A Systematic Review of the Role of Pharmacists in Vaccination Services in
Low-and Middle-Income Countries
By
Stephen McMillan
Honors Thesis
UNC Eshelman School of Pharmacy University of North Carolina at Chapel Hill
3/5/2020
Approved:
A Systematic Review of the Role of Pharmacists in Vaccination Services in
Low-and Middle-Income Countries
Tatenda T. Yemeke1, Stephen McMillan1, Sachiko Ozawa1,2*
1 Division of Practice Advancement and Clinical Education, UNC Eshelman School of Pharmacy 2 Department of Maternal and Child Health, UNC Gillings School of Global Public Health,
University of North Carolina at Chapel Hill
*Corresponding Author Sachiko Ozawa
Associate Professor
Practice Advancement and Clinical Education UNC Eshelman School of Pharmacy
University of North Carolina at Chapel Hill CB#7574, Beard Hall 115H, Chapel Hill NC 27599
Tel: 919-966-2626 Fax: 919-843-3861
Keywords: pharmacist, pharmacy, immunizations, vaccine, low-and middle-income country
Acknowledgements: We thank the directors and coordinators of the Research and Scholarship in Pharmacy (RASP) pathway at UNC Eshelman School of Pharmacy for their guidance. We also thank members of the Global Health Economics for Pharmacy team at UNC for their valuable support.
Abstract (300 words)
Background: Pharmacists’ role in vaccination has expanded in some countries with pharmacists
having greater authority to perform various immunization activities, from vaccine storage, vaccine adverse event reporting, vaccination education and advocacy, to vaccine
administration. However, pharmacists’ present involvement in vaccination services is poorly understood across low- and middle-income countries (LMICs).
Objective: To identify and synthesize evidence on pharmacists’ roles in vaccination in LMICs.
Methods: We searched three databases (PubMed, Embase, Scopus) and the gray literature to
identify articles which described pharmacist involvement in vaccination services in LMICs. We abstracted data on reported roles of pharmacists in vaccination, as well as relevant country, vaccines, and populations served.
Results: From the initial 612 records we identified, twenty-five (n=25) studies representing 22
LMICs met our inclusion criteria. The most commonly reported role of pharmacists in vaccination across identified LMICs was vaccine advocacy and education (n=15 countries). Pharmacist administered vaccination and storage of vaccines at pharmacies was reported in 8 countries. An additional 6 countries reported allowing vaccination at community pharmacies by other healthcare professionals. Immunization related training for pharmacists was reported or required in 8 countries. Fewer studies reported that pharmacists have access to patient immunization records in their respective LMICs (n=6 countries) or had reported pharmacist involvement in vaccine adverse event reporting (n=4 countries).
Conclusions: Pharmacists have the potential to play an important role in increasing access to
vaccines and improving coverage, yet evidence of their role in immunization remains limited across LMICs. Greater documentation of pharmacists’ involvement in vaccination services in LMICs is needed to demonstrate the value of successful integration of pharmacists in
Introduction
Immunizations offer some of the safest, most efficient, and cost-effective preventative measures for controlling and eradicating deadly infectious diseases [1]. The World Health Organization (WHO) estimates that vaccinations save the lives of 2-3 million people each year, and increased vaccination coverage could annually prevent an additional 1.5 million premature deaths globally [2]. Yet various barriers and challenges limit vaccination coverage resulting in the frequent occurrence of vaccine preventable diseases [3-5]. For example, the global
vaccination coverage rate of three doses of diphtheria, tetanus and pertussis (DTP) vaccine has stalled at 86%, with many countries still yet to attain global immunization coverage goals set by the Global Vaccine Action Plan of reaching 90% national coverage and 80% district level
coverage [2, 6-8]. Gaps in vaccination coverage are particularly stark across low- and middle-income countries (LMICs) where large variations in coverage are observed [9], leaving some populations behind. It is essential to consider programmatic and policy interventions to improve access to vaccines.
A growing number of middle- and high-income countries have been expanding the role of pharmacists to offer vaccination services, which has resulted in expanded vaccination access and higher vaccination rates [10-15]. For example, pharmacists in the United States (US) are expected to not only supply, dispense, and advocate for vaccination, but they are also expected to administer some vaccinations and manage patients’ vaccination plans [10]. With the backing of the American Pharmacists Association (APhA), over 280,000 pharmacists in the US have been trained on pharmacy-based vaccine delivery [10]. Pharmacist provision of vaccines in the US has led to significant increases in vaccination coverage, especially for adult and influenza vaccines [16-18]. Other countries such as Argentina, Australia, the Philippines, South Africa, and the United Kingdom have also legally authorized vaccination by pharmacists or in pharmacies [10, 19-21]. This trend in expanded pharmacists’ scope of practice demonstrates increased
appreciation of pharmacists’ involvement in healthcare as educators, facilitators, and immunizers.
