among Pregnant Women in Machakos Central
Division,
Kenya.
By:
Kyania Martin Mulala, BSc.N(UoN),
157/12642/2005
Thesis submitted in partial fulfillment for the requirement
of the award of a Degree of Master of Public Health in the
"-School of Health Sciences of Kenyatta University.
May, 2013
-Xyama, Martm MuJaIa -Perception and practices on malaria control among
1~llllml~lnI~"lnllll~
2013/431922DECLARA TION
This thesis is my original work and has not been presented for a degree inany other University.
Signature ...
Date ...:2-.0. (. . .,. ?""o.13. Kyania Martin Mulala,
157/12642/2005.
Supervisors:
This thesis has been submitted for examination with our approval as University supervisors.
.
11)(.
'
Signature.Lj ."'..,/ . f\fI ~.
Date ..I:. ~(;~)....7..'/' .?to.I.?J. .. Professor Michael Otieno,
Department of Medical Laboratory Sciences, Kenyatta University.
Signature
j~.:.
Date ....•51..
l{/ .?-:-:':?7.3
Dr. George O. Orinda,
DEDICATION
ACKNOWLEDGEMENT
I would like to thank members of the Department of Community Health of the School of
Health Sciences, Kenyatta University, for providing a conducive environment which ultimately enabled me complete this study. I register very special thanks to my
supervisors; Dr. Michael Otieno from the department of Medical Laboratory Sciences,
Dr. George Orinda of the Department of Biochemistry and Biotechnology, and Dr.
Syprine A. Otieno from the department of Zoological Sciences for giving valuable advice
in writing the thesis. Very special thanks go to the Chairman of the Department, Dr. Isaac Mwanzo, for his advice and encouragement throughout the research process. Without
their support it would have been difficult to complete my research work and write up this
ACT
AL
ANC CDC CME DDT DOT FGDEIR
GDP GoK I-lIV lEC IPTi IRS !TN KDHS KMOH KMOMS MCI-I MDGs MOT--!NGO
ABBREVIATIONS
Arternisininf.ombination Therapy
Arternetherl.umenfantrine
Antenatal Care
Centers for Diseases Control
Continuous Medical Education
Dichlorodiphenyltrichloroethane
Directly Observed Therapy
Focus Group Discussion
Entomological Inoculation Rate
Gross Domestic Product
Government of Kenya
Human Immunodeficiency Virus
Information Education and Communication
Intermittent Preventive Treatment in infants
Indoor residual Spraying
Insecticide Treated bed Nets
Kenya Demographic Health Survey
Kenya Ministry of Health
Kenya Ministry of Medical Services
Maternal and Child Health
Millennium Development Goals
Ministry of Health
PfEMPi
RBM
RDTs
SP
SSA
SPSS
Plasmodiumfalciparum Erythrocyte Membrane Protein 1.
Roll Back Malaria
Rapid Diagnostic Tests
SulphadoxinePyrimethamine(Fansider)
Sub-Saharan Africa
DEFINITION OF TERMS
Anthropophily: Tendency to target humans for blood meal.
Awareness: Interested in and knowing about something especially current events. Endemic: Regularly found in a particular area or country or particular group of
people.
Endophily: Tendency to enter and rest inside of houses.
Epidemic: The rapid spread of a disease among many people inthe same place. Factor: Underlying dimension that positively or negatively influences other
observed variables.
Incidence: Number of new episodes of illness arising in a population over an
estimated period.
insecticide: Chemical substance used to kill or inhibit insect vectors. Morbidity: The state of being diseased
Mortality: The incidence of death in apopulation in a given period Parasite: A living thing that lives in or on another living organism.
Perception: This is the ability to see, hear or understand things. A deeper natural understanding and awareness than isusual. Awareness increases
perception.
Prevalence: A measure of morbidity based on the current sickness ina population estimated either at a particular time or over a stated period.
Strategy:
Vector:
A plan designed for aparticular purpose.
TABLE OF CONTENTS
DECLARA1'ION i
DEDICATION ii
ACI(NOWLEDGEMENrr iii
ABB]~E\!IA'I'lONS iv
DEFINITION OF TERMS vi
TA.BLE OF CON'fEN1'S viii
LISrr OF 'I'ABLES xiv
LIS1' OF FIG··UT{ES xv
A.BS'rn.AC'r xvi
CHAPTER ONE: INTRODUCTION 1
J.J Background of the study 1
J.2 Problem statement 3
1.3 Justification 4
1.4 Research questions 5
J.5 Hypothesis 5
1.6 Objectives of the study 5
1.6.1 Broad objective : 5
1.6.2 Specific objective 5
CH
A
PT
E
R T
W
O
:
LI
TE
R
ATU
R
E
R
EVIEW
7
2.1 Malaria: History, etiology and morbidity 7
2.2 Occurrence and distri bution of malaria in Kenya 12
2.2.1 Lakeside endemic malaria 13
2.2.2 Coastal endemic malaria 13
2.2.3 Highlandmalaria 13
2.2.4 Arid, seasonal malaria 14
2.2.5 Low malaria risk 14
2.3 Parasitology '" 14
2.3.1 Life cycle of plasmodium parasite 14
2.4 Pathogenesis 17
2.5 Clinical features 18
2.5.1 Uncomplicated malaria 18
2.5.2 Severe malaria 19
2.6 Diagnosis 19
2.6.1 Microscopy 19
2.6.2 Rapid diagnostic tests 20
2.7 Management 20
2.8 Prevention and Control 21
2.8.1 Intermittent preventive treatment in pregnancy 22
2.8.2 Insecticide treated bed nets 22
2.8.3 Chemoprophylaxis in the non-immune population 23
2.8.4 Community education on behavior change 23
CHAPTER THREE: MATERIALS AND METHODS 26
3.1 Research design 26
3.2 Study site 26
3.3 Study population 26
3.4 Sample size determination 27
3.5 Study variables 28
3.6 Data collection procedures 28
3.7 Ethical considerations 28
3.8 Data management, analysis and presentation 29
CHAPTER FOUR: RESULTS AND DISCUSSION 30
4.1 Results 30
4.1.1 Introduction 30
4.1.2 Socio-demographic/economic factors 30
4.1.2.1 Age of respondents 30
4.1.2.2 Marital status 31
4.1.2.3 NUJ11ber of children 31
4.1.2.4 Level of education 32
4.1.2.5 Religion 33
4.1.2.6 Residence 33
4.1.2.7 Occupation 35
4.1.3 Perceptions about malaria 35
4.1.3.1 Perceived common diseases 35
4.1.3.2 Perceived risky practices 36
cl\1YATTA
U
NIVfRS
ITV
4.1.3.2 Perceived risky practices 36
4.1.3.3 Perceived reasons for malaria spread 37
4.1.3.4 Perception on treatment and control.. 37
4.1.3.5 Perception on group at high risk of malaria infection 39
4.1.3.6. Danger of malaria during pregnancy .40
4.1.4 Awareness on causes, signs and symptoms of malaria 40
4.1.4.1 Associated causes of malaria .40
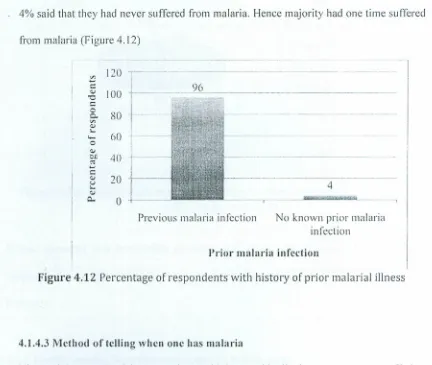
4.1.4.2 Proportion of respondents having suffered malaria 43
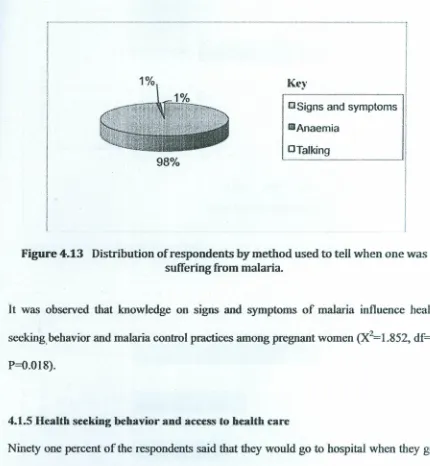
4.1.4.3 Local methods of diagnosing malaria .43
4.1.5 Health seeking behavior and access to healthcare 44
4.1.6 Resources availability 46
4.1.6.1 ITN availability 46
4.1.6.2 Awareness of free IPTs , 47
4.1.6.3 Other methods for mosquito control .48
4.2 Discussion 50
4.2.1 Perceptions about malaria 50
4.2.2 Awareness of causes, signs and symptoms ofmalaria 52
4.2.3 Health seeking behavior and access to care 53
4.2.4 Resources availability for malaria control 54
CHAPTER FIVE: SUMMARY,CONCLUSIONS AND
RECOMMENDATIONS 57
5.1 Introduction 57
5.3 Conclusions 59
5.4 Recommendations 60
5.5 Further research 61
APPENDICES
6
7
Appendix I: Interview Schedule 67
Appendix II: Focus Group Discussion guide 71
Appendix Ill: Map of malaria distribution in Kenya 72
Appendix IV: Letter of approval , , 73
Appendix V: Map of the study area 74
