Evaluation of a Unique, Nurse-Inserted, Peripherally Inserted Central
Catheter Program
Beth Gamulka, MDCM*‡§; Cristina Mendoza, RN*; and Bairbre Connolly, MB, BCh, BAO㛳¶
ABSTRACT. Background. Concerns regarding the safety and success of peripherally inserted central cath-eters (PICCs) placed at the bedside in the pediatric pop-ulation initially precluded the development of a nurse-inserted PICC program at our pediatric center. Previously, all PICCs were inserted by interventional radiologists (IRs) with fluoroscopic guidance. A new nurse-inserted PICC program was initiated with collab-oration between PICC nurses and IRs.
Methods. Three nurses participated in the project. Pa-tients who met preestablished selection criteria were ap-proached. All insertions were performed with sterile technique on the fluoroscopy table, with IRs available to support the PICC nurse. Veins were accessed visually or through palpation. Final tip position was confirmed in all cases with contrast material administration and fluo-roscopy. Additional fluoroscopy was performed only if placement difficulties were encountered. All patients were monitored prospectively.
Results. Ninety-nine patients (age: 3–18 years; aver-age aver-age: 13.6 years) met the selection criteria. Two pa-tients underwent primary insertion by an IR. The re-maining 97 patients underwent an insertion attempt by a nurse. Sixty-nine PICCs (71.1%) were placed successfully by a nurse, 15 (15.5%) required minor assistance from an IR, and 13 (13.4%) were inserted by an IR after an unsuc-cessful nurse attempt. No insertion complications were noted. Insertion difficulties included difficulty advanc-ing the catheter (19.6%), difficulty cannulatadvanc-ing the vein (6.2%), and tip malposition (2.1%). Postinsertion compli-cations occurred for 27.8% of PICCs, and 13.4% required removal before the end of therapy.
Conclusion. This novel, pediatric nurse-inserted PICC program has a good safety profile, high success rate, and low postprocedural complication rate. Pediat-rics2005;115:1602–1606;peripherally inserted central cath-eter, central venous cathcath-eter, nurse.
ABBREVIATIONS. PICC, peripherally inserted central catheter; TPN, total parenteral nutrition; IV, intravenous; IGT, image-guided therapy; IR, interventional radiologist.
P
eripherally inserted central catheters (PICCs) allow for middle- to long-term courses of in-travenous (IV) therapy in the hospital and at home, blood sampling, and reductions in venipunc-tures. The purpose of this study was to evaluate a new, nurse-inserted, PICC program for children at a tertiary care pediatric center.The nurse-inserted PICC program at our pediatric academic health sciences center grew out of an iden-tified need to provide long-term IV access for chil-dren. Since 1992, interventional radiologists (IRs) at our hospital inserted PICCs under fluoroscopic guid-ance. However, patients who required vascular ac-cess devices were prioritized along with other pa-tients who were dependent on the expertise of the IRs for image-guided procedures. This led to the perception by health care providers that PICC inser-tions were difficult to arrange. Consequently, health care providers turned to the IV team nurses for as-sistance with middle- to long-term vascular access.
Although nurses in the NICU inserted PICCs at the bedside, there was no similar option in the rest of our hospital. In the past, IV team nurses were able to offer midline catheters as the best alternative to short, peripheral, IV catheters. However, midline catheters are not ideal for patients who require blood sampling, treatment with vesicant drugs, long-term treatment with irritant drugs (eg, vancomycin or cloxacillin), or blood transfusions. The experience with midline catheters at our pediatric center also suggests that they are not optimal for total parenteral nutrition (TPN). In our recent review of data for 142 children with midline catheters, 52.3% of children who were receiving TPN through midline catheters could not complete therapy with this device because of complications.
Our solution to the problem of timely PICC inser-tions outside the NICU focused on the development of a pediatric nurse-inserted PICC program with sev-eral unique features. Other centers reported their experiences initiating PICC programs, but most in-volved either bedside nurse insertions or exclusively IR insertions in a fluoroscopy suite. Few studies re-ported experiences in pediatric programs.1–4
Con-cerns have been raised about the high rate of malpo-sitioned catheters inserted at the bedside, where the tip does not sit at the junction between the superior vena cava and the right atrium.5The success rate of
IRs for PICC insertion is high, primarily because of the use of ultrasonography and fluoroscopy to ob-serve the vein and to position the catheter appropri-From the *Vascular Access Program, ‡Division of Pediatric Medicine, and
㛳Department of Image-Guided Therapy, Hospital for Sick Children, To-ronto, Ontario, Canada; and Departments of §Pediatrics and ¶Diagnostic Imaging, University of Toronto, Toronto, Ontario, Canada.
