The Journal in 1947 and 1997: A Dramatic Change
Abraham B. Bergman, MD
T
he opportunity to analyze the differences in what was written in the first four volumes ofPediatrics in 1948 through 1949 and the con-tents of the most recent volumes in 1996 through 1997 begs the question of why medical journals should be read. For most physicians, at least initially, it is the perceived need to “keep up.” The implied message, reinforced by medical school and residency faculty, is that those who fail to be familiar with the most late-breaking developments will invariably make mistakes and kill someone. Most physicians have an unread stack of journals on bedside tables with attendant guilt that comes as naturally to us as breathing. This dark cloud dissipates only slowly through the years as we see so much “new” infor-mation become obsolete, discredited, or simply un-used, and question the extent to which journal arti-cles affect how we practice.
It is in this realm—the relevance of journal articles to influencing medical practices—where the contents of past and current volumes diverge. In essence, althoughPediatricshas consistently been directed to-ward the interests of general pediatricians like my-self, there were a higher percentage of articles in earlier editions that affected how we practiced. In the 1996 through 1997 volumes, there is a smaller pro-portion of articles that the general pediatrician needs to read to stayau current. I do not mean to disparage my favorite journal. It is just that “keeping up” is no longer the primary reason to readPediatrics; intellec-tual stimulation and relaxed pleasure is. I enjoy read-ing the Journal in the same way I enjoy a current affairs periodical such as the New Republic. The arti-cles may not change what tests I order or what antibiotic I prescribe, but rather provide enrichment through appreciation of developments taking place in my profession.
Not surprisingly, there are similarities and differ-ences in the articles contained in the 1948 through 1949 and 1996 through 1997 volumes of Pediatrics. The most notable similarity is the consistent focus on a broad range of articles of interest to general pedi-atricians, rather than to subspecialists or scientists. Of course in the 1940s and 1950s, subspecialists did not exist. Although many pediatricians developed expertise in a particular area, few practiced
exclu-sively in a subspecialty. Pediatric practice at the time involved caring for the acutely ill, premature infants, as well as for children with chronic diseases. Thus, readers in the early years could read the Journal cover to cover, and find virtually every article rele-vant to their work. The practices of pediatricians today are so varied that it would be impossible for any journal to serve the same purpose. Yet the breadth of Pediatrics today is impressive, more so than any of its “competitors.” A pediatrician today, whether practicing in primary care, public health, a subspecialty, or an academic setting, will find at least some relevant articles in every issue.
The most notable difference in articles then and now is not so much in the subject material, but in the style of writing. In essence, articles in the early vol-umes, even those on technical subjects, are so emi-nently readable. Most were written by a single au-thor who had command of the English language. The articles are written with authority, because authors such as Helen Taussig, Grover Powers, Daniel Dar-row, Louis Diamond, and Arnold Gesellwere recog-nized as authorities.
In contrast, wading through the articles of vol-umes 97 through 100 was more of a chore. The style tends to be stilted, abbreviations are intrusive, jargon is abundant, and there are too many voluminous tables and figures that are appreciated only by math-ematically minded gnomes.
The deterioration in the quality of medical writing mirrors the pathetic state of medical speaking, in which the objective of most speakers seems to be assaulting the audience with a mass of computer-generated, multicolored slides in a darkened room. I believe that most of our young trainees believe that the first words of any medical lecture must be “lights out, first slide please.”
Subjects Not Covered
Although the subject of papers in the early editions of Pediatrics reflected the problems confronted in practice, there also were many clinical issues that pediatricians were dealing with at the time about which little or nothing was written. Children were subjected to many practices that would later be sidered barbaric. Parents were told rather than con-sulted about what was going to happen to their child and seen more as impediments than facilitators of the medical care process. Visiting hours in hospitals were strictly limited. An indelible memory that I retain from my first year at Western Reserve Univer-sity Medical School in 1954 was a field trip to Rain-bow Convalescent Hospital in Cleveland, OH. From the Departments of Pediatrics of Harborview Medical Center and the
University of Washington School of Medicine, Seattle, WA. Received for publication Mar 19, 1998; accepted Mar 19, 1998.
