http://www.ijcmph.com pISSN 2394-6032 | eISSN 2394-6040
Original Research Article
Exploration of epidemiologic profile and strategic prevention
framework for surgical site infection rates in a tertiary care
hospital of Bhopal city
Vidit Goyal
1, Rituja Kaushal
2*
INTRODUCTION
Surgical wound infections are a common cause of nosocomial infection. The United States Centers for Disease Control and Prevention (CDC) has developed criteria that define surgical site infection (SSI) as infection related to an operative procedure that occurs at or near the surgical incision within 30 days of the procedure or within 90 days if prosthetic material is implanted at surgery.1 There has been recent controversy regarding the CDC decision to shorten post-discharge surveillance to 90 days instead of one year after certain procedures.2 This change was aimed at simplifying post-discharge surveillance and reducing delayed feedback, but it has not been universally adopted as yet.3 SSIs are often localized to the incision site but can also extend into deeper adjacent structures.
SSIs are the most common nosocomial infection, accounting for 38 percent of nosocomial infections. However, the overall risk of SSI is low; it is estimated that SSIs develop in 2 to 5 percent of the more than 30 million patients undergoing surgical procedures each year (i.e., 1 in 24 patients who undergo inpatient surgery in the United States has a postoperative SSI).1,4-5
Surgical site infections (SSIs) are associated with substantial morbidity and mortality, prolonged hospital stay, and increased cost.6-8 The relation between the HAI rates and the type of hospital (public, academic and private), and the relation between HAI rates and the country’s socio-economic level (defined as low-income, mid-low-income and high- income) have recently been analyzed and published by the International Nosocomial Infection Control Consortium INICC.9-10 Such studies’ findings showed that a higher country socio-economic
ABSTRACT
Background: Post-operative surgical site infections are deadlock for any successful surgery. This exigency triggers draining of extra resources for management of the quagmire.
Methods: This prospective direct surveillance study based on incidence design was undertaken to gauge and estimate the nature of propensity of various surgical site infections in a tertiary care hospital over a period of twelve months.
Results: Calculated cumulative SSI rate for the year 2016 was found to be 4.32%.
Conclusions: It was concluded that a multidisciplinary approach integrating periodic training sessions on infection control, checklists based routine surveillance & following some benchmark etc. are the linchpin in controlling hospital acquired infections including surgical site infection rates in any clinical setting.
Keywords: Surgical site infection rates, Surveillance, Incidence, Bhopal, India
1
Department ofMicrobiology, 2Department of Community Medicine, LN Medical College and RC, Bhopal, India
Received: 19 December 2017
Revised: 12 January 2018
Accepted: 13 January 2018
*Correspondence:
Dr. Rituja Kaushal,
E-mail: [email protected]
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
level was correlated with a lower infection risk.9-10 Within this context, INICC reports can be an alternative valid benchmarking tool for HAI rates in hospitals worldwide due to their shared factual and socio-economic hospital backgrounds.
Many factors influence surgical wound healing and determine the potential for infection.11 These include patient-related (endogenous) and process/procedural-related (exogenous) variables that affect a patient’s risk of developing an SSI. Some variables are obviously not modifiable, such as age and gender. However, other potential factors can be improved to increase the likelihood of a positive surgical outcome, such as nutritional status, tobacco use, correct use of antibiotics and the intraoperative technique. Staphylococcus aureus, coagulase-negative Staphylococci, Enterococcus spp., and Escherichia coli remain the most frequently isolated pathogens. An increasing proportion of SSIs are caused by antimicrobial-resistant pathogens, such as methicillin-resistant S. aureus (MRSA), or by Candida albicans.12-14
Aim
This study was undertaken in a tertiary care institute a) to explore epidemiological trends of surgical site infection’s rate on monthly basis b) to discuss root causes/risk factors responsible for occurrence of SSIs & to observe
the importance of regular training sessions,
surveillance/Surgical safety checklists for improvement.
METHODS
This prospective clinical surveillance study based on incidence design was undertaken from 1.1.16 to 31.12.16 i.e. for a period of 1 year in a tertiary care centre/JK hospital of Bhopal to accomplish above mentioned objectives. This tertiary care centre is a private academic one. Bhopal is a city of central India and from international socioeconomic status point of view current India is considered as a developing country and majority of Bhopal’s population belongs to mid-low income group.