Appendix VI: Current global malaria distribution 75
LIST OF TABLES
Table Page
Table 4.1 Number of children 32
Table 4.2 Occupation 35
Table 4.3 Risky practices to malaria infection 36
Table 4.4 Perception on treatment ofmalaria 38
Table 4.5 Perception on control ofmalaria 48
Table 4.6 Perception on the most risky group 39
Table 4.7 Perception of danger during pregnancy .40
Table 4.8 Level of malaria awareness .41
Table 4.9 Availability of ahealth facility .46
LIST OF FIGURES
Figure Page
Figure 4.1 Age of respondent. 30
Figure 4.2 Marital status 31
Figure 4.3 Education level 32
Figure 4.4 Religion 33
Figure 4.5 Residence .34
Figure 4.6 House status 34
Figure 4.7 Perceived common diseases 36
Figure 4.8 Awareness on malaria spread 37
Figure 4.9 Reasons for malaria spread .41
Figure 4.10 Persistency of malaria .42
Figure 4.11 Period when malaria is high .43
Figure 4.12 Previous malaria attacks .43
Figure 4.13 Diagnosing malaria .44
Figure 4.14 Action taken during sickness .45
Figure 4.15 Time to walk to the nearest health facility .45
Figure 4.16 ITN ownership .46
ABSTRACT
Malaria is endemic in Kenya. It is the most important cause of morbidity and mortality in
children under five years of age. It accounts for 30% of outpatient visits and nearly 20% of admissions to health facilities here Kenya. In Machakos District, Malaria has been the
top cause of morbidity and mortality particularly in children under 5 years and women in the reproductive age. Records from the Machakos District hospital show that malaria cases have been steadily increasing from a low of 151,181 in the year 2002 to a high of 435,987 in the year 2010. The main objective of the study was to establish the perception and practices of pregnant women on malaria control in Machakos Central Division. The research design used was a descriptive survey and the study was done at Machakos
District Hospital. A sample of 384 pregnant women from the division was interviewed using an interview schedule. In addition three focus group discussions of eight respondents each were conducted. Results showed that factors that were found to influence perceptions and practices of pregnant mothers on malaria control were education (X2=8.J5!, df=J, p<0.004), occupation (l=4.029, df=l , p<0.045), believe that malaria can be treated/controlled through medical intervention (X2=!7.703, df=l , p<O.OOOJ), perception that children under five years and pregnant women are at a high risk of malaria infection (X2=8.909, df=l , p<0.003), accessibility of health facility (X2=5.096, df=l , p<0.024), and knowledge on associated causes of malaria(x2=1.8!5, df= 1, p<O.O 18). Focus group discussion revealed that lack of proper information on part of pregnant women on causes and diagnosis of malaria, and availability of control
measures hindered successful control. The study also found that stigma surrounding teenage pregnancy was a major obstacle for pregnant teenagers in their efforts to seek medical care. The study concludes that education and occupation are important factors in
1.1 Background of the study
Malaria is a major public health problem in Kenya, causing an enormous burden to
health and economy. The disease remains a leading cause of morbidity and mortality in
the country, especially in children under five years and pregnant women (KMOH, 2006).
Malaria accounts for 30% of out patient attendances and 19% of admissions to our health
facilities. In Machakos Hospital, cases of reported malaria in the out patient department
stood at 30.8 %, being the highest reported disease by the end of year 20) 0 (KMOMS,
20 I0). The disease is prevalent despite several measures put in place to prevent its
spread.
The main focus of malaria control measures in Kenya include case management (early
diagnosis and prompt treatment with effective drugs), vector control using insecticide
treated mosquito nets (lTNs), malaria intermittent treatment in pregnant women, malaria
epidemics prevention and control, information, education and communication, and
operational research (Mboera et al., 2007). Despite these strategies, malaria cases and
deaths have been increasing in the country, mainly due to injudicious use of antimalarial
drugs, delayed health seeking, and reliance on clinical judgment without laboratory
confirmation in most of the peripheral health facilities(Mboera et al., 2007).
Whilst antimalarial interventions are undoubtedly important, it is also well recognized
that accessibility to anti-malaria interventions alone will not bring about the desired
change. Several studies have demonstrated that compliance to anti-malaria interventions
depends substantially on social, behavioral and cultural factors that affect understanding
and practices about prevention (Agyepong, 1992a; Ahorlu et al., 1997;Espino et al.,
1997; Agyepong and Manderson, 1999b). In addition, factors such as vulnerability,
economic constraints, inadequacy or unavailability of appropriate health services, and
other related factors play an important role in explaining health seeking behavior of the
people (Hausmann et al., 2003)
Studies in the past have mainly been carried out in high malaria risk areas such as the
lakeside and coastalareas due to the overwhelming burden of the disease among young
children and pregnant women in those areas. Recently, however, there has been an
increased need to understand perceptions and practices of the women about the disease,
particularly health and treatment seeking behaviors in low malaria risk areas in Sub
Saharan Africa (Tanner and Vlassoff, 1998; Nuwaha, 2002; Guyatt and Snow, 2004;
Ndyomugyenyi et al., 2007).
Due to the huge burden of malaria among pregnant women and children under the age of
five years, targeting women in the reproductive age group to deal with the disease has
recently been widely recognized. It has been acknowledged that the success of malaria
control inchildren and pregnant women depends on the understanding of the local
socio-cultural factors affecting women's perceptions of causes and modes of transmission of
the disease, health seeking behavior and practices of malaria prevention measures
(Reuben, 1993; Kengeya et al., J994; Rahman et al., 1995; Tarimo et al., 2000; Camara
et al., 2003; Launiala and Kulmala, 2006; Mbonye, 2006). However, research focusing
on malaria issues among women in the reproductive age group with children under the
age of five years in low risk malaria areas has been scarce(Tanner et al., J998; Rahman
Understanding the local perceptions and practices of women is of utmost relevance in
terms of enhancing community's potential to deal with village-based malaria
interventions. This particular study was carried out in a low malaria risk area to examine
women's perceptions and practices related to malaria transmission, symptoms/recognition, treatment, prevention, and treatment seekingbehaviour. The purpose of the study was to generate information that might support the design and implementation of appropriate interventions as part of broader malaria control strategies.
