Improving knowledge of breastfeeding management: a
practice development intervention for paediatric nurses
Alison Williams*
Children’s Nutrition Research Centre, The University of Queensland, Australia
Jeanine Young
Professor of Nursing, School of Nursing and Midwifery, University of the Sunshine Coast, Visiting Fellow, Children's Health Queensland Hospital & Health Service
Dr Lauren Kearney
Nurse Researcher, Royal Children’s Hospital, Children’s Health Queensland Hospital and Health Service, Herston, QLD 4029 Australia
Dr Samantha Keogh
Senior Research Fellow, Griffith University, NHMRC Centre for Research Excellence in Nursing, Centre for Clinical Nursing Royal Brisbane & Women’s Hospital, Herston, QLD 4029, Australia
*Corresponding author
Abstract
Aim
The primary aim of this study was to evaluate the impact of a targeted, practical education intervention on paediatric nurses’ knowledge of appropriate breastfeeding management in an acute practice setting.
Background
Breastfeeding provides the optimal method for infant growth and nutrition, yet studies have demonstrated knowledge deficits of Australian paediatric nurses regarding the management of the mother–infant breastfeeding dyad. Limited evidence is available evaluating which educational approach is effective in the dynamic and busy acute care setting.
Design
This study was a two-phased, mixed-method design, conducted in a large, tertiary, metropolitan children’s hospital in south-east Queensland, Australia.
Methods
Reference groups were conducted in Phase One to advise development of the resource kit. Phase Two was the experimental phase and included a pre-test knowledge survey, the educational intervention, and a post-test knowledge survey.
Results
Pre- and post-test response rates of 75% (n=49) and 34% (n=23) respectively were achieved from the population of 67 eligible participants. Post-intervention study results demonstrated knowledge improvement in four key breastfeeding management areas: importance of baby-led feeding; reduction in otitis media risk for breastfed infants; ongoing management of maternal milk supply when breastfeeding is interrupted; and the correct storage and management of expressed breast milk. Areas for further knowledge improvement included management of more complex breastfeeding scenarios, such as mastitis.
Conclusion
The implementation of a resource kit and brief education series has improved the knowledge of paediatric nurses in some areas of breastfeeding practice and management.
Keywords: Breastfeeding, paediatric nurse, nurse education.
What is known about this topic
• Breastfeeding is the optimal method of infant nutrition. The knowledge of paediatric nurses regarding breastfeeding has been explored in the literature, and shown to be limited. Educational support for paediatric nurses in the area of breastfeeding knowledge and skills has been identified as important.
What this paper adds
• This paper describes the development and implementation of a pragmatic, focused and practical educational series formulated to address the knowledge and practice needs of paediatric nurses in the area of breastfeeding management in the acute care setting. It demonstrated areas of knowledge improvement through the intervention, and identified areas for further research, such as the need to investigate the impact this knowledge has on child and family outcomes.
Declarations
The authors of this paper have no competing interests which would bias the publishing of this paper.
This project was funded through a Nursing Research Project Grant, donated by the Royal Children’s Hospital Foundation (Qld) (grant number — 10245).
Guarantor Please forward all correspondence to Jeanine Young.
Contributorship All authors.
Implications for clinical practice
Improved breastfeeding knowledge and practical skills of paediatric nurses will support the provision of appropriate breastfeeding management in acute care settings and promote the continuation of breastfeeding for the hospitalised infant. Given the recognised short- and long-term benefits of breast milk for infants, optimising support of breastfeeding families is essential for optimal health outcomes.
Acknowledgements
Dr Robert Ware, Biostatistician, Queensland Children’s Medical Research Institute, University of Queensland, for his contributions to the statistical analysis.
Introduction and background
Breastfeeding provides the optimal method for infant growth and nutrition, and is well recognised as the complete nutrition source during the first six months of life1. The health benefits of
breastfeeding are significant to mothers and infants, reducing the risk of multiple acute and chronic conditions, such as pneumonia, ear infections, Crohn’s disease and childhood obesity1,2. Breastfeeding is a key indicator of childhood health
and wellbeing and has been listed as a priority area by international health agencies and governments3. Breastfeeding
initiation rates are high for infants in Australia (96%), although only 39% are exclusively breastfed to three months of age3,
with the figure falling to 15% by around six months, when complementary foods should be commenced3, and has been
listed as a priority area for improvement by the Australian Institute of Health and Welfare4. Consistent, evidence-based
breastfeeding support from health care professionals can significantly enhance a woman’s ability and confidence to breastfeed5. However, many health professionals are provided
minimal education to equip them to adequately support breastfeeding mothers6,7, thus compromising their ability to
help. For example, one study cited 85% of undergraduate nursing students were unaware of the recommendation to breastfeed for at least a year8.
