http://www.ijcmph.com pISSN 2394-6032 | eISSN 2394-6040
Original Research Article
Contributing factors for intestinal parasitic infection
in children: a study of Nepal
Rajesh Kumar Das
1*, Pradip Kumar Mahato
2, Prabin Neupane
3INTRODUCTION
Protozoa and Helminthes are the common causes of intestinal health problems in the tropical and subtropical regions of the world. According to World Health Organization (WHO), around 450 million people develop parasitic illnesses around the world.1 Up to 270 million preschool and 600 million school children are living in area where high transmission of parasitic worm occurs. These indicate that children are the major risk group for
parasitic infection in many developing countries. The major reasons behind such infections have been attributed to deteriorated environment, contaminated water supply, poverty and poor sanitation.2
The parasitic diseases are commonly manifested as enteritis, diarrhoea, and dysentery. The common intestinal parasites causing infections are Entamoeba histolytica, Giardia lamblia (G. duodenalis, G. intestinalis), Cryptosporidium parvum or Cryptosp-oridium hominis and others. Intestinal parasites like
ABSTRACT
Background: Intestinal parasitic diseases are common health problems among children in Nepal. The presence of these diseases is an indication of poor hygienic practices. So our objective is to find out the factors that are responsible to cause such infections in our study population.
Methods: This is a cross-sectional study to find the causes of parasitic intestinal infection in children. Stool specimens were collected from children below 15 years and studied by microscopy method to detect the causative organisms of infection.
Results: Among the sample size of 305, 154 (50.5%) cases were found microscopically positive for parasitic
diseases. Age and sex-wise study did not show the significant relationship (P>0.05) for infection. Entamoeba histolytica and Giardia lamblia had higher prevalence i.e., 18.03% (55/154) and 16.06% (49/154). Likewise, infection was higher in children using untreated water sources and municipal water. Many children with unsanitary habits like not washing hands properly before and after eating meals and after using toilet and nail biting habits developed more positive infection. The relationship in this case was significant (P<0.05).
Conclusions: Thus, the contributing factors for intestinal parasitic infection in children are lack of hygienic practices
among children. Such habits can cause ingestion of infective parasites in the intestine which eventually causes diseases.
Keywords: Parasitic infection, Microscopy, Prevalence, Unsanitary habits, Hygienic practices
1
Department of Epidemiology, University of Indonesia, Depok, Indonesia
2Department of Zoology, Khalinga University, India
3Department of Microbiology, Kathmandu College of Science and Technology, Tribhuvan University, Kathmandu,
Nepal
Received: 18 April 2019
Revised: 07 June 2019
Accepted: 08 June 2019
*Correspondence:
Mr. Rajesh Kumar Das,
E-mail: [email protected]
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under
the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ascaris lumbricoides, Trichuris trichiura and
Ancylostoma duodenale are the most prevalent and affect about one-sixth of the world population.3 Amoebiasis (disease caused by Entamoeba histolytica) is the third leading cause of death from parasitic diseases worldwide, with its greatest impact on the children of developing countries. In developed countries, protozoan parasites more commonly cause gastrointestinal infections compared to helminthes.4
The most common causes of intestinal parasites are through consumption of contaminated water, infected soil, inadequate sanitation and hygiene, and improper hygiene.5 Colonization of IPs in gastro-intestine of children results growth retardation and reduced mental development, school absenteeism, low academic performance, susceptible to malnutrition and infection.6 Unsafe disposal of human waste, unsanitary habits i.e. lack of hand washing facilities, eating unwashed raw vegetables and fruits, soil-eating behavior and lack of available safe water invite the organisms into the body.7 According to the annual report Nepal, intestinal worm infection ranks fourth accounting for morbidity among "top-ten-diseases".8 In Nepal, 25% of population is below poverty line and they have little or no access to primary health care, and other basic services. In such circumstances, the government plan to bring down the infection rate has been affected as shown by researches conducted in various districts of Nepal.9,10
In the context of Nepal, continuous monitoring of intestinal parasitic infections and their associated risk factors are essential to save children. There is no recent information about intestinal parasitic infection and associated risk factors in the study area. Therefore, the present study was aimed to determine the status of the intestinal parasitic infection in children.
METHODS
Study area and population
This cross-sectional study was carried out children (0-15 years) from January-August 2017 in Sunsari district of Eastern plains of Nepal which borders with Bihar, a highly populated state of India. This region has warm and humid sub-tropical climate that may contribute to higher chances of parasitic diseases. For this study, stool specimens were collected from the children hailing from the rural areas. These areas do not access to basic sanitary facilities and open-defecation is not rare. The sample size was 305 and collected from subjects willing to participate in research work. Each enrolled subject's information about age, gender, hand washing practices and others were taken in the form of a questionnaire.