Address correspondence to: Abraham B. Bergman, MD, Box 359774, Har-borview Medical Center, 325 9th Ave, Seattle, WA 98104.
Wards were filled with children “convalescing” from acute rheumatic fever, poliomyelitis, rheumatoid ar-thritis, and Legge–Calve–Perthe’s disease. Many of them were on bedrest for 2 years! When I started working at Children’s Hospital in Seattle, WA, in 1964, the operating room schedule was filled tonsil-lectomy/adenoidectomies and procedures to “cor-rect” femoral anteversion, tibial torsion, flat feet, pec-tus excavatum, and umbilical hernias. None of these issues, however, are discussed. Why? Hoary tradi-tion and authority were very much part of the med-ical scene. Few controlled clinmed-ical trials were carried out because of both the paucity of funds and the implied threat to established practices. Individual physicians exercised exclusive control over their pa-tients; corporate entities such as hospitals had little influence over how physicians practiced. The three worst words in medicine, “in my experience,” were in common use and ensured that the thoughts of those with the whitest hair and longest beards would prevail. It was not until the 1970s that Staheli and colleagues were able to show that rotational “defor-mities” of the lower extremities such as tibial torsion and femoral anteversion corrected themselves.1
Overview of Volumes 1 Through 4
Pediatrics was an all-inclusive journal in 1948 through 1949; “all the (pediatric) news fit to print.” In addition to the original articles, there were three special features sections: the pediatrician and the public; trends in health legislation and administra-tion; and public health, nursing, and medical social work, as well as proceedings and reports of the American Academy of Pediatrics (AAP). Medical newsletters, “throwaway” journals, and Ross round-tables and conferences did not yet exist. Neither did continuing medical education courses in exotic loca-tions.
A sense of pure pleasure accompanied a perusal of the old issues; it was like meeting up with old friends. That is in part attributable to their nontech-nical nature and discussion of issues familiar to most all clinicians, along with more skillful use of the English language. Opinions are expressed clearly, most in the first-person. An example of clear writing is the conclusion of the first paper describing “room-ing-in”:
We are not holding a brief for rooming-in as a panacea . . . On the contrary, we believe there are many parents for whom it is not applicable; nor can it serve to prevent difficulties in children of very unhappy or disturbed parents. But we do believe that for children of natural happy and healthy parents it can offer protection against some of the severe emotional difficulties of children which the routinized child care re-gimes of yesteryear have encouraged.2
Another example is the conclusion of a review by Grover Powers on the feeding of premature infants:
No new concepts of infant nutrition have been presented, but an old one is emphasized . . . it is that infants dietaries [sic] can be understood intelligently only when analyzed in terms of the unit of metabolism; the calorie.“3
Would a present-day review boldly state that ”no new concepts . . . have been provided?“ I doubt it.
Comparisons
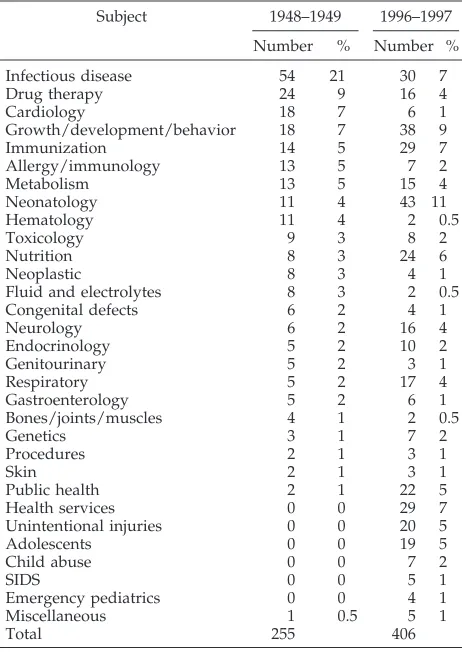
Table 1 shows the subjects of original articles cov-ered in volumes 1 through 4 with volumes 97 through 100. Because my classification of the papers was done arbitrarily (ie, is pneumonia in the new-born classified under neonatology, pulmonary, or infectious disease?), little credence should be placed in the exact numbers. I am impressed more with the similarities than the differences. Not surprisingly volumes 1 through 4 contained fewer original pa-pers, 255, compared with 406 in volumes 97 through 100. The stable of pediatric research workers has expanded greatly, and for many of them, the need to publish papers is as basic as imbibing food and wa-ter.