Globally, the majority of patients first seek care from pharmacies and drug shops, and
Success of pharmacist driven vaccination in some countries suggest that pharmacists can play a greater role in improving vaccination coverage in LMICs. However, evidence of pharmacists’ present involvement in vaccination services in LMICs is uncertain [26-28]. A 2016 global survey of country members of the International Pharmaceutical Federation (FIP) found limited
evidence of pharmacist involvement in vaccination services in LMICs [10]. Reviews and meta-analyses of pharmacist’s roles in vaccination have not included studies from LMICs [14, 16, 29-31]. In the absence of prior reviews, we conducted a systematic review of published literature describing roles of pharmacists in offering vaccination services across LMICs. A comprehensive review of the literature on pharmacists’ involvement in vaccination services across LMICs can clarify pharmacists’ current roles and help inform potential regulatory and policy changes for pharmacists’ scope of practice in vaccination services in efforts to improve immunization coverage.
Methods
We searched three databases (PubMed, Embase, and Scopus) on January 13, 2020 to identify papers that describe the role of pharmacists in vaccination in LMICs. We used variations of the following search terms: (“pharmac*” or “chemist*”) and (“immuniz∗,” or “vaccin∗,”) and a list of LMIC terms. LMIC terms included the names of every low- or middle-income country as per World Bank country income classification [32] and other country grouping terms such as “developing country” or “low income country” (Appendix 1). We also conducted a Google search for the gray literature using the same pharmacist vaccination and country grouping terms, and reviewed references of pertinent review articles.
We screened titles and abstracts to identify studies that described involvement by pharmacists in vaccination in LMICs.We included studies that mentioned pharmacists or chemists,
immunizations or vaccinations, and took place in a LMIC. We excluded papers that did not include pharmacists, vaccination, or took place in high-income countries. We also excluded studies that were not published in English and conference posters and proceedings that were not subsequently published. Those articles marked for inclusion, or whose titles and abstracts were not sufficiently detailed to determine relevance, were then reviewed using the full text. Two authors (SM and TY) independently screened titles and abstracts and assessed full texts for eligibility. The full study team reached consensus for inclusion of discrepant studies, based on inclusion and exclusion criteria which were decided a priori.
This systematic review was registered in the PROSPERO database and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines [33].
Results
Initial database searches yielded 612 records, of which 402 were unique after elimination of duplicates across databases. Initial screening of these titles and abstracts resulted in 128 studies whose full-text was assessed for eligibility. Based on the full texts, we identified 25 studies [21, 23, 34-53] which reported pharmacists’ involvement in offering vaccination services in LMICs. Figure 1summarizes our search process.
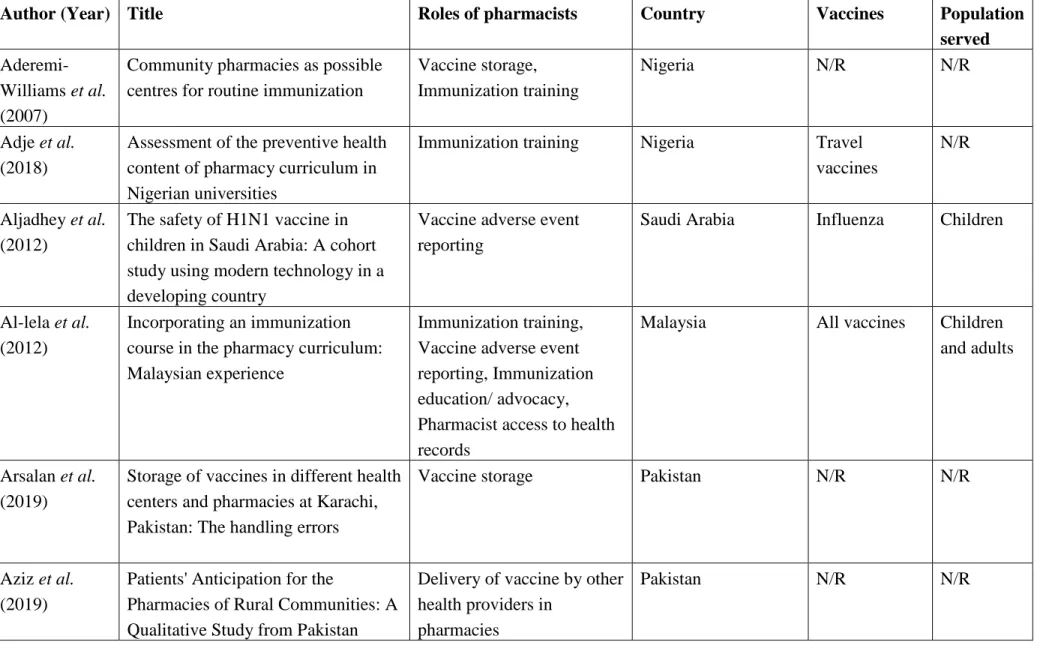
The 25 studies reported pharmacist involvement in vaccination services across 22 LMICs: Argentina, Bolivia, Brazil, Costa Rica, China, Democratic Republic of Congo, Ethiopia, India, Iraq, Jordan, Lebanon, Malaysia, Nigeria, Pakistan, Philippines, Russia, Saudi Arabia, Senegal, South Africa, Turkey, Uganda, and Vietnam. There were 6 papers from South Africa, 4 each from Nigeria and Pakistan, 3 from Malaysia, 2 each from Brazil, Lebanon and Turkey, and one study each from the remaining countries. Thirteen studies did not specify a vaccine, while 6 studies involved all vaccines, 2 studies focused on the influenza vaccine, and one study each centered on Haemophilus influenzae type b (Hib), Hepatitis B, Human Papillomavirus (HPV) and travel vaccines. Of the 11 studies that specified the target population served by pharmacists offering vaccination services, 5 studies discussed services across all ages, 3 studies focused on children, 2studies focused on adults, and one study focused on adult injection drug users. Based on the 25 included studies, Table 1 summarizes the reported roles of pharmacists in vaccination services, alongside the country setting, type of vaccines, and the populations served.
