Bridging the Gap: Building Sustainable Partnerships Between Community Health Centers and Intimate Partner Violence Services in North Carolina
By
Susannah Matthai
Senior Honors Thesis School of Nursing
University of North Carolina at Chapel Hill
April 26th, 2019
Approved:
Table of Contents
Abstract………. 3
Bridging the Gap ……….………. 4
Background...………. 5
Epidemiology……….. 5
Health Implications ………..……….. Effect on Community ………..……….. Literature Review……….. Forum Report……… Pre-Registration………... Agenda………. Results……….. Discussion……… Conclusion………. 6 8 9 16 17 18 20 25 28 Acknowledgements………... References………. 29 31 Appendices……….... 35
Abstract
Rates of intimate partner violence (IPV) in North Carolina are significantly higher than the national average, with lifetime prevalence estimated at 44% for women and 19% for men. IPV contributes to greater health burden, leading to significant short- and long-term physical, mental, and behavioral health consequences. The purpose of this project was to conduct a community forum to bring together key stakeholders to identify ways community health centers and IPV service agencies can work together to address health needs of survivors. The UNC School of Nursing partnered with the North Carolina Coalition Against Domestic Violence to conduct this forum. During the event, participants utilized a group priority sort model to determine priority health care needs and populations in need of services. The highest priority health care needs included 1) trauma-informed health care services, 2) bilingual services, and 3) emergency health care. The highest priority populations were 1) victims/survivors of human trafficking and sexual violence, 2) LBGTQ+ individuals, and 4) individuals with disabilities. Participants also
conducted a SWOT analysis, brainstorming strategies to capitalize on new partnerships and opportunities to improve care services. Strategies focused primarily on the efficient use of resources and addressing the needs of vulnerable populations. The forum identified several strategies to narrow gaps in care and recommendations for sustaining partnerships between community health centers and IPV service agencies. With this information, it is the hope that the forum can be replicated in the other regions of North Carolina in order to improve services statewide.
Keywords: intimate partner violence, domestic violence, community forum, community health center
Bridging the Gap: Building Sustainable Partnerships Between Community Health Centers and Intimate Partner Violence Services in North Carolina
According to the Centers for Disease Control and Prevention (CDC), intimate partner violence (IPV) is a serious, preventable public health concern that includes intentionally
assaultive and coercive behavior including physical harm, sexual assault, stalking and emotional abuse, inflicted by an intimate partner onto another (Breiding, Basile, Smith, Black, &
Mahendra, 2015). IPV may be more commonly known as domestic violence, however, the term has been updated to account for violence occurring outside of the traditional framework of
“familial relations” and for violence occurring outside of the home (Salber & Taliaferro, 2006).
Other terms used to describe IPV include family violence, dating violence, and spousal abuse.
An intimate partner includes current or former spouses, boyfriends and girlfriends, and ongoing sexual partners of same or opposite sex (Salber & Taliaferro, 2006). It is important to note that sexual intimacy is not necessary for violence or abuse to meet the classification requirements.
Victims of IPV often need assistance with a variety of issues requiring appropriate referral to health, social, legal, and financial services. According to Miller & McCaw (2019), victims of IPV are more likely to seek healthcare services than those without a history of IPV. This is most likely a result of the health consequences associated with violence; thus, healthcare providers not only need to be equipped to treat survivors, but they must also be knowledgeable about other services victims may need and how to connect them with these services.
The purpose of this paper is to first, provide an overview of IPV and its significance as a pervasive public health problem. Secondly, this paper will include a review of the literature examining the role of the healthcare system and providers in addressing the needs of those affected by IPV. Third, this paper will report the events and findings of a community forum,
held in partnership by the School of Nursing at the University of North Carolina at Chapel Hill and the North Carolina Coalition Against Domestic Violence (NCCADV), to engage local healthcare stakeholders on building sustainable partnerships between community health centers and domestic violence programs in order to narrow gaps of care and strengthen continuity of care for community members seeking services. Finally, recommendations will be made for the direction of future initiatives in order to address gaps in care for community members affected by IPV.
Background Epidemiology
Despite being underestimated and underreported, most recent data indicates an
astonishingly high prevalence of IPV. In the United States, over ten million men and women experience physical harm by a partner each year (Breiding et al., 2015). To put this in
perspective, more than 1 in 4 women and 1 in 10 men have experienced either physical harm, sexual assault, or stalking by a former or current intimate partner in their lifetime (Breiding et al., 2015). While there are certain factors increasing the risk of IPV, it can happen to anyone
regardless of gender, age, sexual orientation, ethnicity, race, culture, religion, or socioeconomic status. Both men and women experience forms of IPV, however, statistics indicate that women are impacted significantly more by IPV (Smith et al., 2015). The National Intimate Partner and Sexual Violence Survey specifics that 1 in 5 women experienced rape, 1 in 6 were stalked, and 1 in 4 experienced sexual or physical violence by an intimate partner and reported IPV-related health concerns (Smith et al., 2015). Comparatively, 1 in 14 men were forced to sexually penetrate another person, 1 in 17 were stalked, and 1 in 10 experienced sexual or physical violence by an intimate partner and reported IPV-related health concerns (Smith et al., 2015).
Additionally, many of those affected are victimized under the age of 25, with a large partition experiencing their first victimization in childhood or adolescence (Breiding et al., 2011).
Collectively, these numbers highlight IPV as an extensive public health concern requiring an immediate increase in prevention efforts nationwide to reduce the occurrence of IPV and promote healthy intimate relationships.
In North Carolina, the prevalence of IPV is significantly higher than the national average, with the lifetime prevalence estimated at 44% for women and 19% for men (United Health Foundation, 2018). According to the North Carolina Violent Death Reporting System, 20% of homicides were due to domestic violence in 2015 (North Carolina Department of Health and Human Services). North Carolina’s unusually high statistics emphasize the need for new, innovative strategies to reduce risk factors, increase protective factors, mitigate the negative short- and long-term effects of IPV, and prevent it from occurring in the first place.
Health Implications
Acute harm from IPV may result in hospitalization, disability, and even death (Black, 2011). While the immediate harm of physical violence is significant, there are also negative long-term health consequences associated with IPV. According to the CDC (2015), individuals experiencing IPV are at higher risk for adverse health outcomes compared to many other
conditions, such as obesity, diabetes, and smoking. Approximately 80% of female survivors and 35% of male survivors experience long term health effects from sexual violence (Gerberding et al., 2008). Women in ongoing abusive relationships are 70% more likely to have heart disease, 80% more likely to experience a stroke, and 60% more likely to develop asthma (Gerberding et al., 2008). Furthermore, the perpetrating partner may influence the ability of the patient to seek
and adhere to treatments, obtain prescriptions, and make it to medical appointments. Table 1 presents some of the most common negative health outcomes associated with IPV.
TABLE 1: NEGATIVE HEALTH OUTCOMES ASSOCIATED WITH IPV (Centers for Disease Control and Prevention, 2015)
Physical Psychological & Behavioral During Pregnancy
Acute physical injuries PTSD Delayed prenatal care
Death Anxiety Preterm birth
Migraines Depression Neonatal death
Chronic pain Suicidal ideation Antenatal hemorrhage
Fibromyalgia Low self-esteem Intrauterine growth restriction Gastrointestinal disorders Disordered eating Uterine rupture
Asthma Disrupted sleep patterns Increased drug and alcohol use Cardiovascular and circulatory
conditions
Increased alcohol consumption
Increased homicide Sexually transmitted
infections
Increased drug usage Preterm birth Bladder and kidney infections High-risk sexual behaviors Neonatal death Pelvic inflammatory disease
Unintended pregnancies Sexual dysfunction
Health implications of IPV are not limited to solely the partner being abused.