When an infant is admitted to hospital or attends an emergency department this can be a very stressful time for the family. How health care professionals manage this vital mother–baby breastfeeding dyad during this time has a crucial implication for the ongoing success of breastfeeding. Stress is known to negatively affect breastfeeding and breast milk synthesis9,10, subsequently making this a high risk time to
wean or supplement with artificial infant formulas.
McLaughlin and colleagues11 investigated Australian
paediatric nurses’ knowledge and attitudes toward breastfeeding and found overall positive attitudes toward breastfeeding; however, significant knowledge deficits in
the areas of supplemental formula feeding, immunologic properties of breast milk and duration and frequency of breastfeeding existed. This is consistent with other studies which also demonstrated positive attitudes among health care professionals, yet identified a lack of accurate knowledge and understanding around crucial aspects of breastfeeding12,13.
Consistent and sustainable approaches in facilitating knowledge improvement of breastfeeding management are required in order to address identified knowledge deficits known to impact breastfeeding outcomes7,8,11, and to
increase the extent to which evidence-based breastfeeding management is incorporated into everyday care and discharge planning by paediatric nurses within acute clinical practice settings.
Research objective
The primary objective of this study was to develop and pilot a specific education intervention with the aim of improving knowledge of paediatric nurses in providing evidence-based breastfeeding management in an acute care hospital environment.
Research questions
To achieve this research objective, three specific research questions were developed:
1. Given breastfeeding knowledge deficits of paediatric nurses identified in earlier studies11, and busy acute
care clinical units in which they work, which method of breastfeeding education for clinicians would be most appropriate, feasible and acceptable?
2. What are the priority knowledge and practice needs of paediatric nurses caring for breastfed infants in the acute care setting?
3. What impact does a targeted educational intervention have on paediatric nurses’ knowledge of evidence-based breastfeeding management?
Methods
This study was a two-phased, mixed-method design, conducted in a large, tertiary, metropolitan children’s hospital in south-east Queensland, Australia.
Phase One
Phase One was the development phase and involved the formation of two reference groups. The aim of the reference groups was to address Research Question One, and specifically to determine the approach of breastfeeding education for paediatric nurses that would be most appropriate, feasible and acceptable in acute paediatric settings.
Sample
Reference group one comprised of representation from the hospital family advisory council, Australian Breastfeeding Association (ABA), community child health liaison nurse, hospital dietician and a Baby Friendly Hospital Initiative coordinator (the hospital Baby Liaison Nurse was also invited, but unable to attend). Reference group two comprised of the nursing directors for medical, surgical, education and research divisions. Both reference groups were presented with clinical scenarios of typical infant hospitalisation situations, designed to stimulate response, discussion and
to prioritise paediatric nursing knowledge (or educational) and practice requirements to support breastfeeding in the acute care setting. A member of the research team who had over 20 years of clinical experience supporting breastfeeding mothers in both acute and community settings facilitated both groups. These sessions affirmed the direction of the educational intervention in the second phase of the study.
Phase Two
Phase Two was the experimental phase and included a pre-test knowledge survey, the educational intervention and a post-test knowledge survey.
Sample
The sample was drawn from the population of eligible paediatric nurses (n=67) working in an acute surgical unit of a metropolitan tertiary children’s hospital in south-east Queensland, Australia. Eligibility criteria included being an enrolled or registered general nurse, full-time or part-time, permanently or temporarily employed in the selected unit. Nursing staff on leave (that is, sick, maternity, recreational or long service) for more than four weeks during this time were excluded. This unit was chosen due to the high proportion of infants aged <12 months routinely admitted and the nurse unit manager’s support for the project and its aims.
Intervention
The evidence-based breastfeeding management intervention included a series of five 20–30 minute educational sessions delivered in a two-week period by a nursing clinical facilitator with qualifications in child health nursing, midwifery and research.
The five sessions included:
• Breastfeeding clinical scenarios. • Breastfeeding techniques.
• Breast milk expression (hand and mechanical) and management of expressed breast milk.
• Troubleshooting breastfeeding issues and supportive strategies for families.
• Resources and referral pathways.
Each session was repeated five to six times during the two-week period to maximise opportunity for participation by clinicians. In addition, a practical resource kit including presenter and participant objectives for each of the five sessions, a DVD (Baby-led Breastfeeding … The Mother–Baby Dance14); breast model; a Clinician’s Breastfeeding Triage
Tool15; and posters of baby feeding cues, were provided to
each clinical area to be used for ongoing education and as a clinical resource.