There has been a considerable number of reports about knowledge, attitudes, and
practices relating to malaria and its control from different parts of Africa. These reports
concluded that misconceptions concerning malaria still exist and that practices for the
control of malaria have been unsatisfactory (Vundule and Mharakurwa, 1996; Hla
-Sheinel al., 1998; Miguel et af., 1999). Thus, an advanced knowledge of the community
beliefs and practices with respect to the disease is required to obtain and maintain its
participation insurveillance and control activities (Reubushet af., 1994).
1.2 Problem statement
There has been a steady increase of malaria cases reported in Machakos General Hospital
since the year 2002. Hospital records indicate that malaria cases reported steadily increased from a low of 151,182 in 2002 to a high of 436,500 in 20 IO(KMOMS, 20 I0). Majority of these were pregnant women and children under five years. These cases
accounted for up to 34% of the disease burden inthe district.As such the overall problem addressed in this study is that despite the availability of effective and proven control
methods for malaria, the disease has been on the increase and this therefore calls for the
particularly in the vulnerable groups, namely pregnant women and children under five years.lf the underlying factors are not identified urgently and the incidences of this
disease curbed, we shall continue losing women and children as a result of maternal and
infant mortalities related to malaria. This in the long run will defeat intervention efforts towards the attainment of the 2015 Millennium Development Goals particularly on reduction on child mortality, improvement of maternal health and combating HIV/AIDS, malaria and other diseases.
1.3Justification
Mothers in general are the first persons to identify the fever or health changes on their children and thereby seek healthcare, thus playa major role as they protect themselves and their children. The participation of mothers in fighting malaria plays a vital role not
only for them and their children, but to the entire community in which they live. If
mothers protect themsel ves and their ch iIdren against mosqu ito bites and also seek medical care appropriately, then morbidity and mortality related to malaria are likely to
reduce.
Malaria continues to be the top cause of morbidity and mortality in pregnant women and children under five years of age in spite of available effective and proven control
measures. There is still no effective vaccine for the disease. ln the last five years
approximately 34% of the entire disease burden in Machakos district was due to malaria,
75% of which were children under the age of five years(KMOMS, 20I 0). Cases of this
disease continue to increase every year. These figures are alarming and every option for control ought to be instituted.This study thereforeattempts to fully establish the
1.4Research questions
1.What perceptions do pregnant women inMachakos Central Division have concerning malaria?
2. What is the awareness level of the pregnant women 111Machakos Central Division concerning malaria infection?
3. What actions do pregnant women 111Machakos Central Division take to combat malaria?
4. What necessaryresources do pregnant women in Machakos Central Division possess for malaria control?
1.5 Hypothesis
There is no significant relationship between mothers' perception on malaria and malaria prevalence in Machakos Central Division.
1.60bjectivcs of the study
1.6.1 Broad Objective
To establish theeffect of the perceptions, awareness and practices of pregnant women in Machakos Central Division on malaria control.
1.6.2 Specific Objectives
I. To establish the perceptions of pregnant women In MachakosCentral Division
concerning 11l~laria.
3. To find out the actions taken by pregnant women in Machakos Central Division 111
curbing malaria.
4. To establish availability of resources needed by the pregnant women in Machakos
Central Division for malaria control.
1.6Significance of the study
This study hasestablished the underlying factors hindering pregnant women from
combating malaria. This knowledge may assist policy makers in drawing guidelines that
would also help in controlling malaria.The report will be useful to service providers such
as nurses and doctors in the district in their efforts towards malaria control. Also,
stakeholders in the humanitarian field involved in malaria control will be highlighted
more on malaria control issues and hence provide more support to empower women in
the tight against the disease. And finally, health educators will be provided with extra
information that they would use in teaching the community alternative ways of
CHAPTER TWO:LITERATURE
REVIEW
2.1 Malaria: Historical background, etiology and burden of the disease
Malaria, a mosquito-borne, protozoan disease, is older than recorded history, and
probably plagued prehistoric man (Lambert et 01.,2002). The first record of treatment for the disease dates from 1600 A.D. in Peru, and utilized the quinine-rich bark of the Cinchona tree (Lambert et al., 2002). Scientifically therefore, it is not a newly described disease. The French physician Charles Louis Alphonse Laveran first identified the parasite under the microscope in 1880. Ronald Ross and Giovanni Grassi recognized the
mosquito as the malaria vector in 1897 (Good and Marsh, 2002). Four Nobel prizes have been awarded for work associated with malaria; to Sir Ronald Ross (1902), Charles
Louis Alphonse Laveran (1907), Julius Wagner-Jauregg (1927) and Paul Hermann Muller (1948) (CDC, 2004). However, despite enormous and diverse efforts to control
this disease, malaria is among the top three most deadly communicable diseases and the
most deadly tropical parasitic disease today(Sachs and Maloney, 2002).
Approximately 40% of the world's population lives in regions where malaria transmission is endemic, mainly tropical and sub-tropical regions (Altman et al., 2002). Malaria has been successfully controlled, in fact effectively eliminated, in temperate regions of the world (Sachs and Maloney, 2002). The control strategies employed in temperate regions included changes in agricultural and construction practices, reducing
the availability of standing water, and targeted vector control using insecticides such as
DOT (Greenwood and Mutabingwa, 2002). Industrialization and improved housing
conditions were instrurriental in the elimination of the' disease in temperate countries (Budiansky, 2002). Windows and walls reduce the amount of contact people have with
another factor for the success of erad ication programs as well. The role of the mosqu ito in the life cycle of P. falciparum requires that the parasite be able to maintain an
extended infection in order to ensure transmission ability during the following season
(Kyes et 01.,200 I). Strong seasonality results in lower basal levels of case reproduction
(Sachs and Maloney, 2002). Now that the sequences of the three participants in the life
cycle of human malaria, P. falciparum, Anopheles gambiae, and Homo sapiens, are all
completed and available, perhaps new strategies of disease control will succeed.
Anopheles gambiae, Anopheles arabiensis and Anopheles funestustransmit most of
human malaria and are all found in Africa (Besansky et 01., 2004). Anopheles gambiae,
the most famous and significant of these three, is one of sixty anopheline mosquitoes
able to transmit malaria to humans (Budiansky, 2002). Anopheles gambiae is the
primary malaria vector; this can be attributed, in part, to its relatively long life, strong
anthropophily and endophily (the tendency to target humans for blood meal and the
tendency to enter and rest inside of houses, respectively(Besansky et al., 2004).
Malaria occurs in endemic or epidemic form throughout the tropics except for areas
above 2000metres above sea level: Australia, the USA, and most of the Mediterranean '-'::;"fli"u/
littoral are malaria free (Kumar and Clark, 2002).Although many efforts have been put to
control malaria and been successful to varying degrees, approximately 500 million
clinical cases of malaria are reported each year (Alnwick, 200 I)and mortality estimates
range between 0.7 and 2.7 million. Most of these deaths, (75%) , are young African
In sub-Saharan Africa, where malaria mortality is highest, 90% of reported
malaria-related deaths are children under the age of five (Gardner, 2002). However, the actual
figures of iIIness, morbid ity and mortal ity may be very different from those cited above.