Accepted for publication Oct 4, 2004. doi:10.1542/peds.2004-0542 No conflict of interest declared.
Address correspondence to Beth Gamulka, MDCM, Vascular Access Pro-gram, Hospital for Sick Children, Toronto, ON, Canada. E-mail: [email protected]
ately. In expanding our program, there was an in-centive to maintain a high insertion success rate while ensuring the safety of the procedure. Rather than initiating nurse insertions at the bedside, we developed a hybrid program combining the advan-tages of a nurse-inserted PICC program and an IR PICC service. We thus expanded our vascular access service by incorporating the new nurse-inserted PICC program in the hospital’s image-guided ther-apy (IGT) suites.
Our nurse-inserted PICC program is a collabora-tive effort between the division of IGT and the vas-cular access/IV team. All catheter insertions are per-formed in the IGT fluoroscopy suite. Three nurses with extensive experience in IV access volunteered to participate in the project and received practical train-ing from one of the manufacturers of PICC catheters. Four IRs supervised the nurses in PICC insertion.
The aim of this prospective descriptive study was to evaluate the success of a novel, nurse-inserted, PICC program. The evaluation of the program fo-cused on the insertion success rate of the PICC nurses and on periprocedural and long-term compli-cation rates for PICCs.
METHODS Patients and Study Design
All children were inpatients or outpatients at our hospital, which is a tertiary care, pediatric, academic, health sciences center. The program was initiated in December 2001, and data for all patients who met the inclusion criteria between December 2001 and June 2003 were reviewed. Patient criteria for inclusion in the nurse-inserted PICC program were established before the initia-tion of the project and reflected patients who were midline cath-eter candidates. Inclusion criteria included cooperative patients ⬎3 years of age, a history of⬍3 previous central venous catheters in the superior vena cava, and palpable or easily observed brachial or cephalic veins. Patients with a particular medical condition that necessitated general anesthesia for a procedure were excluded. However, patients who otherwise fulfilled the criteria but received general anesthesia for another procedure were included. The eval-uation of the program received approval from the hospital re-search ethics board.
Physicians, bedside nurses, and IV team nurses identified can-didates for the nurse-inserted PICC program. Once identified, the patients were triaged by a specially designated resource nurse within the vascular access program and were then assessed by a PICC nurse, to ensure that inclusion criteria were met.
We evaluated all patients who consented and underwent an attempted PICC insertion performed by a nurse. Data were gath-ered prospectively until the catheter was removed or until the end of the observation period in July 2003 (the minimal follow-up period was 21 days). Periprocedural and postprocedural compli-cations were recorded. PICC nurses assessed inpatients daily and tracked catheter function and site condition. They performed all weekly site dressing changes on inpatients. Patients discharged from the hospital with a PICC in situ were monitored by telephone by the PICC nurse. Inpatient catheter maintenance included hep-arinization with 150 units of heparin (100 U/mL solution) every 24 hours for all catheters that were accessed intermittently. Catheters with continuous infusions did not receive heparin. Outpatients received daily PICC care by a home care nurse, who followed the same heparinization and dressing policies. Problems with outpa-tient PICCs were addressed by the hospital’s PICC nurses after contact by the patient’s family or by the home care nurse. The PICC nurses provided preinsertion and postinsertion education to patients and families and performed all inpatient dressing changes.
Variables included demographic characteristics such as patient age, gender, diagnostic category, and reason for PICC insertion. Dwell time was calculated as the difference between the insertion
and removal dates. “Successful” insertions included nurse inser-tions that did not require assistance from the IR (other than confirmation of the tip position with fluoroscopy after completion of the procedure). “Successful-assisted” insertions included inser-tions in which nurses required verbal or hands-on assistance by an IR during the insertion. “Unsuccessful” insertions were those performed completely by an IR after a failed nurse attempt.
Insertion difficulties included problems cannulating the vein, advancing the catheter, or positioning the tip. Insertion complica-tions included bleeding, hemothorax, pneumothorax, arterial can-nulation, and arrhythmia. Postinsertion complications included external or internal catheter fracture, thrombosis, catheter-related local or systemic infection, as defined by national infection-control standards,6catheter occlusion, catheter dislodgment, dermatitis,
and mechanical phlebitis.
