A Review on Detection and Performance
Analysis on R-R Interval Methods for ECG
Priyanka Mayapur1
B.E Student, Dept. of Electronics and Communications Engineering, Agnel Institute of Technology and Design, Goa, India1
ABSTRACT: Electrocardiogram (ECG)is a signal that records the electrical performance of the heart. A reliable, real time analysis of ECG and its considerate features is a necessary prerequisite for monitoring R-R Interval, hence HRV and cardiovascular control. The work proposed in this paper reviews the various methods used to detect the R-R interval and its related features that summarizes the various techniques used by researchers and also provides generic advantages about the various methods used. The processing of the data was done on the Lead-II ECG signals and on a tool called as Matlab.
KEYWORDS: Electrocardiogram (ECG), R-R Interval, Lead-II Configuration, Matlab, Heart Rate Variability.
I. INTRODUCTION
Invented by Willem Einthoven in 1901, an ECG is an advanced recording method of bioelectric signal that records the electrical impulses of the heart that results due to the depolarization and repolarization of the ions in the blood which include a fairy period of graphs corresponding to the consecutive heart action phases [1, 2, and 3].
The work proposed in this paper consists of an ECG recorded in an image consisting of all 12 channels or lead recordings interlaced 3 second intervals from combinations of leads per row.
They often occur in the same order aligned in columns:
First row: I, AVR, V1, V4||Second row: II, AVL, V2, V5 ||Third row: III, AVF, V3, V6
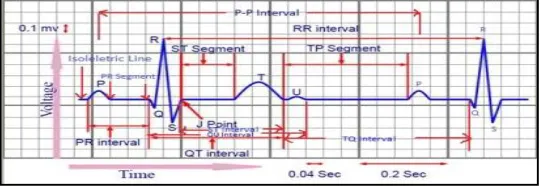
Since distinct diseases manifest differently in each of the leads, it is important to isolate the different leads involved. Lead-II Configuration is the most preferred monitoring lead of choice for continuous ECG monitoring as it is the most useful lead for detecting cardiac arrhythmias (irregular heartbeat) as it lies close to the cardiac axis and allows the best view of P and R waves, thus helping in interpreting rhythms. In the morphology of ECG signal where the normal rhythm of the heart represents no disease or disorder is called Normal sinus rhythm (NSR). The tracing of each heartbeat would consist of several waves or peaks, segments, intervals and joints as a recurrent wave sequence like which is shown in Figure 1 below:
Waves: P, Q, R, S, T, U; Segments: PQ, ST; Intervals: PQ, R-R, QT, TP, TQ; Additional:J point &QRS Complex
II. RELATED WORK AND IMPORTANCE OF THE R-R INTERVAL
The work in the previous papers proposedthe various methods which could have been used to determine the R-R interval and HRV. In this paper, those methods are reviewed and discussed about in detail in Section IV.
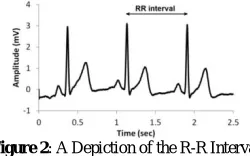
An efficient analysis of ECG could help in accurate determination in the cardiovascular studies. The trace of any ECG signal constitutes significant waves and intervals as displayed in Fig. 1 and would be considered being in rhythm only if it follows the sequence of P-QRS-T-U waves. Any signal disobeying the rhythm could indicate some serious peculiarities.Now, of the various morphological markers of ECG, the QRS Complex and the R Peak are considered to be the most significant parameters with respect to easier evaluation. Among which,the R-Peak is considered to be the most important fiducial point in the signal due to its larger amplitude and also is the sharpest component with respect to all the other peaks in a Normal Lead-II ECG Signal. Proper detection of the R-Peak is said to have a major contribution in determining a fundamental called as the R-R interval, i.e. HRV, which is one of the strongest driving factor and the biggest entity in analyzing an ECG signal. The number of R peaks in a specific time interval translates to the heart rate. The R-R interval begins at the peak of one R wave and ends at the peak of the next R wave and represents the time between two QRS complexes as shown in Figure 2 below. It is also called as the inter-beat interval (IBI) or beat-to-beat interval and plays a vital role in diagnosing heart rhythm irregularities, heart rate and can help us learn the irregularities in the various facets of the heart.