Approximately 5 million children are exposed to IPV every year and face ramifications as a result (Turner, Finkelhor, & Ormrod, 2010). Of these 5 million children, 45-70% are also victims of the abuse (Salber & Taliaferro, 2006). Regardless of whether or not a child is directly
harmed, being exposed to IPV has significant implications, affecting the emotional, behavioral, and cognitive development of the child. For example, children are a risk of developing
aggressive tendencies, increasing their likelihood of being a perpetrator themselves later in life (Turner, Finkelhor, & Ormrod, 2010). Additionally, they are at risk for depression, anxiety, phobias, low self-esteem, trouble sleeping, and somatic complaints such as stuttering or learning disabilities (Salber & Taliaferro, 2006). These factors may have a lasting effect that carry on into adolescence and even adulthood. It is important to note that perpetrators may also
experience negative health outcomes as a result of their violence, thus contributing to the overall health implications of IPV at large (Salber & Taliaferro, 2006).
Effect on Community
IPV not only has an impact on the individual and the family, but it also negatively influences our workplace, education systems, social services, the criminal justice system, our health care system and the economy (Salber & Taliaferro, 2006). The annual estimated cost of domestic violence is $460 billion (Lomborg & Williams, 2018). According to the National Bureau of Economic Research, each sexual assault costs society approximately $267,000 (Lindo, Siminski, & Swensen, 2015). These costs include healthcare services, judicial system expenses, and lost productivity of the victim and of the possible incarcerated offender. An estimated 8 million days of paid work are lost yearly due to IPV (Rothman, Hathaway, Stidsen, & de Vries, 2007).
In North Carolina, 67 out of 86 identified IPV programs participated in the National Census of Domestic Violence Services to report information about services provided during a 24-hour period in 2016. The findings of the report indicate 1,502 victims were served in this 24- hour period, with 812 seeking refuge in emergency shelters or transitional housing (National Census of Domestic Violence Services, 2016). Due to lack of resources, 147 requests were unmet by IPV services during the same 24-hour period (National Census of Domestic Violence Services, 2016). This report emphasizes the need and importance of IPV services and reiterates the breadth of the problem facing communities and society at large.
Given the high rates of IPV along with the negative impact it has on an individual’s health and the larger community, the role of the healthcare system is crucial in order to alleviate and reduce the burden of IPV. It is critical that a formalized and routine approach to screening
for and responding to IPV be established across clinical settings and providers. This requires providers to have adequate training, proper knowledge of reporting protocol, thorough
understanding of available services, and the ability to appropriately connect patients with these services. As such, this report will begin by conducting a literature review overviewing the current role of the healthcare system and provider in addressing the needs of patients seeking IPV services, examining identified barriers and the response to these challenges.
Literature Review
Past research on IPV has established the fact that healthcare visits provide a unique opportunity for providers to screen patients, particularly women, for IPV. As such, several guidelines and recommendations for screening women for IPV in healthcare setting have been produced. Current recommendations from the U.S. Preventive Service Task Force (USPSTF) suggest that all women of reproductive age be screened for IPV by providers. A woman who screens positive should be provided with or referred to intervention services (USPSTF, 2013).
These recommendations follow sufficient evidence that detection and intervention have minimal risks, are effective in identifying past and current risk of IPV, and result in significant benefits including a decrease in abuse and physical or emotional harm (Curry, 2018). Despite these recommendations, IPV screening rates among providers in actual practice remain low (Swailes, 2017). A possible explanation for this is that there is a general “lack of consensus regarding what constitutes best practices for detection and early intervention of IPV”, challenging providers with identifying and implementing effective methods when assisting victims (Williams, Halstead, Salani, & Koermer, 2016, p. 2193). Thus, there is a need to identify barriers facing healthcare providers in order to increase screening rates and standardize comprehensive care to better address needs of those seeking services.
Current research has focused on just this issue, examining actual implementation of screening protocols for IPV in acute care settings and the barriers providers face in responding to disclosures. Findings from this research indicate that screening practices vary greatly across care facilities and that providers are relying on “handoffs” to social workers in response to a positive screen (Alvarez, Debnam, Alexander, & Glass, 2018). Some barriers faced by physicians include la ack of knowledge, inadequate training in trauma-informed care, personal discomfort with the issue, and time constraints (Sprague et al., 2002). As a result of these barriers, victims are not being appropriately treated or connected with essential resources to help them meet immediate safety needs along with short and long term emotional, physical, social, and financial needs.
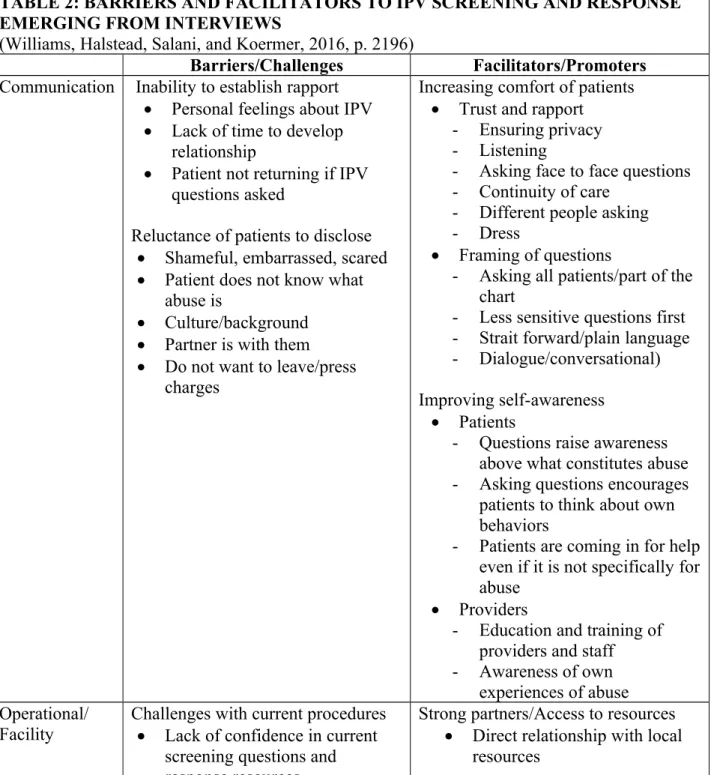
A study conducted by Williams, Halstead, Salani, and Koermer (2016) explored how screening methods were implemented in clinic and emergency care settings in order to identify barriers and facilitators providers experience when responding to IPV. In-depth interviews with healthcare providers knowledgeable about the screening protocols within their institution were used to collect data from 16 healthcare facilities. The results from these interviews indicated that providers respond to IPV on a spectrum ranging from doing nothing to conducting extensive assessments of acuity and safety, with the majority of participants falling in the middle of this continuum (Williams et al., 2016). The study identified barriers and facilitators related to communication and operational/facility structure. Communication barriers related to the patient’s unwillingness to disclose and inability to establish rapport with the patient, while communication facilitators were related to increasing the patient’s comfort and improving self- awareness of both patients and providers (Williams et al., 2016). Operational/facility barriers were challenges with current procedures and facility concerns such as time limitations and lack
of privacy (Williams et al., 2016). Comparatively, operational/facility promoters were having strong partners and access to resources and time and availability (Williams et al., 2016). A complete list of barriers and facilitators identified through this study are outlined in Table 2 below.
