Management of Bariatric Surgery Patients: Implications for Pharmacy Practice Learning Objectives
1. Review the epidemiology, associated complications, and treatment options related to obesity
2. Understand selection criteria in assessing candidates for bariatric surgery 3. Discuss the risk and benefits of bariatric surgery
4. Outlines the various types of bariatric surgery procedures
5. Discuss various micronutrient deficiencies associated with bariatric surgery including proper monitoring and supplementation
6. Define the role of the pharmacists in the management of bariatric surgery patients
Obesity: Impact and Treatment
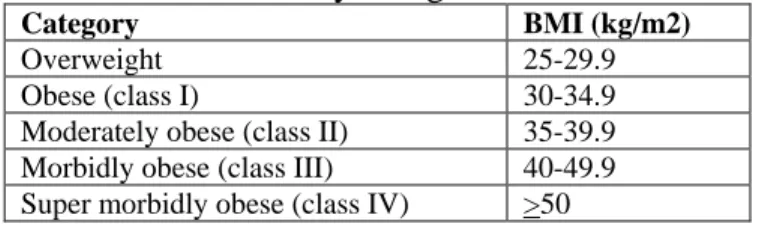
Obesity is a major health concern in the United States and throughout the Western world. Obesity is defined as a body mass index (BMI) of greater than 30 kg/m2 and can be further subdivided into various obesity classes (Table 1). Obesity is a chronic health condition that has been increasing in prevalence over the last several decades, with the percent of obese American adults rising from 15.3% in 1995 to 23.9% in 20051. In 2007, it was estimated that approximately 61 million American adults were considered obese, which is nearly one-third of the American population1. Moreover, 4.8% of the obese population are classified as morbidly obese1. Obesity is a major health concern not only due to the rapid rise in prevalence due to the morbidity, mortality, and economic impact associated with obesity. In 2005, it was estimated that the total cost of obesity in the United States was one-hundred billion dollars, with approximately half of that total relating to direct medical costs2. The cost of the obesity epidemic extends beyond
monetary costs, however. Obesity is the second most common preventable cause of death in the United States according to the Centers for Disease Control and Prevention, with only smoking causing more American deaths than obesity3. Deaths attributed to obesity in the United States have been estimated to be 280,000 to 325,000 people annually4. The life expectancy of an obese individual is severely reduced, with a twenty-five year old morbidly obese male expecting to lose twelve years of life expectancy1. Obesity is related to a myriad of medical conditions that contribute to the reduction in life expectancy, quality of life, and cost associated with obesity. Obese individuals have an increased risk of type 2 diabetes mellitus, hypertension, arthritis, sleep apnea, certain types of cancers, depression, asthma, coronary heart disease, gastroesophageal reflux disease (GERD), hypercholesterolemia, infertility, osteoporosis, cerebrovascular accident (CVA), and pulmonary hypertension1.
Table 1: Adult Obesity Categories based on BMI1
Category BMI (kg/m2)
Overweight 25-29.9
Obese (class I) 30-34.9
Moderately obese (class II) 35-39.9 Morbidly obese (class III) 40-49.9 Super morbidly obese (class IV) >50
Any condition such as obesity, which carries significant morbidity and mortality, requires prompt and effective treatment. Management of obese patients is dictated mainly by their individual risk factors and the severity of their condition. Obesity management modalities may include lifestyle changes, including exercise and dieting, use of
pharmacological agents to aid in weight loss, and surgical options. Any treatment modality used in the treatment of obesity should be aimed at not only weight loss, but also reducing an individual’s risk of concurrent disease states and improving quality of life. Lifestyle changes alone produce poor long-term results. Pharmacological agents produce only modest weight loss and have various adverse effects. Generally, patients can expect to lose 10 to 12% percent of their initial weight over six to twelve months with lifestyle changes, with or without pharmacological agents5. However, most patients regain any weight lost within five years5. Bariatric surgery provides the most effective treatment for obesity producing significant results with 40 to 75% of excess body weight loss, depending on the specific procedure performed5. Moreover, 70% of patients