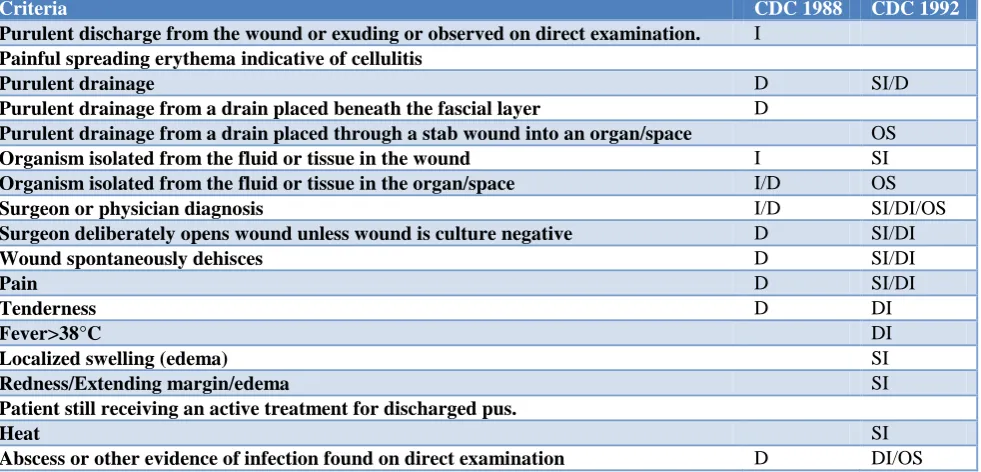
Table 1: Criteria taken under consideration for evaluation of SSIs.
Criteria CDC 1988 CDC 1992
Purulent discharge from the wound or exuding or observed on direct examination. I
Painful spreading erythema indicative of cellulitis
Purulent drainage D SI/D
Purulent drainage from a drain placed beneath the fascial layer D
Purulent drainage from a drain placed through a stab wound into an organ/space OS
Organism isolated from the fluid or tissue in the wound I SI
Organism isolated from the fluid or tissue in the organ/space I/D OS
Surgeon or physician diagnosis I/D SI/DI/OS
Surgeon deliberately opens wound unless wound is culture negative D SI/DI
Wound spontaneously dehisces D SI/DI
Pain D SI/DI
Tenderness D DI
Fever>38°C DI
Localized swelling (edema) SI
Redness/Extending margin/edema SI
Patient still receiving an active treatment for discharged pus.
Heat SI
Abscess or other evidence of infection found on direct examination D DI/OS
Note: CDC 1988 definitions: I, incisional surgical wound infection; D, deep surgical wound infection. CDC 1992 definitions: SI, superficial incisional; DI, deep incisional; OS, organ/space. The SISG and NPS allow fever (>38°C), tenderness, edema, an extending margin of erythema or if the patient is still receiving treatment for the wound. CDC: Centers for Disease Control and Prevention.
All registered post-operative IPD and OPD patients of every age group and both genders who were operated in the same setting for specific surgeries and fitting the definition of SSIs were included. All those post op patients (in the given period of study) who reported in OPDs for surgical site infections, were readmitted as IPD patients for exploration of the cause. Only those cases were included who were having their pre and post-operative data available in detail and in orderly fashion. All post op patients who were operated in different settings for specific surgeries plus who were not fitting the definition of SSIs were excluded from the study.
Above mentioned variables were taken under consideration for data collection purposes. CDC/NHSN operational definitions were used as epidemiological tool for data collection purposes. Data was collected from registers of microbiology department and was tallied with investigation registers of respective ward/unit. Periodic sessions of training on infection control practices were started from December 2015 as per hospital protocol. Subsequently bundled care interventions based supervisory checklist was included for monitoring and surveillance purposes in order to prevent surgical site infections. For statistical analysis purposes, formula used = Total surgical site infections noted /Total surgeries
done ×100. Due permission was taken from relevant authorities for data collection purposes & confidentiality of data was maintained.
RESULTS
In our study commonly isolated microbes were S. aureus, Enterobacter, E. coli, Klebsiella. Commonly and routinely performed surgical procedures in our setting were various orthopedic procedures, gynae procedures, pediatric surgeries, laprotomies, rectal surgeries, cholecystectomies, cardiovascular surgeries, neuro-surgeries etc. Table 2 depicts month wise SSI rates data.
Table 2: Distribution of surgical site infections rates data per 100 surgeries done on monthly basis.
Total surgeries done (GA+SA) Total surgical site
infections noted Name of the month SSI rates in %
270 26 January-16 9.62
289 35 February-16 12.11
286 17 March-16 5.9
308 12 April-16 3.89
249 15 May-16 6.02
316 5 June-16 1.58
267 7 July-16 2.62
265 13 August-16 4.90
289 5 September-16 1.73
260 5 October-16 1.92
290 5 November-16 1.72
333 3 December-16 0.90
Table 3: Distribution of various microbes isolated from surgical site infections/various wounds/pus swabs etc. as per antibiotic resistance pattern in the year 2016.
