http://www.ijcmph.com pISSN 2394-6032 | eISSN 2394-6040
Review Article
Effects of diabetes mellitus on gallbladder
Bandar Alshalawi
1*, Abdullah Almuslam
2, Reem Alqahtani
3, Al-Hanuf Al-Bokhari
4,
Wed Alnajjar
5, Amani Alsafi
6, Rehab Almajnooni
4, Firas Hasaballah
7,
Nof Alqarni
5, Mutlaq Alsolami
1INTRODUCTION
Type 2 diabetes has become prevalent worldwide.1 Gallstone disease residues a mutual gastrointestinal disorder in developed countries.2 The metabolic syndrome of truncal obesity, insulin resistance, type II diabetes mellitus, hypertension, and hyperlipidemia is linked with increased hepatic cholesterol secretion and is a major risk factor for the development of cholesterol gallstones. Gallstone disease is associated to numerous cardiometabolic risk factors, for example, obesity, unhealthy diet, sedentary lifestyle, and dyslipidemias (hypertriglyceridemia and low high-density lipoprotein
cholesterol).3,4 Furthermore, there is expanding confirmation to recommend that parts of the metabolic disorder including insulin protection, hyperinsulinemia, and elevated triglycerides might be related with expanded hazard.5
Epidemiological investigations on the danger of gallbladder sickness among diabetes patients have been conflicting. A few investigations have discovered a positive relationship amongst diabetes and danger of gallbladder illness or gallstones.6 nevertheless, different examinations found no relationship.7 Furthermore, the extent of the hazard assessments has changed
ABSTRACT
Diabetes has been theorized to build the danger of gallbladder complaint in light of the perception that insulin resistance and obesity are related with gallbladder. We conducted this meta-analysis using a comprehensive search of MEDLINE, PubMed, EMBASE, Cochrane Database of Systematic Reviews, and Cochrane Central Register of Controlled Trials till 15 January 2017 for prospective observational studies that assessed the relationship of the effects of diabetes mellitus on gallbladder. We identified 8 prospective studies that could be included in the meta-analysis which included 6,089,807 participants. The summary RR for diabetes patients was 1.42 (95% CI: 1.32–1.87, I2=99.4%, p<0.0001). Although heterogeneity in general was very high, there was no heterogeneity between the studies with longer duration of follow-up. There was no evidence of publication bias. Our study shows additional support for an increased risk of gallbladder disease between diabetes patients.
Keywords: Gallstones, Gallbladder disease, Diabetes mellitus 1
King Abduaziz University, Rabigh, KSA
2Imam Abdulrahman Bin Faisal University, Dammam, KSA
3King Khalid University, Abha, KSA
4Umm-AlQura University, Makkah, KSA
5
King Abdulaziz University, Jeddah, KSA
6King Fahad Armed Forces Hospital, Jeddah, KSA
7Alfaisal University, Riyadh, KSA
Received: 08 May 2018
Accepted: 25 May 2018
*Correspondence:
Dr. Bandar Alshalawi,
E-mail: [email protected]
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
impressively, and this could conceivably be because of frustrating by other hazard factors, for example, physical activity, obesity or other hazard factors. As the pervasiveness of diabetes is anticipated to increment from 366 million individuals in 2011 to 552 million by 2030 it will be essential to illuminate whether there is a relationship between a diabetes determination and gallbladder sickness hazard free of body bloatedness and other frustrating elements.
Consequently, we conducted a meta-analysis of prospective studies to define the overall shape of the association between the effects of diabetes mellitus on Gallbladder.