Descriptive statistics were used to examine the success rate for PICC nurses, insertion difficulty and complication rates, postin-sertion complication rates, and average dwell times. Comparisons were made between median dwell times for catheters removed because of complications and those removed at the end of therapy.
Technique
Informed consent is obtained from the parent or guardian by the PICC nurse, and assent is granted by the child. The PICC placement is performed in the IGT suite, with sterile technique. Topical anesthetic is applied to the chosen site (basilic or cephalic vein) before the procedure. All inserters use sterile technique with a combination of topical anesthetic (EMLA [AstraZeneca, Wil-mington, DE] or Ametop Gel [Smith and Nephew, Hull, United Kingdom]), skin infiltration with lidocaine, and IV sedation. Veins are accessed either by direct observation or by palpation.
The catheter is flushed with saline solution and trimmed to the correct length, with care being taken not to cut the guidewire inside the catheter. The assistant places the patient in a supine position, with the arm abducted to a 90° angle. The site is cleansed with a chlorhexidine/alcohol preparation and draped, and a tour-niquet is applied by the assistant. The vein is accessed visually or by palpation with the peel-away introducer needle at a 25° to 45° angle. The stylet from the introducer is removed, and the catheter is threaded through the peel-away sheath. The tourniquet is re-leased and the catheter is advanced centrally. The patient is asked to tuck her or his chin on the ipsilateral shoulder, to prevent the catheter from going up the jugular vein. At that point, the catheter is confirmed fluoroscopically to be in the lower one third of the superior vena cava. The guidewire is removed from the catheter. The catheter position is then confirmed fluoroscopically, with contrast agent administration, by the IR.
If the catheter does not advance or if fluoroscopy indicates that the catheter has gone into any vein other than the superior vena cava, then the IR advances the catheter over a directing guidewire until central access is obtained and confirmed with contrast agent administration. If access fails with visual landmarks or palpation, then the IR may use ultrasonography with a sterile cover in the same sterile field, without moving the patient. The PICC nurse may then be in a position to continue, or the IR may complete the procedure.
RESULTS
Ninety-nine patients requiring PICCs fulfilled the selection criteria. Ninety-seven patients (98%) under-went an initial insertion attempt by a nurse; 1 patient who had undergone a previous PICC insertion by an IR refused a nurse-inserted PICC. Another patient was not included because of an underlying coagu-lopathy. Reasons for PICC insertion included antibi-otic or antiviral therapy (N⫽ 59 [60.8%]), TPN ad-ministration (N⫽28 [28.9%]), chemotherapy (N⫽4 [4.1%]), or other medications (N ⫽ 6 [6.2%]). The average age of the children was 13.6 years (range: 3–18 years). There were 52 male patients and 45 female patients. Thirty-seven catheters were used exclusively for inpatients, whereas 60 catheters were used for outpatients.
Systems, Salt Lake City, UT]) were inserted by PICC nurses. PICCs inserted by an IR after an initial nurse attempt were either noncuffed (Bard Per-Q-Cath) or cuffed (Cook Critical Care, Bloomington, IN). Nurses inserted 81 single-lumen (3F or 4F) catheters and 3 double-lumen (4F or 5F) catheters. IRs inserted 12 single-lumen (3F or 4F) catheters and 1 double-lu-men (5F) catheter. The cephalic vein was accessed in 31 insertions and the basilic vein in 66 insertions. Topical anesthetic alone was used for 81 patients (83.5%). The remaining patients received a combina-tion of topical anesthetic and infiltracombina-tion of lidocaine (N⫽12), IV sedation (N⫽2), and general anesthesia (N⫽2).
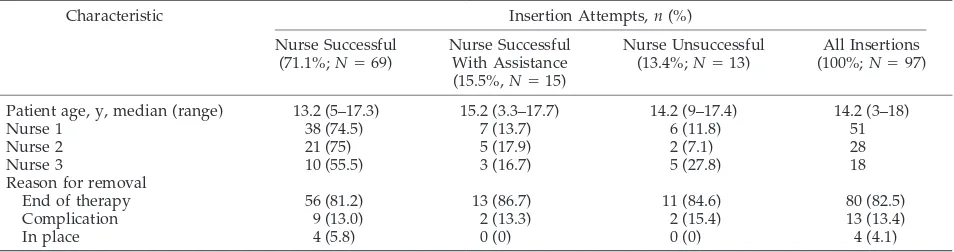
A summary of patient characteristics and insertion attempt outcomes is presented in Table 1. Sixty-nine PICCs were inserted successfully by a PICC nurse, yielding a success rate of 71.1%. Twenty-eight inser-tions required assistance. Fifteen (15.5%) of those insertions involved minor adjustments, such as repo-sitioning with fluoroscopy, saline flush, and/or guidewire, and the other 13 PICCs (13.4%) were in-serted completely by an IR after a failed attempt by the nurse. Insertion difficulties included tip malpo-sition (2.1%), difficulty cannulating the vein (6.2%), and difficulty advancing the catheter (19.6%). No insertion-related complications (bleeding, hemotho-rax, pneumothohemotho-rax, arterial cannulation, atrial perfo-ration, or arrhythmia) were observed.
