of funding models.
• For a multi-community Agreement, the recipient will complete a separate Community-based Reporting Template for each community under its Agreement.
• This template consists of three parts. You must complete all three parts: 1) Identification Information
2) Common Information, and 3) Program Component Reporting.
• When completing questions that require numbers as answers, be sure to enter “0” when the answer is none. Do not leave any answers blank. In cases where the response for all questions in a table is “0”, write “All entries are zero” once at the top of the table. • Your responses to certain questions will require more space than provided in the
template. Where necessary, use another sheet of paper. Be sure to label them with the question number and submit them as part of your completed template.
• Submit your completed template to the First Nations Health Authority by the due date stated in your Health Funding Agreement.
Other Types of Program Reporting
Programs that currently report to First Nations Health Authority using other tools,
processes and/or electronic systems such as the HCC e-SDRT and e-HRTT, and COHI dental database are required to continue to input into these processes and systems within the agreed upon time frames, in addition to answering the related questions in this template. The programs listed below are not reported through this template. If you deliver any of the following programs, refer to your Health Funding Agreement for the reporting
requirements.
• Mandatory reporting on Public Health • First Nations Health Benefits Program
• Indian Residential Schools Resolution Health Support Program • Environmental Health Research projects
• Aboriginal Health Human Resource Initiative
• National Native Alcohol and Drug Abuse Program - Residential Treatment • Youth Solvent Abuse Treatment Centre Program
• e-Health Infostructure
• Health Services Integration Fund, and • Health Facilities and Capital Program.
If you would like more information, please contact the First Nations Health Authority: [email protected].
Part 1 is mandatory. Provide the Health Funding Agreement number as indicated in your Health Funding Agreement. For items 4 and 5 below, include the contact name and
information and have the report authorized and signed prior to submitting the completed report to the First Nations Health Authority.
Health Funding Agreement Number ___________________________________________ Highest type of funding model in the Health Funding Agreement
__________________________________
Are the services delivered in the Agreement for multiple communities? Yes No If yes, for how many communities? ________
Note: A separate Community-based Reporting Template should be completed and submitted for each community.
1) Community name: _________________________________________________ 2) a) Organization/recipient name(s): ____________________________________
b) Health facility name: _____________________________________________ 3) Reporting period covered by this report: _______________________________ 4) Submitted by:
___________________________________ __________________________________ Contact Name (please print) Position ___________________________________ __________________________________
Signature Date (day/month/year) 5) Authorized by (recipient):
___________________________________ __________________________________ Name (please print) Position
___________________________________ __________________________________ Signature Date (day/month/year)
Part 2 is mandatory.
1. Programs and Services Delivered
Communities are required to complete all sections of this template that apply to all health programs and services they deliver. Refer to the FNHA Program Compendium for more details about the programs listed below, which you may be delivering under different names. In the table, indicate the programs and services provided in your community during the reporting year by putting a check mark (√) in the boxes for all that apply. See the Guide for a list of acronyms.
A. Healthy Child Development
Healthy Pregnancy and Early Infancy (Prenatal Nutrition, Maternal and Child Health, Fetal Alcohol Spectrum Disorder) Early Childhood Development (Aboriginal
Head Start on Reserve)
Oral Health (Children’s Oral Health Initiative)
B. Mental Wellness
Mental Health and Suicide Prevention (National Aboriginal Youth Suicide Prevention Strategy, Brighter Futures, Building Healthy Communities)
Substance Abuse Prevention (National Native Alcohol and Drug Abuse Program, Youth Solvent Abuse Program)
C. Healthy Living
Chronic Disease Prevention and Management (Aboriginal Diabetes Initiative)
Injury Prevention
D. Communicable Disease Control and Management
Vaccine-preventable Diseases and Immunization
Blood-borne Disease and Sexually Transmitted Infections
Respiratory Infections
Communicable Disease Emergencies
E. Home and Community Care F. Clinical and Client Care (to be completed only by communities with a nursing station or Health Centre with Treatment providing clinical and
treatment services 24 hours a day either 5 or 7 days per week)
Are the clinical and client care services provided by First Nations Health Authority (FNHA)?
Yes No
If No, please complete section F. If Yes, this section is to be completed by the First Nations Health Authority.
Part 2 – Common Information
2. Health Team
Indicate the number of Health Care Workers in your community for each category, full-time and part-time, at the end of the reporting year.
Category of Health Care Workers
Number of Full-Time Number of Part-Time and Visiting Total Number in Category Health Manager
Community-based, Band employed Registered Nurses including nurse
practitioners (NP), registered nurses (RN), and licensed practical nurses (LPN)
NP # NP# NP#
RN# RN# RN#
LPN# LPN# LPN#
First Nations Health Authority employed Registered Nurses including nurse
practitioners, registered nurses, and licensed practical nurses
NP# NP# NP#
RN# RN# RN#
LPN# LPN# LPN#
Other licensed or regulated health professionals
Community-based health workers (e.g., CHR, NNADAP, ADI, AHSOR, CPNP, MCH Home Visitors, FASD Community Coordinators and Mentors, HCC Personal Care Workers, Youth Worker, Mental Health Worker)
Administrative, janitorial staff and
housekeeping staff working in health facilities and for health programs
Totals
Do you have an arrangement with a medical officer of health or medical health officer to provide public health services to your community? Yes No
If Yes, who do they work for?
Province or Regional Health Authority/local health unit First Nations Health Authority
Part 3 – Program Component Reporting
Part 3 is mandatory.
In Part 3, complete the information for the program components that apply to the programs and services managed in your community under your Health Funding Agreement with the First Nations Health Authority, and as indicated in Part 2 of this reporting template.
