_____________________________________________________________________________________________________
*Corresponding author: E-mail: [email protected], [email protected];
(Past name: British Journal of Medicine and Medical Research, Past ISSN: 2231-0614, NLM ID: 101570965)
Clinical and Radiographical Performance of
Different Types of Posts
Mohammed M. Al Moaleem
1,2*, Muneera R. Gohal
3, Abdulrahman A. Mobaraky
3,
Amna M. MobarakI
3, Fahad M. Kariri
3, Hassan A. Madkhali
3, Mosaab M. Qohal
3,
Saleh M. Alhuraysi
3, Ali E. Shutayfi
3, Saeed A. Al Amri
3and Nabiel Al Ghazali
41
Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan, Saudi Arabia. 2
Department of Dentistry, Faculty of Medical and Health Sciences, Taiz University, Republic of Yemen. 3College of Dentistry, Jazan University, Jazan, Saudi Arabia.
4
Department of Prosthodontics, College of Dentistry, Aleppo University, Aleppo, Syria.
Authors’ contributions
This work was carried out in collaboration between all authors. Author MMAM designed the study, performed the statistical analysis, wrote the protocol and the first draft of the manuscript. Authors MRG and AAM did follow-up the cases clinically. Author AMM managed the final manuscript and the revisions. All authors read and approved the final manuscript.
Article Information
DOI: 10.9734/JAMMR/2017/35778
Editor(s):
(1) Rodrigo Crespo Mosca, Department of Biotechnology, Institute of Energetic and Nuclear Research (IPEN-CNEN), University of Sao Paulo (USP), Brazil. (2)Joao Paulo Schwartz, Department of Orthodontics, Universidade Estadual Paulista (UNESP-FOAr), Brazil. (3)Salomone Di Saverio, Emergency Surgery Unit, Department of General and Transplant Surgery, S. Orsola Malpighi University Hospital, Bologna, Italy.
Reviewers:
(1) Rafael Menezes Silva, University of São Paulo-USP, Brazil. (2)Goo Chui Ling, National University of Malaysia, Malaysia. (3)Anonymous, Federal University of Pelotas, Brazil. (4)Denzil Valerian Albuquerque, Dr. Mohamed Al-Said Specialized Dental Center, Qatar. (5)Hacer Deniz Arisu, Gazi University, Turkey. (6)Mona Ionas, University Lucian Blaga of sibiu, Romania. Complete Peer review History:http://www.sciencedomain.org/review-history/21251
Received 28th July 2017 Accepted 26th September 2017 Published 4th October 2017
ABSTRACT
Background: A post is an important part of restoring a tooth that has lost a coronal portion and is implicated in the type of core materials or post systems used in tooth restoration.
Objectives: To evaluate and compare the radiographic and clinical performance of three different
types of posts, namely, glass fiber post (GFP), custom-made cast post (CMP), and prefabricated metal post (MP).
Materials and Methods: Eighty-eight posts were selected, and roots were restored using one of the posts after endodontically treated teeth (ETT). The ETT were fabricated by final year undergraduate dental students. Composite resin cores were placed before cementation of individual porcelain fused to metal crowns. Clinical and radiographic assessments were performed to determine recurrent caries, periapical lesions, post fractures, crown or post mobility under figure pressure, loss of post retention, and damage to biological width. The survival rates were recorded at 3, 9, and 18 months of follow-up intervals from the final cementation of crowns. Data were analyzed in SPSS by identifying the frequency and percentages and by conducting Kaplan–Meyer analysis. Categorical values were evaluated through chi-square test and descriptive statistical analysis was carried out through log-rank test.
Results: The 88 posts evaluated in this study yielded nearly equal percentages of anterior (45; 51.1%) and posterior (43; 48.9%) teeth. The majority of posts were GFP (51; 58%), and the
remaining posts were MP (16; 18.2%). The major cases of recurrent caries and periapical lesions were found in CMP during the 18-month follow-up. By comparison, the mobility
of crowns under figure pressure was associated with CMP during the 9- and 18-month assessment. Loss of post retention was detected in MP during the 3- and 18-month follow-up. Among the three posts, CMP yielded the highest degree of damage to the biological width during the 3-month follow-up.