Data collection
Phase one
Key words and themes were transcribed by the group facilitator (nurse researcher) from responses to the case scenario during reference group discussions. Emergent themes which reflected the concepts discussed were checked with participants during discussion and at the end of the sessions to ensure clarity and understanding16.
Phase two
Data were collected through a pre- and post-test knowledge survey with a shortened version of the knowledge and
attitudes survey tool used by McLaughlin and colleagues, which had been adapted and used with permission11. The
survey contained three sections: demographic information (nine questions); breastfeeding knowledge (20 questions, using a five-point Likert scale); and breastfeeding knowledge relevant to the hospitalised infant (eight questions, using a four-point Likert scale; 10 questions using a five-point Likert scale)17.
Procedure
In liaison with the nurse unit manager, the roster schedule was used to identify current staff. Participants received a survey and information sheet distributed via the internal mail system. Consent was implied by the return of a completed questionnaire via the addressed return envelope. Respondents were asked to use a unique identifier to allow matching of pre- and post-test surveys while ensuring anonymity of the individual. The same survey was administered prior to delivery of the education sessions, and then readministered during a two-week period, four weeks after the education intervention.
Ethical approval for the study was granted from the local hospital Human Research Ethics committee (approval number EC00175).
Data analysis
Phase One data analysis
The responses generated from each of the reference group discussions were recorded and thematically analysed for emergent themes16 and checked with participants at the
conclusion of each session. These data were then utilised to inform the development of the education sessions and breastfeeding management resource kit.
Phase Two data analysis
Medians, interquartile ranges (IQR), frequencies and percentages were used to report the central tendency, spread and empirical distributions of categorical and non-symmetric continuous variables elicited at each survey. When continuous data were distributed symmetrically, the means and standard deviation were reported. All bivariate comparisons of categorical frequencies were undertaken using Fisher’s exact test, while the Wilcoxon signed ranks test was used to detect pre-test and post-test differences based on the participant’s response most consistent with the evidence. Participants completing both pre- and post-test surveys were used in a paired analysis to determine intervention effectiveness in impacting nursing knowledge of breastfeeding the hospitalised infant. Statistical computations were facilitated with the use of IBM SPSS Statistics Version 20. An alpha-level of 5% was considered statistically significant for all comparisons.
Results
Phase One
The verbatim data from both reference groups yielded four key concepts: (1) maternal support and reassurance; (2) maintenance of breast milk supply; (3) referral sources; and, (4) the development of a clinical area breastfeeding management resource kit.
When presented with the clinical scenario, group participants stated that it was essential that the nurse provide support to the breastfeeding mother through verbal “praise and positive comments” regarding her efforts to provide breast milk for her infant. This discussion also highlighted this dialogue as an opportunistic time for the nurse to “reiterate to the parent the health benefits of breastfeeding”.
The group members also discussed the importance of knowing how to maintain a mother’s breast milk supply when it may be affected by the infant’s illness or stress of hospitalisation. This discussion centred on what paediatric nurses needed to know to support breastfeeding mothers, which included the use of breast pumps and privacy while expressing.
Thirdly, referrals and who was best equipped to support the breastfeeding family was discussed, which included the need for clarification around community child health nursing support, and support from other agencies, such as the Australian Breastfeeding Association, when the infant was hospitalised.
There was overall consensus for the need to establish a practically based, breastfeeding management resource for the clinical area, specifically designed for the needs of paediatric nurses to complement the considerable amount of health care literature already available that supports breastfeeding knowledge and practice.
Phase Two
Pre-test survey data
Pre- and post-test response rates of 75% (n=49) and 34% (n=23) respectively were achieved from the population of 67 eligible participants.
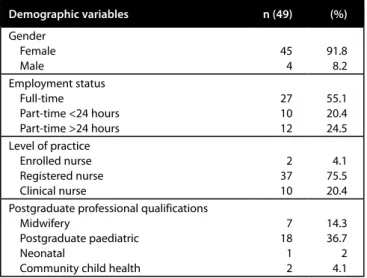
Demographic characteristics
Participant demographics are provided in Table 1. The mean duration of employment in an acute paediatric clinical setting was 7.7 years (SD±7.7 years).