Complete Question 1. only for workers in A. Healthy Child Development, B. Mental Wellness, and C. Healthy Living.
Question 1. Worker Information and Training: In the table below, for each employee contributing to work in Healthy Child Development (HCD), Mental Wellness (MW), or Healthy Living (HL), provide the job title, primary activity area of the employee, full time or part time, certification type, and licensing and training information as indicated. For Training, use a check mark (√) to indicate completion of the training.
Worker Information *Training completed during the reporting year
Job Title (list each individual separately, one per row)
Primary Activity Area (Use HCD, MW, or HL)
Fu
ll/
Pa
rt Ti
m
e (FT o
r P
T)
Certification or Accreditation Type – regulated or unregulated (Use only letter codes as provided in Table 1 below. Enter multiple codes where required.) Certified Training (Indicate completion with a check mark) Continuing Education Training (Indicate completion with a check mark) Short Course Training (Indicate completion with a check mark)*Certified Training: Educational program at least one academic year in length. *Continuing Education Training: Short-term courses that upgrade or maintain skills. *Short Course Training: Courses between 1 week and 3 months that are not recognized with classes in a certification program.
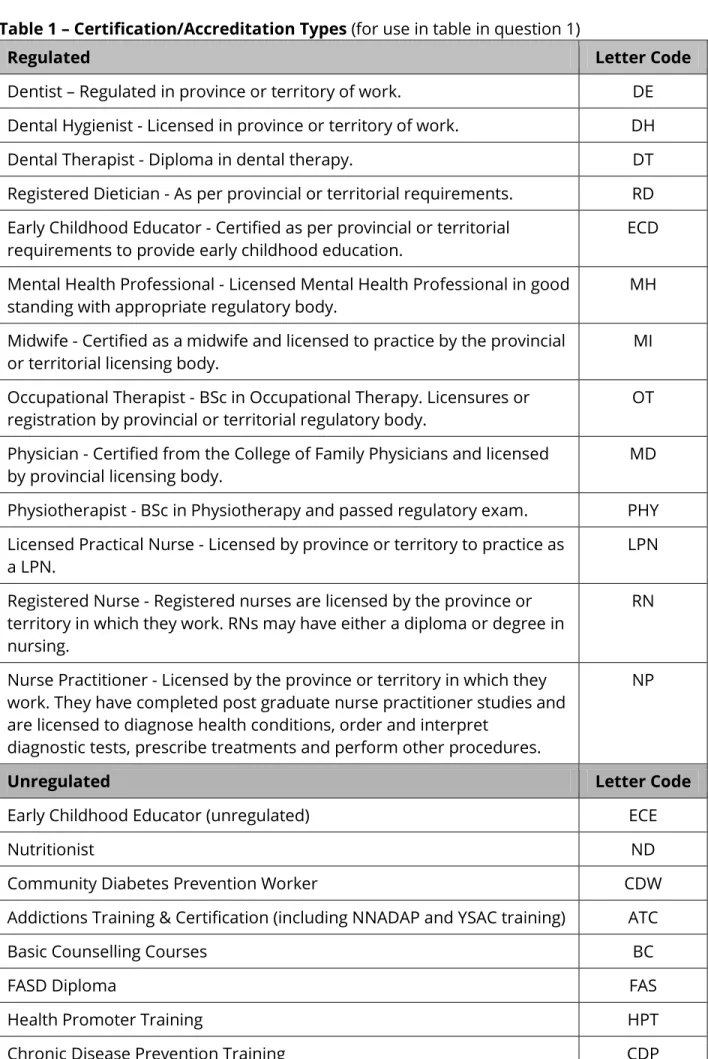
Table 1 – Certification/Accreditation Types (for use in table in question 1)
Regulated Letter Code
Dentist – Regulated in province or territory of work. DE Dental Hygienist - Licensed in province or territory of work. DH Dental Therapist - Diploma in dental therapy. DT Registered Dietician - As per provincial or territorial requirements. RD Early Childhood Educator - Certified as per provincial or territorial
requirements to provide early childhood education.
ECD Mental Health Professional - Licensed Mental Health Professional in good
standing with appropriate regulatory body. MH
Midwife - Certified as a midwife and licensed to practice by the provincial or territorial licensing body.
MI Occupational Therapist - BSc in Occupational Therapy. Licensures or
registration by provincial or territorial regulatory body. OT Physician - Certified from the College of Family Physicians and licensed
by provincial licensing body.
MD Physiotherapist - BSc in Physiotherapy and passed regulatory exam. PHY Licensed Practical Nurse - Licensed by province or territory to practice as
a LPN. LPN
Registered Nurse - Registered nurses are licensed by the province or territory in which they work. RNs may have either a diploma or degree in nursing.
RN
Nurse Practitioner - Licensed by the province or territory in which they work. They have completed post graduate nurse practitioner studies and are licensed to diagnose health conditions, order and interpret
diagnostic tests, prescribe treatments and perform other procedures.
NP
Unregulated Letter Code
Early Childhood Educator (unregulated) ECE
Nutritionist ND
Community Diabetes Prevention Worker CDW
Addictions Training & Certification (including NNADAP and YSAC training) ATC
Basic Counselling Courses BC
FASD Diploma FAS
Health Promoter Training HPT
Chronic Disease Prevention Training CDP
Regulated Letter Code
Basic Diabetes Education BD
Aboriginal Trauma Certificate Program ATP
Home Visitor Applied Certificate HVC
Children’s Oral Health Initiative Aide COH
A. Healthy Child Development
Question 2. Pre and Postnatal Nutrition Activities: Indicate with a check mark (√) the
pre and postnatal nutrition activities and services that were delivered in your community. If an activity you provide could fit under more than one category provided below, choose its ‘best fit’, and account for it only once.