Accuracy is impeded by the fact that most malarial deaths occur at home, many cases are
misdiagnosed and functional microscopes are not available to most clinics (Greenwood
and Mutabingwa, 2002).Unfortunately, the disease burden is on the rise.
Despite the fact that strong attempts to eradicate malaria have been made, the disease
burden isstill on the rise and some estimate that the number of cases could double in the
next twenty years without the development of new methods of control (Sachs and
Maloney, 2002). Aside from the human tragedy this predicts, an economic disaster is
also likely for the stricken countries. Gallup and Sachs (200 I) report that, during the
period 1965 - 1990, the annual growth rates in malarious countries are 1.3% lower
compared to non-malarious countries. This corresponds to a 50% decrease in per capita
Gross Domestic Product (GDP) (Gardner, 2002). Maloney and Sachs (2002)
hypothesize that this apparent correlation between poverty and malaria runs both ways.
Poverty may increase the incidence of malaria; malaria may also increase the likelihood
of poverty. An increase in population in malarious regions, compounded by weak public
health systems in developing countries, climate changes (Hay e/ al., 2004), new
agriculture practices such as irrigation and dam construction (Sachs and Maloney, 2002),
increased resistance-to antimalarial treatments and insecticides and the complexity and
flexibility of the genetics (Gardner, 2002) have all contributed to the increase in malaria.
During the period between 1975-1996, only 3 of 1,223 drugs developed were
outstripped supply. This can be explained, in part, by the fact that the large number of
people suffering from malaria and other diseases commonly found in Africa are not
customers (Kettler and Marjanovic, 2004). They can .not purchase new drugs and therefore do not exist as a viable market for a biotechnology company's investment.
The involvement of biotechnology companies is crucial in the fight against malaria.
When the Plasmodium falciparum sequence became available, the biotechnology
companies acted quickly to advance this knowledge into products. Aside from the new
vaccine candidates developed, biotechnology companies produced both a needle-free
injection device (Bioject Medical Technologies) and kits for parasite detection (AMRAD
corp.) (Kettler and Marjanovic, 2004). The contribution of their research power is
essential for the success of malaria control campaigns. The difficulty of involving the
biotechnology companies lies in their dependency upon earning a profit and in the fact
that they mostly receive outside funding. Funding is not easily procured when a viable
market does not exist. Most biotech companies would be interested in researching these diseases, even if only for public relations purposes, if they were given any compensation
incentive. Policy changes must be made to make the production of these drugs possible.
These policies would need to be enacted on a global scale. Models based on national
laws such as the American Orphan drug act have been proposed (Kettler and Marjanovic,
2004). These would lower the cost and risk for the companies while increasing the
expected return.
Additionally, more specific regions need to be identified as regions In need of more
resources. One study in Kenya showed that the insecticide-treated bed net (ITN)
organizations (NGOs) were present, rather than to areas where malaria transmission was
highest (Greenwood and Mutabingwa, 2002). Organized strategies need to be employed
to achieve the highest possible efficacy. Four studies of home management of malaria
revealed large reductions in severe illness when children were treated at early stages.
Intermittent preventive treatment in infants (IPTi) was tried in conjunction with normal
vaccine schedules. Healthy babies were given full treatments of antimalarial drugs and
this reduced the amount of malaria and anaemia(Toure and Oduola, 2004). One
important element of this study was the Lise of organizations involved in vaccine
distribution to administer malaria treatment. This type of cooperation is cost-effective and could cover extensive areas. These studies suggest that improvements can be made
by training local healthcare workers to educate themselves and people in their
communities about appropriate drugs to prescribe (Toure andOduola, 2004). With the
cooperation of science, government and charitable foundations itmay soon be possible to
bring malaria under control.
Malaria is endemic in Kenya. It remains a leading cause of morbidity and mortality
especially in young children and pregnant women. It accounts for 30% of outpatient
visits and nearly 19% of admissions to health facilities in the country (KMOH, 2006). Its
incidence is still on the increase despite available and effective control tools. Malaria in
Kenya varies from region to region largely due to climate and temperature, including the
effects of altitude.
The KMOH Annual Health Sector Report 2005- 2007 indicated clearly that malaria has
been the top cause of out patient morbidity and that there has been a steady increase in
malaria infection rate in the year 2007 reporting a rate of 52] cases per 1000 population
of people. It was followed by Nyanza and Coast provinces which reported 473 and 270
cases per 1000 population of people respectively. This is contrary to reports that Nyanza
and Coast provinces are more malarious than Eastern province.
In Machakos District, malaria has been the top cause of morbidity and mortality.
Hospital records indicate that malaria cases have been on the increase for the last six
years consecutively. Cases of reported malaria increased from 15 1,184 in the year 2002
up to 363,122 in 2006 and to 436,500 in 2010. Malaria accounted for approximately 34%
of the disease burden in the district. Since not all people visit health facilities when they fall sick, there are many more that die at home and thus the true figures of death and
disease from malaria are likely to be higher. It continues to be a top killer disease in Kenya. It accounts for 34,000 deaths annually among children under five years of age
and more than 8 mill ion out-patient treatments at heal th faci lities, majority being
pregnant women and children under the age of five years (KMOH, 2006a). During
pregnancy, malaria causes anemia, miscarriages and can result in low birth weight
babies. The Roll Back Malaria (RBM) initiative where Kenya is a member is a global
response that recognizes the disease malaria as an economic burden and barrier to
development for m ill ions of Africans.
2.2 Occurrence and distribution of malaria in Kenya
Malaria endemicity in Kenyavaries from region to region and there has been a huge
diversity of risk of malaria infection largely driven by climate and temperature including
broadly categorized into one of the five malaria ecological zones(Appendix II/).These
categories are stated below as has also been noted inKMOMS 2010.
2.2.1 Lakeside endemic
This occurs mainly among many districts close to lake Victoria. Malaria transmission
here occurs throughout the year. The community acquires immunity before adulthood
and the risks of disease and death from malaria are concentrated among children and
pregnant women. Transmission is perennial and the parasite prevalence among children
often exceeds 50%.
2.2.2 Coastal endemic
Coastal region of Kenya is similar in endemicity to the lakeshore region with parasite
prevalence often exceeding 50%. However, the transmission and maximal disease risk
period exhibit strong seasonality and the intensity of transmission is lower as you move
towards Soma Ii boarder.
2.2.3 Highland
These cover areas around mount Kenya; Nanyuki, Meru, Embu, Kirinyaga, and
Muranga. A common feature of malaria in the highland districts is that while there is
always a potential for limited transmission lending itself to an overall low disease risk on
an average year, variations in rainfall and ambient temperatures between years can lead
2.2.4 Arid, Seasonal
Many districts in a large part of North Eastern, North Western, parts of Eastern and
southern part of the Rift valley provinces mostly experience malaria where communities
are located near water(KMOH, 2006b).The arid and rainfall limited effects upon
transmission lend the transmission of parasites only to a few months of the year or absent
during occasional years. Other districts might experience transmission every year for a
few months. All districts in this category will experience low infection prevalence rates
in childhood. The study area for this research lies on this region.
2.2.5 Low malaria risk
This region covers highlands within Central province and Nairobi provmce.
Parasitological surveys in these areas on the whole suggest low parasite prevalence
among chiIdren aged below 14 years. Many areas here experience no malaria risk, for
instance, the central areas of Nairobi, Nyeri and Nakuru.
2.3 Parasitology
Human malaria results from infection with Plasmodium falciparum, Plasmodium vivax,
Plasmodium ovale or Plasmodium malariae. Plasmodium falciparum causes a large
majority of the clinical cases and mortalities (Bozdech et al., 2003). The protozoan
Plasmodium is transmitted to humans by mosquitoes of the genus Anopheles. The
mosquito picks up the parasite during a blood feeding from a person with parasitaernia.