TABLE 2: BARRIERS AND FACILITATORS TO IPV SCREENING AND RESPONSE EMERGING FROM INTERVIEWS
(Williams, Halstead, Salani, and Koermer, 2016, p. 2196)
Barriers/Challenges Facilitators/Promoters Communication Inability to establish rapport
Personal feelings about IPV
Lack of time to develop relationship
Patient not returning if IPV questions asked
Reluctance of patients to disclose
Shameful, embarrassed, scared
Patient does not know what abuse is
Culture/background
Partner is with them
Do not want to leave/press charges
Increasing comfort of patients
Trust and rapport - Ensuring privacy - Listening
- Asking face to face questions - Continuity of care
- Different people asking - Dress
Framing of questions
- Asking all patients/part of the chart
- Less sensitive questions first - Strait forward/plain language - Dialogue/conversational) Improving self-awareness
Patients
- Questions raise awareness above what constitutes abuse - Asking questions encourages
patients to think about own behaviors
- Patients are coming in for help even if it is not specifically for abuse
Providers
- Education and training of providers and staff
- Awareness of own experiences of abuse Operational/
Facility Challenges with current procedures
Lack of confidence in current screening questions and response resources
Strong partners/Access to resources
Direct relationship with local resources
- Lack of standardized procedures
- Current procedures seem ineffective
Unsure of how to ask questions in a comfortable way
Facility concerns
Time limitations
Lack of privacy (for EDs)
Competition among facilities
Prompts and reminders Time and availability
Scheduling sufficient time
Prompts and reminders
Private rooms
Access to provider phone/email
These findings indicate important aspects of the care process that affect implementation of provider screening and response to IPV. The authors recommended the use of a multilevel approach in order to address the many factors influencing effective screening implementation and response (Williams et al., 2016). Additionally, they call for improved dissemination strategies for available resources as many participants were unware of various established screening and counseling toolkits and assessment instruments (Williams et al., 2016).
Recommendations to improve communication strategies were also given, such as: ensuring patients are educated on what constitutes violence, ensuring privacy, utilizing nonthreatening language and approach, and shaping response strategies to align with the goals and desires of the patient (as opposed to the provider) (Williams et al., 2016). Another recommendation proposed was to designate a specific staff member to be trained in trauma-informed care including IPV screening and response (Williams et al., 2016). This would be for the purpose of combatting significant time constraints facing providers. Overall, this study puts forth valuable
recommendations for ways to capitalize upon current strengths and suggestions for how to overcome barriers in screening for and responding to IPV in clinic and ED settings.
Similarly, Clark, Renner, and Logeais (2017) studied IPV screening, response, and referral practices of health care providers in an outpatient clinic setting. Their findings largely
corroborate the results reported by Williams et al. (2016), citing barriers such as lack of training, no established referral network, and inadequate knowledge of IPV and associated resources (Clark, Renner, & Logeais, 2017). The authors found that the current screening process included little variation and options for response between a negative and positive screen. Additionally, the typical provider response to a positive screening was to call the clinic’s social worker;
however, the social worker’s numerous responsibilities limited accessibility for response and follow up for patients (Clark et al., 2017). This emphasized the consequence of lacking an on- site, formal survivor advocate and process to connect patients to community-based services. The authors recommend a systems-level approach, with involvement and support from leadership, to incorporate routine screening, care coordination, and formalized referral (Clark et al., 2017).
They also address the need to work on care services for overlooked populations such as males, transgender individuals, racially and ethnically diverse groups, and older adult survivors (Clark et al., 2017). These are important inclusions as we work to standardize screening and narrow gaps in care for all victims of IPV.
There is consensus within past research that we need a new direction for health-service response to IPV in order to narrow the aforementioned gaps in care for survivors (Jewkes, 2013).
The recommended solution has called for a patient-centered comprehensive approach to care through coordinated community response. Dutton, James, Langhorne, & Kelly (2014) consider the patient-centered comprehensive approach to include universal education on IPV for all patients, utilization of written materials to guide the patient and provider conversation, discussing IPV as it relates to the visit, and referral to other victim services in an encouraging and supportive manner (Dutton et al., 2014). Research has shown that when a comprehensive approach is utilized, programs showed “sustained increased rates of screening, disclosure, and
case identification” along with effective screening protocols, thorough training of staff,
institutional support, and immediate access to referral services (Dutton et al., 2014, p. 82). This reflects strong coordinated community response, in which providers and systems apply a “whole person care” treatment perspective thus, reducing likelihood of future abuse and increase
personal wellness (Shorey, Tirone, & Stuart, 2014).
While the need for a coordinated community response has been well established in the research, there is very little evidence reflecting successful integration of coordinated services into practice (Shorey et al., 2014). Additionally, the theoretical guidance and structure for what coordinated response looks like is largely lacking. This may be the result of various challenges to integration of services such as confusion regarding best practice and policies on IPV,
insufficient efforts for change coming from leadership, and staff turnover, making sustaining partnerships difficult (Colombini, Mayhew, & Watts, 2008). Additionally, as victims seek health care services at a variety of locations and present with a range in severity of problems, coherent and efficient local partnerships are necessary to facilitate effective referrals to internal and/or external non-health services (Colombini et al., 2008). Since the majority of the research examines the response to IPV in acute care settings, more research in other care settings is needed in order to understand how to improve IPV response and strengthen partnerships.
Collectively, this research confirms that the role of the health care provider extends beyond identifying IPV to encompass treatment that recognizes not only the effect of IPV on the patient’s health but also the need to link patients with advocacy services and non-health related resources. When providers lack the training to respond to a disclosure in this way, the patient’s needs likely go unaddressed. This suggests the need for coordinated services and partnerships
between health care providers and IPV agencies to provide trauma-informed training, connect patients with resources, and develop a process for referrals (Dutton et al., 2014).
Futures Without Violence, a national health and social justice nonprofit working to end violence against women and children, has started an initiative aiming to implement just these types of partnerships with the hope it may instigate positive change and serve as a model for how to coordinate care services effectively. Project Catalyst is a statewide transformation of health, IPV, and human trafficking currently underway in Colorado, Guam, and North Carolina (Futures Without Violence, 2019). This project is working with the NCCADV and the North Carolina Community Health Center Association (NCCHCA) to create partnerships between IPV agencies and community health centers in North Carolina. Starting with five agencies and five health centers, the goal of Project Catalyst is to improve and integrate response to IPV and human trafficking by offering training, technical assistance, and creating partnerships to sustain trauma- informed care (Futures Without Violence, 2019). By the end of the project period, the goal is to have reached a minimum of 50% of North Carolina’s health centers (Futures Without Violence, 2019). In addition to this project, Futures Without Violence has an extensive online toolkit designed specifically for community health centers and IPV agencies looking to create and/or expand current partnerships. Project Catalyst is a promising new initiative, as research has clearly indicated a need for increased training and partnerships between community-based organizations and IPV service agencies.
In light of Project Catalyst taking place in North Carolina and due to the lack of research, the UNC School of Nursing partnered with the NCCADV to conduct a community forum to explore current infrastructure and partnerships between community health centers and IPV agencies in the North Carolina triangle region. This forum provided insight into how providers
at community health centers in North Carolina respond to IPV, the challenges of providing care, and current referral practices and available resources. Additionally, the forum provided a unique opportunity for stakeholders to discuss how to develop and maintain partnerships (along with the foreseen challenges) between community health centers and IPV agencies.