undergoing certain bariatric procedures sustain 50% excess weight loss for at least 5 years following surgery5. However, the most significant outcome attributed to weight loss seen with bariatric surgery is the drastic improvement in obesity-related conditions. Bariatric surgery patients have a significantly reduced risk of conditions including infectious disease, musculoskeletal issues, respiratory conditions, and psychiatric
disorders1. In patients with type 2 diabetes mellitus, a recent meta-analysis indicated that bariatric surgery lead to resolution of the clinical and laboratory manifestations of
diabetes in 82% of patients in the first two years after surgery6. Moreover, this result was sustained in 62% of patients more than 2 years after surgery6. Cardiovascular benefits seen with bariatric surgery include improvement in blood pressure control, improved ventricular function, and sustained normalization of lipid profiles5. Apenic episodes associated with obstructive sleep apnea are reduced in the majority of patients following bariatric surgery and eliminated in 40% of patients5. A study investigating medication use after bariatric surgery found significant reductions in the number of mediations used to treat hypertension and diabetes following surgery7. Improvements in mortality rates following bariatric surgery have also been observed. In a study following patients for six years after bariatric surgery, patient undergoing surgery had a mortality rate of 9% compared to 28% in individuals who were approved for surgery but did not undergo the procedure5. Moreover, in the same study, it was concluded for each year of follow-up, bariatric surgery patients had a 1% mortality rate compared to 4.5% in patients not undergoing surgery5. Lastly, bariatric surgery may offer financial benefits in improved productivity and reduction in health care expenditures. One study found 45% of patients previously on public assistance found full or part-time employment following surgery, while another study indicated that that bariatric surgery pays for itself in approximately 3 years due to reductions in health care expenditures5. With the rapid rise in the number of obese patients and the potential benefits offered through bariatric surgery, it is no surprise that the number of bariatric procedure performed has increased dramatically in the past several years. Approximately 10,000 bariatric procedures were performed in the early 1980’s4, followed by an escalating number of cases, with approximately 16,000 surgeries in the early 1990’s7, 103,000 surgeries in 20038, and 177,600 surgeries in 20069.
Bariatric surgery is an option for the treatment obesity in certain patients. According to a 1991 National Health Institute Health Consensus Development
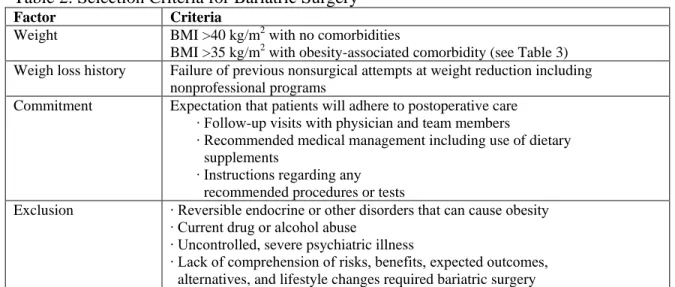
Conference, bariatric surgery should be considered in patients with either a BMI over 40 kg/m2 or patients with BMI over 35 kg/m2 with co-existing medical conditions1. These criteria form the basis for several guidelines for the treatment of obesity, including guidelines endorsed by the National Heart, Lung, and Blood Institute, American Society for Bariatric Surgery, American Association of Clinical Endocrinologists (AACE), the Obesity Society (TOS), and the American Society of Metabolic and Bariatric Surgery (ASMBS)1,10. The American College of Physicians took a more conservative approach to bariatric surgery, recommending the procedure only in individuals with BMI over 40 kg/m2 and a coexisting medical condition1. However, in 2004, a National Coverage Advisory Committee indicated that bariatric surgery could be offered to Medicare beneficiaries with a BMI of 35 kg/m2 or greater with at least one obesity-related co-morbidity10. Additional selection criteria endorsed by the recent AACE/TOS/ASMBS guidelines are listed in Table 2 and are typical of other guidelines on the management of bariatric surgery patients.