2.3.1 Lifecycle of plasmodium parasite
To understand the challenges biologists face in combating this disease, and the strategies
this parasite.
Plasmodiumparasites are protozoa of the Phylum
Apicomplexa(often
referred to as sporozoans). These arc animal parasites which exist in two hosts, have
sexual and asexual stages, alternate between haploid and diploid phases and must be able
to survive inside both hosts. The life cycle begins with the bite of an infected female
anopheline mosquito. The mosquito takes her blood meal from the vertebrate (in this
case a human) and injects both anticoagulant and haploid sporozoites into the human
blood stream (Yartey, 2006). The sporozoites quickly travel to the hepatocytes (liver
cells), where they mature.
The complex life cycle stages influence malaria vaccine development, each stage has different antigens that lead to protective immunity.
Source of diagram: http:
//
ww
w
.ce1n
e
torg
.
uk
/
med
i
cine
/
malaria.
In the hepatocyte the sporozoites undergo multiple asexual fissions, or schizogony, to
produce thousands of infective, haploid merozoites. TIle rnerozoites are released into the
from this that the immunity provided by the sickle cell trait can be explained. These
parasites have high metabolic demands and cannot survive in the compromised red blood
cells of a human with sub-optimal oxygen carrying-capacity. At this point, the patient is
still in the prepatent period and does not exhibit any clinical symptoms(Kyes et al.,
200 I).
Inside the erythrocyte, the rnerozoites again begin to replicate and divide asexually.
Each merozoite gives rise to 6-32 daughter merozoites (Kyes et al., 200 I)) during 24-72
hours, depending on the species. Ultimately the infected erythrocytes lyse and
merozoites are again released into the bloodstream and invade more cells. This cycle
continues until the patient dies or the parasite is slowed by either the host immune
system or chemotherapeutic agents. The destruction of the erythrocyte and release of
merozoi tes corresponds to the hallmark cl inical presentation of the disease, the period ic
fevers.
The other possible life cycle for the merozoites isdifferentiation into macrogarnetocytes
and microgarnetocytes that do not destroy the erythrocyte they inhabit while in the
human host. They are ingested by anopheline mosquitoes and develop into male and
female gametes. Inside the gut of the mosquito the erythrocytes do lyse and the gametes
meet and fuse into diploid zygotes (the ookinete). This is the only diploid stage during
the life time of the Plasmodium parasite. The ookinetes develop into oocysts and
migrate to the salivary gland of the mosquito (Good and Marsh, 2002). The cycle isthus
2.4 Pathogenesis
The pathology of malaria is related to anaemia, cytokine release and in the case of P.
falciparuni, widespread organ damage due to impaired microcirculation. The anaemia
seen in malaria is multifactorial: haernolysis of infected red blood cells, haernolysis of
non-infected red cells(blackwater fever), dyserythropoiesis, splenomegaly and
sequestration, and folate depletion (Kumar and Clark, 2002). In P.falciparum malaria,
red cells containing schizonts adhere to the lining of capillaries in the brain, kidneys, gut,
liver and other organs. By causing mechanical obstruction, schizonts rupture, release
toxins and stimulate further cytokine release.
The classic example of the strong selective pressure malaria puts on the human
population is the high incidence of the potentially fatal sickle cell gene reported in
regions with endemic malaria. People with one allele for sickled blood cells, the sickle
cell trait, have a survival advantage in regions with endemic malaria. They are more
likely to survive an infection by P. falciparum. Therefore, people with the sickle cell
trait are more likely to survive to a reproductive age. However, the offspring of two
people with sickle cell trait have a 25% chance of bearing offspring with sickle cell
anaemia, which is often fatal and greatly reduces a person's expected longevity. The
enormous effects that malaria has on countries where it is endemic explains this
selection.
The virulence patterns of malaria were being documented as early as the 1920s. Malaria,
specifically the fevers induced by infection with Plasmodium, was used at the time as
treatment for syphilis. It was also noted that reproducible virulence patterns were seen
was achieved by infecting previously naive patients (Kyes et al., 200 1). Even through
these most rudimentary types of experiments it was observed that immunity to a certain
strain of Plasmodium was not equivalent to immunity to the disease malaria. More
recently, controlled studies indicate that immunity to severe malaria is acquired more
rapidly than immunity to mild malaria, especially in regions where transmission is high
(Gupta et al., 1999).
2.5 Clinical features
Typical malaria is usually seen in non-immune individuals. This includes children in any
area, adults in hypoendemic areas and any visitors from non-malarious regions (KMOT-I,
2006b). The incubation period is between 10-21 days, but can be longer. The common symptoms are fever, general malaise, headache, muscle pains, joint pains, abdominal
pains, diarrhea, vomiting, irritability and refusal to feed. At first the fever may be
continuous or erratic. The temperature usually reaches 41 degrees celcious, and is
accompanied by rigors and drenching sweats. Malaria caused by P. [alciparum IS
typically more severe than that caused by the other plasmodium species. The vast
majority of deaths are due to P.falciparum. Patients can deteriorate rapidly, and children
can change from reasonable health to coma and death within hours.The clinical course of
malaria may present as uncomplicated or severe.
2.5.1 Uncomplicated malaria
This is usually characterized by fever in the presence of peripheral parasitaemia, Other
features may include chills, profuse sweating, muscle pains, joint pains, abdominal pain,
diarrhea, nausea, vomiting, irritability and refusal to feed. These features may occur
2.5.2 Severe malaria
This is a life-threatening manifestation of malaria and is defined as the detection of
Ffalciparum in the peripheral blood in the presence of any of the following clinical or
laboratory features: Alteration in the level of consciousness(ranging from drowsiness to
deep coma, cerebral malaria (unarousable coma not attributable to any other cause in a
patient with falciparum malaria), prostration (inability to sit upright, stand or walk
without support in a child who normally does so, or inability to drink in children too
young to sit), respiratory distress, multiple generalized convulsions ( 2 or more episodes
within a 24 hour period), pulmonary oedema, circulatory collapse (shock, septicaemia),
abnormal bleeding (Disseminated Intravascular Coagulation), jaundice, haemoglobinuria
(black water fever), acute renal failure - which present as oliguria or anuria, severe
anaemia (Hb <Sgrams per deciliter or haematocrate< IS%), and hypoglycaernia (blood
glucose level < 2.2 mmol/l).
2.6 Parasitological Diagnosis of malaria
The commonly used confirmatory tests to detect the presence of malaria parasites are
microscopy or rapid diagnostic tests (ROTs). Quality assurance of microscopy and ROTs
isvital for the sensitivity and specificity of the results.
2.6.1 Microscopy
Microscopy is the standard method for parasitological diagnosis of malaria. This isdone
by examining a stained thick or thin blood smear for the presence of malaria parasites.
Thick films are recommended for parasite detection and quantification and can be used
to monitor response to treatment. Thin films are recommended for species identification.
2.6.2 Rapid Diagnostic Tests
These tests are immunochrornatographic tests based on the detection of specific parasite
antigen, either parasite lactate dehydrogenase (pLOH) activity or the presence of
Histidine-Rich Protein? (HRP2). Most of the RDT tests available are specific for
Ffalciparum. However, there are a few tests with the ability to differentiate between P.
falciparum and non Pfalciparum (vivax, malariae and ova/e). ROTs are simple to use
and are sensitive in detecting low parasitemia. Use of ROTs is not recommended for
follow-up as 1110stof the tests remain positive for upto two weeks following effective
antimalarial treatment and clearance of parasites. They also can not be used to determine
parasite density.
