THE PREVALENCE OF FOOT FUNGAL INFECTIONS AND THEIR ASSOCIATED FACTORS
AMONG THE DIABETIC PATIENTS ATTENDING MINISTRY OF HEALTH PRIMARY
HEALTH CARE
1, *
Alotaibi, N.A., Alghamdi, M.M. and Alharthi, A.H.
1
Family medicine Resident, King Abdulaziz University Hospital, Jeddah, Saudi Arabia
2Consultant Preventive Medicine, Ministry of Health, Jeddah, Saudi Arabia
3Consultant Family Medicine, Joint Program of Family Medicine, Jeddah, Saudi Arabia
ARTICLE INFO ABSTRACT
Background:
consequences in diabetic patients who are more susceptible to infection. The previous few researches carried out in Saudi Arabia recommended further studies to elaborate patter
in at risk group especially diabetic patients. Therefore, the current study aim to determine the prevalence of foot fungal infection and its associated factors among diabetic patients attending primary health care centers in Jed
diabetic patients were selected randomly from primary health care centers in Jeddah by multistage sampling. Interview questionnaire was used for the collection of the patient data and associate factors with foot fungal infection. In addition to demographic characteristics; clinical foot examination was done to detect foot fungal infection. Wagner scale was used in the presence of foot ulcer. Independent sample t test and chi square were used to
Out of all responding patients (200), females constituted (52%), male constituted 104(48%) their mean age accounted for 55.6±14.21 years, it ranged between 6
unemployed or retired
prevalence was significantly higher in older patients, unemployed or retired patients, those who had previous fungal infection and those who had hypertension; while it was lower in pat
take care regularly of their feet, regularly checking inside of the shoes and wearing socks p<0.05. Conclusion and recommendations:
diabetic patients attending primary health c
diabetic patients for foot fungal infection, and emphasize health education about foot care.
Copyright©2019, Alotaibi et al. This is an open access distribution, and reproduction in any medium, provided
INTRODUCTION
Foot fungal infection is a common health problem, clinicians are usually facing main two presentations of fungal infection of the feet: tinea pedis (athlete’s foot) and onychomycosis (nail infection). The estimated worldwide prevalence in gen population ranges between 15%-20% with often coexistence of
the two forms (Thomas et al., 2010). The most frequently
reported risk factors for foot fungal infection are humid warm climate, unhealthy life style and immune-compromised patients
(Assadamongkol et al., 2016). Among other factors
potentiating foot fungal infection, diabetes mellitus had been reported to increase likelihood of infection. In 2012, Bristow and Spruce emphasized the increased risk of foot fungal infection in diabetic patients if compared to otherwise healthy individuals, moreover, diabetic patients with foot fungal infection are more likely to develop complications, including
ISSN: 0975-833X
Article History:
Received 22nd March, 2019 Received in revised form 29th April, 2019
Accepted 25th May, 2019
Published online 30th June, 2019
Citation: Alotaibi, N.A., Alghamdi, M.M. and Alharthi, A.H.
patients attending ministry of health primary health care centers, Jeddah, 2018
Key Words:
Foot fungal Infections.
*Corresponding author: Alotaibi, N.A.,
RESEARCH ARTICLE
THE PREVALENCE OF FOOT FUNGAL INFECTIONS AND THEIR ASSOCIATED FACTORS
AMONG THE DIABETIC PATIENTS ATTENDING MINISTRY OF HEALTH PRIMARY
HEALTH CARE CENTERS, JEDDAH, 2018
Alotaibi, N.A., Alghamdi, M.M. and Alharthi, A.H.
Family medicine Resident, King Abdulaziz University Hospital, Jeddah, Saudi Arabia
Consultant Preventive Medicine, Ministry of Health, Jeddah, Saudi Arabia
edicine, Joint Program of Family Medicine, Jeddah, Saudi Arabia
ABSTRACT
Background: Foot fungal infection is a common health problem, that could result in serious consequences in diabetic patients who are more susceptible to infection. The previous few researches carried out in Saudi Arabia recommended further studies to elaborate patter
in at risk group especially diabetic patients. Therefore, the current study aim to determine the prevalence of foot fungal infection and its associated factors among diabetic patients attending primary health care centers in Jeddah. Subjects and Methods: Through a cross section design, 200 diabetic patients were selected randomly from primary health care centers in Jeddah by multistage sampling. Interview questionnaire was used for the collection of the patient data and associate factors with foot fungal infection. In addition to demographic characteristics; clinical foot examination was done to detect foot fungal infection. Wagner scale was used in the presence of foot ulcer. Independent sample t test and chi square were used to test for significant differences.
Out of all responding patients (200), females constituted (52%), male constituted 104(48%) their mean age accounted for 55.6±14.21 years, it ranged between 6
unemployed or retired (78%). Foot fungal infections were detected in 84(42%) of patients. The prevalence was significantly higher in older patients, unemployed or retired patients, those who had previous fungal infection and those who had hypertension; while it was lower in pat
take care regularly of their feet, regularly checking inside of the shoes and wearing socks p<0.05. Conclusion and recommendations: The prevalence of foot fungal infection is remarkably high in diabetic patients attending primary health care centers in Jeddah, We recommend regular checkup of diabetic patients for foot fungal infection, and emphasize health education about foot care.
access article distributed under the Creative Commons Attribution License, the original work is properly cited.