Table 1: Demographic characteristics
Demographic variables n (49) (%) Gender Female Male 45 4 91.8 8.2 Employment status Full-time Part-time <24 hours Part-time >24 hours 27 10 12 55.1 20.4 24.5 Level of practice Enrolled nurse Registered nurse Clinical nurse 2 37 10 4.1 75.5 20.4 Postgraduate professional qualifications
Midwifery
Postgraduate paediatric Neonatal
Community child health
7 18 1 2 14.3 36.7 2 4.1 The pre-test survey also included the participants’ sources of breastfeeding knowledge, with personal experience (26, 53.1%) and advice from professional colleagues (28, 57.1%) cited most often. Undergraduate nursing course (18, 36.7%); professional conferences (7, 14.3%); and professional journals (8, 16.3%) were also cited as breastfeeding knowledge sources.
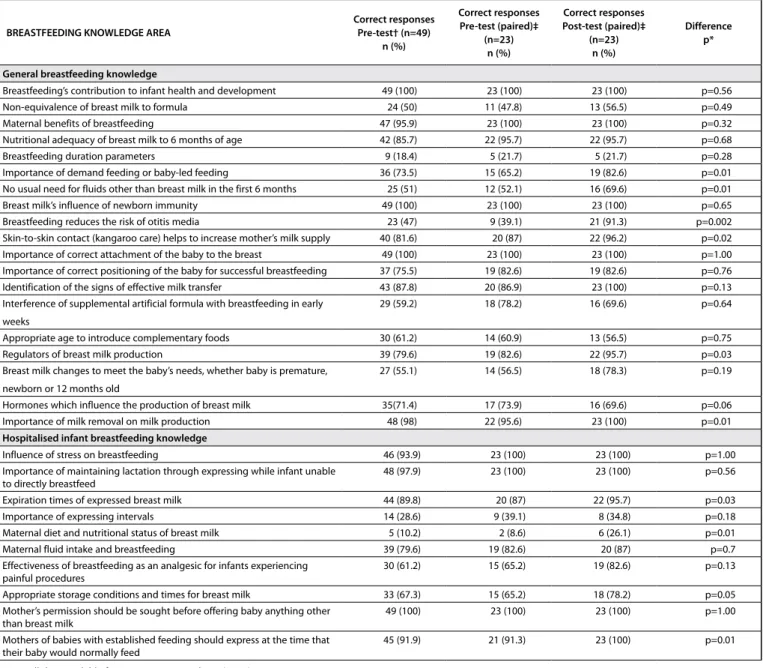
Changes in breastfeeding knowledge
Forty-nine paediatric nurses completed the pre-intervention survey, with 23/49 (47%) also completing the post-intervention survey. Comparing those who completed the post-intervention survey against those who did not, there were no statistically significant differences found in any measured demographic variables. Table 2 presents a summary of the correct responses (most consistent with the evidence) from the general and hospitalised infant breastfeeding knowledge sections of the survey including the knowledge differences (if present) after the educational intervention. Within the questionnaire nurses were also asked under which circumstances breastfeeding would be recommended to cease. In all of the instances the correct answer was ‘never’. Sore nipples and mastitis were knowledge areas most poorly understood with around a third to almost half of the respondents, respectively, still not aware of correct management post-intervention.
Discussion
The admission and treatment of an infant in hospital can cause considerable stress and concern for families. How nurses care for families, specifically in the area of breastfeeding during this time can dramatically affect the course of infant nutrition from that point forward. Informed by an earlier study that investigated the knowledge and attitudes of paediatric nurses regarding breastfeeding11, this study aimed
to respond to these findings by a) developing an appropriate, feasible and acceptable strategy to meet the learning needs of paediatric nurses working in acute paediatric settings, and b) evaluating the effectiveness of this strategy.
Development of the breastfeeding management
resource kit
One of the key aims of the study was to develop and test the impact of targeted education on paediatric nurses’ knowledge of breastfeeding in a dynamic and demanding clinical setting. The reference group consultations yielded important insights into the environment where the paediatric nurses worked and their perceptions of their learning needs in the area of breastfeeding. This prompted the development of the clinical area breastfeeding management resource. It was not the intention of the authors to provide a comprehensive course or online learning programme about breastfeeding to the paediatric nurses, as these have been developed and found to be effective18,19. Rather, the reference groups
confirmed that the development of a complementary and practical resource kit, which could be immediately sourced by nurses in their clinical environments, would assist in informing effective help provided by a paediatric nurse to a breastfeeding mother–baby dyad.
Attending to infant feeding and nutrition is a fundamental role within paediatric nursing, and should be supported within the health system1 to ensure best practice and thus quality care
for families. It is, therefore, essential that paediatric nurses be provided with accessible, evidence-based information (and in this case a practical resource kit), which can inform best practice. In the absence of timely, specialised breastfeeding support (such as an International Board Certified Lactation Consultant) within the acute paediatric environment, it is not
unreasonable that all clinical nurses working with mothers and babies be informed and supported in their role of providing effective infant nutrition care to families.