Table 2: Selection Criteria for Bariatric Surgery10
Factor Criteria
Weight BMI >40 kg/m2 with no comorbidities
BMI >35 kg/m2 with obesity-associated comorbidity (see Table 3) Weigh loss history Failure of previous nonsurgical attempts at weight reduction including
nonprofessional programs
Commitment Expectation that patients will adhere to postoperative care ∙ Follow-up visits with physician and team members
∙ Recommended medical management including use of dietary supplements
∙ Instructions regarding any recommended procedures or tests
Exclusion ∙ Reversible endocrine or other disorders that can cause obesity ∙ Current drug or alcohol abuse
∙ Uncontrolled, severe psychiatric illness
∙ Lack of comprehension of risks, benefits, expected outcomes, alternatives, and lifestyle changes required bariatric surgery
Table 3: Obesity-associated Comorbidities10
Coronary artery disease Type 2 diabetes mellitus Obstructive sleep apnea (OSA)
Obesity-hyperventilation syndrome (OHS)
Pickwickian syndrome (combination of OHS and OSA) Non-alcoholic fatty liver disease
Hypertension Dyslipidemia
Gastroesophageal reflux disease (GERD) Pseudotumor cerebri
Venous stasis disease Severe urinary incontinence Debilitating arthritis
Types of Bariatric Surgeries
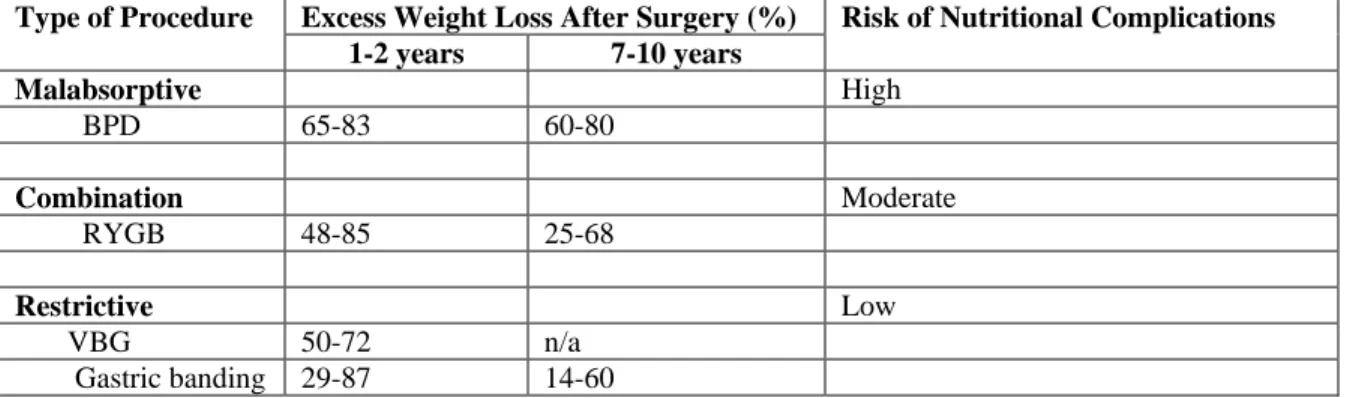
The term bariatric surgery encompasses a number of a variety of procedures. These procedures differ not only in the methods used to induce weight loss, but also differ in terms of the complications and expected weight. In general, procedures are generally categorized into three types: malabsorptive, restrictive, or combination procedures. A comparison of the various bariatric surgery procedures in terms of expected weight loss and complication risk is outlined in Table 4.10
Malabsorptive procedures evolved from the first bariatric procedure, the jejunoileal bypass, which involved simply creating a connection between the proximal jejunum and the terminal ileum2. However, this procedure had a high rate of
complications and is no longer performed. Bilopancreatic diversion (BPD) with or without a duodenal switch involves removal of a portion of the stomach and creation of a small gastric pouch. The gastric pouch is then connected to a distal portion of the small intestine, limiting absorption and digestion to a short segment, or common channel, prior to passing to the large intestine1,10. Weight loss is induced mainly due to protein and calorie malabsorption10. BPD is rarely performed currently due to the high rate of nutrient and metabolic complications associated with this procedure1.
Restrictive procedures involve restricting the storage capacity of the stomach, which limits food intake and produces satiety. A vertical banded gastroplasty (VBG) is a restrictive procedure involving the use of a stapling procedure to create a small gastric pouch and using a mesh band to create a stoma, or outlet, to the remaining stomach. VBG was associated with various complications and often lead patients to eat high-calorie liquids due to inability to eat larger, solid meals2. Moreover, long term weight loss with VBG is disappointing; one study showed no patients maintained 50% excess weight loss at 5 years after surgery2. VBG has largely been replaced by another restrictive procedure, laparoscopic adjustable gastric banding (LAGB). In LAGB, a prosthetic band encircles the stomach to create a gastric pouch. The band is connected to a subcutaneous port, which allows for adjustment of the size of the gastric pouch1. LAGB has unique
complications including band slippage, band erosion, and port infections10. Also, in one study, nearly 35% of patients had undergone conversion to gastric bypass procedures within 5 years of the LAGB procedure2.
Gastric bypass or Roux-en-Y gastric bypass (RYBG) is a combination procedure involving the creation of gastric pouch, which is then connected to Roux limb, allowing bypass of a portion of the small intestine1. Modifications involve lengthening the Roux limb to increase the malaborptive component on a RYGB procedure2. RYBG is the most commonly performed bariatric surgery in the United States10.