Nutrition Screening, Education and Counselling Activity Offered Check (√ ) Nutrition or dietary screening
One-on-one nutrition counselling/education Group nutrition counselling/education Baby food making workshops/classes Grocery store tours
Maternal Nourishment Check (√ ) Food vouchers distributed
Community kitchens/community cooking classes
Food boxes or groceries distributed
Community gardens
Traditional food gathering/distribution/preparation
Breastfeeding Promotion, Education, and Support Check (√ ) Education workshops
One-on-one breastfeeding support Group breastfeeding support Peer support program
Supportive Elements that address specific needs of at-risk clients
(e.g., transportation, child care, etc.) Check (√ ) Yes
No
Question 3. Reach of Pre and Postnatal Nutrition Programming: Of the total number of women served by pre and postnatal nutrition programming during the reporting year, indicate the number of participants who first received services in their 1st trimester, 2nd trimester, or 3rd trimester, and the number of participants who first received services after giving birth (postnatal).
Enrolment Timeframe Number Pregnant women who first received services in their 1st trimester (0-12
weeks)
Pregnant women who first received services in their 2nd trimester (13-26 weeks)
Pregnant women who first received services in their 3rd trimester (27-40 weeks)
Women who first received services after they had given birth (with an infant or infants 0-12 months of age)
Question 4. Breastfeeding: For participants with infants six months or older, indicate the duration of breastfeeding rates for the time periods below. Time periods are consistent with the Pre and Post Natal Outcome Tracking Tool provided with the CBRT.
Breastfeeding Duration Number
Total number of participating mothers with babies who turned six
months during the reporting year
Mothers who breastfed for less than 3 months (less than 15 weeks) Mothers who breast fed for longer than 3 months and shorter than 6 months (15 weeks to 23 weeks)
Mothers who breast fed for 6 months (24 weeks to 27 weeks)
Mothers who breast fed for longer than 6 months (28 weeks or more) Mothers who did not initiate breastfeeding
Unknown whether breastfeeding was initiated
Question 5. Risk Factors: For all pregnancies concluding in the reporting year, indicate the number where the following risk factors were present among participants. If necessary, refer to the Pre- and Post Natal Outcome Tracking Tool provided with CBRT, or other
tracking tools for this information.
Risk Factors Number Total number of participants whose pregnancies concluded during the
reporting year
Maternal age less than 20 Maternal age 35 or higher
Smoking by mother during pregnancy
Drug or solvent use by mother during pregnancy Alcohol use by mother during pregnancy
Diabetes diagnosed before pregnancy
Diabetes diagnosed during pregnancy (gestational diabetes) Post partum mood disorders (previous diagnosis)
Question 6. Total Number of Births: Indicate the number of babies born to mothers who live in the community during the reporting year. This information may not be available from your program sources. You may have to use another source in your community to obtain this information. See Guide for details.
Total Births Number Total number of babies born to mothers who live in the community
Question 7. Birth Weight: Indicate the number of babies who were full term, pre-term, and unknown term for each of the birth weight categories provided in the table. Count only babies born to program participants during the reporting year. Refer to the Pre- and Post Natal Outcome Tracking Tool provided with the CBRT, or other tracking tools, for this information.
Birth Weight Category
Number Full
term Pre-term Unknown Term Less than 5lb 9oz (less than 2500g)
Between 5lb 9oz and 8lb 11oz (2500g – 4000g) More than 8lb 11oz (more than 4000g)
Birth weight unknown
Question 8. Solid Food Initiation: For infants who turned 6 months old during the
reporting year, indicate the numbers who initiated solid food in each of the time periods in the table below. Refer to the Pre- and Post Natal Outcome Tracking Tool provided with the CBRT, or other tracking tools, for this information.
Solid Food Initiation Number Solid food initiated before 6 months
Solid food initiated at 6 months Solid food initiated after 6 months Unknown when solid food was initiated
Question 9. Maternal and Child Health Screening and Assessment: Indicate with a
check mark (√) which types of screening and assessment services were delivered in the reporting year. If an activity you provide could fit under more than one category provided below, choose its ‘best fit’, and account for it only once.
Screening and Assessment for: Check (√) Risk factors for pregnant women and new mothers such as post
partum depression, chronic conditions such as Type 2 diabetes, gestational diabetes, and tobacco/alcohol/drug/solvent use
Risk factors for developmental milestones for infants and children Vision/hearing/dental screenings or assessments for referral
Question 10. Maternal and Child Health Home Visiting and Case Management Programming Reach: Indicate in the fields provided, the number of participants who received home visits and/or case management services. (‘participant’ is defined as the primary contact for services, including their family and dependants). See Guide for details.
Home Visits and Case Management Number Total Number who received home visits
Total Number who received case management
Question 11. First Home Visit: Of all the pregnant women and new mothers receiving home visits through maternal and child health programming during the reporting year, indicate the number who received their FIRST home visit in their 1st trimester, 2nd
trimester, or 3rd trimester, and the number of participants who first received services after giving birth (postnatal).
First Home Visits Number Pregnant women who received their first Maternal and Child Health
home visit in their 1st trimester
Pregnant women who received their first Maternal and Child Health home visit in their 2nd trimester
Pregnant women who received their first Maternal and Child Health home visit in their 3rd trimester
Women who received their first Maternal and Child Health home visit within 6 months of giving birth (postnatal)
Question 12. Fetal Alcohol Spectrum Disorder (FASD): Use a check mark (√) to indicate which services were delivered. Then provide the number of families receiving FASD
community coordination services or FASD case management services, and the total number of clients receiving FASD mentoring services. See Guide for details.