Across the 22 countries which reported some pharmacists’ roles in vaccination services, the extent of their roles varied comparatively across countries (Table 2). For example, in Malaysia, Nigeria, and Turkey, pharmacists reported vaccine adverse events as part of ongoing national pharmacovigilance programs [37, 46, 47], whereas pharmacists in a study in Saudi Arabia were involved in vaccine adverse event reporting only as part of a safety trial of the H1N1 vaccine [36]. Some studies reported that pharmacist administration of vaccines was limited to certain classes of vaccines such as travel vaccines [21], or required regulatory ordinance permission [41].
Discussion
Evidence of the roles of pharmacists in vaccination services remains limited across LMICs, despite pharmacists’ potential to play a valuable role in increasing access to vaccines and improving immunization coverage. The small number of studies identified and the limited reported role of pharmacists highlights opportunities to test interventions to integrate pharmacists in immunization programs in LMICs and improve documentation of pharmacists’ involvement in vaccination services. Greater evidence is needed to assess the value of
pharmacists’ expanded scope of practice in offering vaccination services in LMICs.
While some studies described expanding immunization training in pharmacists’ curriculums, greater efforts are needed to extend pharmacists’ immunization training across all LMICs to ensure pharmacists can educate, advocate for, and remind people who are due for vaccination. Training is one of the first steps needed for pharmacists’ increased involvement in vaccination services, where pharmacists can play an important role in imparting knowledge through vaccine advocacy and patient education. Extended immunization training in pharmacists’ curriculum was one of the initial changes made in countries where pharmacists have now been extended authority to administer vaccines [12].
Our finding that pharmacists in identified studies were commonly involved in the storage of vaccines suggests that supporting infrastructure such as cold-chain equipment exist at
pharmacies in reported LMICs to support vaccination services. This makes it potentially feasible to integrate community pharmacies as vaccination locations in immunization programs in respective countries. As pharmacies are located in communities and are more accessible to the population, integrating community pharmacies into immunization programs may reduce geographic barriers due to distance or terrain for people to access vaccines [5]. Community pharmacists may also remove other barriers to vaccination as a convenient and trusted healthcare provider [16, 17]. Pharmacists’ most frequently reported role in vaccine advocacy and education provides a further platform to reduce barriers to vaccination, reduce vaccine hesitancy and improve vaccine acceptance [54, 55]. Some countries have reported authorizing physicians or nurses to offer vaccinations at community pharmacies as an initial step to
In addition, studies reported pharmacist reporting of vaccine adverse events and pharmacist access to patient immunization records. Vaccine adverse event reporting systems are essential to ensure vaccine safety and surveillance, and maintain people’s confidence in vaccines. Access to immunization records allow pharmacists to identify missed vaccinations, offer reminders to patients, and update immunization records to improve reporting of immunization coverage. Further integration of such systems and procedures across healthcare providers are needed for pharmacists to be incorporated in the overall health system to present a united front in offering vaccination services in LMICs.