Community Forum Event
The UNC School of Nursing partnered with the NCCADV to host a community forum on March 20th, 2019 from 9am-3pm at the Durham Convention Center in Durham, North Carolina.
The purpose of the forum was to help inform state wide efforts to improve relationships between community health centers and IPV agencies. Stakeholders in the triangle region (also known as the North Region) of North Carolina, such as healthcare providers, IPV advocates and service providers, administrators/managers, care managers, social workers, researchers, students, and community members were invited to participate in the event. The triangle region consists of the following counties: Chatham, Durham, Edgecombe, Franklin, Granville, Harnett, Johnston, Lee, Moore, Nash, Orange, Person, Vance, Wake, and Warren. The forum objectives were to 1) describe current infrastructure/partnerships between community health centers and domestic violence programs in the NC triangle region; 2) identify opportunities and challenges for building and sustaining partnerships between community health centers and domestic violence programs in the NC triangle region; 3) explore strategies for maximizing opportunities and overcoming challenges to building and sustaining partnerships between community health centers and domestic violence programs in the NC triangle region; and 4) identify priority health care needs for survivors of IPV in the NC triangle region. This forum was piloted in the triangle region with the hope of replicating the event in other counties to improve partnerships and inform IPV practice state wide.
Pre-Forum Registration and Participants
A list of key stakeholders to invite to the forum was generated through a variety of methods. Community health centers within the triangle region were identified utilizing the Health Resources and Service Administration database (see Appendix A). IPV agencies were identified through the NCCADV’s online resource list of domestic violence service agencies by county (see Appendix B). Phone calls were then made to all organizations to identify
appropriate personnel to invite to the forum. Name, email address, and position within the organization were collected through these phone calls. Jessica Williams, PhD, MPH, PHNA- BC, from the UNC School of Nursing and the leading organizer of the forum, identified researchers and students from various institutions in the area. These collective efforts contributed to a master list of possible stakeholders in the triangle region.
An electronic “save the date” notice was emailed to potential participants seven weeks before the event (See Appendix C). Formal invitations were sent via email including a
registration link were participants were asked to complete a series of questions asking for more specific participant information and to gain perceptions concerning key challenges in addressing IPV (see Appendix D). If participants were affiliated with a community health center or IPV agency, they were prompted to answer questions on the forum related to current partnerships in their respective organizations. All attendees were asked to answer what they thought were the top three priority health needs for survivors of IPV and the top three priority survivor
populations in the triangle region. The answers to these two questions were used to inform forum activities and discussion. Forty-three participants registered for the event. A wide range of stakeholder groups were represented (See Figure 1) with the largest groups identifying as IPV advocate/service providers (25%) and health care providers (18%).
FIGURE 1: REGISTERED PARTCIPANTS Forum Agenda and Activities
To meet the objectives of this project, several activities were conducted including presentations, priority sorts, and a SWOT analysis. Refer to Appendix E to see the official forum program outlining the purpose and goals of the event, agenda breakdown, and speaker biographies.
Presentations. The forum began with words of welcome and forum briefing provided by Jessica Williams. Erika Ferguson, MPP, Director of the Office of Healthy Opportunities for the N.C. Department of Health and Human Services, introduced how addressing the unmet health- related resources needs of IPV survivors fits in to the Healthy Opportunities initiatives. For example, included in the initiatives is establishing a statewide coordinated care network (NCCARE360) to connect patients to community resources and assess the outcome of this referral. Melinda Manning, JD, MSW, Director of UNC Hospital’s Beacon Program, gave a more in-depth presentation on the context of addressing IPV in the healthcare setting, covering recent statistics and challenges of providing care services. Lastly, Cassandra Rowe, MPH, the Healthcare Program Coordinator for NCCADV, addressed NCCADV’s participation in Project Catalyst and why creating partnerships between community health centers and IPV agencies is relevant and essential in meeting the needs of IPV victims.
Group Priority Sort. Following these presentations, participants were assigned to one of three tables to create diverse groups to allow for sharing of unique perspectives and
experiences during breakout activities. Group facilitators (one per table) were given instructions and materials to guide two activities. Participants were first led through a group priority sort activity, a structured participatory method used to inform decision making regarding priority issues. This method encourages the sharing of experience, perspectives, and opinions of the various stakeholders to cultivate a better understanding of the various challenges facing victims of IPV. Groups sorted prepopulated card sets for survivor populations and healthcare needs in two parts: a rapid sort and a forced choice sort. The rapid sort was done quickly for the purpose of familiarizing the group with the cards and initial impressions. During the rapid sort,
participants were asked to sort the cards into five categories, with one being of lowest priority and five indicating highest priority (see Appendix F for images). The forced choice sort then allowed groups more time to discuss what issues and populations were of top priority compared to others. During this portion, participants were then asked to sort the cards so there were an equal number of cards in each group. They were then asked to sort the cards within the highest priority category (category 5) from most important to least important. To see a complete description of this activity, refer to Appendix G for facilitator instructions.
SWOT Analysis. The second breakout group activity participants were led through was a SWOT analysis, a tool utilized to identify strengths (S) and weaknesses (W) of current
partnerships, as well as external opportunities (O) and threats (T). Participants were asked to brainstorm 3-5 items for each category with the facilitator tracking ideas on a provided flip chart (see Appendix F for images). These lists were then used to develop strategies for establishing and maintaining partnerships between community health centers and IPV agencies. To see a
complete description of the SWOT activity, refer to Appendix G to see facilitator instructions.
Following completion of both activities, groups came together to debrief and discuss identified priorities, challenges, and recommended strategies.
Forum Results
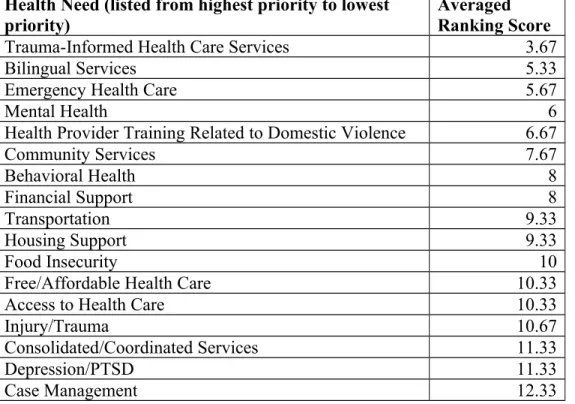
To identify the most salient priority health needs and populations across groups, each card was given a number (1-29 for survivor populations and 1-35 for health needs) based on where each group ranked the card. The three rankings were averaged between each group to determine a final ranking score. Group two combined related cards, thus for scoring, the cards grouped together were assigned the same number. Upon comparing top priorities across the three groups, the highest priority health care needs included 1) trauma-informed health care services, 2) bilingual services, 3) emergency health care, and 4) mental health. Table 3 presents top health care needs of survivors across all groups.