2.7 Management
Worldwide, great and varied efforts are being made to learn about this disease and to
determine how to manage and control it.The official malaria eradication program, run by the World Health Organization (WHO), was cancelled in the late 1960s because of
growing difficulties, given that the complex and persistent nature of this disease became
increasingly obvious. Management strategies today include the development of vaccines
and chemotherapeutic agents, vector control, insecticides, education, and insecticide
treated bed nets. Resistance to drugs by both the mosquito and the parasite is a growing
obstacle inthe battle against malaria. Combination therapy has been shown to increase
the efficacy of treatment (Toure and Oduola, 2004).
.Currently, management of malaria is based on severity of the illness and the individual's
immune status. Generally, treatment regimen is based on whether the malaria is
malaria in Kenya is artemether-Iumefantrine, currently available as co-formulated tablet
containing 20 mg of Arternether and 120 mg of lumefantrine. This is administered as a 6
-dose regimen given over three days.The recommended medicine of choice for severe
malaria is parenteral quinine, preferably route of administered intravenously. However,
the intrarnascular route can be used as an alternative where intravenous route is not
feasible(KMOH ,2006b).
2.8 Prevention and control
Currently, malaria control programs do not attempt to eliminate malaria totally.
Complete elimination of the parasite (and thus the disease) would constitute eradication
(COC, 2004). While eradication would be more desirable, it's not currently a realistic
goal for most of the countries where malaria is endemic. Certain barriers to effective
malaria control have been identified. These include, drug resistance, insecticide
resistance, inadequate health infrastructure in poor countries, poverty and lack of
education (COC, 2004). An effective vaccine for this disease has not yet been produced.
Controlling malaria has remained aformidable task.
There are several strategies currently used in the prevention and control of malaria.
These include; intermittent preventive treatment in pregnancy, use of insecticide treated
nets, chemoprophylaxis in the non-immune population, community education on
2.8.1 Intermittent preventive treatment inpregnancytfl'Tp)
Pregnant women are usually at a particular risk of malaria infection(Mbonye et al.,
2006). The consequences of malaria in pregnancy include anaemia and febrile illnesses
in the mother, foetal death and low birth weight. Women at their first and second pregnancies are at a greater risk. Pregnant women therefore are advised to take IPTs
during pregnancy. All pregnant women attending health facilities should receive two
doses of IPT starting at quickening time and with a four weeks interval. This is given free in government health facilities. The current recommended medicine for IPT is
Sulphadoxine 500mg Pyrimethamine 25mg given as a dose of three tablets. This
treatment reduces the amount of malaria parasites in the individual to a level that would
not cause the disease. Through IPT the number of still births due to malaria is likely to
reduce. IPT should be given under directly observed therapy (DOT) in an antenatal clinic
and can be given on an empty stomach. This is so to avoid chances that some women
would forget to take if given to go home with the tablets.
2.8.2 Insecticide treated bed nets (ITNs)
Bed nets are encouraged to be used by all and more so to populations living in high
malaria transmission. The nets block contact between people and the mosquito. The
insecticide in the net helps kill and also repel the vector. Treated nets are being provided free in the government hospitals to all pregnant women. it is expected that all pregnant
women and children under five years old should sleep under an ITN. Use of ITN should
be encouraged early and consistently throughout pregnancy and after delivery. By so
doing malaria burden shall be greatly reduced in the vulnerable group, pregnant women
2.8.3 Chemoprophylaxis in the non-immune population
Chemopropylaxis is recommended in various groups of people who are at a high risk of
malaria infection. These include visitors from malaria free countries such as Europe,
patients with sicle cell disease, and patients with tropical splenomegaly syndrome or
hyperimmune malaria splenomegaly. Such people should use appropriate propylaxis to
boost their immunity against malaria. They should also use other barrier methods to
protect themselves against mosquito bites. Early treatment should also be sought incase
such persons fall ill of the disease even if a prophylaxis has been taken.Travelers should
carry a full course of arternether-lumefantrine for use incase they develop a fever and
have no immediate access to health services.
t8.4 Community education 011 behavior change
Health information, education and communication are a critical intervention for behavior
change towards improved health practices. The people should be informed on the
following: to seek prompt treatment for fevers, how to recognize symptoms and signs of
severe disease, that they should adhere to treatment plan, and that they should use the
appropriate prevention measures. Many women in the community are unaware of the
free services offered in government health facilities. Public health campaigns to address
these issues should continuously be done. This way the people are made aware of the
available tools provided to combat malaria.
2.8.5 Vector control
Anopheles gambiae, Anopheles arabiensis and Anopheles funestus transmit 1110Stof
human malaria and are all found in Africa (Besansky, 2004). Anopheles gambiae, the
transmit malaria to humans (Budiansky, 2002). It isthe primary malaria vector; this can
be attributed, in part, to its relatively long life, strong anthropophily and endophily (the
tendency to target humans for blood meal and the tendency to enter and rest inside of
houses, respectively) (Besansky, 2004). Adult mosquitoes normally rest during the day
inside human habitats and emerge to feed at night (Holt and Patrick, 2002). Their larvae
tend to develop in temporary bodies of water, such as those typically found near
agricultural sites or even in flooded hoof prints(Vogel, 2002). All of these characteristics
combine to make P.falciparum asuccessful vector.
That this behavior is remarkable can be highlighted with a comparison of the
entomological inoculation rate (ElR) of infectious mosquitoes in Asia or South America
compared to sub-Saharan Africa. The 'EIR measures how often one person is bitten by
an infectious mosquito. In Asia or South America a person's EIR rarely exceeds 5 bites
per year. In sub-Saharan Africa a person may have an EIR of over 1,000 bites per
year(Greenwood and Mutabingwa, 2002). The authors also report that during a single
night insub-Saharan Africa, hundreds of mosquitoes typically collect in a room occupied
by humans; 1-5% of these are infectious.
Some disease control strategies deal with these anopheline mosquitoes rather than the
parasite. One strategy for attacking mosquitoes is to develop more effective insecticides.
The main obstacles to this line of attack are growing insecticide resistance and
environmental concerns. The publication of the Anophels gambiaegexvsttv: (Holt and
Patrick, 2002) should help to locate genes involved in resistance and to design chemicals
for attacking new targets in the mosquito. The failure of the WHO's malaria eradication
program was, to a significant degree, due to increasing resistance to DDT and the fact
The current, most widely used, technique for vector control is bed nets treated with the
insecticide pyrethroid. However, it is only amatter of time before pyrethroid, like DOT,
loses its efficacy. Genomics may prove key in the development of new insecticides and
may also improve the longevity of available insecticides (Hemingway et al., 2002).
The viability of introducing genetically modified mosquitoes, which are either unable to
transmit malaria to humans or are sterile, is also being investigated. The completed
genome of Anopheles gambiae has encouraged comparative studies between these
mosquitoes and other arthropods and model organisms such as Drosophilia
melanogaster. These studies may provide clues to account for their great effectiveness
as aPlasmodium vector and could prove to be an effective tool for disease control. Ito et
al., (2002)reported the creation of a stable strain of transgenic mosquitoes that were
unable to transmit Plasmodium under laboratory conditions. Using bacteriophages they
identified a peptide that blocks the parasite from crossing the epethelia of the mosquito.
During a successful life cycle ofa Plasmodium parasite they must cross the epethilium of
both the midgut and the salivary glands. Attaching units of this peptide to a promoter
activated by a blood meal, they were able to inhibit the development of the majority of
parasites. This laboratory success is great but there remain many challenges before
genetically modified mosquitoes could be considered a viable method for malaria
control.