Conclusion: GFP achieved a success rate of approximately 100% ETT restoration. By contrast, custom-made cases showed a higher degree of failure than MP did during the 18-month follow-up by the 6th year undergraduate students.
Keywords: Custom-made post; endodontically treated teeth; survival rate; glass fiber post; stainless steel post.
1. INTRODUCTION
The restoration of an endodontically treated tooth (ETT) is a key step of treatment planning because of its effect on the long-term prognosis of teeth [1]. Loss of hard tissues leads to a
reduced load carrying capacity of ETT
[2]. Therefore, posts are recommended for an ETT highly susceptible to fracture because it possesses a weak coronal tooth structure [3,4].
Various post and core systems for the restoration of a tooth with a treated root canal have been investigated. Post failures and prosthetic failures have been considered the most common causes of failure in ETT [5].
Prefabricated posts are traditionally prepared with metals, such as custom-made cast post (CMP), which is visible from the structure of ETT, especially in the anterior region [6]. With high rigidity, a prefabricated metal post (MP) likely vibrates at high frequencies when it is loaded with lateral forces [7] and can cause longitudinal fractures in roots or metal corrosion [8]. Consequently, these phenomena lead to tooth loss [9]. Mismatch in moduli can induce stress highly concentrated in a cement lute because the modulus of elasticity of metallic materials, such
as CMP and MP, is higher than that of the supporting dentin; therefore, material failure occurs [10,11].
Glass fiber post (GFP)-supported resin dowel systems were introduced in 1992. Dowels are
composed of unidirectional glass fibers
embedded in a resin matrix that strengthens these dowels without compromising the modulus of elasticity. A GFP also distributes stress over a broad surface area, thereby increasing the load threshold at which a dowel begins to show evidence of micro-fractures. A GFP and dowels reduce the risk of tooth fractures, and their survival rates are higher than those of teeth restored with Zirconia dowels [12,13].
The clinical use of glass fiber posts in comparison with conventional ready-made metal posts and the traditional cast made posts for
the restoration of compromised coronal
2. MATERIALS AND METHODS
2.1 Samples Design and Collection
This prospective study was conducted for male and female patients who visited the Endodontic and Prosthodontic Department in Dental College, Jazan University in the Kingdom of Saudi Arabia for regular treatment were selected in this study. Ethical approval was obtained from the Faculty of Dentistry, Jazan University, and all of the study subjects signed a written consent to participate in the study.
2.2 Samples Inclusion and Exclusion Criteria’s
The following inclusion criteria were considered: posts were constructed by 6th year male and female students, patients aged 17 years and above. All of the teeth from maxillary and mandibular arches were selected, and all of the cases were ETT composed of MP and GFP. Their cores were prepared with a composite resin or CMP. The healthy periodontium did not bleed while probing and exhibited a good bone support. All of the teeth were characterized by an adequate ferrule length (presence of 1-2 mm of the clinical crowns) and a biological width to allow the production of a finished line on a strong tooth structure and to restore ETT with PFM crowns.
The following exclusive criteria were considered: teeth that could be used as abutments for fixed prostheses; absence of all molar teeth or adequate posterior vertical stops; and occlusal interference or fremitus affecting the tooth to be restored.
2.3 Samples Post-space Preparation,
Post-fabrication, and Cementation
Eighty-eight posts were selected for this study. After the root canal treatment of the teeth was finished, the roots were restored by GFP, MP, or CMP, and composite resin cores were used before individual PFM crowns were cemented.