FASD Activities Activity Offered Check (√)
Number of Participants FASD Community capacity building activities (e.g.,
awareness and prevention activities, and development of action plans)
FASD Community coordination/FASD case management FASD Mentoring
Question 13. Aboriginal Head Start On Reserve (AHSOR): Provide information on AHSOR program delivery in your community by completing the table below and checking all that applies. See Guide for details.
13A) How many communities are served by your AHSOR program?
13B) Does your AHSOR program offer
Outreach/Home-visiting? Yes No
13C) Is your AHSOR site Centre-based? (if NO, please proceed to Question 14 below. If YES, please continue completing this table)
Yes No 13D) Is your AHSOR program licensed? Yes No 13E) How many full/half days per week does your
Centre-based AHSOR program operate?
# of Full days:
# of Half days: 13F) Is your AHSOR program co-located? Yes No 13G) If YES, is your AHSOR program co-located with a
school or daycare facility? Yes No
Question 14. AHSOR Activities: Indicate with a check mark (√) which activities were provided.
Activity Type Activity Offered Check (√ ) Teaching children their First Nation language(s) (e.g., reading a story,
teaching letters or numbers, etc.)
Traditional ceremonies and activities (e.g., smudging, gathering traditional foods, visits from Elders, etc.)
Early literacy skills (e.g., reading to children, singing songs, etc.) Fine and gross motor development activities (e.g., catching a ball, holding a pencil, etc.)
Providing healthy foods (snacks and/or lunches)
Healthy personal hygiene and dental habits (e.g., teeth brushing, hand washing, etc.)
Physical activity (e.g., outdoor play, games, dance, etc.)
Linkages (including referrals and collaborations) to professionals and community supports and providers (e.g., housing, education,
specialists, etc.)
Parent and family support activities (e.g., workshops for new mothers and young parents, support groups, etc.)
Visits from health professionals (e.g., nurses, dental hygienists, others) Safety education and awareness activities, (e.g., play ground safety, car seat technician training, car seat use, seat belt use, bike safety, etc.)
Question 15. Number of Children in AHSOR Programming: Indicate total participation in AHSOR programming by age and program delivery type (centre-based and/or
outreach/home visiting) and the number of children on a waiting list, if applicable. See Guide for details.
Age
Number of Participants by Program Delivery Type
Does the program keep a waiting list. Indicate Yes or No. If Yes, how many children are on the waiting list? Centre-Based Outreach/Home Visiting Number of children younger than 3 years old Number of children 3 to 6 years old Total
Question 16. AHSOR Children and Special Needs: For each program type, indicate the number of children in the AHSOR program who have been diagnosed, screened/assessed, or referred for special needs during the reporting year, as well as the number of children on a waiting list at the end of the reporting year. A single child may be counted in more than one category if it applies. See Guide for details.
Special Needs
Diagnosis, Screening/Assessment, Referrals, Wait List
Number of Children by Program Type
Centre-based Home Visiting Outreach/ Number of AHSOR children who have been diagnosed
with special needs
Number of AHSOR children screened/assessed for special needs
Number of AHSOR children referred to other community resources (e.g., nurses, doctors, specialists, etc.) for special needs support or diagnosis
Number of AHSOR children on a wait list for special needs diagnostic assessment
Question 17. Frequency of Parent/Family Participation: For centre-based AHSOR programs only, indicate the total number of adult parent and family participants involved and the frequency of their involvement (e.g., daily, weekly, monthly or special occasions). Count each person only once under the appropriate heading.
Daily Weekly Monthly/Special Occasions Total Number of
Parent/Family Participants
Question 18. Children’s Oral Health Initiative (COHI): All communities delivering COHI,
regardless of agreement type, are expected to continue to use the Dental Service Daily Record and Dental Screening Forms according to the frequency and terms outlined in their Health Funding Agreement program plan.
In addition, please answer the following question:
Indicate the total number of children living in the community by age group, and the number participating in COHI activities.
Age Total Number Living in the Community (If necessary, obtain data from a non-program source)
Number Participating in Children’s Oral Health
Activities Children less than 5
years
Children 5 to 7 years
Question 19. Healthy Child Development Service Linkages: Use a check mark (√) to
indicate where service linkages occurred between community health staff and external
organizations and agencies during the reporting year. Service linkages can be formal or
informal arrangements, collaborations, or processes with external individuals and organizations to facilitate the delivery of health services. See Guide for details and
examples. Type of Service/Service Linkage Regional Health Authority/ Health Service Zone Educational Organization Non-profit Organization Provincial Services Nutritionist/dietician Physical activity/recreation Specialist care Treatment/management Diagnostics/screening Drug/alcohol treatment Dental
Type of Service/Service Linkage Regional Health Authority/ Health Service Zone Educational Organization Non-profit Organization Provincial Services service supports Occupational Therapist or Speech and Language Pathologist
Question 20. Data Tracking Tools and Support: Use a check mark (√) to indicate your responses to the following questions (except in 20B).
20A) Do you use any First Nations Health Authority tracking tool(s) to track your work in Healthy Child Development activities?
Yes No If No, go to question 21 in the next section. If Yes, go to question 20B.
20B) Provide the name of the tracking tool(s) being used.
In questions 20C) to 20 E), rate your level of satisfaction with the tracking tool(s) by indicating your level of agreement with the following statements:
20C) “The tracking tool(s) is (are) useful in tracking work in Healthy Child Development.” (Mark your level of agreement with this statement in the appropriate box.)
Strongly disagree Disagree Neutral Agree Strongly agree 20D) “The tracking tool(s) has (have) aided in the
completion of the CBRT.” (Mark your level of agreement with this statement in the appropriate box.)
Strongly disagree Disagree Neutral Agree Strongly agree 20E) “The tracking tool(s) has (have) been useful across
activity areas.” (Mark your level of agreement with this statement in the appropriate box.)
