This article has been peer reviewed.
Can Fam Physician 2011;57:e128-33
Research
|
Web exclusive
Accident or osteoporosis?
Survey of community follow-up after low-trauma fracture
Sonia Singh
MD MHScRamona Foster
RNKarim M. Khan
MD PhDAbstract
Objective To describe the postfracture osteoporosis management of at-risk patients presenting with low-trauma fracture in a suburban community hospital setting.
Design Telephone survey.
Setting Hospital emergency department serving a retirement community in White Rock and South Surrey, BC.
Participants Men and women older than 40 years of age who presented with low-trauma fracture between October 1, 2004, and April 30, 2005.
Main outcome measures The prevalence of bone mineral density testing, osteoporosis medication prescriptions, referrals to fall prevention programs, and calcium and vitamin D supplementation within 6 months of the index fracture, as well as patient perceptions of future risk of fracture and sources of osteoporosis information.
Results A total of 181 people met the eligibility criteria and 161 were contacted; 84 (52%) people responded, of whom 53 were interviewed. At the time of their index fractures, 79% (42 of 53) of patients surveyed were not taking osteoporosis medication. After the index fracture, 30% (16 of 53) received new bone mineral density testing, and 8% (4 of 53) were starting courses of new osteoporosis medication. Sixty-eight percent (36 of 53) of all patients were taking calcium supplements and 50% (26 of 53) were taking vitamin D supplements. Eight percent (4 of 53) of patients were referred to a fall prevention program and 9% (5 of 53) were prescribed hip protectors; 19% (10 of 53) of patients thought they were at risk of having another fracture.
Conclusion Osteoporosis management of patients after low-trauma fracture in this community was suboptimal; the role of the media, family and friends, and allied health professionals to prevent fractures in at-risk individuals needs to be further explored.
EDITOR’S KEY POINTS
• Low-trauma fractures are associated
with osteoporosis and a high risk of future fracture, but many patients with low-trauma fractures do not receive the recommended care for future fracture prevention.
• Low-trauma fractures in people older
than 40 years of age should be seen as a marker for osteoporosis by both health providers and patients. The connections among low-trauma fracture, low bone strength, and increased risk of future fracture remain poorly understood by most patients.
• Future fracture prevention strategies
Cet article a fait l’objet d’une révision par des pairs.
Can Fam Physician 2011;57:e128-33
Accident ou ostéoporose?
Enquête sur le suivi communautaire
d’une fracture résultant d’un traumatisme peu sévère
Sonia Singh
MD MHScRamona Foster
RNKarim M. Khan
MD PhDRésumé
Objectif Décrire comment on traite l’ostéoporose post-fracture chez les patients à risque qui consultent pour une fracture résultant d’un traumatisme peu sévère dans le contexte d’un hôpital communautaire de banlieue.
Type d’étude Enquête téléphonique.
Contexte Service hospitalier d’urgence desservant une localité de retraités à White Rock et South Surrey, BC.
Participants Hommes et femmes de plus de 40 ans consultant pour une fracture résultant d’un traumatisme peu sévère entre le 1er octobre 2004 et le 30 avril 2005.
Principaux paramètres à l’étude Prévalence des mesures de densité minérale osseuse, prescriptions de médication pour l’ostéoporose, références à des programmes de prévention des chutes et prescriptions de suppléments de calcium et de vitamine D dans les 6 mois suivant la fracture, et perception des patients concernant le risque de fracture ultérieure et leurs sources d’information sur l’ostéoporose.
Résultats Sur 181 personnes répondant aux critères de sélection, 161 ont été contactées; 84 personnes (52 %) ont répondu et 53 d’entre elles ont été interviewées. Au moment de la
fracture suspecte, 79 % (42 sur 53) des participants ne prenaient pas de médication pour l’ostéoporose. Après la fracture, 30 % (16 sur 53) ont eu une nouvelle mesure de densité minérale osseuse et 8 % (4 sur 53) ont débuté un traitement pharmacologique pour l’ostéoporose. Sur les 53 patients, 36 (68 %) prenaient des suppléments de calcium et 26 (50 %) des suppléments de vitamine D. Quatre patients sur 53 (8 %) ont été référés à un programme de prévention des chutes et 5 (9 %) ont reçu une prescription pour des protecteurs de hanche; dix patients (19 %) estimaient être à risque d’avoir une autre fracture.