Bariatric procedures, such as the RYBG and BPD, may also be performed laparoscopically, which reduces wound complications and allows shorter hospital stays and quicker postoperative recovery. However, higher rates of certain surgical
complications occur with laparoscopic procedures, such as anastomatic strictures and bowel obstructions. Regardless, most bariatric procedures today are being performed laparoscopically10.
Table 4: Comparison of Bariatric Surgery Procedures10
Type of Procedure Excess Weight Loss After Surgery (%) Risk of Nutritional Complications 1-2 years 7-10 years Malabsorptive High BPD 65-83 60-80 Combination Moderate RYGB 48-85 25-68 Restrictive Low VBG 50-72 n/a Gastric banding 29-87 14-60
Bariatric Surgery Complications
Bariatric surgery is not a “quick fix” for obesity. Bariatric surgery patients must be willing to comply and participate in extensive, and often indefinite, postoperative care. Patients must understand not only care plans required following surgery, but also the risks and benefits of undergoing bariatric surgery. The benefits of bariatric surgery have been previously discussed and are significant with proper follow-up and postoperative care. Bariatric surgery, much like any other medical procedures or treatment modalities, carries certain risks. The mortality rate associated with bariatric surgery is estimated at 0.1 to 0.2%, with pulmonary embolism (PE) and serious surgical complications, such as anastomotic leak, being the most common causes of death following surgery1.
Anastomotic leak carries up to a 30% mortality rate following RYGB, but is relatively rare, occurring in 0 to 4.4% of cases11. The risk of thromboembolism is higher in obese patients in general and the rate of PE following RYGB is estimated at 0 to 1.1%11. Bariatric surgery patients should receive routine thromboembolism prophylaxis, including sequential compression devices and the use of subcutaneous unfractionated heparin or low-molecular weight heparin agents10. The AACE/TOS/ASMBS advocated prophylaxis for three days before and after surgery or until the patient is ambulatory10. Certain risk factors increase the mortality associated with bariatric surgery including an inexperienced surgeon, advance patient age, male sex, BMI >50 mg/k2, and co-existing medical conditions1. The Swedish Obese Subjects (SOS) Trial indicated postoperative complications occurred in 13% of patients (0.5% of patients experiencing bleeding, 0.8% of patients experiencing embolism or thrombosis, 1.8% experiencing wound
complications, and 6.1% of patient experiencing pulmonary complications)1.
Various gastrointestinal complications can occur following bariatric surgery. Rapid weight loss following bariatric surgery is associated with a rise in the incidence of cholelithiasis, with 38 to 52% of patients developing cholelithiasis within one year of surgery11. In fact, prophylactic cholecystectomy at the time of bariatric surgery is a highly debated topic due to the high incidence of undiagnosed gallbladder disease in the obese population. For patients not undergoing cholecystectomy during bariatric surgery, supplementation with ursodiol is often advised for six months following bariatric surgery to decrease the incidence of gallstone formation10. Dumping syndrome, including
symptoms such as flushing, lightheadedness, fatigue, and diarrhea when ingesting meals high in carbohydrates, occurs in 70-76% of RYGB patients10. Dumping syndrome can
often be managed by nutritional changes such as eating small, frequent meals, avoiding liquids for 30 minutes prior to a meal, and avoiding simple sugars in meals10. Vomiting is also a common complication following bariatric surgery, mainly occurring early in the postoperative period. Persistent vomiting occurring six months or more following surgery may indicate surgical complications such as obstruction, ulceration, reflux, inflammation, or gastric dysmotility, and requires additional follow-up and evaluation10.
Diarrhea and steatorrhea occur frequently in patient undergoing BPD or BPD/DS, but is less common after RYGB procedures and is often an indication of macronutrient
deficiencies or other issues, including bacterial overgrowth10. Bacterial overgrowth can easily be treated with empiric antibacterial therapy with metronidazole10. Persistent or severe gastrointestinal symptoms may also indicate the presence of additional
complications including stomal stenosis or ulceration, often due to anastomotic ischemia, Helicobactor pylori infection, or use of certain medications including non-steroidal anti-inflammatory drugs (NSAIDS)10.
Pregnancy following bariatric surgery is discouraged for twelve to eighteen months following surgery due to rapid weight loss. However, because obesity is often associated with impaired fertility, weight loss following surgery may also improve a patient’s ability to conceive. Contraceptive choice following bariatric surgery is further complicated by concerns regarding decreased effectiveness of oral contraceptives due to alternations in enterohepatic recycling following surgery12. Patients may consider using alternative contraceptive options or non-oral routes of administration for hormonal contraceptives12. Pregnancy following bariatric surgery requires careful evaluation prior to conception and throughout pregnancy, although the weight loss following bariatric surgery reduces the risk of several pregnancy-related complications including gestational diabetes, preeclampsia, and cesarean delievery10.