Figure 2: A Depiction of the R-R Interval
III. CLINICAL USE OF THE HEART RATE VARIABILITY
Heart Rate Variability (HRV) could be defined as the variation in the time interval between heartbeats. It is also known as "cycle length variability", "RR variability" and "heart period variability". A slight calculation error in determining HRV can lead to grossly erroneous HRV analysis results. Measurement of HRV helps in evaluating cardiac autonomic regulation and thus provides significant information regarding cardiac irregularities or injuries. It also provides information about the sympathetic-parasympathetic autonomic balance. The activity of autonomous nervous system is clearly depicted by HRV analysis, one of the most crucial markers and thereby is used as a quantitative indicator of stress and a change in the electrical potential over time is reflected in the ECG signal measurement can be used to diagnose stress-related disorders. So it is very necessary to detect R-R Interval and HRV for a better conference of a survival advantage.
IV. THE ACTUAL REVIEW BACKGROUND
applied to detect the R peaks which were then followed by calculating the R-R interval by subtracting the next R wave from the previous. Later, using the sliding window technique, detection of P wave and thus PP interval time series were done [5].
In the above paper [5], it can be seen that this algorithm is intended for discrete-time ECG signals that have been obtained by sampling the real, continuous time signals at a specific rate. This is true because the literature survey claims that this algorithm uses integer filters (algorithm is intended for integer programming on microprocessor) that realize pole and zero locations that are useful for the intended sampling rate, but become unreasonable for different sampling rates. Also the selection of the window size should be carefully selected [10]. This algorithm recognizes the QRS complexes or the R Peaks by analyzing slope and amplitude of ECG signals by taking into account the width of appearing ECG waves. It provides a real time accurate detection of the QRS Complex and the R peak permitting the use of low amplitude thresholds in order to get high detection sensitivity, thus obtaining accurate results leading to formulation of highly accurate R-R interval time series which proved to be useful in highly dependable cardiovascular variability studies.
R-R interval is a very important entity in the heart diagnostic studies and it can be calculated once the R peak is detected. In papers proposed by Jiapu Pan et al [6], Shital L. Pingale [7], Pankhuri Trivedi et al [8], Kritika Bawa et al [9] and Faezeh Marzbanrad et al [16], a similar procedure for detection of the R peak or the QRS Complex has been carried out with absolute accuracy.
This algorithm (PTA) discussed above was found to have a higher accuracy for various beat morphologies than other traditional methods in real-time.
Studies indicate that even a single artifact in the RR signal could impart substantial spurious variance into all commonly analyzed frequency bands including those associated with respiratory sinus arrhythmia, thus motivating the need for a reliable QRS detector with minimal detection error. A lot of papers have been dedicated in detecting the QRS Complex with the various methods in order to detect the R peak so that one can calculate the R-R interval successfully. Among which was a paper proposed by Natalia M. Arzeno et al who devised an algorithm based on Hamilton-Tompkins algorithm in association with Hilbert transform-based method. Herein five methods were used; one being Hilbert transform with automatic threshold where in the signal is transformed with a filter of response in the frequency domain, processed with an all-pass filter with -90° shift for positive frequencies and +90° shift for negative frequencies. This transform is an odd filter and the zero-crossings of the differentiated ECG would be represented as peaks in the output of the transform which would correspond to the R-peaks. Second procedure being Hilbert transform with secondary threshold where in the concept of secondary threshold was introduced having a similar structure of the algorithm as the method one, the third method consisted of Squaring function with patient-specific threshold which rectified the differentiated ECG by applying a squaring function. Forth method being Squaring function with automatic threshold where in Hamilton-Tompkins algorithm was extended to include an automatic adjustment of the primary threshold in order to obviate subjective choice of threshold coefficients and the last method being the Second derivative of the ECG with automatic threshold where in the second differentiation stage creates a one-sample delay and preserves most of the energy at the high frequencies corresponding to the QRS complex [11].