Conclusion La façon de traiter l’ostéoporose chez des patients victimes d’une fracture résultant d’un traumatisme peu sévère était sous-optimale dans cette communauté; on devra explorer davantage le rôle des médias, de la famille, des amis et des autres professionnels de la santé afin de prévenir les fractures chez les sujets à risque élevé.
POINTS DE REPèRE Du RéDacTEuR
• Les fractures résultant de traumatismes
peu sévères sont souvent associées à l’ostéoporose et à un fort risque de nouvelles fractures, mais plusieurs patients avec de telles fractures ne reçoivent pas les soins recommandés pour prévenir d’autres fractures.
• Chez les plus de 40 ans, les fractures
résultant de traumas mineurs devraient être considérées comme des indices d’ostéoporose par le personnel soignant et le patient. La plupart des patients ne comprennent pas le lien qui existe entre une fracture résultant d’un traumatisme peu sévère, un os moins solide et un risque accru de future fracture.
• Les stratégies pour prévenir de nouvelles
Research
|
Accident or osteoporosis?
L
ow-trauma fracture (fracture due to a fall from standing height or less) might be the first indica-tion of underlying osteoporosis. Quite often these fractures are attributed to accidents. The fracture is treated and patients go through rehabilitation to regain lost function. Why the fracture occurred and what can be done to prevent future fractures are rarely explored. Despite the well-established association between low-trauma fractures with underlying osteoporosis and an elevated risk of future fracture (relative risk 2 to 19),1-3 less than 30% of people who sustain low-trauma frac-tures receive investigation or treatment for osteopo-rosis.4-8 A systematic review of 35 studies worldwide suggests that this care gap is an international phenom-enon.9 Current Osteoporosis Canada clinical practice guidelines recommend that patients who suffer low-trauma fracture should be investigated and consid-ered for osteoporosis treatment, including medications, lifestyle changes, fall prevention strategies, calcium and vitamin D supplementation, and exercise.10 Just as chest pain initiates investigation for coronary artery disease, low-trauma fracture should initiate investiga-tion for osteoporosis.The health care expenditure associated with osteoporosis-related fractures is estimated at $1.2 billion per year in Canada.11 Morbidity and mortality associated with these fractures is high. Following hip fracture, 50% of patients are unable to walk without aid, 25% require long-term care placement, and 20% die within the first year.12 Fractures of the wrist, ver-tebra, and humerus also lead to a lower quality of life and chronic disability.13 Therefore, there is a strong incentive to try to reduce the mortality, morbidity, and financial burden suffered by patients after low-trauma fracture.
Studies looking at ways to close this care gap have focused on urban hospitals or outpatient follow-up clinics, emergency department (ED) follow-up ini-tiatives, or nurse case managers.14-20 These findings might not apply to rural and suburban community hospital settings, where much of the fracture follow-up is provided by community-based family physi-cians. A limited number of studies have taken a more community-based approach in rural settings.21 To our knowledge, this is the first study conducted in a com-munity hospital setting in British Columbia that takes a broad approach to describing community follow-up for osteoporosis after low-trauma fracture. This study represents the first step in a research program with the objective of developing a broad-based community program to address fracture prevention in at-risk indi-viduals. To develop such a program, we wanted to first identify local gaps and strengths in care and identify potential community resources for postfracture man-agement. The objective of our study was to describe
the current management of osteoporosis after low-trauma fracture in a suburban community hospital setting.
METhODS
The sampling frame for the survey consisted of all con-senting adults older than 40 years of age who presented to the Peace Arch Hospital ED with low-trauma frac-ture between October 1, 2004, and April 30, 2005. The community of White Rock and South Surrey, BC, is a popular retirement community located within the Fraser Health Authority. Approximately 25% of the popula-tion is older than 65 years of age and at high risk of osteoporosis-related fracture. According to data from medical records, the local community hospital, Peace Arch Hospital, treats approximately 400 low-trauma frac-tures per year in patients older than 40 years of age. Low-trauma fracture was defined as a fracture due to a fall from standing height or less. We conducted a 6-month follow-up survey from April 2005 to December 2005.
The study population comprised a sample of all patients who provided informed consent and who had sufficient cognitive and English-language skills to com-plete the telephone survey with the research nurse (R.F.). We excluded patients who were younger than 40 years, who did not have low-trauma fracture by history, or who had underlying bone disease other than osteo-porosis. Potential study subjects were identified by ED chart audits using a standardized audit tool, and con-sent packages were con-sent to all potential study subjects with an invitation to participate in the study. The con-sent form included optional concon-sent for review of family physician charts to assess validity of self-report.