Psychological issues following bariatric surgery are also important to consider. Patients often report improvement in anxiety and depression following surgery as well as an apparent reduction in psychiatric conditions. However, these improvements seem to wane within two to three years following surgery. Some studies have reported issues with substance abuse, alcoholism, and suicide following bariatric surgery, although such issues have occurred in a small number of patients and the factors leading to these outcomes are unclear currently10.
Nutritional issues also occur following bariatric surgery. Following surgery, patients must slowly progress to solid food, usually beginning with clear liquids within twenty-fours after surgery followed by a standardized meal progression, often including consultation with a registered dietitian. Generally, once able to tolerate solid meals, patients are encouraged to eat small, frequent meal, chew food thoroughly, and avoid drinking beverages while eating solid foods10. Food intolerance, particularly to meat products, is common, leading to protein malnutrition in up to 13% of patients undergoing long-limb RYGB procedures. Protein malnutrition is the most common macronutrient complication associated with bariatric surgery and necessitates regular monitoring of protein intake and nutritional intake as well as possible protein supplementation or, at the least, encouragement of the ingestion of protein-rich foods10. Micronutrient deficiencies are also a large concern following BPD and RYGB bariatric surgery due to both changes in food intake and changes in gastrointestinal anatomy. Micronutrient deficiencies can
lead to skeletal complications, anemia, neurologic issues, and other issues and necessitate ongoing supplementation10.
Micronutrient Deficiencies and Associated Complications
Recommendations from the AACE/TOS/ASMBS guidelines for micronutrient screening and supplementation are discussed below. It should be noted that these recommendations only represent one of many guidelines available regarding supplementation in bariatric patients. Although guideline recommendations vary in regard to supplementation, the AACE/TOS/ASMBS offer recent, comprehensive guidance for the management of bariatric patients, including micronutrient supplementation 10.
All patients undergoing bariatric surgery should receive a daily multivitamin containing the recommended daily allowance (RDA) for vitamins and minerals as well as supplementation with calcium 1200-2000 mg per day and vitamin D 400-800 mg per day. In patients undergoing malabsorptive procedures, additional supplementation with iron 40 to 65 mg per day, and vitamin B12 350 micrograms per day (or more) is also recommended. In general, multivitamin supplements are better tolerated as a chewable formulation and should contain at least 400 micrograms per day of folic acid.
Skeletal complications related to issues with micronutrient deficiencies are an ongoing concern in many bariatric surgery patients, but have not been documented following LAGB surgery. Calcium deficiency and metabolic bone disease can occur in patient undergoing RYGB or BPD for a variety of reasons including decreased intake of calcium-containing foods, bypassing of calcium absorption sites in the duodenum and proximal jejunum, and vitamin D deficiency. Vitamin D deficiency is often due to decreased sunlight exposure, decreased absorption in proximal small intestine, and poor mixing of pancreatic and biliary secretions. Moreover, rapid weight loss is associated with bone loss. Secondary hyperparathyroidism can occur following both RYGB and BPD procedures due to low vitamin D levels, which leads to reduced calcium absorption and subsequent increase in parathyroid hormone (PTH). PTH allows the conversion of vitamin D to its active form and increase intestinal absorption of calcium. If dietary calcium is not absorbed, due to decreased intake or impaired absorption (as in bariatric surgery), secondary parathyroidism ultimately leads to bone loss and increased the risk of developing osteoporosis13. Indeed, bariatric patients typically present with low serum and urine calcium levels, very low vitamin D levels, and high PTH levels14. Calcium
deficiency and vitamin D deficiency develop in a significant number of patients necessitating calcium and vitamin D supplementation. The AACE/TOS/ASMBS guidelines recommend calcium supplementation of 1200 to 2000 mg daily. Calcium citrate preparations are generally preferred because this salt form can be absorbed without gastric acid production. Vitamin D supplementation can be provided with ergocalciferol 50,000 units one to three times per week, although doses of 50,000 to 150,000 units daily may be needed in severe deficiency. Calcitriol may be used in cases when 25-hydroxy vitamin D (25-OHD) levels fail to normalize and PTH levels remain elevated despite supplementation. Adequate supplementation is indicated by normalization of serum calcium, 25-OHD, and twenty-four hour calcium excretion rates. PTH levels may remain elevated despite normalized 25-OHD levels. Also, bone density measurements are
recommended with use of dual-energy c-ray absorptiometry (DEXA) to monitor for the development of osteoporosis at baseline with a follow-up measurement at two years following surgery. Bisphosphonate therapy in patient with osteoporosis (T score -2.5 or below for the hip or spine) may be initiated after correction of calcium and vitamin D deficiency. Oral bisphosphonate therapy may lead to gastric ulceration, so intravenous agents may be preferred.