Articles on infectious disease, growth, develop-ment and behavior, immunization, drug therapy, and nutrition are well represented in both time pe-riods. Public health and health services papers now appear as original contributions. The contrasts are more interesting. Neonatology, the subject of 4% of papers in the early volumes, now tops the list at 11%. PerhapsPediatrics might draw more manuscripts in that field because a neonatologist, Jerold Lucey, has been the editor since 1973.
Eighteen papers (7%) in cardiology were pub-lished in the first 2 years, compared with 6 (1%) in the most recent period. There were 11 papers in hematology (4%) and 8 papers on cancer (3%) in the early years, compared with the current 6 in cardiol-ogy (1%), and 4 (1%) on cancer. General pediatricians
TABLE 1. Subjects ofPediatricsArticles 1948 –1949 Versus 1996 – 1997
Subject 1948–1949 1996–1997 Number % Number %
Infectious disease 54 21 30 7
Drug therapy 24 9 16 4
Cardiology 18 7 6 1
Growth/development/behavior 18 7 38 9
Immunization 14 5 29 7
Allergy/immunology 13 5 7 2
Metabolism 13 5 15 4
Neonatology 11 4 43 11
Hematology 11 4 2 0.5
Toxicology 9 3 8 2
Nutrition 8 3 24 6
Neoplastic 8 3 4 1
Fluid and electrolytes 8 3 2 0.5
Congenital defects 6 2 4 1
Neurology 6 2 16 4
Endocrinology 5 2 10 2
Genitourinary 5 2 3 1
Respiratory 5 2 17 4
Gastroenterology 5 2 6 1
Bones/joints/muscles 4 1 2 0.5
Genetics 3 1 7 2
Procedures 2 1 3 1
Skin 2 1 3 1
Public health 2 1 22 5
Health services 0 0 29 7
Unintentional injuries 0 0 20 5
Adolescents 0 0 19 5
Child abuse 0 0 7 2
SIDS 0 0 5 1
Emergency pediatrics 0 0 4 1
Miscellaneous 1 0.5 5 1
in the 1940s and 1950s were actively involved in the care of children with heart disease and cancer; now they fall within the realm of subspecialists.
No articles appeared in the early volumes on either intentional or unintentional injuries. Child abuse and sudden infant death syndrome were yet to be “dis-covered.” Neither were there any articles on adoles-cent medicine. The pediatric realm ended at puberty.
Landmarks
There is no standard definition for the type of article to which the landmark appellation can be applied. My definition is an original description of a disease or treatment that profoundly effects patient management. Although nostalgia for the old days doubtless affects my objectivity, I am still struck by the large number of papers in the first four volumes that can be considered landmarks. Here are just a few:
Bloxsom A, Powell N. The treatment of acute tem-porary dysfunction of the kidneys by peritoneal irri-gation.Pediatrics. 1948;1:52–57.
Swenson O. Diagnosis and treatment of atresia of the esophagus and tracheo-esophageal fistula. Pedi-atrics. 1948;1:195–204.
Taussig HB. Tetralogy of fallot: especially the care of the syanotic [sic] infant and child.Pediatrics. 1948; 1:307–314.
Elmore SE. Ingestion of mercury as a probable cause of acrodynia and its treatment with Dimerca-prol (BAL; Report of Two Cases). Pediatrics. 1948;1: 643– 647.