Reference groups, comprised of experienced clinicians, were in agreement that a further course on breastfeeding was not a priority as information about breastfeeding was available for paediatric nurses. What was identified as a feasible, acceptable and appropriate approach was the development of a practical resource kit that would be suitable for use in short sessions in busy clinical environments or that could be presented within a single, three-hour session by a clinical nurse (facilitator or educator), and act as a clinical resource or reference.
Knowledge of breastfeeding
Pre-survey results suggested that, overall, the cohort (n=49) was positive about breastfeeding, unanimously agreeing that ‘breast is best’ and that part of their role was to support breastfeeding mothers and infants. This finding is consistent with other studies, which also found general beliefs of
paediatric nurses to be positive towards breastfeeding20.
Whilst this is encouraging, it does not necessarily enable a clinician to effectively manage a challenging breastfeeding dilemma with a sick infant and concerned mother. Several studies have reported that many health professionals state they are confident in their ability to support breastfeeding mothers, yet their knowledge regarding correct management strategies is poor7,21. Formal training and/or a user-friendly
educational resource on breastfeeding management produces more effective care practices and increased breastfeeding rates19,22, than positive attitudes alone.
Effectiveness of the intervention in improving
breastfeeding knowledge
Post-intervention study results demonstrated knowledge improvement in four key breastfeeding management areas: importance of baby-led feeding; reduction in otitis media risk for breastfed infants; ongoing management of maternal milk supply when breastfeeding is interrupted; and the correct storage and management of expressed breast milk.
Table 2: Breastfeeding knowledge of paediatric nurses
BREASTFEEDING KNOWLEDGE AREA Correct responsesPre-test† (n=49) n (%) Correct responses Pre-test (paired)‡ (n=23) n (%) Correct responses Post-test (paired)‡ (n=23) n (%) Difference p* General breastfeeding knowledge
Breastfeeding’s contribution to infant health and development 49 (100) 23 (100) 23 (100) p=0.56
Non-equivalence of breast milk to formula 24 (50) 11 (47.8) 13 (56.5) p=0.49
Maternal benefits of breastfeeding 47 (95.9) 23 (100) 23 (100) p=0.32
Nutritional adequacy of breast milk to 6 months of age 42 (85.7) 22 (95.7) 22 (95.7) p=0.68
Breastfeeding duration parameters 9 (18.4) 5 (21.7) 5 (21.7) p=0.28
Importance of demand feeding or baby-led feeding 36 (73.5) 15 (65.2) 19 (82.6) p=0.01
No usual need for fluids other than breast milk in the first 6 months 25 (51) 12 (52.1) 16 (69.6) p=0.01
Breast milk’s influence of newborn immunity 49 (100) 23 (100) 23 (100) p=0.65
Breastfeeding reduces the risk of otitis media 23 (47) 9 (39.1) 21 (91.3) p=0.002
Skin-to-skin contact (kangaroo care) helps to increase mother’s milk supply 40 (81.6) 20 (87) 22 (96.2) p=0.02
Importance of correct attachment of the baby to the breast 49 (100) 23 (100) 23 (100) p=1.00
Importance of correct positioning of the baby for successful breastfeeding 37 (75.5) 19 (82.6) 19 (82.6) p=0.76
Identification of the signs of effective milk transfer 43 (87.8) 20 (86.9) 23 (100) p=0.13
Interference of supplemental artificial formula with breastfeeding in early weeks
29 (59.2) 18 (78.2) 16 (69.6) p=0.64
Appropriate age to introduce complementary foods 30 (61.2) 14 (60.9) 13 (56.5) p=0.75
Regulators of breast milk production 39 (79.6) 19 (82.6) 22 (95.7) p=0.03
Breast milk changes to meet the baby’s needs, whether baby is premature, newborn or 12 months old
27 (55.1) 14 (56.5) 18 (78.3) p=0.19
Hormones which influence the production of breast milk 35(71.4) 17 (73.9) 16 (69.6) p=0.06
Importance of milk removal on milk production 48 (98) 22 (95.6) 23 (100) p=0.01
Hospitalised infant breastfeeding knowledge
Influence of stress on breastfeeding 46 (93.9) 23 (100) 23 (100) p=1.00
Importance of maintaining lactation through expressing while infant unable
to directly breastfeed 48 (97.9) 23 (100) 23 (100) p=0.56
Expiration times of expressed breast milk 44 (89.8) 20 (87) 22 (95.7) p=0.03
Importance of expressing intervals 14 (28.6) 9 (39.1) 8 (34.8) p=0.18
Maternal diet and nutritional status of breast milk 5 (10.2) 2 (8.6) 6 (26.1) p=0.01
Maternal fluid intake and breastfeeding 39 (79.6) 19 (82.6) 20 (87) p=0.7
Effectiveness of breastfeeding as an analgesic for infants experiencing
painful procedures 30 (61.2) 15 (65.2) 19 (82.6) p=0.13
Appropriate storage conditions and times for breast milk 33 (67.3) 15 (65.2) 18 (78.2) p=0.05
Mother’s permission should be sought before offering baby anything other
than breast milk 49 (100) 23 (100) 23 (100) p=1.00
Mothers of babies with established feeding should express at the time that