Isolates Number Sensitivity profile
Gram positive 46 P (2.17), AC (15.21), Cx (21.74),CFZ (15.21) Va (97.83), Gen (63.04), Ak (73.91), Cd (63.04), Lz (97.83), Le (52.17), Azm (36.96), PRT (89.13), CoT (60.87)
Gram negative 101
Amp (18.81), AmpS (25.74), CFZ (43.56), CPZ (46.53), CPZ/S (65.35), PPT (66.34), IMP (84.16), MRP (76.24), Ak (76.24), Gm (67.33), CL (88.12), AZ (47.52), LE (45.54), CoT (57.42)
Organism Number Sensitivity profile
Staph aureus 37 P (2.70), AC (16.22), Cx (21.62),CFZ (16.22) Va (100.00), Gen (59.46), Ak (72.98), Cd (59.46), Lz (97.30), Le (51.35), Azm (37.84), PRT (91.89), CoT (62.16)
Staph epidermidis 2 P (0.00), AC (0.00), Cx (0.00),CFZ (0.00) Va (100.00), Gen (100.00), Ak (100.00), Cd (100.00), Lz (100.00), Le (50.00), Azm (50.00), PRT (100.00), CoT (50.00)
Staph
haemolyticus 7
P (0.00), AC (14.26), Cx (28.57),CFZ (14.26) Va (85.71), Gen (71.43), Ak (71.43), Cd (71.43), Lz (100.00), Le (57.14), Azm (28.57), PRT (71.43), CoT (57.14)
E coli 36
Amp (27.78), AmpS (38.89), CFZ (47.22), CPZ (52.78), CPZ/S (66.67), PPT (63.89), IMP (88.89), MRP (83.33), Ak (80.56), Gm (69.44), CL (91.67), AZ (50.00), LE (58.33), CoT (66.67)
Klebsiella
pneumoni 17
Amp (23.52), AmpS (29.41), CFZ (41.18), CPZ (41.18), CPZ/S (70.59), PPT (76.47), IMP (88.24), MRP (88.24), Ak (82.35), Gm (88.24), CL (88.24), AZ (58.82), LE (64.70), CoT (76.47)
Pseudomonas
aeruginosa 22
Organism Number Sensitivity profile
Proteus mirabilis 9
Amp (22.22), AmpS (33.33), CFZ (33.33), CPZ (33.33), CPZ/S (55.56), PPT (44.44), IMP (77.78), MRP (55.56), Ak (66.67), Gm (55.56), CL (100.00), AZ (44.44), LE (55.56), CoT (33.33)
Citrobacter
freundi 13
Amp (7.69), AmpS (23.08), CFZ (30.77), CPZ (38.46), CPZ/S (53.85), PPT (53.85), IMP (84.62), MRP (69.23), Ak (61.54), Gm (61.54), CL (76.92), AZ (15.38), LE (30.76), CoT (53.85)
Acinetobacter
baumannii 3
Amp (0.00), AmpS (33.33), CFZ (33.33), CPZ (66.67), CPZ/S (66.67), PPT (66.67), IMP (100.00), MRP (100.00), Ak (100.00), Gm (66.67), CL (100.00), AZ (0.00), LE (0.00), CoT (33.33)
Morexella
catarrhalis 1
Amp (0.00), AmpS (0.00), CFZ (0.00), CPZ (0.00), CPZ/S (100.00), PPT (100.00), IMP (100.00), MRP (0.00), Ak (0.00), Gm (0.00), CL (100.00), AZ (100.00), LE (0.00), CoT (100.00)
Candida albicans 1
From January to March 2016 total surgical site infections noted on monthly basis are higher (26 & 35 per month) in comparison to March onwards data where surgical site infections noted are showing declining trends (3-17 per month).
SSI rates noted in first 2 months of year are in the range of 12.11 - 9.62% which then declined to the range of 0.90 – 6.02% from March to December 2016.
Month wise cumulative SSI rate for the year 2016 was calculated as 4.32 episodes per 100 surgical procedures done. In the month May and August there are 2 peaks due to relative increase in numerators (15 and 13 respectively) and fall in denominators (249 and 265 respectively).
DISCUSSION
Ideally from “Risk and Prevention” perspective below mentioned aspects should be taken into consideration appropriately.