TABLE 3: HEALTH NEEDS RANKED ACROSS GROUPS Health Need (listed from highest priority to lowest
priority)
Averaged Ranking Score
Trauma-Informed Health Care Services 3.67
Bilingual Services 5.33
Emergency Health Care 5.67
Mental Health 6
Health Provider Training Related to Domestic Violence 6.67
Community Services 7.67
Behavioral Health 8
Financial Support 8
Transportation 9.33
Housing Support 9.33
Food Insecurity 10
Free/Affordable Health Care 10.33
Access to Health Care 10.33
Injury/Trauma 10.67
Consolidated/Coordinated Services 11.33
Depression/PTSD 11.33
Case Management 12.33
Reproductive Health Care 14.33
Social Support 16.67
Health Insurance Support 17
Mental Health for Children 17
Substance Use 17
Stress/Coping Support 17.33
HIV/AIDS & Sexually Transmitted Infections 17.67
Chronic Health Conditions 17.67
Physical Health 18
Health Care Navigation 18.67
Prenatal/Pregnancy Care & Support 19.67
Opioid Use 20
Preventative Health Care 20
Chronic Pain 23
Pain Management 23.33
Continuous/Long-Term Health Care 23.67
Patient Support for Non-Compliance 25
Trauma-Informed Yoga 29.67
Table 4 presents priority survivor populations across all three groups. The highest priority populations were 1) victims/survivors of human trafficking and sexual violence, 2) children exposed to IPV, 3) LBGTQ+ individuals, and 4) individuals with disabilities.
TABLE 4: SURVIVOR POPULATIONS RANKED ACROSS GROUPS Survivor Population (listed from highest
priority to lowest priority) Averaged Ranking Score
Victims/Survivors of Human Trafficking 3
LGBTQ+ Individuals 4
Individuals with Disabilities 4.67
Children Exposed to Intimate Partner Violence 6
Victims/Survivors of Sexual Violence 6.33
Immigrant Groups 7
Victims/Survivors of Child Abuse 7.33
Racial/Ethnic Minority Populations 8
Non-English Speaking Individuals 8.33
Undocumented Populations 10
Homeless Individuals 11.67
Refugee Populations 13.67
Individuals Involved with the Justice System 13.67
African American/Black Individuals 14
Adolescents 14.33
Elderly/Older Adults 15
Single Mothers 15.33
Low Income Individuals 15.67
Men 16.67
Women 17.67
Individuals Struggling with Substance Abuse 18.33
Uninsured Individuals 20.33
College/University Students 21.67
individuals Living with HIV/AIDS 22
Un/Underemployed Individuals 22.33
Individuals with Chronic Health Conditions 22.67
Asian Individuals 22.67
Middle Class Individuals 27.33
Hispanic/Latinx Individuals 41
Table 5 outlines the various strengths, weaknesses, opportunities, threats and strategies brainstormed during the SWOT analysis activity. Strategies focused primarily on the efficient use of resources and addressing the needs of vulnerable populations.
TABLE 5: IDENTIFIED STRENGTHS, WEAKNESS, OPPORTUNITIES, AND THREATS BY GROUPS
Group 1 Group 2 Group 3
Strengths - Much information &
very accessible
- Internet for clients to identify services - Increased public awareness for DV
- Knowledge/experience makes it easier to work and collaborate
- Well known DV service agencies in the area
- DV service agencies are comfortable to reach out to, dependable, and have good outcomes - Integrated behavioral health staff at DV service agencies - CHCs have a whole- person idea of care - DV is a priority at CHCs
- Proximity of a family justice center in the area
- Increased awareness of DV and recognition of health care issues - Increased Medicaid focus on SDH
- Team-based care - Initiatives for high utilization patients - Development of handouts/materials/
posters with information and resources about DV (starting to get these into CHCs)
- CHCs have better awareness of DV than other health care services
Weaknesses - Lack of partnerships - Weak relationships - Poor standardization
between DV agencies and CHCs
- Staff Turnover
- Lack of access to DV services
- Confidentiality issues within services (e.g., disclosure)
- Follow-up/Referral issues
- Mistrust in the community
- Funding (stable sources, private & public)
- Lack of resources (including for families) - No shelters for older boys or men (single fathers)
- Lack of connection to public safety
with some agencies (e.g., OC rape crisis center)
- Understaffing - Lack of consistent screening (tied to understaffing and turnover)
- Funding - Resources
- Staff turnover – difficult to maintain relationships
- Safety concerns - Privacy of patient information
- Screening for health care needs at shelters - Translating
information into implementation
- Lack of time providers have with patients and to get training
Opportunities - Build trust/relationships in the community
- Education (for everyone) - Community dialogues - MOUs between organizations
- Advocacy (services for legislators/policy makers) - Better coordinating funds to avoid duplication of services
- Evaluations for improvement in health after using resources - Emergency shelter - Regional agency cooperation
- All staff to go through trauma-informed care training
- Specialized trauma training related to opioid crisis
- Medicaid and Healthy Opportunities (paying for DV services) - Telehealth - Co-locating DV advocates or training health care staff in advocacy
Threats - Political climate - Security/public safety - Cultural morays - Religion
- Transportation (can get to one but not other services)
- Gender norms - Bureaucracy
- High turnover (information gets lost) - Isolation/not reaching out to other
organizations - Distribution of information/resources
- N360 database:
safety/security of data - Medicaid billing - Patients (especially in rural areas) may not disclose or be willing to seek services in
community setting where they may be known
- Lack of Medicaid
expansion - Disparities in geographic areas - NC not addressing needs of LBGTQI and undocumented
populations Strategies - Need to emphasize
partnerships & cross- training
- Prevent burnout with more resources
- Greater education to the community
- Conversations between organizations (boards, head nurse, influencers) - Ask for funds together with continued meeting to avoid duplication (with strategy meetings to plan) - Education (community and organizations; don’t separate)
- Cultural
sensitivity/responsiveness/
humility - Advocacy
N/A - State-wide roll out of
trauma-informed care training
- Advocate for
increased privacy and security, VAWA compliant
- Training and education around culturally-competent care for providers - Increased funding for translation services and compliance with laws and policies
Figure 2 represents the summary of strategies for improving services provide to survivors and partnerships between community health centers and IPV agencies.
FIGURE 2: STRATEGIES FOR IMPROVING SERVICES AND AGENCY PARTNERSHIPS
Discussion
Results from this forum provided important insights into current partnerships and challenges of providing care to IPV survivors. Several priority health care needs and survivor populations were identified and may now serve as guidelines for shaping future research and practice. Recommendations for how to strengthen and maintain partnerships were also discussed, providing direction for implementation of practical changes in IPV response and referral for underserved populations.
Results from the group priority sort indicate that current efforts of providers and IPV agencies in the triangle region should prioritize providing trauma-informed health care training and services, bilingual services, emergency care, mental health services, and community
services. Additional priorities include improving social determinants of health such as adequate housing, transport, financial support, food insecurity, and access to care. These particular factors
require system-level change and support reflected in policies and initiatives to improve conditions and resources for vulnerable community members.
Results also suggested that top priority survivor populations included victims and
survivors of human trafficking, sexual violence, and child abuse. Additional priority populations include LGBTQ+ individuals, individuals with disabilities, immigrant groups, racial and ethnic minorities, non-English speaking individuals, and undocumented community members. This wide range of priority populations reflects a difference in the decision-making process between breakout groups. During the debrief discussion, some groups indicated that they considered how vulnerable populations were when considering priority populations, whereas other groups considered resource availability.
Collaborative discussion between groups allowed for sharing of brainstorming and ideas generated during the SWOT analysis. Strengths revealed that awareness around the knowledge and importance of IPV has seemingly increased in recent years. Additionally, community health centers and IPV agencies appear to have a strong holistic, team-based approach to care.