Low magnesium levels can lead to issues with PTH secretions and can occur following bariatric surgery and in cases of persistent diarrhea. However, supplementation with a multivitamin containing the RDA of magnesium is adequate to prevent deficiency.
Low phosphorus levels can also occur in the setting of malnutrition, vitamin D deficiency, and metabolic bone disease. Low phosphorus levels may neccsitate oral supplementation and dictates that nutrition support should be initiated cautiously to avoid re-feeding syndrome in severely malnourished bariatric surgery patients. Moreover, appropriate protein intake is also essential to maintaining bone health and is often a concern in bariatric patients14.
Fat-soluble vitamin deficiencies are not typically seen following RYGB or pure restrictive procedures. Steatorrhea following BPD can lead to deficiencies of fat-soluble vitamins including vitamin A, D, E and K. Vitamin A deficiencies can lead to night blindness and loss of vision. Following BPD, patients should be supplemented with 5000 to 25,000 units of vitamin A until levels are normalized. Prophylactic supplementation does not prevent development of deficiency in all patients, so routine monitoring is essential. Vitamin K deficiency leads to bleeding complications and may contribute to metabolic bone disease. Although routine screening is not recommended, vitamin K supplementation may be initiated when the international normalized ratio is above 1.4 or a level evaluated if bleeding issues or osteoporosis occurs. Vitamin E levels are usually normal in patient already using a multivitamin. Screening for vitamin E deficiency is not generally recommended. Signs of vitamin E deficiency include anemia and peripheral neuropathy. Although supplementation may be needed, supplementation should be completed with care to avoid potential exacerbation of bleeding complications associated with concurrent vitamin K deficiency.
Anemia is a common occurrence following bariatric surgery. Iron deficiency and associated anemia is common after RYGB and BPD, requiring prophylactic iron
supplementation. Iron deficiency occurs due to bypassing of the acid environment in the stomach and absorptive sites in the stomach, leading to decreased release and absorption of iron-containing heme. Moreover, food intolerance may lead to decreased intake of iron-containing food such as meat. Also, calcium supplementation decreases iron absorption. Thus, monitoring of iron status and supplementation is mandatory in all bariatric patients. Oral iron supplements containing 320 mg twice daily of elemental iron may be needed to prevent iron deficiency anemia, although lower doses of 80 mg daily may lower risk of iron deficiency. Vitamin C should be included with oral iron
supplements to improve absorption. Intravenous iron supplementation may be necessary in cases of continued deficiency or gastrointestinal side effects from oral supplements. Vitamin B12 deficiency can also occur following bariatric surgery due to impaired formation of intrinsic factor needed for absorption and decreased digestion of protein-bound cobalamins. Vitamin B12 storage in the body is substantial, but vitamin B12 deficiency has been reported within the first year following bariatric surgery. Initiation of
vitamin B12 supplementation within six months following surgery is generally recommended and monitoring for vitamin B12 deficiency is also recommended. Oral supplementation with 350 micrograms or more or intranasal supplementation with 500 micrograms weekly may be used. Parental supplementation with 1000 micrograms monthly may be used if oral supplementation is ineffective. Folate deficiencies are less common because folate is absorbed throughout the entire small intestine. Deficiency is unlikely if a multivitamin is consumed and routine monitoring is not necessary. Folate supplementation is especially critical in females of child-bearing age to prevent neural tube defects. Evaluation of other micronutrients known to cause anemia, including copper, vitamin A, vitamin B1, vitamin E, and selenium, may be needed when screening for iron, folate, and vitamin B12 is negative. Selenium is closely related to vitamin E status and, although selenium deficiency has been noted in bariatric patients, clinically significant symptoms or resultant anemia have not been reported. Copper deficiency has been described in bariatric patients, causing neurologic symptoms similar to vitamin B12 deficiency.
Zinc deficiency can occur with chronic diarrhea. Zinc supplementation can induce copper deficiency so empiric supplementation may lead to copper-related anemia.
Screening in BPD patient may be prudent. Symptoms of zinc deficiency are non-specific and include hair loss and rash.