Ethical consideration
Informed consent was obtained from the parents or local guardian prior to the study and also the questionnaires
were filled before the specimen collection.
Specimen collection
The subjects were provided with wide mouthed clean, dry, properly labeled glass container for collection of samples and recommended 5 grams of solid or 10 ml of liquid stool to be collected. The stool specimens were examined under microscope using direct wet mount (saline) and iodine wet mount preparation to detect protozoal tropozoites, helminth eggs or larvae and parasitic cysts the results were recorded.
Inclusion and exclusion criteria
Subjects below 15 years and willing to participate were included in this study while those who were not interested and above 15 years were excluded from this study. Also samples not properly labeled were not processed.
Faecal examination
Diagnosis of intestinal parasitic infections was done by microscopic examination of the stool. Wet mount examination was used for stool microscopy. Several mounting fluids such as saline, iodine, methylene blue and lacto-phenol cotton blue (LPCB) have been employed for preparation of stool wet mounts. According to traditional method of stool wet mount preparation, 1-2 drops of the mounting fluid (saline, iodine, methylene blue or LPCB) were first placed on to a clean glass slide, 1-2 g of stool is mixed with it and a suspension of stool is prepared. The stool suspension was covered with a cover slip and examined microscopically.11 Similarly, a greater volume of faeces can be added to a drop of methylene blue-glycerol solution on a microscope glass slide to make a thick smear. Likewise, saline wet mounts and iodine wet mount were prepared by separately mixing a small volume of stool sample with a drop of physiological saline, methylene blue dye, and Lugol’s iodine (diluted in 1:5 distilled water), respectively, on a glass slide and placing a coverslip over the smear.
Statistical analysis
The obtained data analysis was performed using Microsoft excel 7 version. Association of intestinal parasitosis was assessed by using the chi-square test and p<0.05 were considered as statistically significant.
RESULTS
Table 1: Sex-wise distribution of cases (n=154).
Gender Total Positive (%) P value
Male 178 95 (53.37)
0.790
Female 127 59 ( 46.46)
Table 2: Age-wise distribution of cases.
Age-group (years)
Total cases
Positive cases
N (%) P value
1-5 66 45 (68.18)
0.196
5-10 150 67 (44.66)
10-15 89 42 (47.2)
Total 305 154 (50.50)
Table 3: Frequency distribution of parasites detected in children.
Parasite types Total
positive (%)
Prevalence (%)
Protozoan parasites 106 (34.75) 34.75
Entamoeba histolytica 55(35.71) 18.03
Giardia lamblia 49(31.81) 16.06
Cryptosporidium 2(1.30) 0.06
Helminthes 29 (18.83) 9.5
Ascaris lumbricoides 7(4.54) 2.29
Ancylostoma duodenale 10(6.49) 3.27
Hymenolepsis nana 9(5.84) 2.95
Taenia spp. 1(0.65) 0.32
Trichuris trichium 1(0.65) 0.32
Enterobius vermicularis 1(0.65) 0.32
Mixed infection 19 (12.33) 6.22
Total 154 (100) 50.50
Table 4: Relationship between drinking water sources and infection.
Water sources Total Infection
(%) P value
Filtered water 14 4 (28.57)
0.526
Hand pump water 140 72 (51.42)
Treated water 8 1 (12.5)
Municipal water 72 38 (52.77)
Well water 16 9 (56.25)
Various source 55 30 (54.54)
Total 305 154
Age-wise microscopic results showed highest prevalence of intestinal diseases in the age-group 5-10 years i.e., 68.18% (45/66) while in the age-group 5-10 and 10-15 years, prevalence was nearly same i.e., 44.66% (67/150) and 47.2% (42/89). There is no association between the age and the incidence of intestinal diseases (P>0.05).
Prevalence and distribution of intestinal parasites
In microscopic examination of stool specimen, children were found infected with different causative agents. The causative agents were protozoa, helminthes and in some cases were found infected with more than one agents were grouped as mixed infection cases. Majority of the children had infection with protozoan parasite 106 (68.83%), secondly many had helminthic infection 29 (18.83%) and those with mixed infection were 19 (6.2%). The occurrences of protozoan diseases caused by
Entamoeba histolytica and Giardia lamblia were higher than helminthic.