Gutta-percha (GP) was removed from the root canal by using Gates Glidden drills (Pulpdent Corporation, USA). A space was then prepared using pesso reamers (Relaxy Fiber Post, 3MESPE, Germany), with increasing sizes. A minimum apical seal of 3–5 mm of GP filling was left on the apical root portion. The teeth were
prepared in accordance with a standard clinical protocol involving hand instruments. For CMP, the root canals were dried and lubricated with petroleum jelly. The posts and cores were fabricated from a resin post and a core (Duralay, Reliance Dental Manufacturing Company, Italy) and then forwarded to the laboratory for casting. The finished and polished cast posts and cores were casted in a nickel-chromium alloy and then cemented after application of rubber dam into the canal by using Zinc Polycaropxylat Cement,
Durelon, Durelone Aplicap (3M ESPE,
Germany). The CMP were constructed and cemented as prescribed by Grandini et al. [14].
GFP was fabricated from a fiber post, Relaxy fiber post (3M ESPE, Germany) after the canals were irrigated with a solution of saline and sodium hypochlorite, and the required GP for post spaces were removed. The lengths of the post of the canal were measured and marked, and the trimmed posts were replaced with the canal to confirm its length. The prepared canal was etched with 37% phosphoric acid for 15 s. The etchant was rinsed with water and dried with paper points. An adhesive primer and a bonding agent, Adper Prompt L-Pop (3M ESPE, St. Paul, MN, USA) self-etching adhesive system were applied to the canal. GFP was cemented in the canals with Relaxy XTM and Unicem AppliCap resin cement adhesive resin cements (3MESPE,
Germany). The cemented GFP was
subsequently light-cured for 60 s. The cores were rebuilt with composite resin in incremental techniques. All the GFPs were prepared and cemented as recommended by Neumann et al. [3] and Gradebot et al. [15].
MP was prepared with a stainless steel screw post (Dental Supplies, China), and each canal was created and cleaned. The length of the post of the canal was determined and cemented with conventional cement. The core was rebuilt with composite resin in incremental techniques.
The group of stainless steel screw posts were selected, inserted and cemented as
recommended by Gradebot et al. [14].
After the posts were cemented, the preparations were further refined and polyvinyl siloxane putty and light body impressions were collected to construct crowns. All of the finished lines were
created on strong tooth structures. The
were performed in accordance with the manufacturer’s instructions.
2.4 Post-operative Evaluations
The patients were educated about oral hygiene and motivated to use proper oral hygiene aids. Clinical and radiographic assessments were conducted for each cemented crown at the baseline time (time of cementation), 3-, 9-, and 18-month intervals. Variables, such as gender, type of post, location of post, and age of patients, were considered during evaluation.
Clinical and radiographic assessments were
performed to determine recurrent caries,
periapical lesion, post fracture, mobility of crown or post under figure pressure, loss of post retention, and damage to the biological width.
The survival rates were recorded at time of cementation, 3, 9, and 18 months of follow-up intervals after the final cementation was conducted. The restorations were evaluated by an expert staff who was not involved in the study or restoration and who did not reveal the data at the time of follow-up (single–blind trial).
2.5 Statistical Analyses
Data were recorded and analyzed using SPSS version 21 (IBM). The three post types were compared in terms of the frequency of failures for the 3, 9, and 18 months of follow-up through Fisher’s exact test. Kaplan–Meier survival curves of the three posts were drawn to describe our data, and the survival rates were compared with a log-rank test. Significance level was set at 5%.
3. RESULTS
A total of 20 subjects (8 males and 12 females) aged between 17 and 60 years with a mean age of 29.83±11.6 years were recruited, and 88 teeth that satisfied the inclusion criteria were evaluated
in these subjects. The frequency and
percentages of the anterior (45; 51.1%) posts were 36 GFP, 4 MP, 5 CMP. The percentage and frequency of the posterior (43; 48.9%) posts were 15 GFP, 12 MP, 16 CMP and it was almost equal in this study. All types of teeth were involved in this study. The majority of the cases were GFP (58%) and the remaining cases were MP (16; 18.2%; Table 1).