their baby would normally feed 45 (91.9) 21 (91.3) 23 (100) p=0.01
†using all data available from pre-test respondents (n=49)
‡using data from nurses who responded to both pre- and post-test questionnaires (n=23) *p values were calculated on the change of knowledge using the Wilcoxon signed ranks test
Baby-led feeding is a fundamental aspect of breastfeeding and supported by significant evidence2,7. When feeding
may be interrupted by procedures, surgery or illness, baby-led feeding will assist in the re-establishment of supply. Correct attachment to the breast is also a fundamental aspect of effective breastfeeding23. While the entire sample
in McLaughlin et al.’s study11 identified that the baby should
have as much as the mother’s areola in their mouth as possible, only 48% of their sample were able to correctly identify that audible swallowing was also an indicator of effective milk transfer. The participants unanimously correctly answered the attachment questions in this study, which is clinically important considering the importance of this component of breastfeeding knowledge.
Similarly, maintenance of maternal milk supply is often a key issue during the acute illness phase for an infant, when maternal willingness or ability to breastfeed directly may be impaired (for example, infant nil by mouth). The improved knowledge of lactation maintenance and the use of hand or electric expression to maintain supply is a particularly important clinical practice improvement supported by the implementation of the breastfeeding management resource kit, and should secure the re-establishment of breastfeeding, if interrupted by infant illness.
Correct identification by 100% of the participants that breastfeeding assists in reducing the risk of common paediatric illnesses is a positive finding. The paired data comparison also demonstrated a statistically significant improvement in the nurses’ knowledge that breastfeeding reduces the risk specifically of otitis media, enabling paediatric nurses to convey this health promotion message to families of unwell or vulnerable infants in their care.
Knowledge improvements were also present in the management and storage of expressed breast milk. Provision of evidence-based information and practical advice to parents while their infant is unable to directly breastfeed is an important role of paediatric nurses, and will encourage ongoing breastfeeding.
Areas for further improvement in breastfeeding
knowledge
Human breast milk differs markedly from all substitute infant feeding preparations, making it uniquely superior to alternatives2. In this study, very limited improvement
was demonstrated in the nurses’ understanding that infant artificial formula is not equivalent to breast milk, with only about half (56.5%) in the post-test survey identifying the correct response. This belief is held amongst many health care professionals in developed countries, with the attitude that breastfed infants are only marginally different from their artificially fed counterparts7.
The duration and exclusivity of breastfeeding, in accordance with recommendations, is directly influenced by the attitudes of health care professionals working with families. Taveras and colleagues24 found that clinicians (both medical and nursing)
did not believe that their advice to breastfeeding mothers on how long they should exclusively breastfeed their babies was very important, yet mothers were in fact influenced by the attitudes health professionals held toward aspects of infant feeding, such as artificial formula supplementation. An American study found a perceived neutral attitude from hospital staff regarding breastfeeding to be directly related to not breastfeeding beyond six weeks, particularly in mothers who had intentions while pregnant to only breastfeed for a short time25. This ambivalence towards the harm of
artificial feeding is influenced by the absence of lactation management education in health care professional curricula, and subsequent paucity of breastfeeding management skills among health care professionals7.
On the contrary, when education, even brief, is provided to health care professionals, improvements emerge in breastfeeding rates and duration. A French randomised trial provided a short training programme for primary care practising physicians in breastfeeding management. Those mothers who attended the routine, follow-up visits for newborn health checks with physicians trained in the breastfeeding skills were more likely to report exclusive breastfeeding at four weeks and overall reported increased breastfeeding duration than the control group18. Similarly, a
self-paced study module, which was guided by an on-site, trained staff member was found to be a cost-effective strategy for improving nurses’ knowledge of breastfeeding, and deemed a good fit for busy work schedules19.