Wenner HA, Tanner WA. Poliomyelitis in families attacked by the disease. II. The presence, appearance and persistence of neutralizing antibodies.Pediatrics. 1948;2:190 –199.
Rabe EF. Infectious croup. I. Etiology. Pediatrics. 1948;2:255–265.
Diamond LK. Replacement transfusion as a treat-ment for erythroblastosis fetalis. Pediatrics. 1948;2: 520 –524.
Johnson AL, McRae DL. Combined use of angio-cardiography and cardiac catheterization in the di-agnosis of congenital anomalies of the cardiovascular system.Pediatrics. 1948;2:643– 651.
Riley CM, Day RL, McL. Greeley D, Langford WS. Central autonomic dysfunction with defective lacri-mation. I. Report of five cases.Pediatrics. 1948;3:468 – 478.
Dammann JF, Gibson S, Potts WJ. Observations on 117 patients operated on for congenital pulmonary stenosis.Pediatrics. 1948;3:575–587.
Swenson O, Neuhauser EBD, Pickett LK. New con-cepts of etiology, diagnosis and treatment of congen-ital megacolon (Hirschsprung’s Disease). Pediatrics. 1948;4:201–209.
Behavioral/Developmental Pediatrics
I had not expected the early volumes ofPediatrics
to contain so many papers on psychosocial, behav-ioral, and developmental subjects. I was wrong. There is a treasure trove of papers written by leaders in the field. The emphasis in all of them is on how the general pediatrician can use the information in
prac-tice. Here is what C. Anderson Aldrich said on the subject of orderly or lawful behavior:
Any person at all familiar with the development of chil-dren in modern times must be impressed with the fact that no one can grow up and live a happy life today unless he learns to conform to the major tenet of social customs. This means that no doctor with any sensitivity to children’s needs will advise that they be allowed always “to do as they please.” Everything that is said in this article is designed not to pro-mote license, but to make conformity possible where it has been extremely difficult or impossible to achieve in the past.4
Arnold Gesell thoughtfully spells out his defini-tion of developmental pediatrics,5 and Bruch and McCune provide helpful hints on managing behav-ior issues, complete with a New Yorker cartoon.6 Benjamin Spock, then in private pediatric practice in New York, proffers this common-sense approach to discipline:
Children are parasitic on their parents for their physical and emotional needs. The good parent must use his or her good judgment, decisiveness and leadership a hundred times a day in steering, stooping, and starting the average small child. The child not only gets into trouble without control; he is miserable without it.7
The consequences of overprotection of children with chronic illness are nicely communicated in a study by two social workers at the Beth Israel Hos-pital in Boston, MA. No behavioral scales and no statistical tests are applied—just good description.8
Some of the studies published, however valuable the information gained, would not pass muster with present-day institutional review boards. The normal values of pancreatic enzymes were determined in 47 healthy children between 11 months and 10 years of age in a hospital in Budapest, Hungary. “The duo-denal contents were collected after a fasting period of 6 –12 hours. The older the child, the longer he was deprived of food.”9 Seeking a cause for retrolental fibroplasia (RLF), the eyes of five premature infants were shielded from 35 to 60 days after birth. Four of the five developed RLF. It was concluded that “lights is not an etiologic factor of RLF in premature in-fants.”10
Overview of Volumes 97 Through 100
As mentioned above, infectious diseases, immuni-zations, nutrition, growth and development, and be-havior remain as important topics. But the explosion of new knowledge would cause readers in 1949 to think that they were reading science fiction. The positive pressure ventilator and newer methods of imaging have had the most profound effects on the care of children; there are plenty of articles describ-ing ways in which they are used. Ventilators, surfac-tant, and other advances in neonatology have low-ered dramatically the weight at which premature infants can be expected to survive. But survive how? Twenty papers were published in these four volumes on the developmental outcome of very low birth weight infants, most of them showing salutary re-sults.
exam-ple, to show the adverse effects of poverty on prac-tically everything? My reaction to too many articles was “so what!” I am skeptical of papers that present data, but do not provide hints on how that data may used to help children.