Weaknesses indicated several concerns regarding understaffing and staff turnover. These are significant barriers when considering building sustainable partnerships as staffing issues make it difficult to maintain organizational collaborations and retain institutional knowledge. Other weaknesses revealed throughout discussion were challenges related to lack of funding such as inadequate resources and inconsistencies in practice. Discussion revealed that groups felt there were several opportunities to strength partnerships, mainly focused on capitalizing available resources such as the Healthy Opportunity initiative and Futures Without Violence toolkits.
Future efforts may also incorporate co-locating DV advocates and health care providers in organizations, utilizing telehealth resources, and incorporating health outcomes in current
evaluations of DV service utilization. Threats to consider while moving forward include issues around maintaining privacy, billing of services, and organizational climates unsuited for
sustaining partnerships. Additional issues to keep in mind are societal threats involving political climate, safety, gender norms, cultural and religious differences, and health disparities.
Participants notes that these have direct impact on resource allocation and the services that they are able to provide, with resources specifically lacking for LBGTQI individuals, undocumented community members, and disabled populations. This information is important to reflect upon as we consider strategies for improving care, strengthening partnerships, and as guidance for future research.
Group consensus regarding the need for improved IPV training for healthcare providers led to resounding support for state-wide roll out of trauma-informed care training. Upon delving into this topic further, participants explained that this encompasses increased awareness of culturally-competent care, cross-organizational training, and an established referral and follow- up process. Other important focuses to consider for future practice include advocating for adhering to the Violence Against Women Act to maintain privacy and security and efforts to increase funding for inadequate resources such as bilingual services. It is also of importance that organizations collaborate in order to avoid duplication of care services and promote continuity of care. Collectively, these recommended strategies may help improve services provided to
survivors and cultivate partnerships between community health centers and IPV agencies.
One of the significant limitations of this forum is that some registered participants did not attend the event and some had to leave early, resulting in decreased representation in certain stakeholder groups and fewer diverse perspectives to contribute to group discussion. Another limitation of the study was lack of time for breakout group activities, causing some groups to
rush or not fully complete instructions. During the group priority sort, group two combined related cards, causing slight discrepancies in analysis and scoring of top priorities. However, should this event be replicated in the future, these limitations may be anticipated and prevented.
Despite these limitations, the forum successfully met its goals of bringing together stakeholders to understand current infrastructure, identify opportunities and challenges of maintaining partnerships, brainstorming strategies for capitalizing on opportunities and overcoming barriers, and identifying priority health needs and survivor populations within the triangle region. The forum cultivated coordination and communication between those working to decrease the incidence of IPV and improve service by identifying gaps in care and developing recommendations for next steps. Findings from the forum suggest that moving forward,
community health centers should focus immediate efforts on training providers in trauma informed care, improve knowledge of available resources, and establish a referral network. IPV agencies can aid in this process by collaborating with community health centers to educate providers and serve as additional resources for information and connection with appropriate services. Both organizations should also anticipate challenges in the near future such as maintain privacy during coordinated care and changes in Medicaid. With the successful completion of this pilot forum, it is the hope that this event can be replicated in the other regions of North Carolina in order to improve services statewide. To promote this goal, lists of community health centers and IPV agencies by county and region are included in the Appendix G.
Conclusions
The importance of the role of the healthcare provider in screening for and responding to IPV has garnered increased recognition in recent years. Despite current USPSTF
recommendations and providers recognizing screening and response as part of their role,
significant barriers still exist to meeting victim’s needs and connecting them with appropriate resources. Multi-level approaches and coordinated care services are proposed solutions for addressing these barriers, however, implementation of such initiatives and evaluation of their effectiveness is limited. It is critical to increase awareness of existing resources for service providers, such as various Futures Without Violence toolkits covering IPV screening and
counseling and guidelines for building partnerships between IPV agencies and community health centers to improve the ability of patients to access resources. Additionally, more research is needed in order to understand how to integrate IPV care and response and to identify the factors that may be enhancing or impeding effective coordination of services.
With NCCADV and the NCCHCA collaborating on the Project Catalyst initiative, these organizations are best positioned to lead the charge in improving partnerships between IPV agencies and community health centers. It is of great hope that this report will aid in this work by providing insights into current partnerships and identifying priority needs of survivors in North Carolina. As this forum has proven effective in bringing together key stakeholders in IPV to offer unique perspectives, discuss challenges, and propose solutions for maintaining
partnerships, it is a goal that the event will be replicated in other counties in the future to guide and support new initiatives.
Acknowledgements
A special thank you to Jessica Williams for spearheading this community forum. Her guidance, support, and expertise have been paramount in the completion of this report. I would also like to acknowledge and thank Cassie Rowe (NCCADV) and Andrea Cummings (UNC SON) for assistance in planning and hosting this event. Additional thanks to the collaborative partners of this event, the UNC School of Nursing and the NCCADV, event speakers, and forum
participants. The funding for this forum was granted to Jessica Williams by the UNC Carolina Center for Public Service, Thorp Faculty Engaged Scholars Program.
References
Alvarez, C., Debnam, K., Alexander, K., & Glass, N. E. (2018). Responding to intimate partner violence: Healthcare providers’ current practices and views on integrating a safety decision aid into primary care settings. Research in Nursing & Health, 41(2), 145 – 155.
Doi: 10.1002/nur.21853
Black, M. C. (2011). Intimate partner violence and adverse health consequences: Implication for clinicians. American Journal of Lifestyle Medicine, 5(5), 428-439. Doi.org/10.1177/155 9827611410265
Breiding, M. J., Basile, K. C., Smith, S. G., Black, M. C., & Mahendra, R. R. (2015). Intimate partner violence surveillance: Uniform definitions and recommended data elements.
Atlanta (GA): National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Breiding, M. J., Smith, S. G., Basile, K. C., Walters, M. L., Chen, J., & Merrick, M. T. (2011).
Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization: National intimate partner and sexual violence survey, United States.
Atlanta (GA): National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Centers for Disease Control and Prevention. (2015). Injury prevention and control: Intimate partner violence: Consequences. Retrieved from: https://www.cdc.gov/ViolencePreventio n/intimatepartnerviolence/consequences.html
Clark, C. J., Renner, L. M., & Logeais, M. E. (2017). Intimate partner violence screening and referral practices in an outpatient care setting. Journal of Interpersonal Violence.
Advanced online publication. 1-12. Doi: 10.1177.0886260517724253
Colombini, M., Mayhew, S., & Watts, C. (2008). Health-sector responses to intimate partner violence in low-and middle-income settings: A review of current models, challenges and opportunities. Bulletin of the World Health Organization, 86(8), 635-642. Doi:10.2471/B LT.07.045906
Curry, S. J. (2018). Screening for intimate partner violence, elder abuse, and abuse of vulnerable adults. JAMA, 320(16), 1678-1687. doi:10.1001/jama.2018.14741
Dutton, M. A., James, L., Langhorne, A., & Kelly, M. (2014). Coordinated public health initiatives to address violence against women and adolescents. Journal of Women’s Health, 24(1), 80-85. Doi:10.1089/jwh.2014.4884
Futures Without Violence. (2019). Project catalyst: State and territory-wide transformation on health, IPV, and human trafficking. Retrieved from https://www.futureswithoutviolence .org/health/project-catalyst/
Gerberding, J. L., Popovix, T., Stephens, J. W., Solomon, S. L., Bernhardt, J. M., & Daniel, K.