Of 97 PICCs inserted, 82.5% (N ⫽ 80) were re-moved at the end of therapy and 4.1% (N⫽4) were still in place at the end of the study. Postinsertion complications are listed in Table 2. Thirteen catheters (13.4%) were removed before the end of therapy because of a catheter-related complication. Another 13 patients (13.4%) experienced complications that required treatment with the catheter in place. These patients experienced mechanical phlebitis (N ⫽ 7), dermatitis (N ⫽ 3), basilic vein thrombus (N ⫽ 1), and line blockage (N⫽2). Complications that neces-sitated removal or exchange of the catheter included catheter occlusion unresponsive to saline flush and thrombolytic agent (N ⫽ 4), dislodgment (N ⫽ 5), external catheter breakage (N ⫽ 3), and suspected catheter-related sepsis (N ⫽ 1). Two catheters frac-tured internally during planned removals at the end of therapy, and snaring procedures were required to retrieve the catheter fragments. All episodes of cath-eter fracture, dislodgment, thrombus, dermatitis, and blockage occurred with catheters used in the
outpa-tient setting. All phlebitis episodes occurred with catheters used for TPN or chemotherapy. All block-ages, dermatitis, fractures, sepsis, dislodgment, and thrombus occurred with catheters not used for TPN. Overall, the complication rate for inpatients was 6.9 cases per 1000 catheter-days and the rate for outpa-tients was 6.4 cases per 1000 catheter-days. More inpatients completed therapy (97.3%) than did out-patients (81.7%).
A comparison of dwell times showed that the me-dian dwell times for catheters removed at the end of therapy and those still in place at the end of the study were 34.5 days and 38 days, respectively. Although catheters removed because of complications had a shorter median dwell time of 22 days, this was not statistically significant, compared with catheters re-moved at the end of therapy (P ⫽.65). Dwell times for catheters used for TPN (21.5 days; range: 5– 80 days) were significantly shorter than those for non-TPN catheters (39 days; range: 6 –199 days) (P⫽.03). Because all catheters used for TPN were for inpa-tients, it is not surprising that the dwell times for inpatients and outpatients were also statistically sig-nificantly different (inpatients: 21 days; range: 5– 80 days; outpatients: 42 days; range: 7–199;P⫽ .002).
DISCUSSION
This study evaluated the initiation of a new pedi-atric nurse-inserted PICC program and raised sev-eral issues that should help direct subsequent devel-opment of the program. The ability of an on-site IR to redirect, to reposition, or to troubleshoot with fluo-roscopy represents a tremendous advantage. Ongo-ing evaluation of success rates should show an im-provement as novices become more experienced with respect to insertion-related difficulties.
TABLE 1. Insertion Attempt Outcomes
Characteristic Insertion Attempts,n(%)
Nurse Successful (71.1%;N⫽69)
Nurse Successful With Assistance (15.5%,N⫽15)
Nurse Unsuccessful (13.4%;N⫽13)
All Insertions (100%;N⫽97)
Patient age, y, median (range) 13.2 (5–17.3) 15.2 (3.3–17.7) 14.2 (9–17.4) 14.2 (3–18)
Nurse 1 38 (74.5) 7 (13.7) 6 (11.8) 51
Nurse 2 21 (75) 5 (17.9) 2 (7.1) 28
Nurse 3 10 (55.5) 3 (16.7) 5 (27.8) 18
Reason for removal
End of therapy 56 (81.2) 13 (86.7) 11 (84.6) 80 (82.5)
Complication 9 (13.0) 2 (13.3) 2 (15.4) 13 (13.4)
In place 4 (5.8) 0 (0) 0 (0) 4 (4.1)
TABLE 2. Postinsertion Complications
Type Catheters
Removed/ Exchanged,
n(%)
Treated in Place, n(%)
Occlusion 4 2
Line fracture at removal 2 0
External breakage 3 0
Mechanical phlebitis 0 7
Dislodgment 5 0
Basilic vein thrombus 0 1
Suspected line sepsis 1 0
Dermatitis 0 3
The advantages of our program include the added safety of having nurses insert PICCs in a monitored, controlled environment, rather than at the bedside. The proximity and availability of the IR and fluoros-copy allow for ongoing education and support dur-ing this early phase. The ability to troubleshoot when an insertion difficulty is encountered is important. Fluoroscopy use is limited to a contrast check of tip position at the end of the procedure for successful insertions, reducing the radiation exposure of the children, compared with insertions by IRs when lim-ited fluoroscopy guidance is used throughout the procedure. No patient transfers, delays, or compro-mise of sterility occurred when IR assistance was required. The catheters chosen for this program were noncuffed and required less pain control for inser-tion. They were selected after consultation with the IRs, to ensure compatibility with guidewires used by the IRs and to allow an easy switch from a nurse insertion to an IR insertion. This program also al-lowed for comprehensive care of inpatients by one group of nurses. The role of an expert PICC team charged with catheter and dressing care might have influenced the low postinsertion complication rate and will be explored in the future.