The field of biostatistics did not exist in the late 1940s, and quantitative analysis certainly beats “in my experience” as a way of making judgments. But do the pages ofPediatricshave to be cluttered with so many t tests and P values? None other than Sir Austin Bradford-Hill, an inventor of modern statis-tical analysis said:
I wonder whether the pendulum (requiring the employ-ment of statistical measures of significance) has not swung too far . . . fortunately I believe we have not yet gone so far as our friends in the USA where, I am told, some editors of journals will return an article because tests of significance have not been applied. Yet there are innumerable situations in which they are totally unnecessary— because the difference is grotesquely obvious, because it is negligible, or because, whether it be formally significant or not, it is too small to be of any practical importance. What is worse, the glitter of the
ttable diverts attention from the inadequacies of the fare.11
The immediate post-World War II era was rela-tively good for children. In the intervening 5 de-cades, attributable in large measure to the profusion of single-parent households, their collective state of well being has plummeted. Thus, the recent pages of
Pediatricscontain papers about the scourges of mod-ern society: drugs; homelessness; foster care; sexu-ally transmitted diseases, including AIDS; and the terrible toll extracted by traffic, guns, cigarettes, and other implements of our overdeveloped society. We also read more about children with chronic diseases, multiple handicaps, and learning disorders. And cer-tainly issues involving gay and lesbian youngsters would not have been recognized, let alone written about in the late 1940s.
Landmarks
It takes years after publication before the impact of a paper is known. Identifying landmark papers in the 1996/1997 volumes, therefore, is guesswork at best. Nevertheless, I doubt that many papers in these volumes will affect profoundly the way that patients are managed. That is because the authors of “break-through” papers first try publications higher on the academic prestige scale like Nature or the New En-gland Journal of Medicine. None of the wonderful ge-netic discoveries in cystic fibrosis, for example, have been published inPediatrics. Also, many present day pediatric subspecialists identify more with their adult medicine counterparts than with pediatricians, and submit papers to subspecialty journals.
Nevertheless, with much trepidation, I nominate the following papers for potential landmark status:
The Vermont-Oxford Neonatal Network. Compar-ison of surfactants in respiratory distress syndrome.
Pediatrics. 1996;97:1–7.
Langnas AN, Shaw BW, Antonson DL, et al. Pre-liminary experience with intestinal transplantation in infants and children.Pediatrics. 1996;97:443– 449.
Ruel MT, Rivera JA, Santizo MC, et al. Impact of zinc supplementation on morbidity from diarrhea
and respiratory infections among rural Guatemalan children.Pediatrics. 1997;99:808 – 813.
Keszler M, Houchang D, Modanlou D, et al. Mul-ticenter controlled clinical trial of high-frequency jet ventilation in preterm infants with uncomplicated respiratory distress syndrome. Pediatrics. 1997;100: 593–599.
Although not a landmark, the following paper, a first-person account by a victim of Munchausen-by-proxy syndrome, offered a startling contrast to what usually appears in current medical journals:
Bryk M, Siegel PT. My mother caused my illness: the story of a survivor of Munchausen by proxy syndrome.Pediatrics. 1997;100:1–7.