L. (2008). Morbidity and mortality weekly report: Adverse health conditions and health risk behaviors associated with intimate partner violence. Atlanta (GA): Coordinating Center for Health Information and Service, Centers for Disease Control and Prevention, and U.S. Department of Health and Human Services.
Jacobson, A., McQuire, M., Zorzi, R., Lowe, M., Oandasan, I., & Parker, K. (2011). The group priority sort: A participatory decision-making tool for healthcare leaders. Healthcare Quarterly, 14(4), 47-53. Doi:10.12927/hcq.2013.22651
Jewkes, R. (2013). Intimate partner violence: The end of routine screening. The Lanet, 382(9888), 190-191. Doi:10.1016/S0140-6736(13)60584-X
Lindo, J. M., Siminski, P. M., & Swensen, I. D. (2015). College part culture and sexual assault.
American Economic Journal: Applied Economics, 10(1), 236-265. Doi:10.3386/w21828 Lomborg, B. & Williams, M. A. (2018, February 22). The cost of domestic violence is
astonishing. The Washington Post. Retrieve from https://www.washingtonpost.com/
opinions/the-cost-of-domestic-violence-is-astonishing/2018/02/22/f8c9a88a-0cf5-11e8- 8b0d-891602206fb7_story.html?utm_term=.78e89a8d9c12
Miller, E. & McCaw, B. (2019). Intimate partner violence. The New England Journal of Medicine, 380(9), 850-857. Doi:10.1056/nejmra1807166
National Census of Domestic Violence Services. (2016). 11th annual domestic violence count:
North Carolina summary. Retrieved from https://nccadv.org/images/pdfs/2016_NC)_Cen sus.pdf
North Carolina Department of Health and Human Services. (2015) North Carolina violent death reporting system: 2015 annual report. Retrieved from https://www.injuryfreenc.ncdhhs.d ata/Surveillance/VDRS/NCVDRS-AnnualReport-FINAL-15Feb2018.pdf
Rothman, E. F., Hathaway, J., Stidsen, A., & de Vries, H. F. (2007). How employment helps female victims of intimate partner violence: A qualitative study. Journal of Occupational Health Psychology, 12(2), 136-143.
Salber, R. P., & Taliaferro, E. (2006). The physician’s guide to intimate partner violence and abuse: A reference for all health care professionals. Volcano, California: Volcano Press.
Shorey, R. C., Tirone, V. & Stuart, G. L. (2014). Coordinated community response components for victims of intimate partner violence: A review of the literature. Aggression and Violent Behavior, 19(4), 363-371. Doi:10.1016/j.avb.2014.06.001
Smith, S. G., Xhang, Z., Basile, K. C., Merrick, M. T, Wang, J., Krensnow, M., & Chen, J.
(2015). The national intimate partner and sexual violence survey: 2015 data brief – updated release. Atlanta (GA): National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Sprague, S., Madden, K., Simunovic, N., Godin, K., Pham, N. K., Bhandari, M., & Goslings, J.
C. (2012). Barriers to screening for intimate partner violence. Women and Health, 52, 587–605.
Swailes, A. L., Lehman, E. B., & McCall-Hosenfeld, J. S. (2017). Intimate partner violence discussions in the healthcare setting: A cross-sectional study. Preventive Medicine Report, 8, 215-220. Doi:10.1016/j.medr.2017.10.017
Turner, H. A., Finkelhor, D., & Ormrod, R. (2010). The facts on children’s exposure to intimate partner violence. Futures Without Violence.
United Health Foundation. (2018). America’s health rankings: Health of women and children – intimate partner violence in North Carolina. Retrieved from: https://www.americashealth rankings.org/explore/health-of-women-and-children/measure/ipv-lifetime/state/NC U.S. Preventative Services Task Force. (2013). Intimate partner violence and abuse of elderly
and vulnerable adults: Screening. Retrieved from https://www.uspreventiveservicestaskfo rc.org/Page/Document/UpdateSummaryFinal/intimate-partner-violence-and-abuse-of- elderly-and-vulnerable-adults-screening
Williams, J. R., Halstead, V., Salani, D., & Koermer, N. (2016). An exploration of screening protocols for intimate partner violence in healthcare facilities: A qualitative study.
Journal of Clinical Nursing, 26, 2192 – 2201. Doi:10.1111/jocn.13353
Appendix A
Community Health Centers within the Triangle Region Community Health
Center Operated By Street Address Country
Angier Medical Center First Choice Community
Health Centers 84 Medical Dr, Angier, NC
27501 Harnett
First Choice Community Health Centers at Lillington
First Choice Community Health Centers
40 Autumn Fern Trl, Lillington, NC 27546
Harnett
Durham Recovery
Response Center Lincoln Community
Health Center, Inc. 309 Crutchfield St, Durham,
NC 27704 Durham
Healthcare for the Homeless
Lincoln Community Health Center, Inc.
412 Liberty St, Durham, NC 27701
Durham Holton Clinic Lincoln Community
Health Center, Inc.
401 N Driver St, Durham, NC 27703
Durham John H. Lucas Sr
Wellness Center
Lincoln Community Health Center, Inc.
3727 Fayetteville St, Durham, NC 27707
Durham Lincoln CHC -Durham
County Human Services
Lincoln Community Health Center, Inc.
414 E Main St, Durham, NC 27701
Durham Lincoln Community
Health Center, Inc. Lincoln Community
Health Center, Inc. 1301 Fayetteville St,
Durham, NC 27707 Durham
Live Well Primary Care Clinic
Lincoln Community Health Center, Inc.
3901 N Roxboro St Ste 101, Durham, NC 27704
Durham Lyon Park Clinic Lincoln Community
Health Center, Inc.
1313 Halley St, Durham, NC 27707
Durham Walltown Clinic Lincoln Community
Health Center, Inc.
815 Broad St, Durham, NC 27705
Durham OIC Family Medical
Center
Opportunities
Industrialization Center, Incorporated
111 S Fairview Rd, Rocky Mount, NC 27801
Nash
OIC Family Medical Center at Community Health Plaza
Opportunities
Industrialization Center, Incorporated
1041 Noell Ln, Rocky Mount, NC 27804
Nash
Carrboro Community Center
Piedmont Health Services, Inc.
301 Lloyd St, Carrboro, NC 27510
Orange Chapel Hill
Community Health Center
Piedmont Health Services, Inc.
1828 Martin Luther King Jr Blvd, Chapel Hill, NC 27514
Orange IFC Community
Health Center
Piedmont Health Services, Inc.
1315 Martin Luther King Jr Blvd, Chapel Hill, NC 27514
Orange Moncure Community
Health Center Piedmont Health
Services, Inc. 7228 Moncure Pittsboro Rd,
Moncure, NC 27559 Chatham
Piedmont Health
SeniorCare Pittsboro Piedmont Health
Services, Inc. 163 Chatham Business Dr,
Pittsboro, NC 27312 Chatham Siler City Community
Health Center
Piedmont Health Services, Inc.
224 S 10th Ave, Siler City, NC 27344
Chatham Person Family
Medical Center, Inc.
Person Family Medical Center
702 N Main St, Roxboro, NC 27573
Person Rural Health Group at
Henderson
Rural Health Group, Inc. 100 W Parkview Dr, Henderson, NC 27536
Vance Rural Health Group at
Norlina
Rural Health Group, Inc. 110 Division St, Norlina, NC 27563
Warren Rural Health Group at
Stovall Rural Health Group, Inc. 100 Durham St, Oxford, NC,
27565 Granville
Rural Health Group at Whitakers
Rural Health Group, Inc. 105 NW Railroad St, Whitakers, NC 27891
Edgecombe Advance Community
Health - APEX
Wake Health Services, Inc.