Foot fungal infection is a common health problem, clinicians are usually facing main two presentations of fungal infection of the feet: tinea pedis (athlete’s foot) and onychomycosis (nail infection). The estimated worldwide prevalence in general 20% with often coexistence of The most frequently reported risk factors for foot fungal infection are humid warm compromised patients Among other factors potentiating foot fungal infection, diabetes mellitus had been reported to increase likelihood of infection. In 2012, Bristow and Spruce emphasized the increased risk of foot fungal compared to otherwise healthy individuals, moreover, diabetic patients with foot fungal infection are more likely to develop complications, including
“secondary bacterial infections, foot ulcers, paronychias, cellulitis, osteomyelitis, gangrene, and low
(Bristow and Spruce
,
2009) that often result in recurrent andprolonged hospital admissions of diabetic patients
al., 2004). The World Health Organization (WHO) ranked
Saudi Arabia as the 7th highest country worldwide and the
second in the Middle East regarding prevalence of diabetic mellitus; it is estimated that there are about seven million individuals in Saudi Arabia living with diabetes and three million with prediabetes (Alwin
considering the worldwide prevalence of foot fungal infection in diabetic patients as being around 30%,
Scher and Baran, 2003) It is estimated that more than two million diabetic patients in Saudi Arabia would have foot fungal infection. Few researches were carried out in Saudi Arabia to demonstrate pattern of foot fungal infection; for example Abanmi and his colleagues (2009) found that the International Journal of Current Research
Vol. 11, Issue, 06, pp.4470-4479, June, 2019
DOI: https://doi.org/10.24941/ijcr.35452.06.2019
Alotaibi, N.A., Alghamdi, M.M. and Alharthi, A.H., 2019. “The prevalence of foot fungal infections and their associated factors among the diabetic patients attending ministry of health primary health care centers, Jeddah, 2018”, International Journal of Current Research
THE PREVALENCE OF FOOT FUNGAL INFECTIONS AND THEIR ASSOCIATED FACTORS
AMONG THE DIABETIC PATIENTS ATTENDING MINISTRY OF HEALTH PRIMARY
Alotaibi, N.A., Alghamdi, M.M. and Alharthi, A.H.
Family medicine Resident, King Abdulaziz University Hospital, Jeddah, Saudi Arabia
Consultant Preventive Medicine, Ministry of Health, Jeddah, Saudi Arabia
edicine, Joint Program of Family Medicine, Jeddah, Saudi Arabia
Foot fungal infection is a common health problem, that could result in serious consequences in diabetic patients who are more susceptible to infection. The previous few researches carried out in Saudi Arabia recommended further studies to elaborate pattern of foot fungal infections in at risk group especially diabetic patients. Therefore, the current study aim to determine the prevalence of foot fungal infection and its associated factors among diabetic patients attending Through a cross section design, 200 diabetic patients were selected randomly from primary health care centers in Jeddah by multistage sampling. Interview questionnaire was used for the collection of the patient data and associated factors with foot fungal infection. In addition to demographic characteristics; clinical foot examination was done to detect foot fungal infection. Wagner scale was used in the presence of foot test for significant differences. Results: Out of all responding patients (200), females constituted (52%), male constituted 104(48%) their mean age accounted for 55.6±14.21 years, it ranged between 6-89 years, and most of them were (78%). Foot fungal infections were detected in 84(42%) of patients. The prevalence was significantly higher in older patients, unemployed or retired patients, those who had previous fungal infection and those who had hypertension; while it was lower in patients who used to take care regularly of their feet, regularly checking inside of the shoes and wearing socks p<0.05. The prevalence of foot fungal infection is remarkably high in are centers in Jeddah, We recommend regular checkup of diabetic patients for foot fungal infection, and emphasize health education about foot care.