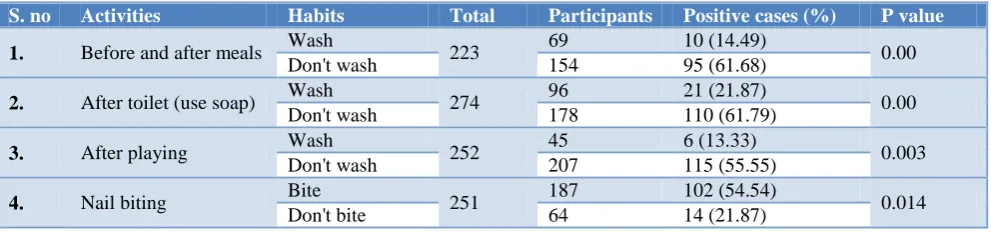
Table 5: Children’s habit about cleaning hand using soap.
S. no Activities Habits Total Participants Positive cases (%) P value
1. Before and after meals Wash 223 69 10 (14.49) 0.00 Don't wash 154 95 (61.68)
2. After toilet (use soap) Wash 274 96 21 (21.87) 0.00 Don't wash 178 110 (61.79)
3. After playing Wash 252 45 6 (13.33) 0.003 Don't wash 207 115 (55.55)
4. Nail biting Bite 251 187 102 (54.54) 0.014 Don't bite 64 14 (21.87)
Relationship between drinking water sources and infection
The higher percentage of positive cases of parasitic infection was found in children who used well water, mixed sources, municipal water and hand pump water. The children using filtered and treated water were less affected with parasitic diseases. However, the result was statistically insignificant (P>0.05) as shown below.
Children’s habit about cleaning hand
According to questionnaires filled, infection rate was higher in children who didn't wash hands properly before and after activities like eating, playing, and defecation and also because of nail biting practices. The relationships were significant (p<0.05).
DISCUSSION
In our study, the results of microscopy showed that various protozoan and helminthic organisms were involved in the parasitic diseases. The prevalence rate of intestinal parasitic was high in our study 50.5% (n=154). This rate is closer to prevalence rate of (58.77%) in Kathmandu, Nepal.13 This finding is also comparable to Magar et al which were 43.3% in the study of a slum area of Kathmandu valley.14 But this rate is higher than other similar study in Western India.12 Such kind of higher prevalence can be attributed to factors like, low socioeconomic status, lack of education, lack of access to treated water etc. Moreover, delayed diagnosis and prevailing environmental factors can make other susceptible children its target for parasitosis; ultimately increasing the infection rate.
Sex-wise prevalence of intestinal parasitic infection (IPI) was found higher in male 53.37% (n=95) than female 46.46% (n=59) but statistically not significant. On the basis of gender, IPI in female children was higher than male children compared to studies like in Chitwan, Nepal 24.8% female and 21.8% male.15 Also the study in Northern Indian state, Uttarakhand, infection was seen more in female patients (17.07%) when compared to males (8.33%) shows the same contrary result.16 The relatively higher prevalence in males is not clearly understood but it may be assumed that they are comparatively more exposed unhygienic practices than female.
In this study, the highest number of parasitic infection was seen between 1 to 5 years age followed by 10-15 years. Pradhan et al reported intestinal parasitic infection was highest among children aged less than 6 years (37.5%) and Khadka et al revealed the occurrence of parasitic infection was highest in age group 8-12 years and lowest in age group 12-15 years; however, it was statistically insignificant. As soon as the children become 1 year of age, they start to walk independently and try to touch, feel or taste their surrounding objects.17,18 Also they spend most of their time playing and many may have habit of sucking their fingers. In Nepal, children start going to school at 5 years so they are at home until 5 years. In such circumstance, uneducated mothers cannot train their child to protect from unhygienic habits.