METHODS
Data sources and searches
We conducted this meta-analysis using a comprehensive search of MEDLINE, PubMed, EMBASE, Cochrane Database of Systematic Reviews, and Cochrane Central Register of Controlled Trials till 15 January 2017 for prospective observational studies that assessed the relationship of the effects of diabetes mellitus on Gallbladder. Both semiparametric and parametric methods were used. No language restrictions were imposed. We followed the standard guidelines for conducting and reporting meta-analyses of observational studies.8
Selection criteria
Studies were included in this meta-analysis if they satisfied the following criteria: the study design was prospective, the exposure of interest was Gallbladder, the outcome was diabetes mellitus, and the investigators reported relative risks (RRs) with 95% Cis. If study populations were reported more than once, we used the result with the longest follow-up duration. Flow diagram showing the selection criteria of assessed studies.9
Data extraction
Two reviewers independently reviewed studies, abstracted data, and resolved disagreements by consensus. Studies were evaluated for quality. A review protocol was followed throughout. We extracted the following data from each study: year of publication, authors, study location, study name, years of follow-up, sample size (number of participants and incident cases), type of diabetes mellitus, and Relative risk (95% confidence interval).
Statistical analysis
The present meta-analysis utilized Stata version 12.0 software for statistical analysis. Mean Difference (MD)
Heterogeneity amongst the trials was determined by means of the Cochran Q value and quantified using the I2 inconsistency test with a significance set at the p value <0.10 or I2 score >50%.10 Whenever it was possible, results were evaluated either considering all the included studies or considering only the randomized trials. Random-effects model were calculated using summary relative risks of gallbladder disease for patients with diabetes mellitus compared with patients without diabetes mellitus.11 .
RESULTS
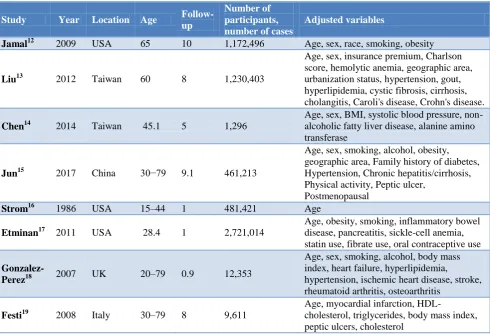
We recognized 872 citations using the search strategy. Of these, we excluded 313 after examining the title and abstract including removal of duplicates. We retrieved and evaluated 22 articles in more detail, of which 14 articles were excluded, leaving 8 studies that were eligible for inclusion (Figure 1).12-19 Major characteristics of included studies have been summarized in Table 1.
Figure 1: Flow diagram showing the selection criteria of assessed studies.9
The summary relative risk for patients with diabetes mellitus versus patients without diabetes was 1.42 (95% CI: 1.32–1.87) with very high heterogeneity, I2=93.6%, p<0.0001. There was no evidence of publication bias neither with Egger's test, p=0.68 nor with Begg's test, p=0.41.
Table 1: Characteristics of included studies.
Study Year Location Age Follow-up
Number of participants, number of cases
Adjusted variables
Jamal12 2009 USA 65 10 1,172,496 Age, sex, race, smoking, obesity
Liu13 2012 Taiwan 60 8 1,230,403
Age, sex, insurance premium, Charlson score, hemolytic anemia, geographic area, urbanization status, hypertension, gout, hyperlipidemia, cystic fibrosis, cirrhosis, cholangitis, Caroli's disease, Crohn's disease.
Chen14 2014 Taiwan 45.1 5 1,296
Age, sex, BMI, systolic blood pressure, non-alcoholic fatty liver disease, alanine amino transferase
Jun15 2017 China 30−79 9.1 461,213
Age, sex, smoking, alcohol, obesity, geographic area, Family history of diabetes, Hypertension, Chronic hepatitis/cirrhosis, Physical activity, Peptic ulcer,
Postmenopausal
Strom16 1986 USA 15–44 1 481,421 Age
Etminan17 2011 USA 28.4 1 2,721,014
Age, obesity, smoking, inflammatory bowel disease, pancreatitis, sickle-cell anemia, statin use, fibrate use, oral contraceptive use
Gonzalez-Perez18 2007 UK 20–79 0.9 12,353
Age, sex, smoking, alcohol, body mass index, heart failure, hyperlipidemia,
hypertension, ischemic heart disease, stroke, rheumatoid arthritis, osteoarthritis
Festi19 2008 Italy 30–79 8 9,611
Age, myocardial infarction,
HDL-cholesterol, triglycerides, body mass index, peptic ulcers, cholesterol
Table 2: Effects of diabetes mellitus on gallbladder.