License, which permits unrestricted use,
“secondary bacterial infections, foot ulcers, paronychias, cellulitis, osteomyelitis, gangrene, and lower-limb amputation,” that often result in recurrent and
prolonged hospital admissions of diabetic patients (Musette et
The World Health Organization (WHO) ranked highest country worldwide and the second in the Middle East regarding prevalence of diabetic mellitus; it is estimated that there are about seven million individuals in Saudi Arabia living with diabetes and three
Alwin et al., 2017). When
considering the worldwide prevalence of foot fungal infection
in diabetic patients as being around 30%, (Dogra et al., 2002;
It is estimated that more than two million diabetic patients in Saudi Arabia would have foot Few researches were carried out in Saudi Arabia to demonstrate pattern of foot fungal infection; for example Abanmi and his colleagues (2009) found that the INTERNATIONAL JOURNAL
OF CURRENT RESEARCH
and their associated factors among the diabetic
prevalence of onychomycosis among attendants of dermatology
clinic in military hospital in Riyadh was (40.3%), (Abanmi et
al., 2008) meanwhile, Al Sheikh (2009) reported a much higher prevalence in the Easter province (71.54%) (Al Sheikh, 2009). The same researchers recommended further studies to elaborate pattern of foot fungal infections in other regions, and to put much concern on at risk group especially diabetic patients. Foot Fungal infections are a common complication for diabetic patients due to impairment in their immunity. They are mostly preventable and can be treated. Therefore, the current study aimed to determine the prevalence of foot fungal infection in diabetic patients and the factors associated with its occurrence, in an attempt to reduce its burden and serious consequences that could affect their quality of life by raising the awareness of the Diabetic Patients and their physicians regarding the importance of regular and proper foot examination
MATERIALS AND METHODS
Through a cross section design, 200 diabetic patients were selected randomly from primary health care centers in Jeddah by multistage sampling during September 2018. Interview questionnaire was used for the collection of the patient data and associated factors with foot fungal infection. In addition to demographic characteristics; clinical foot examination was done to detect foot fungal infection. Wagner scale was used in the presence of foot ulcer. Data entry and analysis was done by using the statistical products and services solution program (SPSS) version 21. Quantitative normally distributed variables were presented as means and standard deviation (SD), and qualitative variables were expressed as frequency and percentages. T test and chi square were used to explore statistical significance in differences of the subgroups. P value < 0.05 was considered as an indication for statistical significance. Independent sample t test and chi square were used to test for significant differences.
RESULTS
Demographic characteristics:Table 1 demonstrates that, Out
of all responding patients (200), females constituted (52%), male constituted 104(48%) their mean age accounted for 55.6±14.21 years, it ranged between 6-89 years, most of them were Saudi (86%). Thirds of them were (31%) are illiterate, while the (22%) had university and postgrad, the (18%) had primary, the (16%) had secondary, the (8%) are read & write, the (7%) had preparatory, and most of them were unemployed or retired (78%).
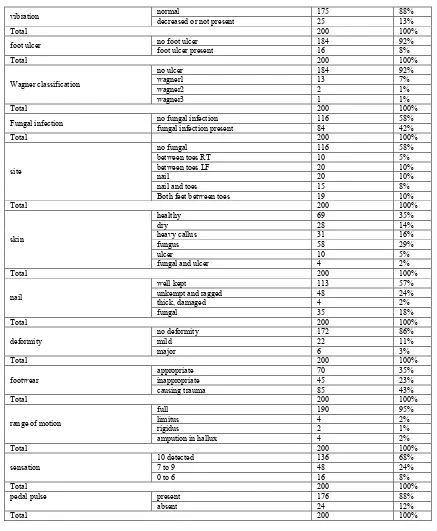
The prevalence of foot fungal infections among diabetic patients: Table 2 demonstrates that, the prevalence of foot fungal infections among diabetic patients.
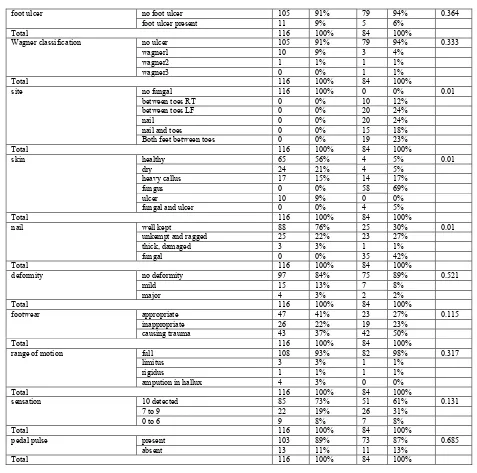
The factors of foot fungal infections for diabetic patients:
[image:2.595.325.538.66.262.2]Table 3 demonstrates that, there was a significant association between the Foot fungal infection with older age, unemployed or retired, oral hypoglycemic and insulin, Hypertension, Six times, previous foot treatment, current foot treatment, current history of foot fungal infection, and previous history of foot fungal infection. The sample of the study also found that it is possible to protect against foot fungal infections with Assign time for foot care always, Drying foot after washing it always, Checking the inside of the shoes always, Wearing socks always.
Table 1. Characteristics of the sample
Characteristics NO. %
Age:
Mean±SD 55.6±14.21
Gender male 96 48%
female 104 52%
Total 200 100%
Nationality Saudi 172 86%
none-Saudi 28 14%
Total 200 100%
level of education illiterate 62 31% read & write 15 8%
primary 35 18%
preparatory 14 7%
secondary 31 16%
university and postgrad 43 22%
Total 200 100%
Profession employed 45 23%
unemployed or retired 155 78%
Total 200 100%
DISCUSSION
Fungal infection of the foot is a common health problem, while it can be uncomfortable and cosmetically displeasing without any serious complications in otherwise healthy individuals, it can lead to secondary bacterial infections, foot ulceration, paronychia, cellulitis, osteomyelitis, gangrene and even lower
limb amputation in diabetic patients.( Armstrong et al., 2005).