Other methods used to control the vector include indoor residual spraying and selective
larviciding in specific sites, screening of house inlets with mesh wire to reduce entry of
CHAPTER THREE:MATERIALS
AND MET
H
OD
S
3.1 Research Design
The research design used in this study was a descriptive survey. The study was aimed at
collecting information from pregnant mothers in Machakos Central Division on their
perceptions and practices regarding malaria control. The tools employed in gathering
information were an in depth researcher administered questionnaire (interview guide)
and a Focus group discussions (FGDs) guide.
3.2Study Area
The study area was Machakos Central Division, Machakos District in Eastern Province
of Kenya (Appendix V).The research was carried out atMachakosGeneral Hospital.The
area is south east of the capital city of Nairobi, approximately 68 kilornetres away. The
area is characterized by hills on its north, east and south eastern side. These hills are
Mua, Kyeveti and Kiirna Kimwe respectively. The southern side and the western side are
the plains of Konza and Kaviti. The area experiences seasonal rainfall. Short rains occur
between November and December while the long rains occur between March and May.
The area is generally warm with mean temperatures ranging between 22 - 30 decrees
celcious. Machakos Central Division has an estimated population of 160,254 residents as
at end of year 20 IO. Estimated number of women of child bearing age is 54,330 (KDHS
2009).
3.3 Study population
These were pregnant women visiting the health facility's antenatal care clinic. They were
selected randomly.Those included in the study were residents of Machakos Central
years were excluded from the study. All pregnant women from within this division and
fall in the reproductive age were subjects to this study.
3.4 Sample size determination
Purposive sampling technique wasin selecting study subject. Pregnant women 11'0111 within the division attending antenatal care or otherwise at the health facilities were considered in sample selection. Machakos Central Division has an estimated population
of 160,254 residents as at end of year 2010. Estimated number of women of child
bearing age is 54,330 (KDI-IS 2009). (Fisher et 01., 1998) formula was used to determine
the sample size. 11
=
(Z2)(pq) / (d2)Where:
n= the desired sample size (if the target population ismore than 10,000) z =the standard normal dev iate at the requ ired confidence level (1.96)
p = the proportion in the target population estimated to have the characteristic being
measured q = I-p
d =the level of statistical significance set at 0.05
Note:ln this study there isno estimate of the proportion in the target population assumed
to have the characteristic of interest i.e. perceptions and practices on malaria. Therefore 50% was used as recommended by (Fisher e/ 01., 1998).
Requiring accuracy at 0.05 level, then the sample size thus was:
3.5 Study Variables
The independent variables for this study were: education level, occupation, presence of a
health facility, pregnancy, age of child, knowledge of signs and symptoms, belief that
malaria is treatable and improved housing.The dependent variables were health seeking
behaviors and malaria control practices. These included the following: visiting a health
facility, possession of ITN, using ITN, using mosquito coils, repellants and sprays,
draining of swamps and closing of windows in the evening.
3.6 Data collection procedures
To obtain data, a research instrument wasdeveloped, pre-tested and used. For this
purpose a researcher administered questionnaire (interview schedulejwasused. The
structured interview guide consisted of both open-ended and closed-ended questions. In
addition three Focus Group Discussions (FGDs) were conducted. The FGDs consisted of
8 members each: Adolescent pregnant women aged between 14 and 19 years, pregnant
women with tertiary level of education aged between 20 and 49 years, and pregnant
women with no tertiary level of education also aged between 20 and 49 years.
Discussions and interviews focused on four thematic areas; perception of disease,
awareness of disease, control methods and constraints or difficulties faced by women in
malarial control.
3.7 Ethical considerations
Research begun after the relevant authorities issued clearance: Kenyatta University
graduate school, Ministry of Higher Education, Science and technology and Ministry of
Health permits. Participants in this participated voluntarily and on request. Informed
to withdraw from the research at any stage without victimization whatsoever. Ail information given was held in confidence and the study subjects were made aware of
this, Research findings will be made available to the relevant authorities,
3.8 Data management, analysis and presentation.
The data was double entered in Microsoft Excel data sheets, cross checked and
transferred, and analyzed using SPSS for Windows version 11,5 (SPSS, Atlanta, GA,
USA), Descriptive statistics were carried out to measure relative frequencies,
percentages, averages, and relative frequencies of the variables, Cross tabulations of
variables were done, and chi-square test was used to determine the statistical significance
or differences of relative frequencies.Results were presented in frequency tables, bar
4.1 Results
CIlAYfER FOUR:RESULTS AND DISCUSSION
4.1.1 Introduction
This chapter presents both qualitative and quantitative findings of the study. The section
covered the following findings: Socio-demographic and Socio-economic factors,
perceptions on Malaria illness, awareness,actions/practiceslhealth seeking behavior and
resource availability. The data is presented using frequency tables, charts and graphs.
4.1.2 Socio-demographic and Socio-economic factors
4.1.2.1 Age of respondents
Seven percent of the respondents were in the age between 14 and 19 years. Thirty seven
percent were in the age of between 20 and 25 years. Twenty sevenpercent were :in the
age ranging from 26 to31 years. Twenty one percent were between 32 and 37 years. Five
percent were between 38 and 43 years. The rest,three percent were between 44 and 49
years (FigA.l). Modal age was 20 to 25 years while mean age stood at 28 years.
40
--35
30
IV b.O 25 CU
-
=
20~ 15
~ 10
g.
.
5o
14-19 20-25 26-31 32-37
Age (years)
44-49 38-43
4.1.2.2 Marital Status
Seventy four percent of respondents were married, 24% percent were not married, 1%
widowed and 1% was divorced or separated.
l
Widowed Divon:ed/sep<mlted
r }~~ 1%
. ",
Key
-Married
•••Not married
Widowed
'"Divorced/separate d
Figure
4
.
2Distribution of respondents by marital status
4.1.2.3 Number of Children
Ninety six percent of the respondents had 1-5 children, 3% had 6-10 children and 1%
Table 4.1Distribution of respondents by number of children
Number of children Frequency Percent
1-5 Children 372
96
6-10 Children 8 3
Above 10 Children 4
1
Total 384 100
4.1.2.4 Level of education
Forty four percent of the respondents had attained primary level of education, 33% had
secondary education, and 22% had college/university education (Figure 4.3).
,---
--I No formal
I
~educationI
C"
.
1%I
L
_
Key
•••No formal education
.".Primary
Secondary
Secondary 33%
.•Tertiary
I
Figure 4.3Distribution of respondents by level of education
In
this study education level was observed to be associated with perception and practicesof malaria control OC=8.51, df-=l, P=O.004). Secondary and tertiary education levels
4.1.2.5 Religion
Seventy percent of the respondents were Protestants while 30% was Roman
Catholic(Figure 4.4).
80 ~
t::: 70
<l.> '0
t::: 60
o
~ 50
<l.>
.:: 40
o
<l.> 30 OJ:)
J3 20
t::: ~ 10 ~
<l.>
0.. 0
Roman Catholic Protestant
Religion
Figure 4.4Distribution of respondents by religion
4.1.2.6 Place of residence and housing status
Thirty live percent of respondents lived in urban areas, 65% lived in rural area (Figure
4.5). Seventy four percent lived in houses made of modern iron sheetslcorrugated, 24%
r
---
-
-Key
Ii!Urban
• Rural
Figure 4.5Distribution of respondents by place of residence
, c
;
~tXs
thatched285
mIron sheets/corrugated
roof
iii!Stone built. tiled roof
100
o
200 300Number
of respondents
L. _
----
---_._--Figure4.6 Distribution of respondents by house status
4.1.2.7 Occu pation
According to occupation, thirty eight percent of the respondents were housewives, 24%
were business ladies, 18% were students, II % were civil servants and 9% were peasant
farmers (Table 4.2).