In the clinical and radiographic assessments, the three types of posts remained unchanged in 3
and 9 months of follow-up in terms of recurrent
caries. Conversely, recurrent caries were
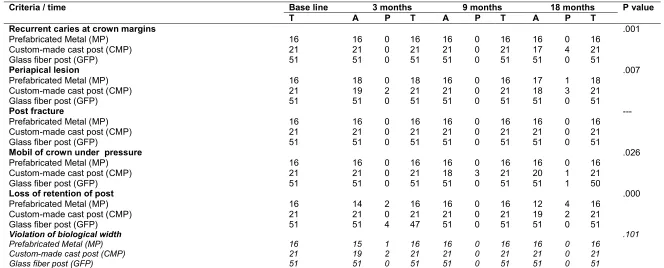
detected in 4 cases of CMP at 18 months. The periapical lesions were observed in 2 cases of CMP during the 3 months of follow-up and became 3 at 18 months follow-up with 1 case of MP. In terms of the mobility of crowns under figure pressure, 3 cases of CMP were observed during the 9-month assessment. Furthermore, 1 case from MP and 1 case from CMP were found during the 18-month follow-up. During 3 and 18 months of follow-up, the highest number of cases that lost their post retention of MP was six cases, that is, 2 and 4 cases during the 3- and 18-month follow-up. In CMP, 2 cases lost their post retention. Damage to the biological width was observed in 2 cases of CMP and 1 case of MP during the 3-month follow-up. No significant differences were found in various time intervals (Table 2).
The overall survival rate after 18 months and a 100% success rate were observed in post-fracture during the follow-up in all of the intervals and in recurrent caries and mobility of the crown under finger pressure during the 3-month follow-up. Although the same percentage of the variables was recorded during the 9-month assessment of the three types of posts, more than 80% was observed in the mobility of the crown under finger pressure in CMP. Conversely, the success rate of the variables ranged from 70% to 80% in MP and CMP and from 95% to 100% in GFP (Table 2).
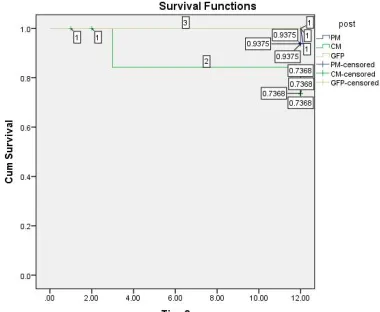
Survival statistical analysis for 18 months: The frequency of failure did not significantly differ during the 18-month follow-up. Kaplan–Meier curves (Figs. 2 and 3] reveal that the periapical lesion and mobility of the crown under finger pressure were running almost identically in different periods, indicating that the two variables exhibited a similar behavior. The loss of post retention and damage to the biological width showed the same trend (Figs. 4 and 5). Conversely, recurrent caries exacerbated as time was extended (Fig. 5).