Can the use of a topical antifungal nail lacquer reduce risk for diabetic foot ulceration? results from a randomised controlled pilot study. International wound journal, 2(2), 166-170. ) That could be attributed to the peripheral neurological and/or vascular abnormalities associated with diabetes mellitus (Chadwick, 2013). In Saudi Arabia, in addition to the high
prevalence of diabetes mellitus being ranked as the 7th country
worldwide, other factors potentiating foot fungal infection as warm humid climate, were the main rationale for conducting the current study, where 200 diabetic patients attending primary health care centers in Jeddah were investigated for foot fungal infection. Out of all diabetic patients investigated in the current study (n=200), foot fungal infections were observed in 84(42%) of them; which is much higher than what had been reported in the general population (15-20%), This differences
was explained by Joshi et al. (1999) who attributed the high
prevalence of fungal infection in diabetic patients to the “diabetic neuropathy with loss of sensible perceptions, impaired sudomotor activity and reduced secretion of sebum” which lead to a defect of the skin barrier with high risk of mycotic infections as well as bacterial super infections” (Joshi
et al., 1999). Comparing the prevalence of foot fungal infections in our diabetic patients with other countries with different climates, revealed a much lower prevalence in
Thailand (31.9%), (Assadamongkol et al., 2016) Mexico (28%)
(Manzano-Gayosso et al., 2008) and Denmark (22%), (Saunte
et al., 2006) which emphasize the role of humid warm climate characterizing the weather in Jeddah in increasing the
likelihood of fungal infection (Aljoufie, 2017).Another factor
might explain the relatively higher prevalence of foot fungal infection in our diabetic patients compared to other countries is the role of ablution. Ablution is a compulsory activity aimed to ensure cleanliness before prayers in Islam five times daily, where Muslims wash the hands, forearms, face and feet, nevertheless, if the feet are not dried carefully after ablution
(Johari et al., 2013) maintain moisture that potentiate
Table 2. The prevalence of foot fungal infections among diabetic patients
Variable NO. %
Duration of diabetes
<1 year 10 5%
1-4 year 41 21%
5-10 year 60 30%
11-15 year 35 18%
>15 54 27%
Total 200 100%
Duration of diabetes
Mean±SD 11.8±8.7
Total 200 100%
type of diabetes type1 18 9%
type2 182 91%
Total 200 100%
Medication
oral hypoglycemic 108 54%
oral hypoglycemic and insulin 66 33%
insulin 25 13%
none 1 1%
Total 200 100%
last HA1C % in 3 month Controlled 39 20%
uncontrolled 161 81%
Total 200 100%
Comorbidities
Hypertension 59 30%
dyslipidemia 26 13%
Hypertension and dyslipidemia 33 17%
Hypertensionand dyslipidemia and cardiac 24 12%
No comorbidity 58 29%
Total 200 100%
foot washing daily frequency
Once 8 4%
Twice 6 3%
three times 10 5%
four times 3 2%
five times 91 46%
Six times 50 25%
Seven times 18 9%
Eight times 10 5%
ten times 4 2%
Total 200 100%
type of foot wear
closed shoe 79 40%
open shoe 115 58%
diabetic shoes 6 3%
Total 200 100%
any current history of foot ulcer yes 19 10%
no 181 91%
Total 200 100%
any previous history of foot ulcer
yes 15 8%
no 185 93%
Total 200 100%
any previous foot treatment yes 48 24%
no 152 76%
Total 200 100%
any current foot treatment yes 29 15%
no 171 86%
Total 200 100%
any current history of foot fungal infection
yes 26 13%
no 174 87%
Total 200 100%
any previous history of foot fungal infection
yes 45 23%
no 155 78%
Total 200 100%
-history of vascular disease yes 29 15%
no 171 86%
Total 200 100%
history of neuropathy yes 99 50%
no 101 51%
Total 200 100%
did you receive any education on foot care in DM
yes 99 50%
no 101 51%
Total 200 100%
any daily foot care routine yes 85 43%
no 115 58%
Total 200 100%
Washing foot at least once daily yes 109 55%
no 91 46%
Total 200 100%
Drying foot after washing it yes 106 53%
no 94 47%
Total 200 100%
Not to walk barefooted yes 135 68%
no 65 33%
Total 200 100%
Care when clipping nails yes 141 71%
no 59 30%
Total 200 100%
Seeking medical advice when there is an ulcer
yes 167 84%
no 33 17%
Total 200 100%
-Having appropriate shoes size yes 137 69%
no 63 32%
Total 200 100%
Knowledge about shoes specifications yes 133 67%
no 67 34%
Total 200 100%
Daily checkup of the foot and Daily observation of foot to detect any ulcer
yes 116 58%
no 84 42%
Total 200 100%