In our study a basic education series and pragmatic resource kit was seen to improve paediatric nurses’ knowledge of breastfeeding in some areas; however, it was beyond the scope of this study to examine the impact this had on Table 3: Reasons to cease breastfeeding
INFANT CONDITION/
CIRCUMSTANCE Correct responsesPre-test (n=49)†
n (%) Correct responses Pre-test (paired)‡ (n=23) n (%) Correct responses Post-test (paired)‡ (n=23) n (%) Difference p* Infant is in hospital 39 (79.6) 19 (82.6) 20 (87) p=0.63 Infant is teething 35 (71.4) 17 (73.9) 19 (82.6) p=0.5
Infant has frequent, loose
stools 36 (73.5) 16 (69.6) 18 (78.3) p=0.63
Infant has an infection 39 (79.6) 18 (78.3) 20 (87) p=0.63
Infant appears to be
continually hungry/unsatisfied 37 (75.5) 18 (78.3) 21 (91.3) p=0.38
Mother has sore nipples 25 (51) 13 (56.5) 15 (65.2) p=0.69
Mother has mastitis 26 (53.1) 11 (47.8) 12 (52.2) p=1.00
Mother is tired 35 (71.4) 17 (73.9) 18 (78.3) p=1.00
†using all data available from pre-test respondents (n=49)
‡using data from nurses who responded to both pre- and post-test questionnaires (n=23) *p values were calculated on the change of knowledge using the Wilcoxon signed ranks test
in-patient and discharge breastfeeding rates. This is an area identified for further research.
Personal experience as source for breastfeeding
knowledge
In this study very few participating nurses reported having breastfeeding-related qualifications. The most often cited source of breastfeeding knowledge was personal experience (53.1%) and advice from professional colleagues (n=28, 57.1%). This finding is similar to other studies investigating where health professionals source their breastfeeding knowledge. A US study found that while paediatric nurses (n=95), had positive beliefs overall towards breastfeeding, their knowledge regarding specific management strategies was limited, with close to 75% of the cohort naming their own personal breastfeeding experience as their most valuable source of breastfeeding knowledge20. Another relatively large North American study
(n=405) of nurse practitioners and nurse midwives, working directly with mothers of young infants, found that nearly 73% had breastfed (or their partner), and of these 24% indicated that it was this experience which had taught them the most about breastfeeding21. General practitioners in an Australian
study also identified personal (or partner) experience as their most useful source of breastfeeding knowledge6, with
other international studies finding personal experience as the number one source of breastfeeding knowledge22. Whilst
personal experience is one valid way of knowing in health care, it is not necessarily the best or most comprehensive source from which to draw, when specific or complex breastfeeding management strategies are required. This is demonstrated in the knowledge areas incorrectly answered by the participants in this study, specifically in the areas of supportive advice, such as mastitis management and care of sore and damaged nipples.
Strengths and limitations
This study has reported the development of an acceptable and feasible resource kit of educational tools to support paediatric nurses developing practical skills to sustain breastfeeding of infants in an acute care setting. The pilot implementation of the resource kit was successful, and kits were made available in all hospital in-patient settings in collaboration with the nurse education team. Changes in the knowledge of the paediatric nurses was conservative, with significant improvements identified in only eight of the 29 knowledge areas. Further evaluation is required following implementation across the institution, and assessment of any effect on in-patient and discharge breastfeeding rates.
Conclusion
An important aspect of everyday nursing care in paediatric acute care facilities is the support and care of breastfeeding families. This paper has described the implementation and effectiveness of a pilot breastfeeding education series and resource kit for paediatric nurses working in a large, metropolitan, tertiary children’s hospital. While improvements in aspects of breastfeeding knowledge and management were identified, areas for ongoing education and knowledge development were also identified, such as knowledge of the harms of not breastfeeding.
Implications for clinical practice
The improved breastfeeding knowledge and practical skills of paediatric nurses will promote the continuation of breastfeeding of the hospitalised infant. Given the recognised short- and long-term benefits of breast milk for infants, optimising this education and support to nurses who provide care to breastfeeding families is essential. A hospital-wide implementation of the breastfeeding resource kits has occurred based on these pilot outcomes. A statewide breastfeeding policy and practice standard is also now available to all nursing staff, with strong links promoting the continuum of care between acute and community services. Evaluation of this targeted education series and resource kit is required to fully optimise paediatric nursing support for breastfeeding mothers of sick infants.
Acknowledgements
This project was funded through a Nursing Research Project Grant, donated by the Royal Children’s Hospital Foundation (Qld) (Grant number 10245). We would also like to thank Dr Robert Ware, Biostatistician, Queensland Children’s Medical Research Institute, University of Queensland for his contributions to the statistical analyses.