212 S Salem St, Apex, NC 27502
Wake Advance Community
Health, Southeast- Raleigh- South
Wake Health Services, Inc.
1011 Rock Quarry Rd, Raleigh, NC 27610
Wake
Cary at Dorcas Plaza Wake Health Services, Inc.
173 High House Rd, Cary, NC 27511
Wake Horizon at South
Wilmington
Wake Health Services, Inc.
1420 S Wilmington St, Raleigh, NC 27603
Wake Horizon at Women's
Center
Wake Health Services, Inc.
112 Cox Ave, Raleigh, NC 27605
Wake Southern Regional
Center Fuquay Varina Wake Health Services,
Inc. 130 N Judd Pkwy NE,
Fuquay Varina, NC 27526 Wake
Appendix B
IPV Agencies within the Triangle Region
IPV Agency Street Address County
Chatham Family Violence Prevention Services
45 W Salisbury Street, Pittsboro, NC 27312 Chatham Coalition for Family Peace PO Box 961, Siler City, NC 27344 Chatham Compass Center for Women and
Families PO Box 1057, Chapel Hill, NC 27514 Orange
Durham Crisis Response Center 206 N Dillard Street, Durham, NC 27701 Durham Families Living Violence Free PO Box 1632, Oxford, NC 27565 Granville Family Violence & Rape Crisis
Services
PO Box 1105, Pittsboro, NC 27312 Chatham Friend to Friend 101A Monroe Street, Carthage, NC 28327 Moore
Harbor, Inc PO Box 1903, Smithfield, NC 27577 Johnston
HAVEN 215 Bracken Street, Sanford, NC 27331 Lee
Infinite Possibilities, Inc. 132 Rafters Ln, Warrenton, NC 27589 Warren
Interact 1012 Oberlin Road, Raleigh, NC 27605 Wake
My Sister's House PO Box 7665, Rocky Mount, NC 27804 Edgecombe North Carolina Coalition Against
Sexual Assault 811 Spring Forest Road, Suite 900, Raleigh,
NC 27609 Wake
Safe Haven Person County PO Box 474, Roxboro, NC 27573 Person SAFE of Harnett County PO Box 728, Lillington, NC 27546 Harnett
Safe Space PO Box 240, Louisburg, NC 27549 Franklin
UNC Hospital's Beacon Program 101 Manning Drive, CB #7600, Chapel Hill, NC 27514
Orange
Appendix C
Community Forum Save the Date
Appendix D
Community Forum Event Registration Form Registration Form Fields:
Name:
Email:
Organization/Affiliation:
Primary Role:
O Healthcare Provider
O Domestic Violence Advocate/Service Provider O Researcher
O Administrator/Manager O Community Member O Student
O Other (please specify): _________________
Are you representing a:
O Community Health Center
O Domestic Violence Service Agency O Other
For Community Health Centers
Does your Community Health Center have a relationship with a domestic violence program(s)?
O Yes O No
O I do not know
If yes, please name the domestic violence program(s) your Community Health Center works with:
___________________________________________________________
If yes, on a scale from 1-10, how strong are your relationships with domestic violence programs?
1 2 3 4 5 6 7 8 9 10
For Domestic Violence Programs
Does your organization have a relationship with a community health center(s)?
O Yes O No
O I do not know
If yes, please name the community health center(s) your organization works with:
______________________________________________________________
If yes, on a scale from 1-10, how strong are your relationships with community health centers?
1 2 3 4 5 6 7 8 9 10 For All Attendees
What do you see as the top 3 priority health needs for survivors of domestic violence in the NC triangle region (these may be diseases/health conditions, health care services, or other related needs)?
1. ___________________________________________
2. ___________________________________________
3. ___________________________________________
Who do you see as the top 3 priority survivor populations in the NC triangle region (these may be demographic groups, groups with certain social conditions, groups with particular
experiences, etc.)?
1. ___________________________________________
2. ___________________________________________
3. ___________________________________________
We will be creating a participant contact list to share at the community forum. Would it be okay to provide your name, organization/affiliation, and email on this list?
O Yes O No
Appendix E
Community Forum Program
Appendix F Breakout Group Images Group Priority Sort
SWOT Analysis
Appendix G
Breakout Groups Instructions for Facilitators Introductions (11:00am – 11:10am):
Ask each person sitting around the table to introduce themselves, providing:
1) Name
2) Organization/Place of work 3) Professional Background
4) Interesting fact about themselves/Anything else they would like to share Breakout Activity #1 (11:10am – 11:50am):
Materials:
- Index cards with pre-populated health needs - Blank index cards
- Numbered pages (1 – 5) Instructions:
1) Set numbered pages in a row on the table.
2) Explain the purpose of the activity to participants.
a. In this activity, we will be discussing health needs of domestic violence survivors.
During registration, everyone identified what the felt were the top 3 health needs of survivors. Everyone’s answers are listed on this set of index cards. We will be working as a group to sort these cards from highest to lowest priority.
3) Rapid Sort
a. Explain the purpose:
i. We are now going to do a rapid sort of the cards. This an opportunity to get more familiar with the health needs listed and provide a starting point for further prioritization. I am going to read each card to you. After I read the card, shout out your “gut” reaction about where the card should be placed based on importance (Number 1-5). I will place that card on the number based on the group majority. We will have an opportunity to discuss and change the order later, so don’t think too much about it at this point.
b. Read each index card aloud to the group. Place the card on the number called out by a majority of participants.
c. Once all of the cards have been sorted, ask participants if they think anything is missing from the list. If so, write down on the blank index cards and ask them to vote on where it should be placed in the piles.
4) Forced Choice Set
a. Explain the purpose:
i. Now we are going to work together to move the index cards so there is an equal number of cards in each category. This will provide an opportunity
for everyone to share their point of view about different health needs and why they feel a card should be in a certain priority category. Final placement of the cards will be based on group consensus. If there is disagreement, you should explain your perspectives and rationale to the group until an agreement is reached.
b. Work together to move the index cards so that there is an equal number in each category.
c. Once the cards have been equally distributed between categories, take the cards in the highest priority group and sort those from lowest to highest priority.
d. Take the cards in the lowest priority group and sort those from lowest to highest priority.
e. If time allots, sort the other priority groups, but this is optional.
5) Keep the cards in order. Someone will come by to collect them.
Notes:
What decisions made by the group were easy decisions?
Note which cards promoted a lot of discourse and discussion.
Lunch (11:50am – 12:10pm):
Participants will break during this time to get their lunch. When participants have returned to the table, begin Breakout Activity #2.
Breakout Activity #2 (12:10pm – 12:45pm):
Group Priority Sort: Priority Populations of Domestic Violence Survivors Materials:
- Index cards with pre-populated health needs - Blank index cards
- Numbered pages (1 – 5) Instructions:
1) Set numbered pages in a row on the table.
2) Explain the purpose of the activity to participants.
a. In this activity we will be doing another priority sort, focused on identifying priority populations of domestic violence survivors. This is also based on information provided by participants during registration. We will follow the same format that we used for the sort of health needs.
3) Rapid Sort
a. Read each index card aloud to the group. Place the card on the number called out by a majority of participants.
b. Once all of the cards have been sorted, ask participants if they think anything is