Assign time for foot care
always 30 15%
often 15 8%
sometimes 43 22%
never 112 56%
Total 200 100%
Washing foot (Ablution at least once)
always 198 99%
sometimes 1 1%
never 1 1%
Total 200 100%
Drying foot after washing it
always 83 42%
often 7 4%
sometimes 25 13%
never 85 43%
Total 200 100%
Using skin lotion or olive oil for the foot
always 68 34%
often 12 6%
sometimes 68 34%
never 52 26%
Total 200 100%
Checking foot for presence of any ulcer
always 50 25%
often 18 9%
sometimes 76 38%
never 56 28%
Total 200 100%
Using a mirror for foot checkup
always 5 3%
often 3 2%
sometimes 4 2%
never 188 94%
Total 200 100%
Checking the foot by one of the family members
always 4 2%
often 8 4%
sometimes 25 13%
never 163 82%
Total 200 100%
Not to walk barefooted
always 92 46%
often 27 14%
sometimes 77 39%
never 4 2%
Total 200 100%
Wearing shoes
always 61 31%
often 29 15%
sometimes 62 31%
never 48 24%
Total 200 100%
-Checking the inside of the shoes
always 83 42%
often 11 6%
sometimes 46 23%
never 60 30%
Total 200 100%
Wearing socks
always 58 29%
often 25 13%
sometimes 63 32%
never 54 27%
Total 200 100%
vibration normal 175 88% decreased or not present 25 13%
Total 200 100%
foot ulcer no foot ulcer 184 92%
foot ulcer present 16 8%
Total 200 100%
Wagner classification
no ulcer 184 92%
wagner1 13 7%
wagner2 2 1%
wagner3 1 1%
Total 200 100%
Fungal infection no fungal infection 116 58%
fungal infection present 84 42%
Total 200 100%
site
no fungal 116 58%
between toes RT 10 5%
between toes LF 20 10%
nail 20 10%
nail and toes 15 8%
Both feet between toes 19 10%
Total 200 100%
skin
healthy 69 35%
dry 28 14%
heavy callus 31 16%
fungus 58 29%
ulcer 10 5%
fungal and ulcer 4 2%
Total 200 100%
nail
well kept 113 57%
unkempt and ragged 48 24%
thick, damaged 4 2%
fungal 35 18%
Total 200 100%
deformity
no deformity 172 86%
mild 22 11%
major 6 3%
Total 200 100%
footwear
appropriate 70 35%
inappropriate 45 23%
causing trauma 85 43%
Total 200 100%
range of motion
full 190 95%
limitus 4 2%
rigidus 2 1%
ampution in hallux 4 2%
Total 200 100%
sensation
10 detected 136 68%
7 to 9 48 24%
0 to 6 16 8%
Total 200 100%
pedal pulse present 176 88%
absent 24 12%
[image:5.595.79.516.48.579.2]Total 200 100%
Table 3 The factors of foot fungal infections for diabetic patients
Variables foot fungal infection
no fungal fungal present
NO. % NO. % p value
Age
Mean±SD 51.9±15.7 60.7±9.7 0.01
gender male 52 45% 44 52% 0.291
female 64 55% 40 48%
Total 116 100% 84 100%
nationality Saudi 100 86% 72 86% 0.539
none-Saudi 16 14% 12 14%
Total 116 100% 84 100%
level of education illiterate 34 29% 28 33% 0.534
read & write 6 5% 9 11%
primary 19 16% 16 19%
preparatory 9 8% 5 6%
secondary 20 17% 11 13%
university and postgrad 28 24% 15 18%
Total 116 100% 84 100%
profession employed 33 28% 12 14% 0.01
unemployed or retired 83 72% 72 86%
Total 116 100% 84 100%
Duration of diabetes
Mean±SD 11.3±7.99 12.6±9.6 0.306
Duration of diabetes <1 year 7 6% 3 4% 0.455
1-4 year 22 19% 19 23%
5-10 year 35 30% 25 30%
11-15 year 21 18% 14 17%
>15 31 27% 23 27%
Total 116 100% 84 100%
type of diabetes type1 18 16% 0 0% 0.913
type2 98 84% 84 100%
Total 116 100% 84 100%
medication oral hypoglycemic 64 55% 44 52% 0.01
oral hypoglycemic and insulin 33 28% 33 39%
insulin 19 16% 6 7%
none 0 0% 1 1%
Total 116 100% 84 100%
last HA1C % in 3 month Controlled 29 25% 10 12% 0.089
uncontrolled 87 75% 74 88%
Total 116 100% 84 100%
comorbidities Hypertension 25 22% 34 40% 0.01
dyslipidemia 14 12% 12 14%
hypertension and dyslipidemia 20 17% 13 15% hypertension and dyslipidemia and IHD 15 13% 9 11%
none of the above 42 36% 16 19%
Total 116 100% 84 100%
foot washing daily frequency Once 4 3% 4 5% 0.01
Twice 4 3% 2 2%
three times 9 8% 1 1%
four times 3 3% 0 0%
five times 53 46% 38 45%
Six times 23 20% 27 32%
Seven times 11 9% 7 8%
Eight times 7 6% 3 4%
ten times 2 2% 2 2%
Total 116 100% 84 100%
type of foot wear closed shoe 51 44% 28 33% 0.232
open shoe 61 53% 54 64%
diabetic shoes 4 3% 2 2%
Total 116 100% 84 100%
any current history of foot ulcer yes 12 10% 7 8% 0.245
no 104 90% 77 92%
Total 116 100% 84 100%
any previous history of foot ulcer yes 11 9% 4 5% 0.632
no 105 91% 80 95%
Total 116 100% 84 100%
any previous foot treatment yes 19 16% 29 35% 0.01
no 97 84% 55 65%
Total 116 100% 84 100%
any current foot treatment yes 12 10% 17 20% 0.05
no 104 90% 67 80%
Total 116 100% 84 100%
any current history of foot fungal infection yes 3 3% 23 27% 0.01
no 113 97% 61 73%