References
1. World Health Organization. Infant and Young Child Feeding: Model chapter for textbooks for medical students and allied health professionals. Geneva: WHO Press; 2009. 2. American Academy of Pediatrics. Breastfeeding and the use of human milk: Policy
statement. Pediatrics. 2005;115(2):496–506.
3. Australian Institute of Health and Welfare. 2010 Australian National Infant Feeding Survey: Indicator Results. Canberra: Australian Institute of Health and Welfare; 2010.
4. Australian Institute of Health and Welfare, editor. Australia’s Health 2012. Australia’s health no. 13. Cat no. AUS 156. Canberra: Australian Institute of Health and Welfare; 2012. 5. Renfrew M, McCormick F, Wade A, Quinn B, Dowswell T. Support for healthy breastfeeding
mothers with healthy term babies. Cochrane Database Syst Rev. 2012;5.
6. Brodribb W, Fallon A, Jackson C, Hegney D. Breastfeeding knowledge: the experiences of Australian general practice registrars. Aust Fam Physician. 2009;38(1/2):26–9. 7. International Lactation Consultant Association. Clinical Guidelines for the Establishment
of Exclusive Breastfeeding. Raleigh, NC: International Lactation Consultant Association; 2005.
8. Spear H. Baccalaureate nursing students’ breastfeeding knowledge: A descriptive study. Nurse Educ Today. 2006;26:332–7.
9. Lau C, Hurst N, Smith E, Schanler R. Ethnic/racial diversity, maternal stress, lactation and very low birthweight infants. J Perinatology. 2007;27(7):399–408.
10. Page-Goertz S, Riordan J. The ill child: breastfeeding implications. In: Riordan J, Wamabach K, editors. Breastfeeding and Human Lactation. 4th ed. Sudbury: Jones and Bartlett Publishers; 2010.
11. McLaughlin M, Fraser J, Young J, Keogh S. Paediatric nurse’s knowledge and attitudes related to breastfeeding and the hospitalised infant. Breastfeeding Review. 2011;19(3):11– 22.
12. Cantrill R, Creedy D, Cooke M. An Australian study of midwives’ breastfeeding knowledge. Midwifery. 2003;19(4):310–7.
13. Brodribb W, Fallon A, Jackson C, Hegney D. Breastfeeding and Australian GP registrars — Their knowledge and attitudes. J Hum Lact. 2008;24(4):422–30.
14. Smillie C. Baby-Led Breastfeeding ... The Mother–Baby Dance; 2007.
15. International Lactation Consultant Association. Clinician’s Breastfeeding Triage Tool. Morrisville, NC: ILCA; 2007.
16. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. 17. Brill J. Likert Scale. Encyclopedia of Survey Research Methods. 2008:428–30.
18. Labarere J, Gelbert-Baudino N, Ayral A, Duc C, Berchotteau M, Bouchon N et al. Efficacy of breastfeeding support provided by trained clinicians during an early, routine, preventive visit: A prospective, randomized, open trial of 226 mother–infant dyad pairs. Pediatrics 2005;115:e139–e46.
19. Bernaix L, Beaman M, Schmidt C, Harris J, Miller L. Success of an educational intervention on maternal/newborn nurses’ breastfeeding knowledge and attitudes. J Obstet Gynecol Neonatal Nurs. 2010;39(6):658–66.
20. Hellings P, Howe C. Breastfeeding knowledge and practice of pediatric nurse practitioners. J Pediatr Health Care. 2004;18(1):8–14.
21. Hellings P, Howe C. Assessment of breastfeeding knowledge of nurse practitioners and nurse-midwives. J Midwifery Womens Health. 2000;45(3):264–70.
22. Finneran B, Murphy K. Breast is best for GPs — or is it? Breastfeeding attitudes and practice of general practitioners in the Mid-West of Ireland. Ir Med J. 2004;97(9):268–70. 23. Riordan J, Wamabach K, editors. Breastfeeding and Human Lactation. 4th ed. Sudbury:
Jones & Bartlett Publishers; 2010.
24. Taveras E, Li R, Grummer-Strawn L, Richardson M, Marshall R, Rego V et al. Opinions and practices of clinicians associated with continuation of exclusive breastfeeding. Pediatrics. 2004;113:e283–e90.
25. DiGirolamo A, Grummer-Strawn L, Fein S. Do perceived attitudes of physicians and hospital staff affect breastfeeding decisions? Birth 2003;30(2):94–100.