Thiamine deficiency occurs during periods of continued vomiting or due to bypassing of absorption sites in the jejunum. Neurological symptoms are characteristic of thiamine deficiency and have been reported shortly following bariatric surgery. Routine screening for thiamine deficiency or additional supplementation is not needed in patients receiving multivitamin therapy, although patients with persistent vomiting warrant evaluation. Evaluation in certain clinical situations and early recognition of symptoms associated with thiamin deficiency are essential to initiating supplementation. Parenteral thiamine supplementation should be provided to patients with active neurological symptoms, such as Wernicke encephalopathy or peripheral neuropathy, with eventual change to oral therapy until symptoms resolve. Dextrose-containing solutions should be avoided in patients with thiamine deficiency to prevent aggravation of thiamine
deficiency. Moreover, persistent vomiting also should initiate an evaluation for surgical complications.
Role of the Pharmacist
The management of bariatric surgery patients requires a multi-disciplinary approach. Pharmacists have an important role to play in the management of bariatric surgery patients.
Prior to bariatric surgery, patient selection and counseling is essential to a successful outcome. A frank discussion with a pharmacist regarding need for life-long monitoring for micronutrient deficiencies and supplementation would certainly be prudent. Also, a discussion regarding the need for monitoring of current disease states and the possibility of decreasing patient’s medication burden following surgery may also be important. Obtaining baseline levels for micronutrients, including calcium, vitamin D, iron studies, as well as a baseline DEXA test is important for comparison following
surgery and, if the pharmacist will be monitoring micronutrient complications, the pharmacist should ensure these tests are complete prior to surgery
Following surgery, pharmacist can plan a large role in patient’s medication therapy. Immediately after surgery, while patients are unable to take medications by mouth, or during complications such as vomiting, alternative formulations may be necessary. Changing medications to more tolerable formulations may be helpful or the use of transdermal, parenteral, or rectal routes may be necessary. Also, because the dissolution and disintegration of tablets or capsules may be reduced, changing oral medications to solutions or suspensions may be desirable15. Alternatively, pharmacists may need to advise if medications may be crushed and mixed with food15. With improvement in chronic disease states such as diabetes and hypertension, continued monitoring and proper medication changes are often necessary. Pharmacists are ideally posed to aid in the monitoring and adjustment of patient’s medication postoperatively. Particular attention should be paid to the adjustment of diabetic and hypertensive medications requirements.
Micronutrient supplementation is essential following bariatric surgery. Pharmacist can play an important role in counseling and adjustment of micronutrient supplements. Compliance is a major concern regarding supplementation, so counseling regarding the purpose and importance of supplementation is essential. Moreover, helping patients choose high-quality, appropriately dosed supplements is also important as supplements are often available over-the-counter and can be overwhelming for patients to choose from.
Following bariatric surgery, many patients need to avoid or use certain
medications with caution. As mentioned previously, NSAID use should be avoided in bariatric patients due to an association with increased gastrointestinal side effects. Additionally, salicylates should also be avoided, although the risk and benefits of daily aspirin therapy in patients with diabetes or other conditions where such therapy is recommended should be considered on an individual basis8. Patients may require
alternatives for pain management including acetaminophen, opioids, and tramadol1. Oral bisphosphonates, although often required following bariatric surgery, may also increase gastrointestinal side effects, so alternative agents or administration routes may be used. Medications with more than two grams of sugar should also be avoided to prevent gastrointestinal issues1.
Absorption and bioavailability of certain medications may be altered following bariatric surgery due to changes in the intestinal length, absorptive surface area, and gastric emptying1,6. Absorption of medication requiring an acidic environment may also be altered due to decreased acidity in gastric pouch created during bariatric surgery8. Extended-release, delayed release, and enteric coated products should be avoid due to reduced or altered absorption. However, when immediate-release products are substituted more frequent dosing may limit compliance. Also, medications absorbed rapidly in the stomach or duodenum may exhibit decreased absorption following bariatric patients8. However, generally medication changes are not necessary in the absence of decreased efficacy or increased adverse effects8. Increased monitoring for therapeutic effects and toxicity is essential, particularly in regard to medications with a narrow therapeutic index. Examples of medications that have potential for decreased absorption following bariatric surgery are listed in Table 51,8. Lastly, medication dosing must be careful considered in
obese individuals and dose adjustments may be necessary with weight loss, particularly with medication dosed based on body weight.