Hamilton Tompkins algorithm eliminated the need for human intervention and also reduced the total detection errors of peaks. The Hilbert transform's all-pass characteristic prevented unnecessary signal distortion.The transform can also be viewed as a measure of energy with a threshold that verifies if the output is enough to carry the energy of a QRS complex. The major disadvantage of this approach is that by squaring the differentiated ECG, normal QRS peaks with small magnitude and wide arrhythmic peaks with decreased slope are reduced in the output of the transform. Infact, the modified Hamilton-Tompkins algorithm as well as the Hilbert transform-based algorithms had comparable, though slightly lower, accuracy; yet these automated algorithms presented an advantage for real-time applications by avoiding human intervention in threshold determination.
Frits L. Meijler et al proposed a paper where variations in the RR intervals on myocardial contractility contributed to the variability of hemodynamic parameters during atrial fibrillation. This was conceived as the analysis of the serial autocorrelation function and the histograms of the RR intervals of patients were analyzed based on which a statistical analysis of the ventricular rhythm of a patient with atrial fibrillation could be studied. The variations in hemodynamics in patients with atrial fibrillation have been mainly attributed to changes in end-diastolic pressure which were related to the variations in RR intervals [12].
Fluctuation in the time intervals between individual heart beats quantifies the variation in the heart rate (HRV). Though R-R is visually inspected, detection of proper R peaks is very significant. In a paper devised by Mirja A. Peltola, methods involved in editing or pre-processing R–R interval time series influences a change in HRV has been talked about with an addition of detecting R peaks using various algorithms. It is claimed that the true marker for HR is the P wave onset, since the P wave is a more accurate marker of onset of the atrial depolarization than the R peak. Due to the low amplitude and difficulty in detection of P wave, R peaks are considered as the most accurate markers for detection of HRV. Several algorithms like Hilbert Transform; Digital Filtering methods like Pan Tompkins and Hamilton and Tompkins; Pattern Recognition and Wavelet Transform have been found to be useful in detection of R peaks. No standardized procedures for detecting R peaks have been recommended but it was seen that high-quality R–R interval software helped in getting a visual view of the actual point positions in the ECG signal of the R peak detection process and the possibility to correct any false points was also stressed upon [13].
From the above survey [13], it can be seen that calculation of R-R interval would be considered trustworthy by software if the software contains a possibility to view the ECG signal and the results of the R peak detection process and a possibility to correct the false points. I might also be convenient to use and give an adequate performance if manual or automatic editing of artifacts with different editing methods and a visual view of the edited R–R interval time series is involved.
A. Gersten et al proposed a paper wherein their main aim was to detect aliasing in the R-R interval spectral analysis. In order to get insight to this problem, three experiments were conducted. One, where the spectrum of an ECG signal at normal resting state was compared with the R-R interval spectrum. Second and third being, ECG signal captured at slow and fast breathing rate were compared with the R-R interval stage respectively. They believed in calculating the R-R interval using two methods; in the first method computer evaluation of R-R interval was done and in the second method a device was used whose output gave R-R interval alone [15].
From the above paper [15], it was seen that the first method used to find out the inter-beat interval was accurate and
flexible with respect to evaluations. And the second method stored smaller amounts of data which could be used easily
on-line.
In this paper [17], it was seen that the procedure used only the largest and the smallest values of the R-R interval resp. in order to calculate the HRV which was a manual technique and faster they rather than using computer analysis which would have required the measurement of all the R-R intervals making the evaluation of ECG too cumbersome.