Total 116 100% 84 100%
any previous history of foot fungal infection yes 15 13% 30 36% 0.01
no 101 87% 54 64%
Total 116 100% 84 100%
-history of vascular disease yes 14 12% 15 18% 0.251
no 102 88% 69 82%
Total 116 100% 84 100%
history of neuropathy yes 59 51% 40 48% 0.651
no 57 49% 44 52%
Total 116 100% 84 100%
did you receive any education on foot care in DM yes 52 45% 47 56% 0.120
no 64 55% 37 44%
Total 116 100% 84 100%
any daily foot care routine yes 51 44% 34 40% 0.622
no 65 56% 50 60%
Total 116 100% 84 100%
Washing foot at least once daily yes 62 53% 47 56% 0.728
no 54 47% 37 44%
Total 116 100% 84 100%
Drying foot after washing it yes 61 53% 45 54% 0.890
no 55 47% 39 46%
Total 116 100% 84 100%
Not to walk barefooted yes 80 69% 55 65% 0.603
no 36 31% 29 35%
Total 116 100% 84 100%
Care when clipping nails yes 83 72% 58 69% 0.703
no 33 28% 26 31%
Total 116 100% 84 100%
Seeking medical advice when there is an ulcer yes 101 87% 66 79% 0.110
no 15 13% 18 21%
Total 116 100% 84 100%
-Having appropriate shoes size yes 81 70% 56 67% 0.635
no 35 30% 28 33%
Total 116 100% 84 100%
Knowledge about shoes specifications yes 78 67% 55 65% 0.794
no 38 33% 29 35%
Total 116 100% 84 100%
Daily checkup of the foot and Daily observation of foot to detect any ulcer
yes 72 62% 44 52% 0.171
no 44 38% 40 48%
Total 116 100% 84 100%
Assign time for foot care always 23 20% 7 8% 0.05
often 9 8% 6 7%
sometimes 18 16% 25 30%
never 66 57% 46 55%
Total 116 100% 84 100%
Washing foot (Ablution at least once) always 115 99% 83 99% 0.349
sometimes 0 0% 1 1%
never 1 1% 0 0%
Total 116 100% 84 100%
Drying foot after washing it always 53 46% 30 36% 0.01
often 1 1% 6 7%
sometimes 8 7% 17 20%
never 54 47% 31 37%
Total 116 100% 84 100%
Using skin lotion or olive oil for the foot always 47 41% 21 25% 0.067
often 4 3% 8 10%
sometimes 37 32% 31 37%
never 28 24% 24 29%
Total 116 100% 84 100%
Checking foot for presence of any ulcer always 33 28% 17 20% 0.302
often 9 8% 9 11%
sometimes 39 34% 37 44%
never 35 30% 21 25%
Total 116 100% 84 100%
Using a mirror for foot checkup always 4 3% 1 1% 0.085
often 2 2% 1 1%
sometimes 0 0% 4 5%
never 110 95% 78 93%
Total 116 100% 84 100%
Checking the foot by one of the family members always 3 3% 1 1% 0.899
often 5 4% 3 4%
sometimes 14 12% 11 13%
never 94 81% 69 82%
Total 116 100% 84 100%
Not to walk barefooted always 59 51% 33 39% 0.053
often 16 14% 11 13%
sometimes 41 35% 36 43%
never 0 0% 4 5%
Total 116 100% 84 100%
Wearing shoes always 39 34% 22 26% 0.069
often 19 16% 10 12%
sometimes 38 33% 24 29%
never 20 17% 28 33%
Total 116 100% 84 100%
-Checking the inside of the shoes always 58 50% 25 30% 0.01
often 3 3% 8 10%
sometimes 24 21% 22 26%
never 31 27% 29 35%
Total 116 100% 84 100%
Wearing socks always 40 34% 18 21% 0.01
often 16 14% 9 11%
sometimes 38 33% 25 30%
never 22 19% 32 38%
Total 116 100% 84 100%
vibration normal 101 87% 74 88% 0.829
decreased or not present
15 13% 10 12%
Total 116 100% 84 100%
foot ulcer no foot ulcer 105 91% 79 94% 0.364
foot ulcer present 11 9% 5 6%
Total 116 100% 84 100%
Wagner classification no ulcer 105 91% 79 94% 0.333
wagner1 10 9% 3 4%
wagner2 1 1% 1 1%
wagner3 0 0% 1 1%
Total 116 100% 84 100%
site no fungal 116 100% 0 0% 0.01
between toes RT 0 0% 10 12%
between toes LF 0 0% 20 24%
nail 0 0% 20 24%
nail and toes 0 0% 15 18%
Both feet between toes 0 0% 19 23%
Total 116 100% 84 100%
skin healthy 65 56% 4 5% 0.01
dry 24 21% 4 5%
heavy callus 17 15% 14 17%
fungus 0 0% 58 69%
ulcer 10 9% 0 0%
fungal and ulcer 0 0% 4 5%
Total 116 100% 84 100%
nail well kept 88 76% 25 30% 0.01
unkempt and ragged 25 22% 23 27%
thick, damaged 3 3% 1 1%
fungal 0 0% 35 42%
Total 116 100% 84 100%
deformity no deformity 97 84% 75 89% 0.521
mild 15 13% 7 8%
major 4 3% 2 2%
Total 116 100% 84 100%
footwear appropriate 47 41% 23 27% 0.115
inappropriate 26 22% 19 23%
causing trauma 43 37% 42 50%
Total 116 100% 84 100%
range of motion full 108 93% 82 98% 0.317
limitus 3 3% 1 1%
rigidus 1 1% 1 1%
ampution in hallux 4 3% 0 0%
Total 116 100% 84 100%
sensation 10 detected 85 73% 51 61% 0.131
7 to 9 22 19% 26 31%
0 to 6 9 8% 7 8%
Total 116 100% 84 100%
pedal pulse present 103 89% 73 87% 0.685
absent 13 11% 11 13%
[image:8.595.58.535.50.523.2]Total 116 100% 84 100%
Table 4. Fungal presentation
Variables NO. %
Site
no fungal 0 0%
between toes RT 10 12%
between toes LF 20 24%
Nail 20 24%
nail and toes 15 18%
Both feet between toes 19 23%
Total 84 100%
Skin
healthy 4 5%
Dry 4 5%