4. DISCUSSION
5
Table 1. Distribution of the post cases according to gender, post type and post location
Variable Gender Post type Post location
Male Female Prefabricated metal Custom-made cast Glass fiber Anterior Posterior
Number 40 48 16 21 51 45 43
% 45.5 54.5 18.2 23.9 58 51.1 48.9
Table 2. Clinical and radiographical evaluation of the different posts at various follow-up intervals
Criteria / time Base line 3 months 9 months 18 months P value
T A P T A P T A P T
Recurrent caries at crown margins
Prefabricated Metal (MP) Custom-made cast post (CMP) Glass fiber post (GFP)
16 21 51 16 21 51 0 0 0 16 21 51 16 21 51 0 0 0 16 21 51 16 17 51 0 4 0 16 21 51 .001 Periapical lesion
Prefabricated Metal (MP) Custom-made cast post (CMP) Glass fiber post (GFP)
16 21 51 18 19 51 0 2 0 18 21 51 16 21 51 0 0 0 16 21 51 17 18 51 1 3 0 18 21 51 .007 Post fracture
Prefabricated Metal (MP) Custom-made cast post (CMP) Glass fiber post (GFP)
16 21 51 16 21 51 0 0 0 16 21 51 16 21 51 0 0 0 16 21 51 16 21 51 0 0 0 16 21 51 ---
Mobil of crown under pressure
Prefabricated Metal (MP) Custom-made cast post (CMP) Glass fiber post (GFP)
16 21 51 16 21 51 0 0 0 16 21 51 16 18 51 0 3 0 16 21 51 16 20 51 0 1 1 16 21 50 .026
Loss of retention of post
Prefabricated Metal (MP) Custom-made cast post (CMP) Glass fiber post (GFP)
16 21 51 14 21 51 2 0 4 16 21 47 16 21 51 0 0 0 16 21 51 12 19 51 4 2 0 16 21 51 .000
Violation of biological width Prefabricated Metal (MP) Custom-made cast post (CMP) Glass fiber post (GFP)
16 21 51 15 19 51 1 2 0 16 21 51 16 21 51 0 0 0 16 21 51 16 21 51 0 0 0 16 21 51 .101
Fig. 1. Kaplan–Meier survival graph of recurrent caries
Fig. 2. Kaplan–Meier survival graph of pre-apical lesion
Fig. 3. Kaplan–Meier survival graph of mobility of post under pressure
Fig. 4. Kaplan–Meier survival graph of the loss of post retention
materials or the type of post systems that should be used. The selection of restorative materials for ETT restoration is dependent on the proportion of the remaining tooth structure. Posts exhibiting beneficial characteristics, such as esthetic property, non-corrosiveness, fracture resistance, and radiopaqueness, should be selected.
This prospective clinical study was performed primarily to evaluate and compare the clinical and radiographic performance of GFP, MCP, and MP prepared by the 6th year undergraduate students in the Faculty of Dentistry, Jazan University.
Clinical studies on GFP for ETT restoration have been widely conducted. In Table 1, GFP represented more than half (58%) of the total sample sizes and this finding was consistent with previous results. These posts exhibit greater flexibility, provide acceptable mechanical and physical properties, and cause a lower probability of root fracture than metallic posts do. These
posts have demonstrated good clinical
performance for more than two years of clinical application [14-16]. In vitro studies have also concluded that GFP insertion under final restorations improves the support for PFM restorations, thereby causing a lower degree of fracture and failure than those of other types of metallic posts [17-24].
The clinical and radiographic assessments associated with CMP revealed 4 cases (20%) of recurrent caries at the crown margin, but this result was inconsistent with that observed by Grandini et al. [15], who showed only 4% of marginal leakage under composite restoration with GFP during the 12-month follow-up and obtained 6% at the end of 30 months. This difference could be attributed to the longer evaluation period in the previous study and to the position of the restored tooth in relation to occlusion.
The preapical X-ray showed 2 cases (10%) in CMP during the 3-month interval and 4 cases in MP and CMP during the 18-month interval. This result was similar to that of Gbadebo et al. [14] and Grandini et al. [15] regarding the percentage of periapical pathological cases.
The absence of any type of post fracture in the restored anterior and posterior teeth in the study period was consistent with the findings of Gbadebo et al. [14] but inconsistent with the
observations of Grandini et al. [15], who achieved 4% of GFP possibly because of the differences in the width of the post used and the type of the final restoration, which was composite restoration. Because marginal leakage occurred in composite restoration and extended to the fracture after a follow-up period. Our results also disagreed with those of Morgano and Milot [9], who observed a fracture in MP during follow-up [25].
The loss of retention was detected in 2 cases of MP during the 3-month follow-up and in 4 cases of MP during the 18-month follow-up. The percentage of these findings was larger than that of Gbadebo et al. [14]. This result may be related to different factors, such as proper adjustment of occlusion at the final cementation of restoration,
improper isolation from cementation, and
cementation protocol. All of the cases were re-cemented after the cause of the loss of post retention was resolved [26].