Given the time frame and available resources, a tar-get sample size of 100 patients was deemed adequate by the research team to describe the osteoporosis man-agement and community resources accessed by people after low-trauma fracture. Based on a 1-month medi-cal record audit and a recruitment of 50%, we estimated that 7 months would be sufficient time to recruit 100 study subjects.
audit was performed by the principal investigator, who was blinded to the results of the patient questionnaires. Ethics approval for the study was obtained through the Research Ethics Board of the Fraser Health Authority in British Columbia.
Management of osteoporosis
Management of osteoporosis was divided into 5 over-arching categories: osteoporosis diagnosis and treat-ment (including bone mineral density [BMD] testing, diagnosis of osteoporosis, and treatment with osteopo-rosis medication); lifestyle changes (including diet, exer-cise, use of vitamin D and calcium supplements, home modifications, and hip protectors); referrals to osteopo-rosis or fall prevention programs; sources of information about osteoporosis; and patient perceptions of future fracture risk.
Data analysis
Descriptive statistics were used to describe the current osteoporosis follow-up practices in the White Rock and South Surrey community. Associations between patient characteristics and outcome measures were explored using χ2 and Cramer V tests using Microsoft Excel and SPSS (version 14.0) statistical programs.
RESuLTS
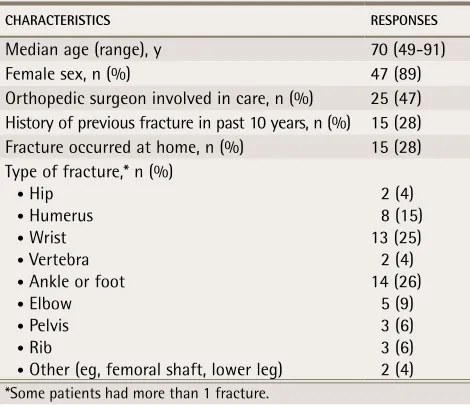
Of the 181 patients who met the sampling frame cri-teria, 20 did not have mailing addresses available; of the 161 remaining, 84 (52%) responded to our invita-tion to participate. Of the respondents, 31 patients could not participate in the study for the following reasons: poor health (n = 2), overlying conditions (eg, cancer, dementia; n = 5), out of the area (n = 4), no interest (n = 5), poor English-language skills (n = 1), or no actual low-trauma fracture (n = 10); 3 patients were deceased at the time of invitation and 1 could not be reached. Therefore, 53 patients remained who were subsequently interviewed and included in the analy-sis. The median age of participants was 70 years, 89% of patients were women, 28% of fractures occurred at home, 47% of patients saw orthopedic surgeons for care, and 28% of patients had had previous fractures in the past 10 years. The most common fractures were wrist and ankle or foot (Table 1).
Results of the 6-month follow-up of osteoporosis diagnosis and treatment measures are outlined in Table 2. Briefly, 11 (21%) of the 53 respondents were already taking osteoporosis medication before their index frac-tures; 4 (8%) had started taking osteoporosis medication within 6 months of their fractures; 16 (30%) had new BMD tests ordered; and 18 (34%) were given new diag-noses of osteopenia or osteoporosis.
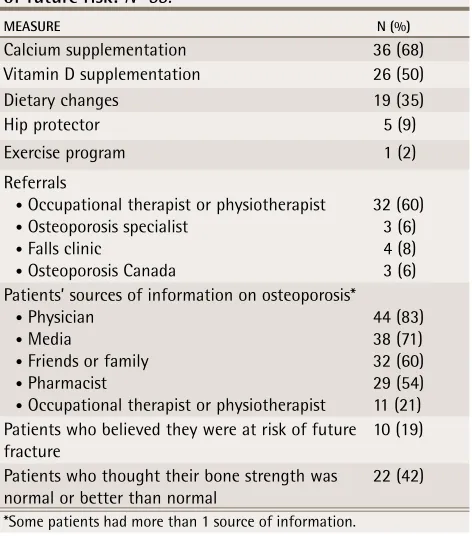
With respect to lifestyle changes, referrals, resources, and patient perceptions after 6 months (Table 3), 68% (36 of 53) were taking calcium supplements, 50% (26 of 53) were taking vitamin D supplements, 35% (19 of 53) had been told to make dietary changes, and 60% (32 of 53) had been referred to occupational or physical thera-pists. All other referrals for osteoporosis-related services occurred in less than 10% of patients. The most common source of osteoporosis information was physicians (for 83% of participants), followed by media (71%), friends and family (60%), pharmacists (54%), and occupational therapists or physiotherapists (21%). Nineteen percent of patients believed they were at risk of future fractures. Most patients thought that their bone strength was nor-mal or better than nornor-mal. Within the 6-month follow-up period, 5 patients (9%) experienced second fractures; 2 of these patients still had not been prescribed any osteoporosis medication.