In a paper tackled by Sonia Rezk et al, the inter-beat intervals analysis was done using a new tool of estimation based on algebraic approach. Their idea focuses on the fact that the estimation of the R wave occurrence is considered as a Time Delay Estimation (TDE) problem. The technique detected the peaks by ignoring the peaks that preceded or followed larger peaks by less than a waiting time equal refractory period. The peaks higher than the detection threshold were termed as the R peak else noise. Also if there were no R peaks detected within 1.5 R-to-R intervals then back search was applied where if a peak higher than half the detection threshold followed the preceding detection by at least 360ms was termed as R peak [18 and 27].
The paper [18 and 27] shows that the algebraic technique or derivative technique adopted allowed parameters estimation, considering the delay as other unknown parameters and gave accurate results.
In a paper proposed by Vyankatesh S. Thorat et al, cardiac arrhythmia is classified with respect to HRV and ECG signal. To determine HRV, R-R intervals were determined where in given an R-wave event, the length of the next R–R wave interval followed a physiologically motivated, time-varying inverse Gaussian probability distribution [19]. It was seen in paper [19] that this method led to short processing time and relatively high accuracy and could be used as a good real-time arrhythmia classification system.
Swetha Bellari et al proposed a paper of detecting R peaks using various methods and also compared the accurate method for the same. Methods like Wavelet transform, Hilbert transform, Pan Tompkins, Combination of Wavelet and Hilbert and Hilbert and Wavelet [20].
And it was seen in [20] that fusion of two algorithms gave a good and accurate output which was the combination of Wavelet and Hilbert transform compared to other algorithms. Thus precise detection of R peaks is helpful in detection of accurate R-R interval which will be helpful in finding out accurate arrhythmia condition of a person.
In a paper proposed by Harjeet Kaur et al, ECG was analyzed using the R-peak parameters. First the signal was processed and denoised using the hybrid linearization method, which was an arrangement of the extended Kalman filter
along with discrete wavelet transform followed by detecting the R peaks using Principal Component Analysis (PCA). In PCA, first the mean of the original ECG signal is calculated, and then mean is subtracted from the original ECG signal followed by calculation of the covariance matrix, computation of the eigenvectors and formation of a feature vector by selecting components. After this, eigenvalues are squared for minimizing smaller values and maximizing larger values and then thresholding is done to retain R-peaks (larger eigenvalues) [21].
From paper [21], it can be seen that PCA is a good tool to reduce multidimensional data to lower dimensions while retaining most of the information. Infact it has increased efficiency given the processes taking place in smaller dimensions and small variations in the background are ignored automatically and it does not does not require large computations unlike few algorithms giving accurate results. ELK plus Internet
In a paper proposed by Deboleena Sadhukhan et al, a simple algorithm has been devised for automatic detection of the R-peaks. This algorithm was based on the double derivative technique which included three stages. First, the squared double differences of the ECG signal are sorted in descending order and compared to a threshold to extract the approximate QRS regions. Second, by magnitude comparison in the detected QRS regions the R peaks are detected where in the position of the maximum of the relative magnitudes is the R point locations of the corresponding QRS window. Lastly, the RR intervals obtained were processed according to some criteria to ensure accuracy of detection [22].
MobyenUddin Ahmed et al proposed a paper to present a way of measuring the ECG signal together with the ECG component analysis such as QRS peak detection and HR calculation to use it in a computer-based stress diagnosis system. Here the inter-beat interval (IBI) was detected computationally by a very accurate detection of R peak which included a procedure where in when a sample value higher than the threshold was considered as R peak [23].
From [23], it can be seen that the reliability of the system is examined in a very short scale study but it showed the performance close to a reference system.
Awadhesh Pachauri et al devised a paper where detection of R wave was done using a Wavelet transform. The wavelets used for detection were Daubechies and Symmetric. The ECG signal under test had been decomposed to the required level using the selected wavelet and the selection of detail coefficient d4 had been done based on energy, frequency and cross-correlation analysis of decomposition structure of ECG signal. In wavelet transform, a linear operation transforms the signal to decompose it at different scales. In case of discrete wavelet transform (DWT), filters of different cut-off frequencies are used for analyzing the signal at different scales. The selected detail coefficient d4 is used to perform the detection of R-wave [24].