Strongly disagree Disagree Neutral Agree Strongly agree
B. Mental Wellness
Question 21. Mental Wellness Activities: Indicate with a check mark (√) which activities and services were offered in your community. If an activity or service you provided could fit under more than one category below, choose the category that is its ‘best fit’, and account for it only once.
21A) Suicide Prevention Activities Activity Offered Check (√ ) Awareness activities (e.g., increasing knowledge of suicide rates and
contributing factors, addressing suicide myths and pre-conceptions, increasing communication about suicide, and decreasing stigma) Sport, recreation and other activities to engage youth
Traditional activities to engage youth (e.g., land-based activities, cultural practices, skill development)
Life skills activities for youth (e.g., leadership, relationships, problem solving, developing positive coping skills)
Training on signs and symptoms and responding to suicidal behaviour (e.g., ASIST, SafeTalk, Mental Health First Aid, train-the-trainer sessions, CISM)
Crisis intervention (e.g., mobilizing to prevent spread of suicide) 21B) Mental Wellness Promotion and Support: Wellness activities teach and promote ways to increase well being, focusing on positive choices for all, regardless of risk for mental health issues and addictions.
Activity Offered Check (√ ) Wellness activities promoting mental health (e.g., parenting skills,
self-care, managing stress, positive relationships, emotional and spiritual well being). Activities may include community celebrations and recreation activities, including physical and social activities.
21C) Substance Abuse, Addictions and Mental Health Activities Activity Offered Check (√ ) Presentations and workshops aimed at preventing substance abuse
Cultural events to support the prevention of addictions and substance abuse, as well as the awareness of mental health issues
Addictions recovery support groups
School-based programs to support awareness of substance abuse and addictions
21D) Crisis Intervention
Activity Offered Check (√ )
Mental health crisis intervention activities (other than those specific to youth suicide prevention)
Question 22. Suicide Interventions: For each type of suicide intervention in the table, indicate the number of interventions, clients, and clients where family was involved. The “total number of interventions” should be the number of events and not the number of individuals (e.g., multiple interventions might occur for a single individual). The “number of clients where the family was involved” should be understood as a sub-set of the total number of clients.
Suicide Interventions Total Number of Interventions Total Number of Clients
Number of Clients Where
Family was Involved in the
Intervention Interventions with youth at
risk for suicide (e.g., counselling, assessments) Interventions with individuals or those affected after an attempted suicide (e.g., support, counselling, treatment planning)
Interventions after a death by suicide with those affected
Question 23. Interventions for Substance Abuse, Addictions and Mental Health: For each type of intervention in the table below, indicate for each age group the number of clients who received interventions and the number where the family was involved. Use the number of clients, not the number of interventions. The number for “where the family was involved” should be understood as a sub-set of the number of clients.
Interventions for Substance Abuse, Addictions, and Mental Health
Number of clients Youths (under 18) Where family was involved in Intervention Adults (18 and over) Where family was involved in Intervention Screening and Basic Assessment (e.g.,
CAGE, MAST or DAST)
Brief Intervention (e.g., supportive discussions including personalized feedback, identification of supportive networks/resources, and goal setting on substance use behaviours)
Interventions for Substance Abuse, Addictions, and Mental Health
Number of clients Youths (under 18) Where family was involved in Intervention Adults (18 and over) Where family was involved in Intervention or referred) such as specialized
addiction or mental health assessment Direct Counselling (e.g., pre-treatment, day or evening programming or
aftercare)
Community-based Supports (e.g., support groups such as AA and NA, counselling, day or evening
programming). Note: Do not include NNADAP or NYSAP residential services. Cultural supports including community based Elders and traditional healers. Referral to Specialized Supports (e.g., psychiatric services, intensive
concurrent disorder treatment, or medically based withdrawal management)
Question 24. Referrals to Treatment Centres: For each client category in the table, indicate the number of clients who were referred to a treatment centre in the National Native Alcohol and Drug Abuse Program (NNADAP) or a treatment centre in the Youth Solvent Abuse Program (YSAP). Note: A client should be counted only once. A family should be counted only once and only in the category “Family referrals”, not as an individual referral in another category.
Client Category
Number of Clients referred to NNADAP Treatment Centre YSAP Treatment Centre Provincial Treatment Centre Other Treatment Centre Males under 12 years
Females under 12 years Males 12-17 years Females 12-17 years Males 18 years and over Females 18 years and over Family referrals
Question 25. Service Linkages for Mental Health and Addictions: Use a check mark (√)
to indicate where service linkages occurred between community health staff and external
organizations and agencies during the reporting year. Service linkages can be formal or
informal arrangements, collaborations, or processes with external individuals and
organizations to facilitate the delivery of health services. See Guide for details and
examples. Type of Service/ Service Linkage Regional Health Authority/ Health Service Zone Educational
Org’s Non-profit Org’s
Police (Band, RCMP, Local/ Provincial) Provincial Services Mental wellness promotion Detoxification services Addiction treatment and aftercare Suicide prevention Mental health treatment and aftercare Client case management Crisis response
Question 26. Data Tracking Tools and Support: Use a check mark (√) to indicate your responses to the following questions (except in 26B).
26A) Do you use any First Nations Health Authority tracking
tool(s) to track your work in Mental Wellness activities? Yes No If No, go to question 27 in the next section. If Yes, go to question 26B.
26B) Provide the name of the tracking tool(s) being used.
In questions 26C) to 26E), rate your level of satisfaction with the tracking tool(s) by indicating your level of agreement with the following statements:
26C) “The tracking tool(s) is (are) useful in tracking work in Mental Wellness.” (Mark your level of agreement with this
statement in the appropriate box.)