Issues like diabetes, nicotine use, steroid use, malnutrition, prolonged preoperative hospital stay, preoperative nares colonization with staphylococcus aureus, type of wound, perioperative transfusion are considered under patient’s characteristics. Similarly preoperative antiseptic showering, preoperative hair removal, patient skin preparation in the operating room, preoperative hand/forearm antisepsis, management of infected or colonized surgical personnel, antimicrobial prophylaxis are preoperative issues. In intraoperative issues - operating room environment, ventilation, cleaning and disinfection of environmental surfaces, microbiologic sampling, surgical attire and drapes, asepsis, instrumental sterilization issues, duration of surgery, use of drain and surgical technique are considered. In postoperative issues - incision care, discharge planning are of at most importance.
Finally comes the role of SSI Surveillance which includes SSI risk stratification, SSI surveillance methods (inpatient, post op patient, outpatient).14
Participation in INICC and other accreditation agency’s program plays a basic role (in many hospital settings), not only in increasing the awareness of HAI risks in the hospitals, but also in providing a platform for the dissemination of information regarding infection control practices. In many INICC hospitals, for example, the high incidence of HAI has been reduced by 30 to 70% by implementing multidimensional programs that include a bundle of infection control interventions, educational training sessions, outcome surveillance, process surveillance, feedback of HAI rates and performance feedback of infection control practices, for central line-associated bloodstream infections, mechanical ventilator-associated pneumonia and catheter-ventilator-associated urinary tract infections etc.15-17
Similarly agency like National Accreditation Board for Hospitals and health care facilities (NABH) is playing a formidable part in improving quality of care of patients in India.
There may be some under reporting of SSIs, as some patients may have presented a SSI after the study period (such as, orthopedic procedures and implants) and these may not have been included.18
In our study setting all possible pre, intra and post-operative issues were handled carefully in routine manner to avoid surgical site infection risks. Like many other hospitals, commonly isolated microbes with their varying sensitivity patterns were S. aureus, Enterobacter, E. coli, Klebsiella. Routinely performed surgical procedures in our setting were various orthopedic procedures, gynecological procedures, pediatric surgeries, laparotomies, rectal surgeries, cholecystectomies, cardiovascular surgeries, neurosurgeries etc. In United States in 2014, SSI rate in % which was measured as cumulative incidence (episodes per 100 surgeries) for 10 selected procedures was 0.9. Similarly for Republic of Korea from 2010-2011 over all SSI rate in % was estimated to be 2.1.19
procedures done. It was less than the study conducted in a government tertiary care hospital of Mysore – 21.66% (Kikkeri et al).20 It was comparable with the study conducted in DY Patil Medical College, Pune – 6% (Shahney et al).21 At the start of study in first 2 months overall SSI rates for various types of surgeries were comparatively higher ranging from 9.62 - 12.11%. After multiple sessions of trainings on bundled care intervention and surgical site improvement project (SCIP), rates dropped down to much lower levels in subsequent months. In between there are certain peaks in SSI data but that might be due to attrition problem as many trained staffs left the job and in their place many newer, untrained staffs joined in and from negligence perspective surgical site infection rates shooted. Issues related to patient’s characteristic like tobacco use, malnutrition, anemia, pre-operative waiting, prophylactic antibiotic, diabetes plus other comorbidities etc. and characteristics related to pre, intra and post-operative care were almost normally distributed throughout the span of study.
Study limitations
Similar to the findings of INICC, this study also has three main clampdowns. First, we were unable to calculate the risk category of the surgical procedures because we did not collect the duration of each surgical procedure, the level of contamination and the ASA score.
Second, we were not able to collect data to differentiate superficial, deep and organ/space SSIs, nor implemented any other kind of post-discharge surveillance, such as phone calls, visits or letters to patients. Third, with a small sample size of cases in some surgical procedures, these results should be interpreted with caution.
CONCLUSION
As epidemiology of SSI is changing with evidence of
increased incidence and severity hence a
multidisciplinary approach including standardized surveillance methods, antibiotic stewardship guidelines along with training of healthcare workers etc. is the crying need. Prevention efforts must include tracking of healthcare facility-onset, healthcare facility-associated SSI for hospital settings. Tracking of community-onset should be done only in conjunction with healthcare facility-onset, healthcare facility associated SSIs. For a valid comparison of a hospital’s SSI rates with the rates from INICC hospitals/other accredited hospitals, it is required that the concerned staffs start collecting their data by applying definitions of surgical procedures as provided by the ICD-9/10, the definitions described by CDC-NHSN in order to identify SSIs, and then the methodology described by CDC- NHSN to calculate SSI rates.