In papers like Vanisree K et al [25] and S. C. Saxenaet al [26], an approach for detection of R –R interval was also done using wavelet transforms using DWT and seven wavelets respectively.
From [24, 25 and 26], it can be seen that Wavelet transform (WT) is a powerful tool to study non stationary signals like ECGs and it provides a description of a signal in the time–frequency domain and works on a multiscale basis ensuring noise is filtered at each level of decomposition eliminating the requirement of any preprocessing with a reduction in errors. Signals can be analyzed by using a well-known method called Fourier Transformation as it transforms the signal from time based to frequency based and frequency content is of great importance. But the serious drawback with this approach is in transforming to frequency domain, the time information is lost. Making it impossible to tell when a particular event occurred through this approach. WT fixes this drawback of obtaining time and frequency information on time along with the fixed size of the time window. A Wavelet Transform, at high frequencies, gives good time resolution and poor frequency resolution, while at low frequencies the Wavelet Transform gives good frequency resolution and poor time resolutions.
In a paper proposed by G Vijayaet al, the detection of QRS complex or R peak is been done by using Artificial Neural Networks using Back Propagation. Also in another paper proposed by them, detection of QRS Complex was done using a Predictive Neural Network (PNN) based technique. The PNN was trained, using the back propagation algorithm, on non-QRS portions of the ECG to predict the signal one-step ahead. High prediction error was then taken as an indication of the occurrence of a QRS complex. Simple peak detection logic was then invoked to mark the exact location and magnitude of either a Q- or an R- or an S- peak within the QRS complex [28 and 29].
From [28 and 29], it can be seen that detection of the R peak or R-R interval using ANN gave a high degree of accuracy and minimized the problem associated with the noises in the ECG signal. Also the neural network based detection mechanism is easily employable when no knowledge about the signal-to-noise ratio of the training data is needed.
V. CONCLUSION
REFERENCES
[1]. Anand Kumar Joshi, ArunTomar, MangeshTomar, “A Review Paper on Analysis of Electrocardiograph (ECG) Signal for the Detection of Arrhythmia Abnormalities”, International Journal of Advanced Research in Electrical, Electronics and Instrumentation Engineering (IJAREEIE), Vol. 3, Issue 10, pp. 12466- 12475, 2014.
[2]. SonalPokharkar, AmitKulkarni ,“ECG Real Time Feature Extraction Using MATLAB”, International Journal of Technology and Science, Volume V, Issue 1, pp. 1-4, , 2015.
[3]. A.Peterkova, M. Stremy, “The raw ECG signal processing and the detection of QRS complex”, IEEE European Modelling Symposium, pp. 1-6, 2015 IEEE.
[4]. Sameer K. Salih, S.A. Aljunid, AbidYahya, Khalid Ghailan, “A Novel Approach for Detecting QRS Complex of ECG signal”, International Journal of Computer Science issues (IJCSI), Vol.9, Issue 6, No 3, pp. 205-215,2012.
[5]. Sahil Verma, Ramesh Kumar Sunkaria, Barjinder Singh Saini, “Heart Rate Determination with RR Interval and PP Interval Time Series”, International Journal of Advanced Research in Computer Science, Volume 3, No. 3, pp. 450-455, 2012.
[6]. Jiapu Pan, Willis J. Tompkins, Senior Member, “A RealTime QRS Detection Algorithm”, IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, Vol. BME32, No. 3, pp.230-236, 1985.
[7]. Shital L. Pingale, “USING PAN TOMPKINS METHOD, ECG SIGNAL PROCESSING AND DIGNOSE VARIOUS DISEASES IN MATLAB”, Proceedings of IRF International Conference, 2014.