Strongly disagree Disagree
Neutral Agree
Strongly agree 26D) “The tracking tool(s) has (have) aided in the Strongly disagree
completion of the CBRT.” (Mark your level of agreement
with this statement in the appropriate box.)
Disagree Neutral Agree
Strongly agree 26E) “The tracking tool(s) has (have) been useful across
activity areas.” (Mark your level of agreement with this
statement in the appropriate box.)
Strongly disagree Disagree
Neutral Agree
Strongly agree
C. Healthy Living
Question 27. Chronic Disease and Injury Prevention: Use check marks (√) to indicate which activities and services were provided. If an activity you provide could fit under more than one category provided below, choose whichever one is the ‘best fit’, and identify it only once.
Chronic Disease and Injury Prevention Activities Offered (√) Activity Physical Activity Check (√ ) Awareness activities related to physical activity (e.g., Diabetes Walks,
Healthy Living Awareness Days) Walking clubs
Sport/recreation activities (e.g., soccer, basketball, etc.)
Traditional physical activities (e.g. jigging, dancing, games, snowshoeing, canoeing)
Nutrition Check (√ ) Cooking sessions or classes (including community kitchens)
Traditional harvesting, food preparation, food preservation (e.g., berry picking, cleaning fish, canning, etc.)
Healthy eating awareness and education (e.g., health fairs, radio shows, etc.)
Grocery tours
Community gardens
Good Food Boxes
Food Vouchers
School-based feeding programs
Additional Check (√ ) Diabetes information sessions or workshops
Development of resource materials (e.g., posters, cookbooks, displays, guides, etc.)
Injury prevention training and awareness raising (e.g., safety committees, tool kits, “A Journey to the Teachings” training, etc.)
Question 28. Diabetes Screening: Indicate which activities and services were provided during the reporting year by checking (√) Yes or No. If an activity could fit under more than one category provided below, choose whichever one is the ‘best fit’ and identify it only once.
Do you conduct diabetes diagnostic screening in your community?
(e.g., fasting glucose, OGTT. See Guide for definitions.) Yes No If Yes, how many individuals were screened in the reporting year?
Do you conduct non-diagnostic diabetes awareness/prevention screening in your community? (e.g., non-diagnostic screenings at schools, workplaces, sporting events, health fairs, etc)
Yes No If Yes, provide an estimate of how many non-diagnostic screenings
were conducted during the reporting year.
Question 29. Diabetes Management: Use check marks (√) to indicate which activities and services were provided. If an activity could fit under more than one category provided below, choose whichever one is the ‘best fit’ and identify it only once.
Diabetes Management Activities Activity Offered Check (√) Diabetes support or healthy living groups
Screening for complications, e.g., retinal screening Screening for complications, e.g., renal screening Referrals to health professionals or services Diabetes self-management sessions
Question 30. Diabetes Clinics and Training: Indicate which activities and services were
provided by checking (√) Yes or No.
Do you provide or support diabetes education clinics and
training for clients to support their self-management (e.g., blood
sugar testing, foot care, diet and exercise advice, traditional
activities)?
Yes No If Yes, how many individuals were served in the reporting year?
Do you provide foot care clinics? Yes No If Yes, how many individuals were served in the reporting year?
Question 31. Healthy Living Service Linkages: Use a check mark (√) to indicate where
service linkages occurred between community health staff external organizations and
arrangements, collaborations, or processes with external individuals and organizations to facilitate the delivery of health services. See Guide for details and examples.
Type of Service/Service Linkage Regional Health Authority/Health Service Zone Educational
Organizations Organizations Non-Profit Provincial Services Healthy eating/nutrition Physical activity/recreation Specialist care Injury Prevention Treatment/management Diagnostics/screening
Question 32. Tracking Tools: Use check marks (√) to indicate your responses to the
following questions, unless otherwise indicated.
32A) Do you use a diabetes tracking tool, chronic disease registry, or other tracking system in the community to track clients living with type 1 and type 2 diabetes or other chronic diseases?
Yes No If No, go to question 33 in the next section. If Yes, go to question 32B).
32B) According to your tracking system, how many individuals in your community are living with diabetes type 1 and diabetes type 2?
Type 1 Type 2 32C) Was your tracking tool supplied by First Nations Health
Authority? Yes No
If No, go to question 33 in the next section. If Yes, go to question 32D). 32D) Provide the name of the tracking tool(s) being used.
In questions 32E) to 32G), rate your level of satisfaction with the tracking tool(s) by indicating your level of agreement with the following statements:
32E) “The tracking tool(s) is (are) useful for tracking work in Healthy Living.” (Mark your level of agreement with this
statement in the appropriate box.)
Strongly disagree Disagree
Neutral Agree
Strongly agree 32F) “The tracking tool(s) has aided in the completion of the
CBRT.” (Mark your agreement with this statement in the
appropriate box.) Strongly disagree Disagree Neutral Agree Strongly agree 32G) “The tracking tool(s) has been useful across activity
areas” (Mark your level of agreement with this statement in Strongly disagree Disagree
the appropriate box.) Neutral Agree
D. Communicable Disease Control and Management (CDCM)
The reporting period for Section D is April 1 to March 31 unless otherwise indicated for a specific question.
Programs/initiatives included under CDCM are:
• Vaccine Preventable Diseases and Immunization;
• Blood Borne Diseases and Sexually Transmitted Infections (HIV/AIDS)
• Communicable Disease Emergencies; and • Respiratory Infections (Tuberculosis)
Question 33. Number of Health Care Workers in CDCM in Your Community: How many people work in CDCM in your community? ___________
Question 34. Worker Information and Training: In the table, provide the worker
information and indicate the training the CDCM health care workers completed during the reporting year.