heavy callus 14 17%
fungus 58 69%
Ulcer 0 0%
fungal and ulcer 4 5%
Total 84 100%
Nail
well kept 25 30%
unkempt and ragged 23 27%
thick, damaged 1 1%
fungal 35 42%
Total 84 100%
used to assign time for foot care always, and drying foot after washing it always had a significantly lower prevalence of foot fungal infection. Similar findings were reported in Japan, where it was found that that daily washing and drying feet may reduce the risk of onychomycosis in patients with diabetes (Rich, 2002). In the same respect, Ilkit and his colleagues reported that the prevalence of tinea pedis was 29.5% in
mosque attendees, (Ilkit et al., 2005) the high prevalence was
explained by the fact that infected individuals transfer dermatophytes to the floor, where they are picked up by
non-infected bare-footed prayers (Fatani et al., 2000). Therefore, in
the current study, it was found that the prevalence of fungal infection was much lower in diabetic patients who reported that they are always wearing socks. When foot fungal infection occurs, it carries the risk of infesting surrounding environment, such as the clothes, shoes, socks and bathroom, therefore it can infect other individuals, as well as infestation of one’s socks and shoes will further expose the feet to the fungus and its spores when worn again, resulting in persistence of infection or
reinfection (Caputo et al., 2001; Cha et al., 2006; Ilkit et al.,
2005). That could explain the findings of our study, where the prevalence of fungal infection was significantly higher among those who reported that they had been infected or previously treated from foot fungal infection. In the same context, Chadwick (2013) addressed that old shoes may become colonized with the fungi which allow longer contact with the skin, he recommended replacement of old shoes, and wearing well-fitting shoes (without high heels or narrow toes). Shoes should also be kept dry, which can be achieved by alternating shoes on a daily basis. Clean, absorbent socks are recommended, preferably made from natural fibers (Chadwick, 2013). In our study, it was observed that diabetic patients who used to inspect the inside of their shoes were less likely to have foot fungal infection. The study showed that diabetic patients with foot fungal infection were significantly older than those without. Similar findings were reported in Thailand
(Assadamongkol et al., 2016) and Mexico (Manzano-Gayosso
et al., 2008). This association between fungal infection and older age can be explained by many factors; first is the apparent deterioration in the immune system of elderly people, especially the adaptive immunity, as a part of the natural aging process, which increase susceptibility to opportunistic
infections, (Weng et al., 2006) and secondly, is the progressive
reduction in physical fitness of elderly people, which limit their ability to take care of their feet.
Lastly, our study showed that diabetic patients who are suffering from hypertension had a significantly higher prevalence of foot fungal infection, in the same context, in Thailand it was observed fungal infection was higher in cases
with coronary heart diseases, (Assadamongkol et al., 2016) that
might be attributed to the deficient perfusion of blood in extremities in patients with cardiovascular diseases, that could potentiate the fungal infection, nevertheless, further researches are recommended to elaborate this supposed association.
Conclusion and recommendation
The prevalence of foot fungal infection is remarkably high in diabetic patients attending primary health care centers in Jeddah. The most important identified factors influencing the prevalence of foot fungal infection included the warm humid climate characterizing the weather in Jeddah, other morbidities namely hypertension, and personal attributes including age of the patient, frequent washing and drying feet, frequent inspection of the inside of the shoes and wearing socks.
From the findings of the current study, we recommend the following:
1. Diabetic patients attending primary health care centers
should be examined thoroughly and regularly for foot fungal infection.
2. Deliberate efforts should be made to organize health
education settings for the diabetic patients in the primary health care centers targeting their knowledge and skills about foot care.
3. Prayers should be encouraged to wear socks in
mosques, and washing feet after going back home.