Patients who had had fractures in the past 10 years were more likely to be taking osteoporosis medication 6 to 9 months after the index fracture compared with those without previous fracture (53% vs 23%, P = .011). Patients were somewhat more likely to be taking osteoporosis medication if they had had BMD testing
Table 1.
Patient characteristics:
N=53.
CHARACteRiStiCS ReSPONSeS
Median age (range), y 70 (49-91)
Female sex, n (%) 47 (89)
Orthopedic surgeon involved in care, n (%) 25 (47) History of previous fracture in past 10 years, n (%) 15 (28) Fracture occurred at home, n (%) 15 (28) Type of fracture,* n (%)
• Hip • Humerus • Wrist • Vertebra • Ankle or foot • Elbow • Pelvis • Rib
• Other (eg, femoral shaft, lower leg)
2 (4) 8 (15) 13 (25) 2 (4) 14 (26) 5 (9) 3 (6) 3 (6) 2 (4)
*Some patients had more than 1 fracture.
Table 2.
Management measures after fracture—
osteoporosis diagnosis and treatment:
N=53.
MeASuRe N (%)
BMD test 16 (30)
Diagnosis of osteoporosis or osteopenia 18 (34) Taking osteoporosis medication
before index fracture 11 (21) Prescribed new osteoporosis medication after index
fracture 4 (8)
Research
|
Accident or osteoporosis?
(43% vs 19%, P = .057) or if they had been given a diag-nosis of osteoporosis (78% vs 3%, P < .001). Age, sex, type of fracture, orthopedic specialist involvement, and patient perception of future fracture risk were not asso-ciated with diagnosis of osteoporosis, referrals for BMD testing, or prescribing of new osteoporosis medications.
Of the 53 participants, 15 (28%) agreed to medical chart audits to validate the self-reports. There were no indications of referrals made, osteoporosis medication prescribed, BMD tests performed, or osteoporosis diag-nosed in the medical records that the patients had not already reported.
DIScuSSION
The results of our study suggest that follow-up for pos-sible osteoporosis treatment after low-trauma fracture in our community remains suboptimal despite exten-sive public education and continuing medical educa-tion about osteoporosis. Although there was a positive association between presence of previous fracture and the likelihood of osteoporosis medication, 1 out of every 10 patients in our study had had additional frac-tures in the 6 months after the index fracture and less than half were started on osteoporosis medications. These results are comparable to those of a similar US study limited to patients hospitalized for low-impact
trauma.22 Twelve months after discharge from hospital, only 26% of patients had been prescribed osteoporosis medication. Calcium and vitamin D supplementation was more frequently reported in our study (68% and 50%, respectively), compared with the US study (22% and 4%, respectively).
Despite the presence of a comprehensive geriatric health program in the White Rock and South Surrey community, very few patients were referred for falls assessment. Most patients were unaware that they were at high risk of future fractures. Only 19% of patients thought they were at risk of future fractures and most thought their bone strength was normal or better than normal. The links between low-trauma fractures, low bone strength, and increased risk of future fracture remain poorly understood by most patients. These link-ages need to be better understood and addressed more effectively by health care providers in order to improve patients’ awareness of their own personal fracture risk.
Patients reported obtaining health information from a variety of different allied health professionals. Physiotherapists or occupational therapists, community pharmacists, home care personnel, ambulance attend-ants, and ED nurses all interact with patients with low-trauma fractures and could play a role in alerting family physicians to the possibility of low-trauma fracture and the need for osteoporosis assessment.