Worker Information *Training completed during thereporting year Job Title Worker
Type (Base on the descripti ons in the Guide) Hours
Per Week Certification Type (Use letter codes provided in the Guide for certification type) Completed Certified Training (Indicate completion with a check mark) Continuing Education Training (Indicate completion with a check mark) Short Course Training (Indicate completi on with a check mark)
*Certified Training: Educational program at least one academic year in length. *Continuing Education Training: Short-term courses that upgrade or maintain skills.
*Short Course Training: Courses between 1 week and 3 months that are not recognized with classes in a certification program.
Question 35. Awareness and Education Activities: For each of the program and service areas listed, indicate the number of related awareness and education activities conducted in your community or organization, and provide a brief description of the activities. You will
need extra space for this question. Refer to the Guide for definitions and examples of national, regional and local/community and further details on how to complete this table.
Program and Initiative
Areas National Regional Local/community
Number of Activities HIV/AIDS-Blood Borne and
Sexual Transmitted
Infections Tuberculosis Immunization Pandemic Planning Infection Prevention and Control
Question 36. Health Status Reports: Use check marks (√) to indicate if you received a health status report with data on communicable diseases from each of the following organizations during the reporting year.
Organization Received Health Status Report on Communicable Diseases
from Organization
First Nations Health Authority Yes No
Province Yes No
District/Regional Health Authority Yes No First Nations and Inuit Health Branch (national office) Yes No
Other (please specify) Yes No
Question 37. If you answered No to all organizations in question 36, go to question 38. Otherwise, answer the two questions below.
a) Did any report you received contain information specific to your community? Yes No If No, go to question 38.
b) Did you use this report for programming decisions in your community? Yes No
If you answered Yes to part b), provide a very brief description below of how the report was used. If you answered No to part b), provide a very brief description of why you didn’t use the report for programming decisions.
Question 38. Pandemic Plans
Question 39. Indicate the population numbers in your community for each age group.
Age Groups
Population Numbers (Include all people living on-reserve, including non-First Nations)
Population Data Source (e.g., AANDC, Health Centre data, other community data) Children less than 1 year
Children 1 to 4 years
Children/ youth 5 to 19 years Adults 20 to 59 years
Adults 60 years and over Total population
38A) Does your community have a Pandemic Plan? Yes (If No, go to question 39) No 38B) When was your community Pandemic Plan last
updated? Day/Month/Year
38C) Has your community tested its Pandemic Plan
engaging the appropriate stakeholders as identified in the Plan?
Yes No
(If No, go to question 38e) 38D) When was your community plan last tested? Day/Month/Year
38E) Does your community have an all hazards emergency plan?
Yes No
(If No, go to question 39) 38F) Has your community Pandemic Plan been integrated
Question 40. Vaccine-Preventable Disease Cases: Do you submit the annual immunization report? Vaccine-Preventable Diseases Yes No Diphtheria Pertussis Tetanus Poliomyelitis
Haemophilus Influenzae, type B (Hib) Measles Mumps Rubella Hepatitis B Invasive Meningococcal Disease Invasive Pneumococcal Disease Varicella
Seasonal Influenza (SI)
Question 41. Immunization Coverage Report: Complete the applicable immunization coverage report form for your region/province according to your provincial immunization schedule. The form will be provided to you by the First Nations Health Authority. Follow the instructions provided in the form and submit it with this completed template.
Note: When completing the immunization coverage report form, be sure to use the reporting period specified in the form (e.g., calendar year, school year, or other period). Immunization coverage report form completed and submitted with reporting template? Yes No
Question 42. TB Testing: Do you submit the monthly reports to BCCDC TB Control? Yes No
Question 43. Use of Provincial or Territorial TB Prevention and Control Programs: Does your community make use of TB clinical, treatment, health promotion, and public
health expertise and resources from the provincial or territorial TB prevention and control programs? Indicate your response with check marks (√) below.
Not applicable because no provincial TB prevention and control programs are available. If not applicable, go to question 45.
Yes, our community makes use of the available expertise and resources.
No, our community does not make use of the available expertise and resources. If No, go to question 45.
If Yes, use check marks (√) to indicate the program elements for which the expertise and
resources are being used.
Program Development Program Implementation Program Evaluation Research
Clinical advice
Question 44. Access to Referrals and Services for HIV Testing and Treatment: Indicate your responses with check marks (√). For a definition of “near”, see the Guide.
Is HIV testing accessible on or near the reserve? Yes No Is HIV treatment accessible on or near the reserve? Yes No
Question 45. HIV/AIDS Support Groups: Are there any HIV/AIDS support groups in your community? Use check marks (√) to indicate your responses.
Yes No
If No, indicate all of the reasons why no HIV/AIDS support groups exist in your community. Limited funding
Insufficient capacity to establish and lead support groups (e.g., sufficient funding is available but there is a lack of training opportunities, venues, or human resources) Need for support groups not identified (e.g., very low rates of HIV/AIDS infection so
HIV/AIDS is not an issue needing support groups)
Individuals with HIV prefer not to involve health centre staff in their follow-up Individuals with HIV prefer to access services off-reserve, especially for HIV/STIs
Other reasons (please specify) (e.g., stigma associated with HIV/AIDS) __________________________________________________
Question 46. Collection of Other Information: Does your community collect any
additional information on blood borne pathogens and sexually transmitted infections? Yes No
If Yes, briefly list in the box below, the types of information collected (e.g., rates of HIV infection, number of counselling sessions conducted, etc.).
Note: You do not have to provide the actual data, just the types of information collected.