Common Problems
What about papers on common problems? With the exception of a few papers emanating from the offices of practitioner-researchers like Breese, Dis-ney, and their colleagues in Rochester, NY,12 most research on common problems was carried out in the clinics of inner city teaching hospitals. Bless the AAP, and its president at the time, Robert Haggerty, for creating the Pediatric Research in Office Settings. As a consequence, information helpful in dealing with the day-to-day problems of community practitioners is emerging, such as when secondary sexual charac-teristics and menses occur in young girls.13
The general pediatricians also was helped by learning that “super glue” can be used instead of sutures to close lacerations,14 most epidural hemor-rhages are associated with unintentional head trau-ma,15the routine urinalysis is useless,16and, from the indefatigable otitis investigators from Pittsburgh, PA, fewer children should be treated with antibiotics for shorter durations.17
CONCLUSIONS
More similarities than contrasts emerged from an examination of the subjects covered in the first four volumes of Pediatrics compared with those covered most recently. It is gratifying that as the official jour-nal of the AAP, the articles remain directed to the broadest possible range of child health practitioners. The primary differences have to do with the scope of practice in 1948/1949 compared with the problems confronting present day pediatricians. Writing styles, however, have changed for the worse; the papers in earlier volumes are easier to read. A plea is made to remedy this situation by returning to clearer writing styles.
REFERENCES
1. Staheli LT, Engel GM. Tibial torsion: a method of assessment and a survey of normal children.Clin Orthop.1972;86:183–186
2. Jackson EB, Olmsted RW, Foord A, Thoms H, Hyder K. A hospital rooming-in unit for four newborn infants and their mothers.Pediatrics.
1948;1:28 – 43
3. Powers GF. Some observations on the feeding of premature infants based on twenty years’ experience at the New Haven Hospital. Pediat-rics.1948;1:145–158
4. Aldrich CA. On the subject of orderly or lawful behavior.Pediatrics.
1948;1:725–732
5. Gesell A. Developmental pediatrics: its task and possibilities.Pediatrics.
6. Bruch H, McCune DJ. Psychotherapeutic aspects of pediatric practice.
Pediatrics.1948;2:405– 409
7. Spock B. Chronic resistance to sleep in infancy.Pediatrics.1948;4:89 –93 8. Cohen E, Herrmann RL. Social adjustment of six patient with hemophilia
prior to and during prophylactic treatment.Pediatrics.1949;3:588–597 9. Veghelyi PV. Pancreatic enzymes: normal outpatient and comparison of
different methods of assay.Pediatrics. 1949;3:749 –764
10. Hepner WR, Krause AC, David ME. Retrolental fibroplasia and light.
Pediatrics.1949;3:824 – 829
11. Bradford-Hill A. The environment and disease: association or causa-tion?Proc Royal Soc Med.1965;58:295–300
12. Breese BB, Fiseney FA, Talpey WB, Green JL. Beta-hemolytic strepto-coccal infection. The clinical and epidemiologic importance of the num-ber of organisms found in cultures.Am J Dis Child.1987;119:18 –26
13. Herman-Giddens ME, Slora EJ, Wasserman RC, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the pediatric research in office settings network.Pediatrics.1997; 99:505–512
14. Bruns TB, Simon HK, McLario DJ, et al. Laceration repair using a tissue adhesive in a children’s emergency department. Pediatrics. 1996;98: 673– 675
15. Shugerman RP, Paez A, Grossman DC, et al. Epidural hemorrhage: is it abuse?Pediatrics.1996 97:664 – 668
16. Kaplan RE, Springate JE, Feld LG. Screening dipstick urinalysis: a time to change.Pediatrics.1997;100:919 –921
1998;102;186
Pediatrics
Abraham B. Bergman
The Journal in 1947 and 1997: A Dramatic Change
Services
Updated Information &
http://pediatrics.aappublications.org/content/102/Supplement_1/186
including high resolution figures, can be found at:
References
BIBL
http://pediatrics.aappublications.org/content/102/Supplement_1/186#
This article cites 16 articles, 12 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/standard_of_care_sub Standard of Care
http://www.aappublications.org/cgi/collection/workforce_sub Workforce
ev_sub
http://www.aappublications.org/cgi/collection/teaching_curriculum_d Teaching/Curriculum Development
b
http://www.aappublications.org/cgi/collection/medical_education_su Medical Education
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
1998;102;186
Pediatrics
Abraham B. Bergman
The Journal in 1947 and 1997: A Dramatic Change
http://pediatrics.aappublications.org/content/102/Supplement_1/186
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.