In the 5 years before our survey, there had been a substantial effort in the White Rock and South Surrey community to educate the public and health provid-ers about osteoporosis. In 2000, osteoporosis public education classes were established covering pathogen-esis, medications, BMD testing, exercise, diet, and fall prevention. Large public forums on osteoporosis (with up to 100 participants) took place every year, hosted by Osteoporosis Canada and the Health Authority Osteoporosis Education Group. The Osteoporosis Canada local chapter staged 4 to 5 smaller public events each year. Continuing medical education courses on osteoporosis for health care providers took place 4 to 5 times per year. Our study suggests that public and health care provider education is not enough and needs to be supplemented with improved communication and integration among family physicians, specialist physi-cians, allied health providers, and community workers. A more comprehensive community approach could be more successful in intensifying investigation and treat-ment of osteoporosis after low-trauma fracture. Our results are consistent with those of Jaglal et al21 who used a multi-component tool kit to educate health pro-viders and patients in 5 rural communities in Ontario about the connection between osteoporosis and low-trauma fracture. Their before-and-after study showed no increase in investigation or treatment of osteoporo-sis following low-trauma fracture and concluded that
Table 3.
Prevention measures after fracture—lifestyle
changes, referrals, resources, and patient perceptions
of future risk:
N=53.
MeASuRe N (%)
Calcium supplementation 36 (68) Vitamin D supplementation 26 (50)
Dietary changes 19 (35)
Hip protector 5 (9)
Exercise program 1 (2)
Referrals
• Occupational therapist or physiotherapist • Osteoporosis specialist
• Falls clinic
• Osteoporosis Canada
32 (60) 3 (6) 4 (8) 3 (6) Patients’ sources of information on osteoporosis*
• Physician • Media
• Friends or family • Pharmacist
• Occupational therapist or physiotherapist
44 (83) 38 (71) 32 (60) 29 (54) 11 (21) Patients who believed they were at risk of future
fracture 10 (19)
Patients who thought their bone strength was
normal or better than normal 22 (42)
successful interventions had to be more targeted (ie, directly linking patients to their physicians) and had to be addressed within the context of the health care sys-tem and resources available in local communities and provinces.
Limitations
This study was based on a relatively small sample and examined osteoporosis management from 1 community only. There were few male patients in the study, which limited our ability to describe osteoporosis follow-up in men. We also had few patients with hip fractures—sev-eral of the patients with hip fractures died within the 6-month follow-up period or had other medical com-plications that precluded inclusion in the study (eg, brain injury, dementia). Given a relatively low participa-tion rate, our sample might not be representative of all patients presenting to our ED.
Conclusion
Despite extensive public and health care education on the subject of osteoporosis, follow-up for osteoporosis after low-trauma fractures in a retirement community in British Columbia continues to be suboptimal. Strategies to better identify high-risk patients and initiate therapy need to be developed that use the broad range of health care professionals interacting with patients with low-trauma fractures. Patients are poorly informed about their personal future fracture risks after low-trauma fracture, and additional research might help to better understand and address these misperceptions.
Dr Singh is a family and emergency physician with the Fraser Health Authority in White Rock, BC. Ms Foster is a registered nurse and a senior biopharma-ceutical representative with Amgen Canada in Vancouver, BC. Dr Khan is Professor in the Department of Family Practice and co-founder of the Centre for Hip Health and Mobility at the University of British Columbia in Vancouver and Fellow of the Australasian College of Sports Physicians.
Contributors
Dr Singh was involved at all stages of the project, from initiating the study design and preparing all data collection instruments to data analysis and manu-script preparation. Ms Foster was involved in designing data collection instru-ments, interviewing all study participants, analyzing the data, and preparing the manuscript. Dr Khan was involved in the study design, in determining outcome measures, and in the manuscript preparation.
Acknowledgment
Dr Singh is supported by a research fellowship from the Department of Family Medicine at the University of British Columbia in Vancouver.
Competing interests
Ms Foster is currently employed by Amgen Pharmaceuticals but participated in this research prior to this employment.
Correspondence
Dr Sonia Singh, Fraser Health, Peace Arch Hospital, 15 521 Russell Ave, White Rock, BC V4B 2R4; e-mail [email protected]
References
1. Klotzbuecher CM, Ross PD, Landsman PB, Abbott TA 3rd, Berger M. Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 2000;15(4):721-39. 2. Cuddihy MT, Gabriel SE, Crowson CS, O’Fallon WM, Melton LJ 3rd. Forearm
fractures as predictors of subsequent osteoporotic fractures. Osteoporos Int
1999;9(6):469-75.
3. Johnell O, Kanis JA, Odén A, Sernbo I, Redlund-Johnell I, Petterson C, et al. Fracture risk following an osteoporotic fracture. Osteoporos Int
2004;15(3):175-9. Epub 2003 Dec 23.