Table 4.2Distribution of respondents by occupation
Occupation Frequency Percentage
House wife 146 38
Business 92 24
Student 69 18
Civil servant 42 11
Peasant farmers
3
S
9
-Total 384 100
Occupation was observed to be associated with perception and malaria control
practices (X2=4.029, df=I, P<0.04S). It was observed that all employed women
had an ITN and sought medical care unlike those not employed.
4.1.3 Perceptions about Malaria
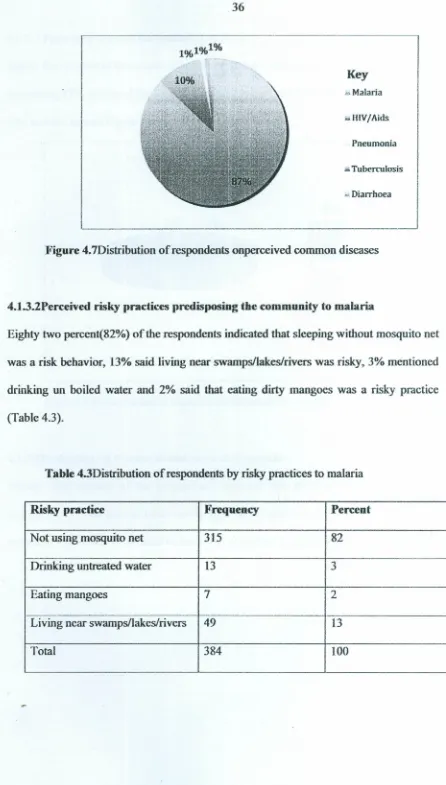
4.1.3.1 Perceived common diseases
Eighty seven percent of the respondents said that malaria was common, 10% mentioned
Key
",Malaria
ii.iHlV/Aids
Pneumonia
••Tuberculosis
••Diarrhoea
Figure 4.7Distribution of respondents onperceived common diseases
4.1.3.2Perceived risky practices predisposing the community to malaria
Eighty two percent(82%) of the respondents indicated that sleeping without mosquito net
was a risk behavior, 13% said living near swamps/lakes/rivers was risky, 3% mentioned
drinking un boiled water and 2% said that eating dirty mangoes was a risky practice
(Table 43).
Table 4.3Distribution of respondents by risky practices to malaria
Risky practice Frequency Percent
Not using mosquito net 315 82
Drinking untreated water 13 3
Eating mangoes 7 2
Living near swamps/lakes/rivers 49 13
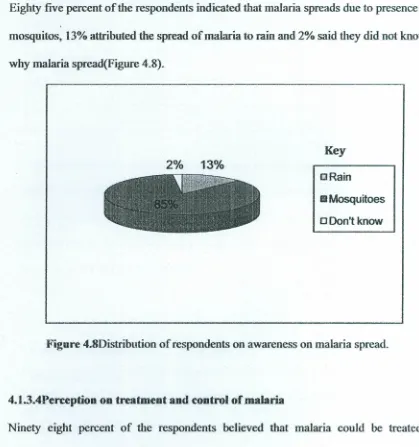
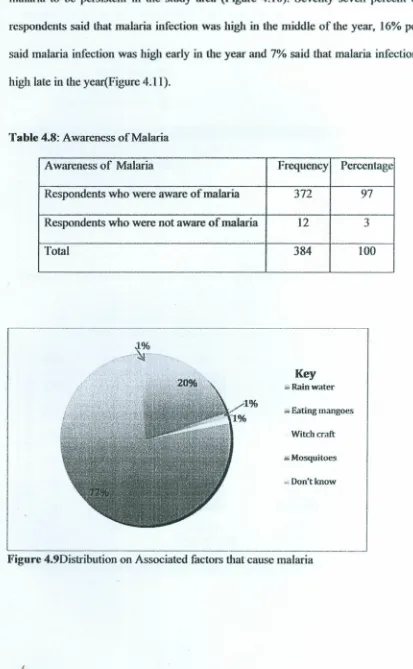
4.1
.
3
.
3
Perceived reasonsfor
spreadof
malaria.Eighty five percent of the respondents indicated that malaria spreads due to presence of
mosquitos, 13% attributed the spread
ofmalaria
to rain and 2% said they did not knowwhy malaria spread(Figure 4.8).
cRain
61Mosquitoes
ODon'tknow Key
2%
13%
Figure 4.8Distribution of respondents on awareness on malaria spread.
4.1.3
.
4Perception on treatment and control of mala ria
Ninety eight percent of the respondents believed that malaria could be treated or
controlled,
t%
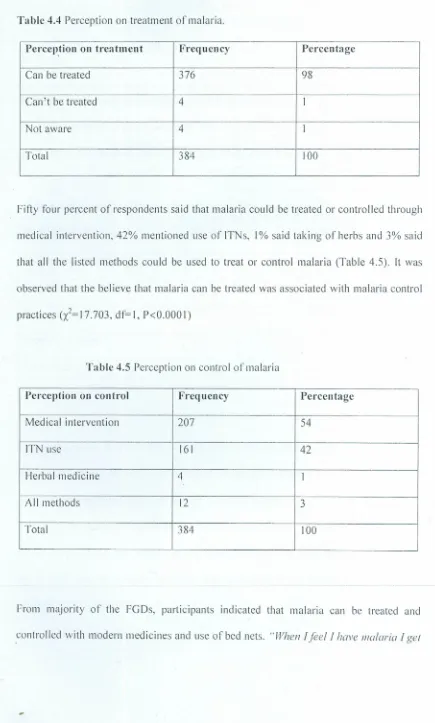
said malaria could not be treated or controlled and 1% said that they didTable 4.4 Perception on treatment of malaria.
Perception on treatment Frequency Percentage
Can be treated 376 98
'--.
Can't be treated 4 I
Not aware 4 I
Total 384 lOa
Fifty four percent of respondents said that malaria could be treated or controlled through
medical intervention, 42% mentioned use of ITNs, I% said taking of herbs and 3% said
that all the listed methods could be used to treat or control malaria (Table 4.5). It was
observed that the believe that malaria can be treated was associated with malaria control
practices Ci=17.703, df=l, P<O.OOOI)
Table 4.5 Perception on control of malaria
Perception on control Freq uency Percentage
Medical intervention 207 54
"
ITN use 161 42
f--.
Herbal medicine 4 1
AII methods 12 3
Total 384 lOa
From majority of the FGDs, participants indicated that malaria can be treated and
malaria drugsfrom the pharmacy or go to the hospital and get well. Ialso use mosquito
net 01night while asleep ",a28year old woman said.
4.1.3.5Pcrccption on group that has high risk of malaria
The l11ajority(46%) of the respondents said that pregnant women were the most affected
group, 29% said children, and 22% said all people were at high risk (Table 4.6).
Table 4.6Distributionof respondents by perception on most risky group of people for malaria infection.
Most affected group Frequency Percentage
Children <S years 112 29
Children> or =S years 9 2
Pregnant women 176 46
People >SO years 4 I
All people 83 22%
Total 384 100%
Most respondents in the FGDs indicated that pregnant women and children are more
easiIy attacked by malaria than the rest of the people. "When we are pregnant malaria comes 11I0,;eeasily than when we are not. Have seen many children/all illa/malaria but when they are older they rarely get the disease ",a34year old woman had said.
It was observed that the perception that children under five years and pregnant women
are at high risk of malaria infection was associated with malaria control practices