Study OR 95% CI
Jamal12 1.81 (1.77–1.85)
Liu13 1.08 (1.05–1.10)
Chen14 1.68 (1.10–3.87)
Jun15 1.17 (1.10-1.25)
Strom16 2.60 (2.40–2.70)
Etminan17 1.67 (1.59–1.74)
Gonzalez-Perez18 1.02 (0.80–1.29)
Festi19 1.75 (1.04–2.96)
Table 3: Subgroup analyses.
Diabetes mellitus and gallbladder disease
N RR (95% CI) I2 (%) P value
Age Yes 8 1.42 (1.31–1.87) 98.6 <0.0001
No 0
BMI or obesity Yes 6 1.59 (1.38–1.81) 86.6 <0.0001
No 2 1.55 (1.12–2.17) 97.4 <0.0001
Physical activity Yes 1 1.20 (1.10–1.31)
No 7 1.61 (1.19–2.11) 84.6 <0.0001
Smoking Yes 4 1.54 (1.38–1.91) 85.1 <0.0001
No 4 1.61 (1.14–2.41) 96.3 <0.0001
DISCUSSION
Numerous potential mechanisms might assist to explain the relation between type 2 diabetes and gallbladder disease. Higher prevalence of gallbladder disease has been reported in persons with insulin resistance, obesity, metabolic syndrome, and hyperinsulinemia.20-22 The cohabitation of these risk factors for type 2 diabetes may be the cause that participants with gallbladder disease had an increased diabetes risk. The adjustment for body mass index and waist circumference moderately attenuated the association between gallbladder disease and type 2 diabetes, suggesting that obesity might only partly explain the higher risk of type 2 diabetes in patients with gallbladder disease.15 The present analysis recommends that a diagnosis of diabetes mellitus can increase the relative risk of gallbladder disease. Positive relations were perceived both in women and men, however, were more noticeable between American studies than in European and Asian studies, nevertheless, there were few examinations from the concluding geographic areas. The present analysis is reliable with different examinations which have discovered that the obesity, insulin resistance, metabolic disorder are related with increased gallbladder disease, as all these factors similarly are strictly associated to the risk of type 2 diabetes.23
Numerous biological mechanisms might clarify an increased risk of gallbladder disease in patients with diabetes mellitus. It has been described that the biliary saturation index is increased and gallbladder motility is decreased in diabetes patients. While the mechanism for the dysmotility in diabetes patients is not fully assumed it has been recommended that it might be as a result of denervation affected by visceral neuropathy.
In the current analysis, the relationship between diabetes and gallbladder disease was reliant on the abdominal obese status in women. The stronger relationship was perceived in non-abdominal obese than abdominal obese women. A study described a comparable interaction between gallbladder disease and abdominal obesity on diabetes.24 It is possible that obese women already had a high risk of diabetes, and gallbladder disease added only modestly deleterious effect on the relative scale. Nevertheless, the absolute risk linked with abdominal obesity between women with gallbladder disease was much greater than those without abdominal obesity. Our result of an increased risk of gallbladder disease among diabetes patients is reliable with studies relating diabetes to increased gallbladder cancer risk, such as gallstones and gallbladder disease are risk factors for gallbladder cancer.24
CONCLUSION
There is a possible risk of the relation between diabetes patients to develop gallbladder disease. To confirm these
Large-scale and long-term randomized controlled trials in various populations must be carried out in future studies to deliver more significant evidence.
Funding: No funding sources Conflict of interest: None declared Ethical approval: Not required
REFERENCES
1. Billings LK, Florez JC. The genetics of type 2 diabetes: what have we learned from GWAS? Ann N Y Acad Sci. 2010;1212:59-77.
2. Portincasa P, Moschetta A, Palasciano G.
Cholesterol gallstone disease. Lancet.
2006;368(9531):230-9.
3. Zaliekas J, Munson JL. Complications of gallstones: the Mirizzi syndrome, gallstone ileus, gallstone pancreatitis, complications of "lost" gallstones. Surg Clin North Am. 2008;88(6):1345-68.
4. Ata N, Kucukazman M, Yavuz B, Bulus H, Dal K, Ertugrul DT, et al. The metabolic syndrome is associated with complicated gallstone disease. Can J Gastroenterol. 2011;25:274–6.