[8]. Pankhuri Trivedi, ShahanazAyub, PhD, “Detection of R Peak in Electrocardiogram”, International Journal of Computer Applications Volume 97, No.20, 2014.
[9]. Kritika Bawa, PoojaSabherwal, “R-Peak Detection by Modified Pan-Tompkins Algorithm”, International Journal of Advancements in Research & Technology, Volume 3, Issue 5, pp.30-33, 2014.
[10]. Josef Goette, Event Detection: “Qrs-Complexes in Ecg Signals”, BioMedSigProcAna, 2017.
[11]. Natalia M. Arzeno, Zhi-De Deng, Chi-Sang Poon, “Analysis of First-Derivative Based QRS Detection Algorithms”, IEEE Trans Biomed Eng. 2008.
[12]. Frits L. Meijler, Jan Strackee, Frant J. L. van Capelle, Jeanny C. du Perron, “Computer Analysis of the RR Interval-Contractility Relationship during Random Stimulation of the Isolated Heart”, Circulation Research, Vol. XXII, pp. 695-702, 1968.
[13]. Mirja A. Peltola, “Role of editing of R-R intervals in the analysis of heart rate variability”, frontiers in physiology, Volume 3, May 2, Article 148.
[14]. Clifford, G. D.,, F. Azuaje, and P. E. McSharry, “ECG statistics, noise, artifacts, and missing data, in Advanced Methods and Tools for ECG Data Analysis”, pp. 55–99, 2006.
[15]. A.Gersten, O. Gersten, A. Ronen, Y. Cassuto, “The RR interval spectrum, the ECG signal and aliasing”, Ben-GurionUniversity of the Negev, 1999.
[16]. Faezeh Marzbanrad, Herbert Jelinek, Ethan Ng, Mikhail Tamayo, Brett Hambly, Craig McLachlan, Slade Matthews, MarimuthuPalaniswami, AhsanKhandoker, “The Effect of Automated Preprocessing of RR Interval Tachogram on Discrimination Capability of Heart Rate Variability Parameters”, Computing in Cardiology 2013.
[17]. Whitsel EA, Raghunathan TE, Pearce RM, Lin D, Rautaharju PM, Lemaitre R, Siscovick DS, “RR interval variation, the QT interval index and risk of primary cardiac arrest among patients without clinically recognized heart disease”, European Heart Journal., pp. 165-73, 2001. [18]. SoniaRezk, C´edric Join, Sadok El Asmi, “INTER-BEAT (R-R) INTERVALS ANALYSIS USING A NEW TIME DELAY ESTIMATION TECHNIQUE”, 20th European Signal Processing Conference (EUSIPCO 2012), 2012.
[19]. Mr. Vyankatesh S. Thorat, Dr. Suresh D. Shirbahadurkar, Mrs. Vaishali V. Thorat, “Classification of Cardiac Arrhythmia With Respect to ECG and HRV Signal”, International Journal of Advanced Research in Computer and Communication Engineering, Vol. 5, Issue 4, 2016. [20]. Swetha Bellari, SnehlataKumari, Celin.S, Anne Frank Joe, “Performance Analysis of R- Peak Detection Methods on ECG Signals”, International Journal of Advanced Research in Electrical, Electronics and Instrumentation Engineering, Vol. 6, Issue 3, pp. 107-111, 2017. [21]. Harjeet KAUR, Rajni RAJNI, “Electrocardiogram signal analysis for R-peak detection and denoising with hybrid linearization and principal component analysis”, Turkish Journal of Electrical Engineering & Computer Sciences, pp. 2163-75, 2017.
[22]. Deboleena Sadhukhana, MadhuchhandaMitraa, “R-peak detection algorithm for ECG using double difference and RR interval processing”, Procedia Technology, Published by Elsevier Ltd, 2012.