Funding: No funding sources Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee
REFERENCES
1. Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC definitions of nosocomial surgical site infections, 1992: A modification of CDC definitions of surgical wound infections. Infect Control Hosp Epidemiol 1992;13(10):606-08. 2. Surgical site infection (SSI) event. Atlanta (GA):
Centers for Disease Control and Prevention; 2013. 3. Surveillance of surgical site infections in European
hospitals – HAISSI protocol. Version 1.02. Stockholm: European Centre for Disease Prevention and Control; 2012.
4. Consensus paper on the surveillance of surgical wound infections. The Society for Hospital Epidemiology of America; The Association for Practitioners in Infection Control; The Centers for Disease Control; The Surgical Infection Society. Infect Control Hosp Epidemiol. 1992;13:599. 5. Lewis SS, Moehring RW, Chen LF, Sexton DJ,
Anderson DJ. Assessing the relative burden of hospital-acquired infections in a network of community hospitals. Infect Control Hosp Epidemiol. 2013;34:1229.
6. Boyce JM, Potter-Bynoe G, Dziobek L. Hospital reimbursement patterns among patients with surgical wound infections following open heart surgery. Infect Control Hosp Epidemiol 1990;11:89.
7. Poulsen KB, Bremmelgaard A, Sørensen AI,
Raahave D, Peterson JV. Estimated costs of postoperative wound infections. A case-control study of marginal hospital and social security costs. Epidemiol Infect 1994;113(2):283-95.
8. Vegas AA, Jodra VM, García ML. Nosocomial infection in surgery wards: a controlled study of increased duration of hospital stays and direct cost of hospitalization. Eur J Epidemiol. 1993;9:504. 9. Rosenthal VD, Lynch P, Jarvis WR, Khader IA,
Richtmann R, Jaballah NB, et al. Socioeconomic impact on device-associated infections in limited-resource neonatal intensive care units: findings of the INICC. Infection. 2011;39(5):439–50.
10. Rosenthal VD, Jarvis WR, Jamulitrat S, Silva CP, Ramachandran B, Duenas L, et al. Socioeconomic impact on device-associated infections in pediatric intensive care units of 16 limited-resource countries: International Nosocomial Infection Control Consortium findings. Pediatric Crit Care. 2012;13(4):399–406.
11. Buggy D. Can anaesthetic management influence
surgical wound healing? Lancet.
2000;356(9227):355-7.
12. Schaberg DR. Resistant gram-positive organisms. Ann Emerg Med. 1994;24(3):462-4.
14. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guidelines for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999;20(4):231-2
15. Rosenthal VD, Maki DG, Rodrigues C, Alvarez Moreno C, Leblebicioglu H, Sobreyra-Oropeza M et al. Impact of International Nosocomial Infection Control Consortium (INICC) strategy on central line-associated bloodstream infection rates in the intensive care units of 15 developing countries. Infect Control Hosp Epidemiol. 2010;31:1264–72. 16. Tao L, Hu B, Rosenthal VD, Zhang Y, Gao X, He
L. Impact of a multidimensional approach on ventilator-associated pneumonia rates in a hospital of Shanghai: Findings of the International Nosocomial Infection Control Consortium. J Crit Care. 2012;27:440–6.
17. Rosenthal VD, Ramachandran B, Duenas L,
Alvarez Moreno C, Navoa-Ng JA, Armas-Ruiz A, et al. Findings of the International Nosocomial approach on catheter-associated urinary tract infection rates in pediatric intensive care units of 6 developing countries. Infect Control Hosp Epidemiol 2012;33:696–703.
18. Singh S, Chakravarthy M, Rosenthal VD, Myatra SN, Dwivedy A, Bagasrawala I, et al. Surgical site infection rates in 6 cities of India: findings of the International Nosocomial Infection Control Consortium. Int Health. 2015;7(5):354-9.
19. Global Guidelines for the Prevention of Surgical Site Infection. World Health Organization 2016, Printed by the WHO document production services, Geneva, Switzerland.
20. Kikkeri NHS, Nagaraja MS, Nagappa DH,
Giriyaiah CS, Gowda NR, Naik RDML. A study on surgical site infections and associated factors in a government tertiary care teaching hospital in Mysore. Int J Med Public Health. 2014;4(2):171-5. 21. Shahne V, Bhawal S, Lele U. Surgical site
infections: A one year prospective study in a tertiary care centre. Int J Health Sci (Qassim). 2012;6(1):79-84.