5. Banim PJ, Luben RN, Bulluck H, Sharp SJ, Wareham NJ, Khaw KT, et al. The aetiology of symptomatic gallstones quantification of the effects of obesity, alcohol and serum lipids on risk. Epidemiological and biomarker data from a UK. prospective cohort study (EPIC-Norfolk). Eur J Gastroenterol Hepatol. 2011;23(8):733-40.
6. Campbell PT, Newton CC, Patel AV, Jacobs EJ, Gapstur SM. Diabetes and cause-specific mortality in a prospective cohort of one million U.S. adults. Diabetes Care. 2012;35(9):1835-44.
7. Boland LL, Folsom AR, Rosamond WD;
Atherosclerosis Risk in Communities (ARIC) Study Investigators. Hyperinsulinemia, dyslipidemia, and obesity as risk factors for hospitalized gallbladder disease. A prospective study. Ann Epidemiol. 2002;12(2):131-40.
8. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000;283:2008–12.
9. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement 2007. 10. Higgins JP, Thompson SG, Deeks JJ. Altman DG.
Measuring inconsistency in meta-analyses 2008. 11. DerSimonian R, Laird N. Meta-analysis in clinical
trials. Controlled Clinical Trials. 1986;7(3):177-88. 12. Jamal MM, Yoon EJ, Vega KJ, Hashemzadeh M,
symptomatic gallstone disease in diabetic patients. World J Gastroenterol. 2012;14;18(14):1652-9. 14. Chen JY, Hsu CT, Liu JH, Tung TH. Clinical
predictors of incident gallstone disease in a Chinese
population in Taipei, Taiwan. BMC
Gastroenterology. 2014;14:83.
15. Strom BL, Tamragouri RN, Morse ML, Lazar EL, West SL, Stolley PD, et al. Oral contraceptives and other risk factors for gallbladder disease. Clin Pharmacol Ther. 1986;39(3):335-41.
16. Etminan M, Delaney JA, Bressler B, Brophy JM. Oral contraceptives and the risk of gallbladder disease: a comparative safety study. CMAJ. 2011;183(8):899-904.
17. González-Pérez A, García Rodríguez LA. Gallbladder disease in the general population: association with cardiovascular morbidity and
therapy. Pharmacoepidemiol Drug Saf.
2007;16(5):524-31.
18. Festi D, Dormi A, Capodicasa S, Staniscia T, Attili AF, Loria P, et al. Incidence of gallstone disease in Italy: results from a multicenter, population-based Italian study (the MICOL project). World J Gastroenterol. 2008;14(34):5282-9.
19. Chang Y, Sung E, Ryu S, Park YW, Jang YM, Park M. Insulin resistance is associated with gallstones even in non-obese, non-diabetic Korean men. J Korean Med Sci. 2008;23(4):644-50.
20. Völzke H, Baumeister SE, Alte D, Hoffmann W, Schwahn C, Simon P, et al. Independent risk factors for gallstone formation in a region with high cholelithiasis prevalence. Digestion. 2005;71(2):97-105.
21. Ruhl CE, Everhart JE. Association of diabetes, serum insulin, and C-peptide with gallbladder disease. Hepatology. 2000;31(2):299-303.
22. Méndez-Sánchez N, Chavez-Tapia NC, Motola-Kuba D, Sanchez-Lara K, Ponciano-Rodríguez G, Baptista H, et al. Metabolic syndrome as a risk factor for gallstone disease. World J Gastroenterol. 2005;11(11):1653-7.
23. Weikert C, Weikert S, Schulze MB, Pischon T, Fritsche A, Bergmann MM, et al. Presence of gallstones or kidney stones and risk of type 2 diabetes. Am J Epidemiol. 2010;171(4):447-54. 24. Gu J, Yan S, Wang B, Shen F, Cao H, Fan J, Wang
Y. Type 2 diabetes mellitus and risk of gallbladder cancer: a systematic review and meta-analysis of observational studies. Diabetes Metab Res Rev. 2016;32(1):63-72.