The evaluation of our novel program showed that nurse-inserted PICCs for children could be inserted safely with minimal anesthesia and had a low postin-sertion complication rate (13.4%). It also confirmed the experience of others who reported success rates similar to ours among novices. This pediatric nurse-inserted PICC program is unique in several ways. Given our center’s experience and needs, expansion of our PICC service needed to maintain established safety and infection-control standards. However, it also needed to allow an expected learning period for novices as they entered the program. A previous study of bedside nurse insertion in an academic cen-ter with pediatric and adult patients suggested that success rates of novices approached 74%, whereas more experienced bedside insertion rates could ap-proach 83% when a limited number of novices were trained and allowed to perform insertions at the bedside.7A similar study among adult patients
con-firmed a 74% success rate for nurse insertions at the initiation of a PICC program.4 Our program was
designed with a similar approach, albeit within the IGT suite rather than at the bedside, and our success rate matches those of previous studies, none of which were exclusively pediatric.
The collaboration between the vascular access nurses and the IGT team (including IRs, technolo-gists, and nurses) also allows for a unique multidis-ciplinary approach. Vascular access nurses join the team within the IGT suite, and their regular fol-low-up care of inpatients bridges a gap in postpro-cedural care. Previously, the IGT team only saw pa-tients within 24 hours after PICC insertion and did not attend to dressing changes or monitor complica-tions regularly, unless children required a contrast study of the catheter or catheter exchange. This pro-gram provides children with better continuity of care and offers team members a better understanding of
minor complications that do not require catheter re-moval.
The number of catheters removed because of a complication in our series was low, compared with a previous study of pediatric PICC insertions by Thia-garajan et al2 (13.4% vs 29%). Although almost one
half of the patients in that study were⬍1 year of age, the mean dwell time was 13 days, which suggests that PICCs replaced peripheral IV therapy for a sub-set of patients. In our series, the median dwell time was 34 days, and our therapy completion rate was
⬎82%, which matches another small study of pedi-atric PICCs.8Our success rate with respect to
com-pletion of therapy might be explained by the older age group of the patients or by differences in catheter care and catheter size. A significant proportion of catheters (68%) in the study by Thiagarajan et al2had
catheter tips in locations other than the vena cava or right atrium, which also might have led to higher complication rates than among our patients, because there is evidence that noncentrally placed catheter tips lead to more complications.9
The rates and types of complications that we en-countered raise some interesting points about cathe-ter care and maintenance. Only 1 suspected cathecathe-ter- catheter-related infection was found, for a patient with a positive central culture for coagulase-negative Staph-ylococcus; no tip culture was sent at the time of re-moval. All catheter dislodgments occurred among outpatients, which might reflect the quality of out-patient nursing care or the increased physical activ-ity of these children. Another complication that re-quired catheter removal or exchange was external breakage. The catheter type used by the PICC nurses does not have a repair kit, which limited the lives of catheters that fractured or leaked.
The disadvantages of this program include the logistic issues involved in coordinating the availabil-ity of PICC nurses, technologists, and IRs. Although most catheters could be inserted within 1 working day after the request, given the large size of our IGT division, coordination may be more difficult in smaller centers. Moreover, our initial inclusion crite-ria were quite limiting, with only 15.7% of all PICC insertions in the hospital during the study period qualifying for a nurse attempt. Most of that limita-tion arose from the complexity of cases treated at our center and our institution’s restrictions on sedation. No child with airway risks is given nurse-assisted sedation. We selected the group of patients for whom vascular access nurses were already inserting mid-line catheters, to minimize the confounding effects of patient cooperation on insertion success rates.