4. Further researches are needed to verify the association
between hypertension and increased likelihood of foot fungal infection.
REFERENCES
Abanmi A, Bakheshwain S, El Khizzi N, Zouman A, Hantirah S, et al. 2008. Characteristics of superficial fungal infections in the Riyadh region of Saudi Arabia.
International Journal of Dermatology, 47(3):229-35. Al Sheikh H. 2009. Epidemiology of dermatophytes in the
eastern province of Saudi Arabia. Res J Microbiol.,
4(6):229-34.
Deformity
no deformity 75 89%
Mild 7 8%
major 2 2%
Total 84 100%
Footwear
appropriate 23 27%
inappropriate 19 23%
causing trauma 42 50%
Total 84 100%
range of motion
Full 82 98%
limitus 1 1%
rigidus 1 1%
ampution in hallux 0 0%
Total 84 100%
Sensation
10 detected 51 61%
7 to 9 26 31%
0 to 6 7 8%
Total 84 100%
pedal pulse present 73 87%
absent 11 13%
Aljoufie M. 2017. Examining the challenges of bicycle use in
Jeddah city. Procedia Environmental Sciences, 37:269-81.
Alwin A, Abdulaziz A, Braham R, Ali Musallam M, Abdullah A, et al. 2017. Type 2 diabetes mellitus in Saudi Arabia:
major challenges and possible solutions. Current diabetes
reviews, 13(1):59-64.
Assadamongkol R, Lertwattanarak R, Bunyaratavej S, Leeyaphan C, Matthapan L. 2016. Prevalence, Risk Factors, and Type of Organism in Fungal Foot Infection and Toenail
Onychomycosis in Thai Diabetic Patients. Journal of the
Medical Association of Thailand= Chotmaihet thangphaet,
99(6):659-64.
Bristow IR, Spruce MC. 2009. Fungal foot infection, cellulitis
and diabetes: a review. Diabetic Medicine, 26(5):548-51.
Caputo R, De Boulle K, Del Rosso J, Nowicki R. 2001. Prevalence of superficial fungal infections among sports active individuals: results from the Achilles survey, a
review of the literature. Journal of the European Academy
of Dermatology and Venereology, 15(4):312-6.
Cha BY, Son HS, Lee JM, Kang SK. 2006. Prevalence of Fungal Infection on Foot in Diabetic Patients and Correlation between Diabetic Ulcer and Fungal Infection on
Foot. The Journal of Korean Diabetes Association,
30(1):64-72.
Chadwick P. 2013. Fungal infection of the diabetic foot: the
often ignored complication. Diabet Foot Can., 1(2):20-4.
Dogra S, Kumar B, Bhansali A, Chakrabarty A. 2002. Epidemiology of onychomycosis in patients with diabetes
mellitus in India. International Journal of Dermatology,
41(10):647-51.
Fatani MI, Al-Afif KA, Hussain H. 2000. Pattern of skin diseases among pilgrims during Hajj season in Makkah,
Saudi Arabia. International Journal of Dermatology,
39(7):493-6.
Ilkit M, Tanir F, Hazar S, GÛmÛsay T, Akbaba M. 2005. Epidemiology of tinea pedis and toenail tinea unguium in
worshippers in the mosques in Adana, Turkey. The Journal
of dermatology, 32(9):698-704.
Johari NH, Hassan OH, Anwar R, Kamaruzaman MF. 2013. A behaviour study on ablution ritual among Muslim in
Malaysia. Procedia-Social and Behavioral Sciences,
106:6-9.
Joshi N, Caputo GM, Weitekamp MR, Karchmer AW. 1999.
Infections in patients with diabetes mellitus. N Engl J Med.,
341:1906-12.
Manzano-Gayosso P, Herníndez-Herníndez F, Mandez-Tovar L, Palacios-Morales Y, Cardova-Martnez E, et al. 2008. Onychomycosis incidence in type 2 diabetes mellitus
patients. Mycopathologia., 166(1):41-5.
Musette P, Benichou J, Noblesse I, Hellot MF, Carvalho P, et al. 2004. Determinants of severity for superficial cellutitis
(erysipelas) of the leg: a retrospective study. European
Journal of Internal Medicine, 15(7):446-50.
Rich P. 2002. Onychomycosis and tinea pedis in patients with
diabetes. Journal of the American Academy of
Dermatology, 43(5):S130-S134.
Saunte DM, Holgersen JB, Hædersdal M, Strauss G, Bitsch M, et al. 2006. Prevalence of toe nail onychomycosis in
diabetic patients. Acta dermato-venereologica, 86(5):425-8.
Scher RK, Baran R. 2003. Onychomycosis in clinical practice:
factors contributing to recurrence. British Journal of
Dermatology, 149:5-9.
Thomas J, Jacobson GA, Narkowicz CK, Peterson GM, Burnet H, et al. 2010. Toenail onychomycosis: an important global
disease burden. Journal of clinical pharmacy and
therapeutics, 35(5):497-519.
Weng N. 2006. Aging of the immune system: how much can
the adaptive immune system adapt?. Immunity, 24(5):495-9.