The damage to biological width is an important factor of the survival rate of any type of ETT. In Table 2, the biological widths of the three cases (one in MP and two in CMP) were altered after 3 months, and this finding was similar to that of Gbadebo et al. [14]. Conversely, Malferrari et al. [7] obtained a contrasting finding attributed to different levels of expertise because their restorations were performed in general practice, whereas our restorations were conducted by students in their final year of study.
The analysis of Kaplan–Meier survival rates in different evaluation periods indicated that the clinical behaviors in various variables did not significantly differ. Figs. 2 and 3 illustrate the periapical lesion and mobility of the crown under finger pressure, which was running almost similarly in different periods. These findings suggested that the two variables exhibited the same pattern.
The limitations of this study included small sample size and short period evaluation. We recommended further studies involving a larger
size of patients and longer follow-up
duration. This study also employed a two-dimensional radiograph, so we advised to use new and recent X-ray techniques during follow-up intervals.
5. CONCLUSIONS
This study was conducted in a controlled academic clinical set-up, with the 6th year undergraduate students for 18 months, and the
following conclusions could be drawn:
GFP yielded a success rate of
approximately 100% in ETT restoration, whereas CMP obtained the highest failure rate.
The three types of posts remained
unchanged in terms of recurrent caries during the 3- and 9-month follow-up. The major cases of recurrent caries and periapical lesions were observed in CMP during the 18-month follow-up.
The highest degrees of the mobility of the crowns under figure pressure were found in CMP during the 9- and 18-month assessment. The loss of post retention was high in MP followed by that in MP
during the 18-month assessment.
Conversely, the damage to the biological width was observed during the 3-month follow-up of CMP.
No significant differences were detected in
the different intervals.
CONSENT
As per international standard or university standard, patient’s written consent has been collected and preserved by the authors.
ETHICAL APPROVAL
As per international standard or university standard, written approval of Ethics committee has been collected and preserved by the authors.
COMPETING INTERESTS
Authors have declared that no competing interests exist.
REFERENCES
1. Mannocci F, Bertelli E, Sherriff M, Waston
TF, Pitt Ford TR. Three year clinical comparison of survival endodontically treated teeth restored with either full cast
coverage or with direct composite
restoration. J Prosthet Dent. 2002;88:297-301.
2. Evidence-based review of clinical studies
on restorative dentistry. J Endod. 2009;35: 1111-5.
3. Naumann M, Blankenstein F, Dietrich T.
Survival of glass fiber reinforced composite post restorations after 2 years: An observational clinical study. J Dent. 2005;33:305-12.
4. Assif D, Gorfil C. Biomechanical
considerations in restoring endodontically treated teeth. J Prosthet Dent. 1994;71: 565-7.
5. Morgano SM. Restoration of pulpless
teeth: Application of traditional principles in present and future contexts. J Prosthet Dent. 1996;75:375-80.
6. Bateman G, Ricketts DN, Saunders WP.
Fibre‑based post systems: A review. Br Dent J. 2003;195:43-38.
7. El-Ela OA, Atta OA, El-Mowafy O. Fracture
resistance of anterior teeth restored with a novel nonmetallic post. J Can Dent Assoc. 2008;74:441.
8. Malferrari S, Monaco C, Scotti R. Clinical evaluation of teeth restored with quartz fiber-reinforced epoxy resin posts. Int J Prosthodont. 2003;16:39-44.
9. Ozkurt Z, Iþeri U, Kazazoðlu E. Zirconia
ceramic post systems: A literature review and a case report. Dent Mater J. 2010;29:233-45.
10. Morgano SM, Milot P. Clinical success of cast metal posts and cores. J Prosthet Dent. 1993;70:11-6.
11. King PA, Setchell DJ, Rees JS. Clinical
evaluation of a carbon fibre reinforced carbon endodontic post. J Oral Rehabil. 2003;30:785-9.