4. Hajcsar EE, Hawker Gillian, Bogoch ER, Investigation and treatment of osteo-porosis in patients with fragility fractures. CMAJ 2000;163(7):819-22. 5. Khan SA, de Geus C, Holroyd B, Russell AS. Osteoporosis follow-up after
wrist fractures following minor trauma. Arch Intern Med 2001;161(10):1309-12.
6. Port L, Center J, Briffa NK, Nguyen T, Cumming R, Eisman J. Osteoporotic fracture: missed opportunity for intervention. Osteoporos Int 2003;14(9):780-4. Epub 2003 Aug 7.
7. Petrella RJ, Jones TJ. Do patients receive recommended treatment of osteopo-rosis following hip fracture in primary care? BMC Fam Pract 2006;7:31. 8. Metge CJ, Leslie WD, Manness LJ, Yogendran M, Yuen CK, Kvern B.
Postfracture care for older women. Gaps between optimal care and actual care. Can Fam Physician 2008;54:1270-6.
9. Giangregorio L, Papaioannou A, Cranney A, Zytaruk N, Adachi JD. Fragility fractures and the osteoporosis care gap: an international phenomenon. Semin Arthritis Rheum 2006;35(5):293-305.
10. Brown JP, Josse RG; Scientific Advisory Council of the Osteoporosis Society of Canada. 2 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada. CMAJ 2002;167(10 Suppl):S1-34. Errata in: CMAJ
2003;168(4):400, CMAJ 2003;168(5):544, CMAJ 2003;168(6):676. 11. Tenenhouse A, Kreiger N, Hanley D. Canadian multicentre osteoporosis
study (CaMos). Drug Dev Res 2000;49(3):201-5. Epub 2000 Apr 27. 12. Riggs BL, Melton LJ 3rd. The worldwide problem of osteoporosis: insights
afforded by epidemiology. Bone 1995;17(5 Suppl):505S-11S.
13. Adachi JD, Ioannidis G, Pickard L, Berger C, Prior JC, Joseph L, et al. The asso-ciation between osteoporotic fractures and health-related quality of life as mea-sured by the Health Utilities Index in the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos Int 2003;14(11):895-904. Epub 2003 Aug 12. 14. McLellan AR, Gallacher SJ, Fraser J, McQuillian C. The fracture liaison
service: success of program for the evaluation and management of patients with osteoporotic fracture. Osteoporos Int 2003;14(12):1028-34. Epub 2003 Nov 5. 15. Cuddihy MT, Amadio PC, Gabriel SE, Pankratz VS, Kurland RL, Melton LJ
3rd. A prospective clinical practice intervention to improve osteoporosis management following distal forearm fracture. Osteoporos Int 2004;15(9):695-700. Epub 2004 Mar 9.
16. Majumdar SR, Rowe BH, Folk D, Johnson JA, Holroyd BH, Morrish DW, et al. A controlled trial to increase detection and treatment of osteoporosis in older patients with a wrist fracture. Ann Intern Med 2004;141(5):366-73.
17. Majumdar SR, Johnson JA, McAlister FA, Bellerose D, Russell AS, Hanley DA, et al. Multifaceted intervention to improve diagnosis and treatment of osteoporosis in patients with recent wrist fracture: a randomized controlled trial. CMAJ 2008;178(5):569-75.
18. Majumdar SR, Beaupre LA, Harley CH, Hanley DA, Lier DA, Juby AG, et al. Use of a case manager to improve osteoporosis treatment after hip fracture: results of a randomized controlled trial. Arch Intern Med 2007;167(19):2110-5. 19. Ashe M, Khan K, Guy P, Kruse K, Hughes K, O’Brien P, et al.
Wristwatch-distal radial fracture as a marker for osteoporosis investigation: a con-trolled trial of patient education and a physician alerting system. J Hand Ther
2004;17(3):324-8.
20. Davis JC, Guy P, Ashe MC, Liu-Ambrose T, Khan K. HipWatch: osteoporosis investigation and treatment after a hip fracture: a 6-month randomized con-trolled trial. J Gerontol A Biol Sci Med Sci 2007;62(8):888-91.
21. Jaglal SB, Hawker G, Bansod V, Salbach NM, Zwarenstein M, Carroll J, et al. A demonstration project of a multi-component educational intervention to improve integrated post-fracture osteoporosis care in five rural communities in Ontario, Canada. Osteoporos Int 2009;20(2):265-74. Epub 2008 Jun 3. 22. Simonelli C, Chen YT, Morancey J, Lewis AF, Abbott TA. Evaluation and