Table 5: Examples of Medications with Potentially Decreased Absorption Following Bariatric Surgery1,8
Medication Absorption site Management
Cyclosporine ∙ Absorption impaired
∙ Consider alternative agents
Digoxin ∙ Monitor serum levels
Enalapril ∙ Hydrolyzed to active form in stomach
∙ Absorbed to small intestine
∙ May exhibit decreased activity ∙ Consider an alternative agents Ketoconazole ∙ Likely absorbed in stomach
∙ Acid required for absorption
∙ Absorption likely to be negligible ∙ Consider alternative agent Lamotrigine ∙ Likely in stomach and proximal
small intestine
∙ Rapid and complete absorption
∙ Monitor for decreased efficacy Metformin ∙ Slow and incomplete absorption in
duodenum
∙ Monitor blood glucose levels Metoprolol tartrate ∙ Rapid and complete absorption
∙ Likely in stomach and duodenum
∙ Monitor blood pressure
Niacin ∙ Primarily in duodenum ∙ Administer with low-fat snack to increase absorption
Olanzapine ∙ Stomach ∙ Monitor for decreased efficacy
∙ Oral-disintegrating tablets not alternative
Quetiapine fumarate ∙ Rapid absorption
∙ Likely stomach and duodenum
∙ Monitor for decreased efficacy
Ramipril ∙ Decreased absorption in
malabsorption
∙ Consider alternative agents ∙ Monitor blood pressure Simvastatin ∙ Hydrolysis in stomach to active
form
∙ Consider alternative agents ∙ Monitor serum lipids Zolpidem ∙ Rapid and complete absorption
∙ Absorption affected by food
∙ Absorption time may increase ∙ Delayed effect
∙ Take on empty stomach
Conclusions
Obesity is a growing epidemic in the United States and is associated with significant morbidity and mortality. Traditional treatments, including lifestyle changes and pharmacological treatments, are generally ineffective. Bariatric surgery offers an effective treatment for obesity in certain patients, producing significant, long-term weight loss and reduction in the complications associated with obesity, including improvements in concurrent disease states and life expectancy. However, bariatric surgery is not without risk and requires life-long lifestyle modifications. Pharmacists have an important role to play in the monitoring and adjustment of medication therapy in bariatric patients as well as counseling regarding essential micronutrient supplementation. Bariatric surgery patients require life-long medical management and a multi-disciplinary approach to therapy offers patients the best opportunity for successful outcomes following surgery.
Pharmacists are an essential component of this multi-disciplinary team and can improve outcomes in patients undergoing bariatric surgery.
References
1. Whipple Guthrie, E. Bariatric surgery: what all pharmacists need to know. US Pharm. 2007;32(9):HS27-HS37.
2. DeWald T, et. al. Pharmacological and surgical treatments for obesity. Am Heart J. 2006;151(3):604-624.
3. Sardo P, Walker JH. Bariatric surgery: impact on medication management. Hosp Pharm. 2008;43(2):113-120.
4. Koffman BM, et. al. Neurologic complications after surgery for obesity.
Neurologic complications after surgery for obesity. Muscle Nerve.2006;33:166-176.
5. Choban PS, et. al. Bariatric surgery for morbid obesity: why, who, when, how, where, and then what? Cleve Clinc J Med.2002;69(11):897-903.
6. Buchwalk H, et. al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med.2009;122:248-256.
7. Malone M, Alger-Mayer SA. Medication use patterns after gastric bypass surgery for weight management. Ann Pharmacother.2005;39:637-642.
8. Miller AD, Smith KM. Medication and nutrient administration considerations after bariatric surgery. Am J Health-Syst Pharm.2006;63:1852-1857.
9. Schweitzer DH, Posthuma EF. Prevention of vitamin and mineral deficiencies after bariatric surgery: evidence and algorithms. Obes Surg.2008;18:1485-1488. 10.Mechanick JI, et. al. American Association of Clinical Endocrinologists, The
Obesity Society, and American Society for Metabolic and Bariatric Surgery medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Surg Obes Relat Dis.2008;4:S109-S184.
11.Brethauer SA, et. al. Risks and benefits of bariatric surgery: current evidence. Cleve Clinic J Med. 2006;73(11):993-1007.
12.Bariatric surgery and medication use. Pharmacist’s Letter/Prescriber;s Letter 2009;25(11):251101.
13.Aills L, et. al. ASMBS allied health nutritional guidelines for the surgical weight loss patient. Surg Obes Relat Dis. 2008;4:S73-S108.
14.Williams SE, et. al. Perioperative management of bariatric surgery patients: focus on metabolic bone disease. Cleve Clinic J Med.2008;75(5):333-349.
15.Hunteman LM. Potential role of medication therapy management for bariatric surgery patients. J Am Pharm Assoc.2008;48(4):440,442.