As this collaborative program matures, there will be opportunities to make the selection criteria less exclusive. As the PICC nurses develop expertise in PICC insertion, the need for assistance from the IRs is expected to decrease. This should lead to more suc-cessful nurse insertions while maintaining patient safety.
ACKNOWLEDGMENTS
Thanks go to Amina Khambalia for assisting with the data analysis and to Carolyne Pehora and Francine Faubert, PICC nurses.
REFERENCES
1. Neuman ML, Murphy BD, Rosen MP. Bedside placement of peripheral-ly-inserted central catheters: a cost-effectiveness analysis.Radiology.1998; 206:423– 428
2. Thiagarajan RR, Ramamoorthy C, Gettman T, Bratton. SL. Survey of the use of peripherally inserted central venous catheters in children. Pediat-rics.1997;99(2). Available at: www.pediatrics.org/cgi/content/full/99/ 2/e4
3. Parkinson R, Gandhi M, Harper J, Archibald C. Establishing an ultra-sound guided peripherally inserted central catheter (PICC) insertion service.Clin Radiol.1998;53:33–36
4. Barber JM, Booth DM, King JA, Chakraverty S. A nurse led peripherally
inserted central catheter line insertion service is effective with radiolog-ical support.Clin Radiol.2002;57:352–354
5. Funaki B, Zaleski GX. Radiologic versus bedside placement of peripher-ally inserted central catheters.Radiology.1998;209:284 –285
6. Division of Nosocomial and Occupational Infectious Diseases, Bureau of Infectious Diseases, Laboratory Centre for Disease Control, Health Can-ada. Preventing infections associated with indwelling intravascular ac-cess devices.Can Commun Dis Rep.1997;23(suppl 8):1–16
7. Cardella JF, Cardella K, Bacci N, Fox PS, Post JH. Cumulative experience with 1,273 peripherally inserted central catheters at a single institution.J Vasc Interv Radiol.1996;7:5–13
8. Miller KD, Dietrick CL. Experience with PICC at a university medical center.J Intraven Nurs.1997;20:141–147
9. Racadio JM, Doellman DA, Johnson ND, Bean JA, Jacobs BR. Pediatric peripherally inserted central catheters: complication rates related to cath-eter tip location. Pediatrics.2001;107(2). Available at: www.pediatrics. org/cgi/content/full/107/2/e28
CORD-BLOOD COORDINATION IS URGED
“The Institute of Medicine is recommending that the Department of Health and Human Services take steps to expand the availability of potentially life-saving stem cells from newborns’ umbilical cords. Blood saved from umbilical cords, which is rich in stem cells, could treat more than 11,000 patients a year with diseases such as leukemia, lymphoma and sickle cell anemia. Currently, 22 public cord-blood banks operate in the U.S., collecting, storing and distributing umbilical cord blood. But they do it in different ways, making it difficult for patients and doctors to find matches in a timely fashion. In addition to the public banks, a number of private facilities store cord blood for the personal use of clients. The Institute of Medicine called upon the HHS to establish quality standards for umbilical cord blood and set up a national center to coordinate the activities of blood banks, both public and closely held. Further, it said the Food and Drug Administration should license cord-blood units. . . . Last year, Congress appropriated $10 million to establish a National Cord-Blood Stem Cell Bank Program, and asked the Institute of Medicine, an independent federal research organization, to come up with a plan for getting it off the ground. Lawmakers are now considering a second piece of legislation— one that would establish the blood-bank network and fund it.”
Dumcius G.Wall Street Journal.April 15, 2005
DOI: 10.1542/peds.2004-0542
2005;115;1602
Pediatrics
Beth Gamulka, Cristina Mendoza and Bairbre Connolly
Program
Evaluation of a Unique, Nurse-Inserted, Peripherally Inserted Central Catheter
Services
Updated Information &
http://pediatrics.aappublications.org/content/115/6/1602
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/115/6/1602#BIBL
This article cites 7 articles, 0 of which you can access for free at:
Subspecialty Collections
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice
Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2004-0542
2005;115;1602
Pediatrics
Beth Gamulka, Cristina Mendoza and Bairbre Connolly
Program
Evaluation of a Unique, Nurse-Inserted, Peripherally Inserted Central Catheter
http://pediatrics.aappublications.org/content/115/6/1602
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.