E. Home and Community Care
All communities with a Home and Community Care (HCC) Program are expected to use the Electronic Service Delivery Reporting Template (e-SDRT), which includes the Electronic Human Resource Tracking Tool (e-HRTT), and should continue to input information according to the “Other Reporting Requirements” schedule. In addition, please answer the questions in this section.
Question 47. Collaborative Service Delivery: Does your community or organization have
a collaborative service delivery arrangement for HCC services or supports with external
providers such as hospitals (including discharge information agreements), Regional Health Authorities, client care access centres, etc.?
Note: Collaborative arrangements may be formal with a written agreement in the form of a Memorandum of Understanding, protocol, agreement, contract, etc. or informal with a non-written agreement to provide services or information to support HCC client services in your community.
Yes No
If Yes, please complete the following table.
Collaborative Agreement with: Number of Agreements (in place at the end of the reporting year) District or Regional Health Authority
Hospitals
Client Care Access Centres Other (Please specify)
Question 48. Complaints and Appeals: Do you have a process in place to manage HCC complaints and appeals?
Yes No
Question 49. Incident and Occurrence Reporting: Do you have a HCC incident and occurrence reporting process in place?
Yes No
Question 50. Accreditation: Has your HCC program been accredited by Accreditation Canada or other recognized accreditation organization?
Yes No
F. Clinical and Client Care (CCC)
Section F is to be completed only by communities with a Nursing Station and/or Health Centre with Treatment providing primary care clinical and treatment services twenty-four hours a day, seven days a week (24/7) or five days a week (24/5). If these services are provided by the First Nations Health Authority, this section should be completed by the First Nations Health Authority.
Clinical and Client Care (CCC) services are defined as essential health care services directed toward First Nations individuals living primarily in remote and isolated communities, enabling them to receive the clinical care they need in their home communities. CCC provides assessment, diagnostic, curative and rehabilitative services for urgent and non-urgent care. It also includes health promotion and disease prevention provided at the client and family level in the course of treatment, as well as referral to care facilities outside the community. CCC does not include any services provided for communicable disease control, including immunization and group or community health promotion activities. Refer to the Guide for more details.
Note: In responding to questions in Section F, include encounters and services provided by all members of the CCC team, including physicians and nurses.
Question 51. Community Members Accessing CCC Services: How many community members accessed CCC services at least once during the reporting year? ______________ Question 52. Service Encounters: For each age group in the table, indicate the number of service encounters for urgent (emergency) and non-urgent clinical services. One
community member may have multiple service encounters.
Age Groups Number of CCC Service Encounters During the Reporting Year Urgent Non-Urgent Under 1 year 1-4 years 5-19 years 20-44 years 45-64 years Over 65 years Total Encounters
Question 53. Classification of Primary Care: The World Health Organization has
developed the International Classification of Primary Care based on the primary reasons for primary care encounters. Complete the following table indicating the number of CCC service encounters for each of the classifications.
Classifications: Primary Reasons For Encounters
Number of Encounters During the Reporting Year Diagnostic, screening, and preventive procedures
Medication provision and clinical procedures Symptoms and complaints
Provision of test results and follow-up Referrals
Chronic disease management Other reasons
Question 54. Full-Time Equivalent (FTE) Nursing Positions: Indicate numbers at the end of the reporting year.
54A) How many nursing permanent Full-Time Equivalents (FTEs) are allocated to deliver the services of the Nursing Station/Health Centre with Treatment? ________ 54B) How many nursing permanent FTEs actually deliver the services of the Nursing Station/Health Centre with Treatment? _________
54C) Of the total nursing FTEs, how many were filled by: i.Band-employed nurses _______
ii.Agency nurses _______
iii.Contract (FNHA) Nurses _______
Question 55. Nursing Overtime Hours: Indicate the total number of overtime hours worked by nurses at the end of the reporting year. _____________
Question 56. Nursing Contract Hours: Indicate the total contract hours worked by agency nurses at the end of the reporting year. ______________
Question 57. Course Completion: Indicate the number of nurses who have completed the following mandatory courses and certifications. Refer to the Guide for course
descriptions. Course Number of Nurses Completing Total # of Training Hours Pathophysiology
Advanced Health Assessment
Pharmacotherapeutics (including a module or course to
meet the upcoming Section 56 Ministerial exemption on
Controlled Drugs and Substances Act (CDSA)) Basic Trauma Life Support
International Trauma Life Support Advanced Trauma Life Support Basic Cardiac Life Support (CPR) Advanced Cardiac Life Support Paediatric Advanced Life Support Trauma Nurse Core Course Immunization Certification
Question 58. Referrals: Indicate the number of referrals (scheduled and non-scheduled) made to the following health care provider groups outside the community.
Outside Health Care Provider Groups Number of Referrals General Practitioners/Family Physicians
Physician Specialists
Diagnostic clinics or laboratories (e.g., mammography, X-rays, ultrasound, CT and other imaging)
Therapy services (e.g., physiotherapy, occupational therapy) Dentists/Oral Surgeons
Nurse Practitioners
Question 59. Collaborative Service Delivery: Does your community or organization have
a collaborative service delivery arrangement for CCC services or supports with external
providers such as hospitals (including discharge information agreements), regional health authorities, etc.?
Note: Collaborative arrangements may be formal with a written agreement in the form of a Memorandum of Understanding, contract, etc. or informal with a non-written agreement to provide services or information to support CCC client services in your community.
Yes No
If Yes, please complete the following table. If No, go to question 61.
Collaborative Agreement with: Number of Agreements (in place at the end of the reporting year)
District or Regional Health Authority Hospitals
Other (please specify):
Question 60. Complaints and Appeals: Do you have a process in place to manage CCC complaints and appeals?
Yes No
Question 61. Incident and Occurrence reporting: Do you have a CCC incident and occurrence reporting process in place?