12. Brown D. Fibre-reinforced materials. Dent
Update. 2000;27:442-8.
13. Usumz A, Cobankara FK, Ozturk N,
Eskitasciogku G, Belli S. Microleakage of endodontically treated teeth with different dowel systems. J Prosthet Dent. 2004;92: 163–9.
14. Grandin S, Goracci C, Tay FR, Grandin R,
endodontically treated teeth. Int J Prosthodont. 2005;18:399-404.
15. Gbadebo OS, Ajayi DM, Oyekunle OOD,
Shaba PO. Randomized clinical study comparing metallic and glass fiber post in restoration of endodontically treated teeth. Ind J Dent Resea. 2014;25(1):58-63.
16. Better K, Kielbassa NM. Post-endodontic
restorations with adhesively luted fiber-reinforced composite post system: A review. Ame J Dent. 2007;20:353-60.
17. Salameh Z, Ownsi H, Aboushelib MN,
Sadig W, Ferrari M. Fracture resistance and failure patteren of endodoically treated mandibular molars with and without glass fiber post in combination with a zirconia-ceramic crown. J Dent. 2008;36:513-9. 18. Adanira N, Bellib S. Evaluation of different
post lengths’ effect on fracture resistance of a glass fiber post system. Eur J Dent. 2008;2:23-28.
19. Nimigean VR, Buţincu L, Nimigean V. A
radiographic study regarding post retained restorations. Rom J Morphol Embryol. 2012;53(3 Suppl):775–9.
20. Torbjorner A, Karlsson S, Odman PA.
Survival rate and failure characteristics for two post designs. J Prosthet Dent. 1995;73(5):439-444.
21. Mentink AG, Meeuwissen R, Kayser AF,
Mulder J. Survival rate and failure characteristics of the all metal post and core restoration. J Oral Rehab. 1993;20: 455-461.
22. Creugers NH, Mentink AG, Kayser AF. An
analysis of durability data on post and core restorations. J Dent. 1993;21(5):281-284.
23. Hatzikyriakos AH, Reisis GI, Tsingos N. A 3-year postoperative clinical evaluation of posts and cores beneath existing crowns. J Prosthet Dent. 1992;67:454-458.
24. Weine FS, Wax AH, Wenckus CS.
Retrospective study of tapered, smooth post systems in place for 10 years or more. J Endod. 1991;17(6):293-297.
25. Bergman B, Lundquist P, Sjogren U,
Sundquist G. Restorative and endodontic results after treatment with cast post and cores. J Prosthet Dent. 1989;61(1):10-15.
26. Ferrari M, Vichi A, Mannocci F, Mason NP.
Retrospective study of the clinical
performance of fiber post. Am J Dent. 2000;13:98-138.
27. Ibrahim H, El- Mowafy Omar, Brown JW.
Radio opacity of non-metallic root canal posts. Int Prosthodont. 2006;19:101-16.
28. Naumann M, Blankenstein F, Kiessling S,
Dietrich T. Risk factors for failure of
glass fiber-reinforced composite post
restorations: A prospective observational clinical study. Eur J Oral Sci. 2005;113: 519-24.
29. Mannocci F, Qualrougb AJE, Worbington
HV, Watson TF, Pit Ford TR. Randomize
clinical comparison of endodnotically
treated teeth restored with amalgam or with fiber posts and resin composite: Five-year results. Oper Dent. 2005;30:9-15.
30. Cagidiaco MC, Carcia-Godoy F, Vichi A,
Grandini S, Goracci C, Ferrari M.
Placement of fiber prefabricated or
custom-made posts affects the 3-year
survival of endodnotically treated
premolars. Am J Dent. 2008;21:179-84. _________________________________________________________________________________ © 2017 Al Moaleem et al.; This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Peer-review history: