Michał Szpinda, Anna Szpinda, Małgorzata Dombek, Marcin Wiśniewski,
Marcin Daroszewski
External Diameters of the Abdominal Aorta
and Iliac Arteries in Human Fetuses
Średnice zewnętrzne aorty brzusznej i tętnic biodrowych
u płodów człowieka
Department of Normal Anatomy, the Ludwik Rydygier Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń, Poland
Abstract
Background. Advances in perinatal medicine have required an exhaustive knowledge of fetal aorto-iliac diameters in the prenatal diagnosis of congenital aorto-iliac abnormalities.
Objectives. This study defines the growth of absolute and relative external diameters of the abdominal aorta and iliac arteries in human fetuses.
Material and Methods. Using anatomical dissection and digital-image analysis, the external diameters of the abdominal aorta, and common, external and internal iliac arteries in 124 spontaneously aborted human fetuses aged 15–34 weeks were examined.
Results. No significant sex differences were found (P > 0.05). The strongest developmental dynamics referred to the abdominal aorta diameters, from 1.18 ± 0.25 to 5.19 ± 0.49 mm for its origin, and from 1.03 ± 0.23 to 4.92 ± 0.46 mm for its bifurcation. The intermediate values were found in both the common and internal iliac arteries: from 0.66 ± 0.19 to 2.30 ± 0.42 mm on the right, and from 0.66 ± 0.14 to 2.16 ± 0.42 mm on the left for the former, and from 0.52 ± 0.15 to 1.77 ± 0.44 mm on the right, and from 0.50 ± 0.14 to 1.65 ± 0.42 mm on the left for the latter. The smallest values were related to the external iliac arteries, which increased from 0.35 ± 0.09 to 1.28 ± 0.26 mm and from 0.31 ± 0.05 to 1.21 ± 0.22 mm on the right and left sides, respectively. The external diameter at the bifurcation of the abdominal aorta was relatively increasing throughout the study period. External diameters of the three iliac arteries were found to decrease in their relative values in the age range of 4–5 months, to start increasing gradually afterwards.
Conclusions. The absolute values of the external diameters of the aorto-iliac segment increase linearly throughout
gestation, whereas the relative values of the three iliac arteries decrease during the 4th–5th month period of gestation,
to start increasing afterwards (Adv Clin Exp Med 2011, 20, 6, 691–698).
Key words: abdominal aorta, common iliac artery, external iliac artery, internal iliac artery, external diameters, digital image analysis, human fetuses.
Streszczenie
Wprowadzenie. Postęp w medycynie perinatalnej wymaga wyczerpującej wiedzy o średnicach aorty i tętnic bio-drowych u płodu w diagnostyce prenatalnej wad wrodzonych tych naczyń.
Cel pracy. Praca ta definiuje wzrost bezwzględnych i względnych średnic zewnętrznych aorty brzusznej i tętnic biodrowych u płodów człowieka.
Materiał i metody. Za pomocą dysekcji anatomicznej i cyfrowej analizy obrazu zbadano średnice zewnętrzne aorty brzusznej i tętnic biodrowych wspólnych, zewnętrznych i wewnętrznych u 124 płodów człowieka w wieku 15–34 ty- godni, które pochodziły z poronień samoistnych i porodów przedwczesnych.
Wyniki. Nie stwierdzono różnic płciowych (P > 0.05). Najsilniejszą dynamikę rozwojową wykazywały średnice aorty brzusznej w zakresie 1,18 ± 0,25–5,19 ± 0,49 mm dla jej początku i 1,03 ± 0,23–4,92 ± 0.46 mm dla jej rozdwojenia. Pośrednie wartości stwierdzono dla tętnic biodrowych wspólnych i wewnętrznych, odpowiednio od 0,66 ± 0,19 do 2,30 ± 0,42 mm po stronie prawej i od 0,66 ± 0,14 do 2,16 ± 0,42 mm po stronie lewej dla pierwszej oraz od 0,52 ± 0,15 do 1,77 ± 0,44 mm po stronie prawej i od 0,50 ± 0,14 do 1,65 ± 0,42 mm po stronie lewej dla drugiej. Najmniejsze wartości średnic zewnętrznych odnosiły się do tętnic biodrowych zewnętrznych, które
wzra-Adv Clin Exp Med 2011, 20, 6, 691–698 ISSN 1230-025X
oRIgINAL PAPERS
in perinatal medicine have required an exhaus-tive knowledge of fetal aorto-iliac diameters in the prenatal diagnosis and monitoring of congenital aorto-iliac abnormalities.
To the best of authors knowledge, no study has investigated a comparative evolution of both absolute and relative diameters of the abdomi-nal aorta and iliac arteries. Therefore, to improve knowledge of the quantitative morphology of the abdominal aorta and common, external and inter-nal iliac arteries, the authors aimed to investigate the following: age-specific reference intervals for their external diameters, their absolute growth in external diameter, their relative growth in external diameter, the influence of sex on the value of the parameters studied.
Material and Methods
The examinations were performed on 124 hu- man fetuses of Caucasian origin of both sexes (60 males, 64 females) derived from spontane-ous abortions or stillbirths. The fetal age varied between 15 and 34 weeks. Legal and ethical con-siderations had been approved by the University Research Ethics Committee (KB/217/2006). The fetuses were free of malformation affecting car-diovascular anomalies. gestational age was de-termined from measurements of the crown-rump (CR) length on the basis of Iffy tables [15]. For statistical analysis, the fetuses were divided into six monthly groups, related to the 4th–9th month
of gestation. The arterial bed was filled with white latex LBS 3060 through a catheter Stericath (di-ameter of 0.5–1 mm), introduced by lumbar ac-cess into the abdominal aorta. The arterial bed filling was performed under controlled pressure of 50–60 mm Hg, using a syringe infusion pump SEP 11S (Ascor SA, Medical Equipment, Warsaw 2001). All specimens were immersed in 10% neu-tral formalin solution for 4–24 months for pres-ervation, and then dissected under a stereoscope
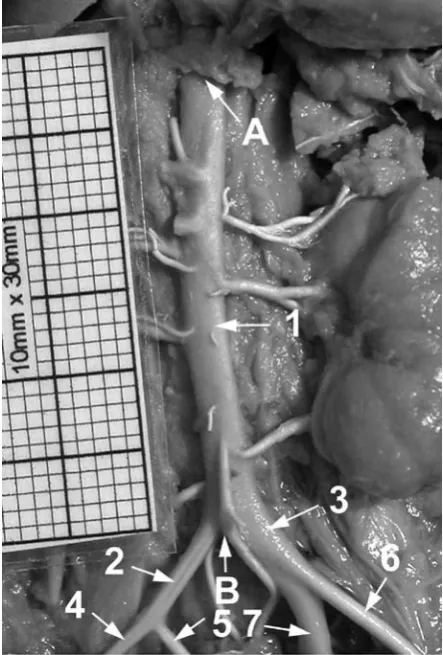
to the optical lens axis, afterwards recorded using a Nikon Coolpix 8400 camera, digitalized to TIFF images (Fig. 1) and assessed using digital image analysis (Leica QWin Pro 16, Cambridge), which semi-automatically estimated the external diam-eters of the marked abdominal aorta and three iliac arteries.
For each specimen the following eight external diameters were evaluated: proximal external diam-eter of the abdominal aorta, measured just below the aortic hiatus of the diaphragm; distal external diameter of the abdominal aorta, measured just above its bifurcation; proximal external diameters of the right and left common iliac arteries, mea-sured at their origins; proximal external diameters of the right and left external iliac arteries, measured at their origins; proximal external diameters of the right and left internal iliac arteries, measured at their origins.
Because of the different sizes of the fetuses the authors expressed each external diameter as a ratio of the proximal external diameter of the abdominal aorta. Both absolute and relative exter-nal diameters were correlated to fetal age in order to represent their growth. The results obtained were assessed using a one-way ANoVA test for unpaired data and post hoc RIR Tukey test. Re-gression analysis was used to determine the signifi-cance of the relation between gestational age and each diameter studied. Correlation coefficients (r) between particular external diameters and fetal age were estimated. Results were considered signifi-cant at P < 0.05.
Results
Aorto-Iliac Diameters 693
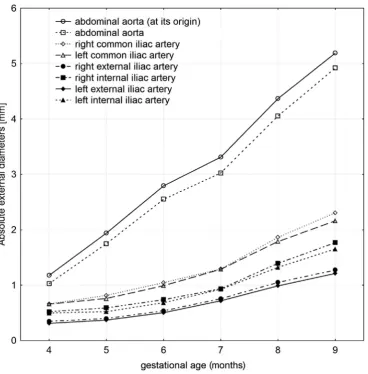
The numerical data revealed the approxi-mately linear increase in the absolute arterial di-ameters during gestation (Fig. 2). Correlation co-efficients between the external diameters and fetal age were statistically significant (P = 0.0000) for each age group and obtained the following val-ues: r1, 2 = 0.96 for the origin and bifurcation of
the abdominal aorta, r3 = 0.86 and r4 = 0.88 for the
right and left common iliac arteries, r5 = 0.88 and
r6 = 0.90 for the right and left external iliac
arter-ies, and r7 = 0.82 and r8 = 0.83 for the right and left
internal iliac arteries, respectively.
The strongest developmental dynamics re-ferred to the abdominal aorta diameters, from 1.18 ± 0.25 to 5.19 ± 0.49 mm for its origin, and from 1.03 ± 0.23 to 4.92 ± 0.46 mm for its bifurca-tion. The intermediate values in external diameter were found in both the common and internal iliac arteries. The values of the common iliac artery di-ameter varied from 0.66 ± 0.19 to 2.30 ± 0.42 mm on the right, and from 0.66 ± 0.14 to 2.16 ± 0.42 mm on the left. The external diameters of the inter-nal iliac arteries increased from 0.52 ± 0.15 to 1.77 ± 0.44 mm on the right and from 0.50 ± 0.14 to 1.65 ± 0.42 mm on the left for the 4-month and 9-month groups of gestation, respectively. The smallest values in external diameter were related to the external iliac arteries, which increased from 0.35 ± 0.09 to 1.28 ± 0.26 mm and from 0.31 ± 0.05
to 1.21 ± 0.22 mm on the right and left sides, re-spectively.
The external diameters of the right iliac ar-teries were found to be greater in comparison to the common (in 84 fetuses – 66.7%), external (in 88 fetuses – 71%), and internal (in 81 fetuses – 65.3%) ones. In 48 fetuses (38.7%) the three iliac arteries were stronger on the right, and in 8 fetuses (6.5%) – on the left side.
The relative growth of the external diameters of the abdominal aorta and iliac arteries was more differentiated than their absolute increase in values (Fig. 3) when compared to the proximal external diameter of the abdominal aorta. The relative ex-ternal diameter of the abdominal aorta at its bifur-cation was increasing throughout the study period. A different tendency was observed for the relative external diameters of the common, external and internal iliac arteries. They were found to decrease in their values in the age range of 4–5 months and to start increasing gradually afterwards.
Discussion
Reference data for the normal growth of ex-ternal diameters of the abdominal aorta and iliac arteries are scarce in human fetuses. Therefore, in this autopsy study, digital image analysis (Leica
Fig. 1. The abdominal aorta and iliac arteries in a female fetus aged 24 weeks: A) aortic hiatus of the diaphragm, B) aortic bifurcation, 1 – abdominal aorta, 2 – right com-mon iliac artery, 3 – left comcom-mon iliac artery, 4 – right external iliac artery, 5 – right internal iliac artery, 6 – left external iliac artery, 7 – left internal iliac artery
Table 1. External diameters of the abdominal aorta and iliac arteries in human fetuses Tabela 1. Średnice zewnętrzne aorty brzusznej i tętnic biodrowych u płodów człowieka Fetal age – months (Wiek płodowy – miesiące) N External diameters – mm (Średnice zewnętrzne – mm) abdominal aorta common iliac artery external iliac artery at its origin (1) at its end (2) right (3) left (4) right (5) mean SD mean SD mean SD mean SD mean SD mean 4 16
1.18 ↓(P
<
0.001)
0.25
1.03 ↓(P
<
0.001)
0.23
0.66 ↓(P
>
0.05)
0.19
0.66 ↓(P
>
0.05)
0.14
0.35 ↓(P
>
0.05
)
0.09
0.31 ↓(P
5
24
1.94 ↓(P
<
0.001)
0.32
1.75 ↓(P
<
0.001)
0.32
0.81 ↓(P
<
0.05)
0.25
0.76 ↓(P
<
0.01)
0.17
0.40 ↓(P
<
0.05
)
0.09
0.37 ↓(P
6
30
2.79 ↓(P
<
0.001)
0.35
2.55 ↓(P
<
0.001)
0.35
1.04 ↓(P
<
0.05)
0.23
0.99 ↓(P
<
0.001)
0.14
0.54 ↓(P
<
0.001)
0.10
0.50 ↓(P
7
22
3.31 ↓(P
<
0.01)
0.51
3.02 ↓(P
<
0.001)
0.50
1.29 ↓(P
<
0.01)
0.30
1.29 ↓(P
<
0.01)
0.27
0.76 ↓(P
<
0.001)
0.16
0.72 ↓(P
8
21
4.37 ↓(P
<
0.01)
0.50
4.05 ↓(P
<
0.001)
0.48
1.86 ↓(P
<
0.01)
0.47
1.79 ↓(P
<
0.01)
0.42
1.05 ↓(P
<
0.01)
0.22
0.99 ↓(P
Aorto-Iliac Diameters 695
QWin 16 Pro, Cambridge) was used to provide an objective comparative evolution of both absolute and relative external diameters of the aorto-iliac segment.
No significant difference between the two sexes was demonstrated in this series, in keeping with most previous studies in fetuses [12, 14], children [16, 17] and adults [18]. on the other hand, Pou-tanen et al. [19] found in children and adolescents that aortic diameters were greater in males than fe-males. Nevertheless, the values were independent of sex when indexed to BSA.
A linear growth of all the analyzed external diameters in fetuses was confirmed in this study. Correlation coefficients between the absolute ex-ternal diameters and fetal age were statistically significant (P = 0.0000) and the highest for the ab-dominal aorta (r1.2 = 0.96), the intermediate for the
right (r3 = 0.86) and left (r4 = 0.88) common iliac,
and right (r5 = 0.88) and left (r6 = 0.90) external
iliac arteries, and the lowest (r7 = 0.82; r8 = 0.83) for
the right and left internal iliac arteries. As it turned out, the decreasing sequence of external diameters with gestational age was presented by the following vessels: the abdominal aorta, right and left com-mon iliac artery, right and left internal iliac artery, and right and left external iliac artery.
The external diameter of the abdominal aorta was observed to be greater at its origin than its bi-furcation, being attributed to a gradual decrease in flow volume as blood is supplied to abdominal organs [20–25]. Özgüner and Sulak [12] reported that the proximal and distal external diameters of the abdominal aorta varied from 1.20 ± 0.2 mm and 1.12 ± 0.2 mm in fetuses aged 9–12 weeks to 8.28 ± 0.7 mm and 6.26 ± 0.6 mm respectively in fetuses aged 38–40 weeks. of note, in fetuses aged 13–37 weeks, which could be comparable to ours, ex-ternal diameters at the origin and bifurcation of the abdominal aorta increased from 2.85 ± 0.7 mm and 2.37 ± 0.6 mm to 5.77 ± 0.8 mm and 4.50 ± 0.4 mm, respectively.
Fig. 2. growth of the absolute external diameters of the abdominal aorta and iliac arteries
The external diameters of the common iliac ar-teries under examination were in keeping with re-sults reported by gościcka et al. [14]. According to Özgüner and Sulak [12], the external diameters of the common iliac arteries during the 9th–40th week
period increased from 0.92 ± 0.1 to 4.13 ± 0.3 mm on the right, and from 0.92 ± 0.7 to 4.07 ± 0.3 mm on the left. It is noteworthy that in fetuses aged 13–37 weeks, the external diameters of the common iliac arteries rose from 1.69 ± 0.3 to 3.06 ± 0.5 mm on the right, and from 1.63 ± 0.3 to 2.94 ± 0.5 mm on the left.
It is worth mentioning that the external diam-eters of the internal iliac arteries were found to be nearly 50% greater than those of the external iliac arteries. As predominant vessels, the internal iliac arteries supply pelvic organs, and then continue as the umbilical arteries to reach the placenta. Beyond doubt, in fetuses the pelvic organs need more blood supply than the lower limbs and the umbilical arteries are funtional ones. Therefore, in
contrast to adults, in fetuses the diameters of the internal iliac arteries are greater than those of the external iliac arteries [12, 14].
Data obtained in the material under examina-tion led authors to conclude that right-sided iliac arteries were stronger than left-sided ones when compared to common (66.7%), external (71%) and internal (65.3%) iliac arteries. All three iliac arteries were found to be stronger on the right – in 38.7% of specimens than on the left – in 5.5% of individuals (Fig. 1). Present findings are partly in disagreement with gościcka et al. [14], who stated that the left iliac arteries were always thinner than the right ones. Conversely, Özgüner and Sulak [12] emphasized no right-left difference in relation to the common, external and internal iliac arteries.
To date, there has been no information con-cerning the relative external diameters of the ab-dominal aorta and iliac arteries – something new which has been addressed by this study. Present results showed that the external diameter of the
Fig. 3. growth of the relative external diameters of the abdominal aorta and iliac arteries
Aorto-Iliac Diameters 697
abdominal aorta at its bifurcation indicated a rela-tive increase in values throughout gestation. The other external diameters presented during the 4th–
5th month of gestation showed a relative decrease
in their values, and then were increasing gradually afterwards. In authors opinion, this fact suggests that blood flow through the iliac arteries increases from the 6th month of gestation to provide more
and more blood to developing pelvic organs and lower limbs.
The external diameters of the abdominal aorta and iliac arteries do not show male-female differ-ences. The absolute values of the external diameters of the abdominal aorta and iliac arteries increase linearly throughout gestation. The relative values of the external diameters of the aortic bifurcation and three iliac arteries decrease during the 4th–5th
month period of gestation, to start increasing af-terwards.
References
[1] Angelini A, Allan LD, Anderson RH, Crawford DC, Chita SK, Ho SY: Measurements of the dimensions of the aortic and pulmonary pathways in the human fetus: a correlative echocardiographic and morphometric study. Br Heart J 1988, 60, 221–226.
[2] Ursell PC, Byrne JM, Fears TR, Strobino BA, Gersony MW: growth of the great vessels in the fetus with cardiac defects. Circulation 1991, 84, 2028–2033.
[3] Comstock CH, Riggs T, Lee W, Kirk J: Pulmonary-to-aorta diameter ratio in the normal and abnormal fetal heart. Am J obstet gynecol 1991, 165, 1038–1044.
[4] Hornberger LK, Weintraub RG, Pesonen E, Murilo-Olivas A, Simpson IA, Sahn C, Hagen-Ansert S, Sahn DJ:
Echocardiographic study of the morphology and growth of the aortic arch in the human fetus. observations related
to the prenatal diagnosis of coarctation. Circulation 1992, 86, 741–747.
[5] Hyett J, Moscoso G, Nicolaides K: Morphometric analysis of the great vessels in early fetal life. Hum Reprod 1995, 10, 3045–3048.
[6] Achiron R, Golan-Porat N, Gabbay U, Rotstein Z, Heggesh J, Mashiach S, Lipitz S:In utero ultrasonographic measurements of fetal aortic and pulmonary artery diameters during the first half of gestation. Ultrasound obstet gynecol 1998, 11, 180–184.
[7] Gembruch U, Shi C, Smrcek JM: Biometry of the fetal heart between 10 and 17 weeks of gestation. Fetal Diagn Ther 2000, 15, 20–31.
[8] Firpo C, Hoffman J, Silverman NH: Evaluation of Fetal Heart Dimensions from 12 Weeks to Term. Am J Cardiol 2001, 87, 594–600.
[9] Castillo EH, Arteaga-Martinez M, Garcia-Pelaez I, Villasis-Keever MA, Aguirre OM, Moran V, Vizcaino A:
Morphometric study of the human fetal heart. I. Arterial segment. Clin Anat 2005, 18, 260–268.
[10] Szpinda M: Morphometric study of the ascending aorta in human fetuses. Ann Anat 2007, 189, 465–472.
[11] Achiron R, Zimand S, Hegesh J, Lipitz S, Zalel Y, Rotstein Z: Fetal aortic arch measurements between 14 and
38 weeks’ gestation: in utero ultrasonographic study. Ultrasound obstet gynecol 2000, 15, 226–230.
[12] Özgüner G, Sulak O: Development of the abdominal aorta and iliac arteries during the fetal period: a morpho-metric study. Surg Radiol Anat 2011, 33, 35–43.
[13] Hirata K: A metrical study of the aorta and main aortic branches in the human fetus. Nippon Ika Daigaku Zasshi 1989, 56, 584–591.
[14] Gościcka D, Szpinda M, Stankiewicz W: Skeletopy of the common iliac arteries in human fetuses. Folia Morphol 1995, 54, 129–136.
[15] Iffy L, Jakobovits A, Westlake W, Wingate MB, Caterini H, Kanofsky P, Menduke H: Early intrauterine
devel-opment: I. The rate of growth of Caucasian embryos and fetuses between the 6th and 20th weeks of gestation.
Pediatrics 1975, 56, 173–186.
[16] Roman MJ, Devereux RB, Kramer-Fox R, O’Loughlin J: Two-dimensional echocardiographic aortic root dimen-sions in normal children and adults. Am J Cardiol 1989, 64, 507–512.
[17] Nidorf SM, Picard MH, Triulzi MO, Thomas JD, Newell J, King ME, Weyman AE: New perspectives in the assessment of cardiac chamber dimensions during development and adulthood. J Am Coll Cardiol 1992, 19, 983–988.
[18] Panagouli E, Lolis E, Venieratos D: A morphometric study concerning the branching points of the main arteries in humans: relationships and correlations. Ann Anat 2011, 193, 86–99.
[19] Poutanen T, Tikanoja T, Sairanen H, Jokinen E: Normal aortic dimensions and flow in 168 children and young adults. Clin Physiol Funct Imaging 2003, 23, 224–229.
[20] Dixon AK, Lawrence JP, Mitchell JRA: Age-related changes in the abdominal aorta shown by CT. Clin Radiol 1984, 35, 33–37.
[21] Arnot RS, Louw JH: The anatomy of the posterior wall of the abdominal aorta. Its significance with regard to hypoplasia of the distal aorta. S Afr Med J 1973, 47, 899–902.
[22] Baden JG, Racey DJ, Grist TM: Contrast-enhanced three-dimensional angiography of the mesenteric vasculature. J Magn Reson Imaging 1999, 10, 369–375.
Conflict of interest: None declared Received: 5.08,2011