[23]. MobyenUddin Ahmed, Shahina Begum and Mohd. Siblee Islam, “Heart Rate and Inter-beat Interval Computation to Diagnose Stress Using ECG Sensor Signal”, School of Innovation, Design and Engineering.
[24]. Awadhesh Pachauri, and ManabendraBhuyan, “Robust Detection of R-Wave Using Wavelet Technique”, World Academy of Science, Engineering and Technology International Journal of Electronics and Communication Engineering Vol:3, No:8, 2009.
[25]. Vanisree K, JyothiSingaraju, “Automatic Detection of ECG R-R Interval using Discrete Wavelet Transformation”, International Journal on Computer Science and Engineering (IJCSE), Vol. 3, No. 4, 2011.
[26]. S. C. Saxena,V. Kumar &S. T. Hamde, “QRS detection using new wavelets, Journal of Medical Engineering & Technology”, Taylor & Francis, 2009.
[27]. Sonia Rezk , Cedric Join, Sadok El Asmi, “AN ALGEBRAIC DERIVATIVE-BASED METHOD FOR R WAVE DETECTION”, 19th European Signal Processing Conference (EUSIPCO 2011), 2011.
[28]. G Vijaya, Vinod Kumar, H. K. Verma, “ANN-based QRS-complex analysis of ECG complexes”, Journal of Medical Engineering & Technology, pp. 160-7, 1998.
[30]. Piyush Kumar TomarDeependraSinha, “Thresholding based R-Peak Detection in ECG Signals”, IJSTE - International Journal of Science Technology & Engineering, Volume 3, Issue 11, 2017.
[31]. Stefan Wunsch ; Johannes Fink ; Friedrich K. Jondral, Improved Detection by Peak Shape Recognition Using Artificial Neural Networks, IEEE, 2016.
[32]. M.B.I. Reaz ; L.S. Wei, Detection of the R wave peak of QRS complex using neural network, IEEE, 2004.
[33]. Luca Citi ; Emery N. Brown ; Riccardo Barbieri, A Real-Time Automated Point-Process Method for the Detection and Correction of Erroneous and Ectopic Heartbeats, IEEE, 2012.
[34]. Huiyue Yang ; YaqingTu ; Haitao Zhang ; Kanghui Yang, A Hilbert Transform based method for dynamic phase difference measurement, IEEE, 2012.
[35]. S.Rezk, C.Join, S.Elasmi, “An algebraicdervative-based method for R wave detection,” in Proceeedings of EUSIPCO, 19, 2011.
[36]. M. V. Kamath and E. L. Fallen, Power spectral analysis of HRV: a noninvasive signature of cardiac autonomic functions, Crit. Rev. Biomed. Eng., Vol. 21, pp. 245-311,1993.
[37]. Jing-Shiang Hwang, Tsuey-Hwa Hu, Lung Chi Chen, “An index related to autocorrelation function of RR intervals for the analysis of heart rate variability”, Physiological Measurement, 2006.
[38]. Balraj Singh, Shashi Kala Nagarkoti, PauriGarhwal, B. K. Kaushik, “A Modified Algorithm for Maternal Heart Rate Detection Using RR Interval”, IEEE, 2011.
[39]. B. U. K'ohler, C. Henning and R. Orgelmeister, “The principles of software QRS detection”, IEEE Eng. Med. Bioi. Mag.Vol. 21, pp. 42-57, 2002.
[40]. G. de Lannoy, A. de Decker, M. Verleysen, “A Supervised Wavelet Transform Algorithm for R Spike Detection in Noisy ECGs”, International Joint Conference on Biomedical Engineering Systems and Technologies, BIOSTEC: Biomedical Engineering Systems and Technologies, 2018.
[41]. Harold Martin ; Walter Izquierdo ; Mercedes Cabrerizo ; MalekAdjouadi, “Real-time R-spike detection in the cardiac waveform through independent component analysis”, IEEE, 2018.
[42]. Malcolm S. Thaller, M.D, “The Only EKG Book Youll Ever Need”.