Evidence from middle- and high-income countries has shown that pharmacists and community pharmacies can be successfully integrated in immunization programs and improve vaccination rates, through educator/facilitator roles and through administration of vaccines [16, 31]. Studies have consistently found significant gains in vaccination coverage when pharmacists were granted greater authorization to administer vaccinations [57-59]. Pharmacists have also increased access to vaccinations by making vaccines more accessible [12, 17, 30, 31]. Moreover, pharmacists have increasingly become integrated in greater patient management and public heath roles across LMICs [26, 27]. Pharmacist-provided services could improve clinical outcomes through management of high blood pressure, cholesterol and glucose levels, and may improve patients’ quality of life or reduce the need for hospitalizations [26]. Benefits of pharmacists’ involvement in vaccination services need to be evaluated more widely across LMICs.
Our study findings from the literature on the limited roles of pharmacists in vaccine
administration is consistent with findings from the 2016 global survey of member organizations by FIP, which found that pharmacists were involved in vaccine administration in 3 out of the 18 LMICs responding to the survey [10]. Similar to our findings from the literature, the FIP survey found limited evidence of mandatory immunization training for pharmacists (6 out of 18 LMICs) and of pharmacist access to immunization records (5 out of 18 LMICs) [10]. The majority of LMICs (14 out of 18 LMICs) in the FIP survey reported pharmacist involvement in vaccine advocacy [10].
We note some limitations to our study findings. We are not able to discuss the role of
pharmacists in vaccination services in countries where we could not find pertinent literature, even if there may be relevant activities taking place. Moreover, the paucity of published literature describing pharmacists’ roles in vaccination services does not necessarily reflect the state of the practice in countries. In some identified studies, vaccination was not the primary study topic, which limited the depth of descriptions of pharmacist roles in vaccination. Our search strategy, while systematic, was limited to the databases and search terms we used and were focused on studies published in English. Further studies including in-country surveys of stakeholders are needed to characterize in greater depth pharmacist involvement in
Conclusions
There is a paucity of studies describing the role of pharmacists offering vaccination services across LMICs. Findings from the current literature highlight opportunities to test the value of interventions to integrate pharmacists in immunization programs in LMICs and improve documentation of pharmacists’ involvement in vaccination services.
Efforts to improve vaccination access in LMICs occur in the context of stagnating immunization coverage and a global health worker shortage, currently estimated around 7.2 million
References
[1] Ozawa S, Clark S, Portnoy A, Grewal S, Stack ML, Sinha A, et al. Estimated economic impact of vaccinations in 73 low- and middle-income countries, 2001-2020. Bulletin of the World Health Organization. 2017;95:629-38.
[2] World Health Organization. (2017). Immunization coverage. Retrieved from
http://www.who.int/mediacentre/factsheets/fs378/en/
[3] Phillips DE, Dieleman JL, Lim SS, Shearer J. Determinants of effective vaccine coverage in low and middle-income countries: a systematic review and interpretive synthesis. BMC health services research. 2017;17:681-.
[4] Esposito S, Principi N, Cornaglia G. Barriers to the vaccination of children and adolescents and possible solutions. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2014;20 Suppl 5:25-31. [5] Ozawa S, Yemeke TT, Evans DR, Pallas SE, Wallace AS, Lee BY. Defining hard-to-reach populations for vaccination. Vaccine. 2019;37:5525-34.
[6] World Health Organization. Global routine vaccination coverage, 2012. Releve epidemiologique hebdomadaire. 2013;88:482-6.
[7] Kamara L, Lydon P, Bilous J, Vandelaer J, Eggers R, Gacic-Dobo M, et al. Global Immunization Vision and Strategy (GIVS): a mid-term analysis of progress in 50 countries. Health policy and planning. 2013;28:11-9.
[8] World Health Organization. Meeting of the Strategic Advisory Group of Experts on immunization, April 2017 - conclusions and recommendations. Releve epidemiologique hebdomadaire. 2017;92:301-20.
[9] Restrepo-Mendez MC, Barros AJ, Wong KL, Johnson HL, Pariyo G, Franca GV, et al. Inequalities in full immunization coverage: trends in low- and middle-income countries. Bulletin of the World Health Organization. 2016;94:794-805b.
[10] International Pharmaceutical Federation (FIP). An Overview of Current Pharmacy Impact on Immunisation - A Global Report. 2016. Place. Published.
https://www.fip.org/files/fip/publications/FIP_report_on_Immunisation.pdf
[11] Chun GJ, Sautter JM, Patterson BJ, McGhan WF. Diffusion of Pharmacy-Based Influenza Vaccination Over Time in the United States. American Journal of Public Health. 2016;106:1099-100.
[12] Bach AT, Goad JA. The role of community pharmacy-based vaccination in the USA: current practice and future directions. Integrated pharmacy research & practice. 2015;4:67-77.
[13] Leuthold C, Bugnon O, Berger J. The Role of Community Pharmacists in Travel Health and Vaccination in Switzerland. Pharmacy (Basel, Switzerland). 2018;6:125.
[14] Isenor JE, Slayter KL, Halperin DM, McNeil SA, Bowles SK. Pharmacists' immunization experiences, beliefs, and attitudes in New Brunswick, Canada. Pharmacy practice. 2018;16:1310- [15] Isenor JE, O’Reilly BA, Bowles SK. Evaluation of the impact of immunization policies, including the addition of pharmacists as immunizers, on influenza vaccination coverage in Nova Scotia, Canada: 2006 to 2016. BMC Public Health. 2018;18:787.
[17] AJMC Perspectives. The Essential Role of Community Pharmacies in Expanding Access to
Vaccines. 2018. Place. Published.
https://ajmc.s3.amazonaws.com/_media/_pdf/A848_Vaccines_Article03.pdf
[18] Kirkdale CL, Nebout G, Megerlin F, Thornley T. Benefits of pharmacist-led flu vaccination services in community pharmacy. Annales pharmaceutiques francaises. 2017;75:3-8.
[19] Hattingh HL, Sim TF, Parsons R, Czarniak P, Vickery A, Ayadurai S. Evaluation of the first pharmacist-administered vaccinations in Western Australia: a mixed-methods study. BMJ Open. 2016;6:e011948.
[20] Perman S, Kwiatkowska RM, Gjini A. Do community pharmacists add value to routine immunization programmes? A review of the evidence from the UK. Journal of public health (Oxford, England). 2018;40:e510-e20.
[21] Baker L. The Role of Pharmacists in Travel Medicine in South Africa. Pharmacy (Basel, Switzerland). 2018;6:68.
[22] Goodman C, Miller R. Performance of retail pharmacies in low- and middle-income Asian settings: a systematic review. Health policy and planning. 2016;31:940-53.
[23] Mayora C, Kitutu FE, Kandala N-B, Ekirapa-Kiracho E, Peterson SS, Wamani H. Private retail drug shops: what they are, how they operate, and implications for health care delivery in rural Uganda. BMC Health Services Research. 2018;18:532.
[24] Gulland A. Shortage of health workers is set to double, says WHO. BMJ : British Medical Journal. 2013;347:f6804.
[25] Liu JX, Goryakin Y, Maeda A, Bruckner T, Scheffler R. Global Health Workforce Labor Market Projections for 2030. Human Resources for Health. 2017;15:11.
[26] Pande S, Hiller JE, Nkansah N, Bero L. The effect of pharmacist-provided non-dispensing services on patient outcomes, health service utilisation and costs in low- and middle-income countries. The Cochrane database of systematic reviews. 2013:Cd010398.
[27] Smith F. Private local pharmacies in low- and middle-income countries: a review of interventions to enhance their role in public health. Tropical medicine & international health : TM & IH. 2009;14:362-72.
[28] Kaddar M, Levin A. Role of the private sector in the provision of immunization services in low- and middle-income countries†. Health policy and planning. 2011;26:i4-i12.
[29] Isenor JE, Bowles SK. Evidence for pharmacist vaccination. Canadian Pharmacists Journal / Revue des Pharmaciens du Canada. 2018;151:301-4.
[30] Baroy J, Chung D, Frisch R, Apgar D, Slack MK. The impact of pharmacist immunization programs on adult immunization rates: A systematic review and meta-analysis. Journal of the American Pharmacists Association. 2016;56:418-26.
[31] Isenor JE, Edwards NT, Alia TA, Slayter KL, MacDougall DM, McNeil SA, et al. Impact of pharmacists as immunizers on vaccination rates: A systematic review and meta-analysis. Vaccine. 2016;34:5708-23.
[32] The World Bank. (2017). World Bank Country and Lending Groups. Retrieved from
https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
[33] Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Medicine. 2009;6:e1000097.
[35] Adje D, Williams F, Arute J, Oparah A, Dangiwa D, Olele H. Assessment of the preventive health content of pharmacy curriculum in Nigerian universities. 2018. 2018;18.
[36] Aljadhey H, Alyabsi M, Alrwisan A, Alqahtani N, Almutairi R, Al Tawil E, et al. The safety of H1N1 vaccine in children in Saudi Arabia: a cohort study using modern technology in a developing country. Drug safety. 2012;35:555-61.
[37] Al-lela OQB, Bahari MB, Elkalmi RM, Jawad Awadh AI. Incorporating an immunization course in the pharmacy curriculum: Malaysian experience. American journal of pharmaceutical education. 2012;76:206-.
[38] Butt ZA, Gilani AH, Nanan D, Sheikh AL, White F. Quality of pharmacies in Pakistan: a cross-sectional survey. International journal for quality in health care : journal of the International Society for Quality in Health Care. 2005;17:307-13.
[39] El Khoury G, Salameh P. Influenza Vaccination: A Cross-Sectional Survey of Knowledge, Attitude and Practices among the Lebanese Adult Population. International journal of environmental research and public health. 2015;12:15486-97.
[40] Gul H, Omurtag G, Clark PM, Tozan A, Ozel S. Nonprescription medication purchases and the role of pharmacists as healthcare workers in self-medication in Istanbul. Medical science monitor : international medical journal of experimental and clinical research. 2007;13:Ph9-14. [41] Hammett TM, Phan S, Gaggin J, Case P, Zaller N, Lutnick A, et al. Pharmacies as providers of expanded health services for people who inject drugs: a review of laws, policies, and barriers in six countries. BMC Health Services Research. 2014;14:261.
[42] Iqbal MS, Iqbal MZ, Bahari MB. Effectiveness of pharmacists-led provider-focused interventions to improve HPV vaccination rates in adults in Malaysia. Value in Health. 2016;19:A424.
[43] Melo AC, Galato D, Maniero HK, Frade JCQP, Palhano TJ, da Silva WB, et al. Pharmacy in Brazil: Progress and Challenges on the Road to Expanding Clinical Practice. The Canadian journal of hospital pharmacy. 2017;70:381-90.
[44] Meyer H, Khosa LA, Nhira S, Chiloane L, Sibanda M, Schönfeldt M, et al. Childhood vaccination and the role of the pharmacist. S Afr Pharm J. 2018;85:26-39.
[45] Ngcobo NJ, Kamupira MG. The status of vaccine availability and associated factors in Tshwane government clinics. South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde. 2017;107:535-8.
[46] Obebi Cliff-Eribo K, Sammons H, Star K, Ralph Edwards I, Osakwe A, Choonara I. Adverse drug reactions in Nigerian children: a retrospective review of reports submitted to the Nigerian Pharmacovigilance Centre from 2005 to 2012. Paediatrics and international child health. 2016;36:300-4.
[47] Ozcan G, Aykac E, Kasap Y, Nemutlu NT, Sen E, Aydinkarahaliloglu ND. Adverse Drug Reaction Reporting Pattern in Turkey: Analysis of the National Database in the Context of the First Pharmacovigilance Legislation. Drugs - real world outcomes. 2016;3:33-43.
[48] Shah SSAM, Naqvi BS, Fatima M, Khaliq A, Sheikh AL, Baqar M. Quality of drug stores: Storage practices & Regulatory compliance in Karachi, Pakistan. Pakistan journal of medical sciences. 2016;32:1071-6.
[51] Buicu F. Vaccination in community pharmacies – A global review and the Romanian opportunity. Farmacia. 2018;66.
[52] Beshir SA, Bt Hamzah NH. Health promotion and health education: Perception, barriers and standard of practices of community pharmacists. International Journal of Health Promotion and Education. 2014;52:174-80.
[53] Ongpoy R. Proposed Adult Immunization Training Program For Filipino Pharmacists. International Journal of Scientific & Technology Research. 2019;8:247-50.
[54] The Lancet C, Adolescent H. Vaccine hesitancy: a generation at risk. The Lancet Child & Adolescent Health. 2019;3:281.
[55] MacDonald NE. Vaccine hesitancy: Definition, scope and determinants. Vaccine. 2015;33:4161-4.
[56] Aziz MM, Jiang M, Masood I, Chang J, Shan Z, Raza MA, et al. Patients' Anticipation for the Pharmacies of Rural Communities: A Qualitative Study from Pakistan. International journal of environmental research and public health. 2019;16.
[57] Steyer TE, Ragucci KR, Pearson WS, Mainous AG, 3rd. The role of pharmacists in the delivery of influenza vaccinations. Vaccine. 2004;22:1001-6.
[58] Taitel MS, Fensterheim LE, Cannon AE, Cohen ES. Improving pneumococcal and herpes zoster vaccination uptake: expanding pharmacist privileges. The American journal of managed care. 2013;19:e309-13.
[59] Tak CR, Gunning K, Kim J, Sherwin CM, Ruble JH, Nickman NA, et al. The effect of a prescription order requirement for pharmacist-administered vaccination on herpes zoster vaccination rates. Vaccine. 2019;37:631-6.
Figure 1. Literature search flow diagram
Records identified via PubMed
(n = 127)
Records identified via Scopus
(n = 307)
Records identified via Embase
(n = 177)
Records after Duplicates Removed
(n = 402)
Title and abstract screening
(n = 402)
Records Excluded (n = 274) Full-text articles
assessed for eligibility
(n = 128)
n = 336
Full-text articles excluded due to: No vaccines (n = 20) No Pharmacist involved (n = 42)
Not LMIC (n = 29) Full text inaccessible (n = 2)
Not in English (n = 2) Conference paper (n = 8) Studies included
for analysis
(n = 25)
Additional gray literature
Table 1. Summary of pharmacists’ roles in vaccination services in the literature
Author (Year) Title Roles of pharmacists Country Vaccines Population
served
Aderemi-Williams et al.
(2007)
Community pharmacies as possible centres for routine immunization
Vaccine storage, Immunization training
Nigeria N/R N/R
Adje et al. (2018)
Assessment of the preventive health content of pharmacy curriculum in Nigerian universities
Immunization training Nigeria Travel
vaccines
N/R
Aljadhey et al.
(2012)
The safety of H1N1 vaccine in children in Saudi Arabia: A cohort study using modern technology in a developing country
Vaccine adverse event reporting
Saudi Arabia Influenza Children
Al-lela et al.
(2012)
Incorporating an immunization course in the pharmacy curriculum: Malaysian experience
Immunization training, Vaccine adverse event reporting, Immunization education/ advocacy, Pharmacist access to health records
Malaysia All vaccines Children and adults
Arsalan et al.
(2019)
Storage of vaccines in different health centers and pharmacies at Karachi, Pakistan: The handling errors
Vaccine storage Pakistan N/R N/R
Aziz et al.
(2019)
Patients' Anticipation for the
Pharmacies of Rural Communities: A Qualitative Study from Pakistan
Delivery of vaccine by other health providers in
pharmacies
Baker (2018) The Role of Pharmacists in Travel Medicine in South Africa
Vaccine administration, Immunization
education/advocacy, Vaccine storage
South Africa All vaccines Children and adults
Beshir et al.
(2014)
Health promotion and health education: Perception, barriers and standard of practices of community pharmacists
Immunization education/advocacy
Malaysia N/R N/R
Buicu et al.
(2018)
Vaccination in community
pharmacies – A global review and the Romanian opportunity
Immunization training, Vaccine administration, Vaccine storage
South Africa All vaccines Children and adults Butt et al.
(2005)
Quality of pharmacies in Pakistan: a cross-sectional survey
Vaccine storage Pakistan N/R N/R
El Khoury et al. (2015)
Influenza Vaccination: A Cross-Sectional Survey of Knowledge, Attitude and Practices among the Lebanese Adult Population
Immunization education/advocacy
Lebanon Influenza Adults
Gül et al.
(2007)
Nonprescription medication
purchases and the role of pharmacists as healthcare workers in
self-medication in Istanbul
Vaccine administration, Vaccine storage
Turkey N/R N/R
Hammett et al.
(2014)
Pharmacies as providers of expanded health services for people who inject drugs: a review of laws, policies, and barriers in six countries
Vaccine administration, Vaccine storage
Vietnam Hepatitis B Adults
International Pharmaceutical Federation (FIP) (2016)
An Overview of Current Pharmacy Impact on Immunisation - A Global Report
Immunization education/advocacy, Vaccine administration, Immunization training, Delivery of vaccine by other health providers in
pharmacies
Argentina, Bolivia, Brazil, China,
Democratic Republic of Congo, Costa Rica, Ethiopia, Iraq,
Jordan, Lebanon, Nigeria, Pakistan, Philippines, Russia, Senegal, South Africa
All Vaccines Children and adults
Iqbal et al.
(2016)
Effectiveness of pharmacists-led provider-focused interventions to improve HPV vaccination rates in adults in Malaysia
Immunization education/advocacy
Malaysia Human
papillomavirus
Adults
Mayora et al.
(2018)
Private retail drug shops: What they are, how they operate, and
implications for health care delivery in rural Uganda
Vaccine administration, Vaccine storage
Uganda N/R N/R
Melo et al.
(2017)
Pharmacy in Brazil: Progress and challenges on the road to expanding clinical practice
Vaccine administration , Vaccine storage
Brazil N/R N/R
Meyer et al.
(2018)
Childhood vaccination and the role of the pharmacist
Vaccine administration, Immunization training, Vaccine storage
South Africa N/R N/R
Ngcobo et al.
(2017)
The status of vaccine availability and associated factors in Tshwane
government clinics
Obebi Cliff-Eribo et al.
(2016)
Adverse drug reactions in Nigerian children: a retrospective review of reports submitted to the Nigerian Pharmacovigilance Centre from 2005 to 2012
Vaccine adverse event reporting
Nigeria N/R N/R
Ongpoy (2019) Proposed adult immunization training program for Filipino pharmacists
Immunization training Philippines N/R Adults
Ozcan et al.
(2016)
Adverse Drug Reaction Reporting Pattern in Turkey: Analysis of the National Database in the Context of the First Pharmacovigilance
Legislation
Vaccine adverse event reporting
Turkey N/R N/R
Shah et al.
(2016)
Quality of drug stores: Storage
practices & Regulatory compliance in Karachi, Pakistan
Vaccine storage Pakistan N/R N/R
Sharma et al.
(2015)
Implications of private sector Hib vaccine coverage for the introduction of public sector Hib-containing pentavalent vaccine in India: Evidence from retrospective time series data
Vaccine storage India Hib
(Pentavalent)
Children
Truter (2018) Exploratory study of the dispensing patterns of vaccines by a sample of community pharmacies in Southern Africa
Vaccine storage, Vaccine administration
South Africa All vaccines Children and Adults
Table 2: Descriptions of pharmacists’ roles in vaccination services by country
Country [Study] Reported role of pharmacists in vaccination services
Argentina [10] Pharmacists administer vaccinations, are involved in vaccination advocacy, and immunization training is required for pharmacists.
Bolivia [10] Pharmacists are involved in vaccination advocacy and vaccines are administered at pharmacies by other healthcare professionals.
Brazil [10, 43] Vaccines are stored and sold in community pharmacies and can be administered in community pharmacies by pharmacists. Official regulation of vaccine administration by pharmacists started in 2017. Pharmacists can access patient vaccination records.
Costa Rica [10] Pharmacists administer vaccinations, are involved in vaccination advocacy, and immunization training is required for pharmacists. Pharmacists can access patient vaccination records.
China [10] Pharmacists are involved in vaccination advocacy. Democratic
Republic of Congo [10]
Pharmacists are involved in vaccination advocacy and vaccines are administered at pharmacies by other healthcare professionals. Immunization training is required for pharmacists.
Ethiopia [10] Pharmacists are involved in vaccination advocacy. India [49] Vaccines are stored and sold at retail pharmacy outlets. Iraq [10] Pharmacists are involved in vaccination advocacy. Jordan [10] Pharmacists are involved in vaccination advocacy.
Malaysia [37, 42, 60]
Immunization training has been introduced in pharmacists’ training curriculum and pharmacists are involved in vaccine education and advocacy. Pharmacists conduct vaccine adverse event reporting and have access to patient vaccination records.
Nigeria [10, 34, 35, 46]
Pharmacists are involved in vaccination advocacy and can access patient vaccination records. Immunization training related to the vaccination schedule, storage, and travel vaccine recommendations are included in pharmacists’ training curriculum. Pharmacists are also involved in the reporting of vaccine adverse events.
Pakistan [10, 38, 48, 56]
Vaccines are stored and sold at drug stores operated by pharmacists. Vaccines are administered at pharmacies by government vaccinators/other healthcare professionals. Pharmacists can access patient vaccination records. Philippines [10,
53]
Pharmacists are involved in vaccination advocacy and immunization training is required for pharmacists. Pharmacists and other healthcare professionals administer vaccines at pharmacies.
Russia [10] Pharmacists are involved in vaccination advocacy.
Saudi Arabia [36] Pharmacists were involved in vaccine adverse event reporting for H1N1 vaccines as part of a study on the safety of the vaccine.
Senegal [10] Pharmacists are involved in vaccination advocacy and immunization training is required for pharmacists. South Africa [10,
21, 44, 45, 50, 51]
Community pharmacists who are trained and licensed can administer vaccines; however, they are not allowed to prescribe or administer certain regulated classes of vaccines, including travel vaccines. Immunization training is included in the pharmacists’ curriculum. Pharmacists are involved in patient education on immunization, store and sell vaccines, and can access patient immunization records. Other healthcare professionals administer vaccines at pharmacies.
Turkey [40, 47] Pharmacists administer and store vaccines, and contribute to reports on vaccine adverse events in the national pharmacovigilance database.
Uganda [23] Some retail drug shops in rural areas operated by pharmacists sell and administer vaccines; however, national regulations do not allow provision of immunization services by pharmacists.