Protozoan organisms seem to be main causative agent of parasitic diseases in our study. Comparison of infection rate between protozoa (34.75%) and helminth (9.5%) shows protozoan parasites infects more children. Among the protozoan diseases, Entamoeba histolytica, Giardia lamblia and Cryptosporidium were the causative agents of the infection. Some children were found infected with both protozoa and helminthes and they were grouped under mixed infection. The overall prevalence rate of mixed infection was 6.2%. This finding is in accordance with study of Rai et al.19 But the prevalence rate is quite
higher than study in Laitpur, Nepal.20 In mixed parasitic infection or multi-parasitism cases, the children were found to have infection with Entamoeba histolytica and
Giardia, Giardia and hookworm, Entamoeba histolytica
and Hookworm, Entamoeba histolytica and
Hymenolepsis nana and many others. This finding was in accordance with various previous findings from Nepal.18,19,21
According to this study, the most prevalent parasites were 18.03% Entamoeba histolytica, 16.06% Giardia lamblia, 0.06% Cryptosporidium spp, 2.29% Ascaris lumbricoides, 3.27% Hookworm, 2.95% Hymenolepis nana, 0.32% Tapeworm, 0.32% Trichuris trichium and 0.32% Enterobius vermicularis. Entamoeba histolytica
was predominant parasites to cause parasitic infection. Shrestha et al also found Entamoeba histolytica was found to be predominant (9.23%) followed by Giardia lamblia (5.76%). Trichuris trichuria (5%) was the commonest helminth accompanied by Ancylostoma duodenale (2.65%) and Ascaris lumbricoides (2.3%).22 As per the results of both studies, Entamoeba histolytica
was the main cause of intestinal parasitic infection which is similar to this study.
The finding shows a big difference in the infection rate among the children using various sources of water. Highest occurrence rate (56.25%) of intestinal parasites was found in children consuming well water. Second highest occurrence was found in those who used water from various sources like lake, river or others and such people were included under mixed water sources. From our finding, we understand open water sources are heavily contaminated now-a-days because of human activities. Such water source can no longer be safe for drinking purpose. For instance, children who consumed treated water were less attacked by parasitic diseases.
After extraction, improper treatment and improper management of water supply may cause to mix with sewage before reaching to the household works and drinking. Increasing human activities give an easy access to pathogenic organisms to water sources. In the rainy season, the over flooded water, the sewage water etc. are contaminated with supply water.23 Drinking direct water accelerates the infection rate given the chances of contamination and transmission are high.10
by Yodomani et al and Suharijha et al which is in accordance with this study.24,25
CONCLUSION
The finding of this study shows protozoa is the main causative agent of intestinal parasitic diseases in our study population. Among the parasites, Entamoeba histolytica and Giardia are the major threats. Higher prevalence is found in children consuming untreated and open water sources. Besides, unhygienic habits seem to be another important factor to cause intestinal infections. Habits like not washing hands with soap and water and nail biting practices can easily spread the infection.
Funding: No funding sources Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee
REFERENCES
1. Bdri S, Adwen G. Prevalence of intestinal parasitic infections in Jenin Governorate, Palestine: a 10 year retrospective study. Asian Pacific J Trop Med. 2010;3(9):745–7.
2. World Health Organization (WHO): Neglected Tropical Diseases - PCT Databank 2010.
3. Harhay M, Horton J, Olliro P. Epidemiology and control of human gastrointestinal parasites in children. Expert Rev Anti-Infect Ther. 2010;8(2):219–34.
4. Rashidul Haque. Human Intestinal Parasites. J Health Popul Nutr. 2007;25(4):387-91.
5. Kathrin Z, Benjamin S, Daniel M, Robert B, Jennifer K, Jürg U. Effect of Sanitation on Soil-Transmitted Helminth Infection: Systematic Review and Meta-Analysis. PLOS Medicine. 2012;9(1):e1001162.
6. Brooker S. Estimating the global distribution and disease burden of intestinal nematode infections: adding up the numbers – a review. Int J Parasito. 2010;40(10):1137–44.
7. Freeman MC, Chard AN, Nikolay B, Garn JV, Okoyo C, Kihara J, et al. Associations between school- and household-level water, sanitation and hygiene conditions and soil-transmitted helminth infection among Kenyan school children. Parasites & Vectors. 2015;8:412.
8. Department of Health Services (DoHS), Ministry of Health and Population, Kathmandu, Nepal Annual Report-2010/2011.
9. Shrestha R, Maharjan M. Prevalence of intestinal helminth parasites among school-children of Bhaktapur district, Nepal. Nepalese J Zoology. 2013;1:48.
10. Sherchand JB, Ohara H, Sherchand S, Cross JH, Shrestha MP. Intestinal parasitic infections in rural
areas of Southern Nepal. J Inst Med. 1997;19:115-21.
11. Parija SC. Stool Microscopy, Nepal: BPKIHS. 1998;88.
12. Mishra S, Duttroy B, Shroff B. The prevalence of intestinal parasitic infections in the urban slums of a city in Western India. J Infect Public Health. 2013;6(2):142-9.
13. Yadav K, Prakash S. Study of Intestinal Parasitosis among School Children of Kathmandu, Nepal: Asian J Biomed Pharmaceutical Sci. 2016;6:59:40-7.
14. Thapa Magar D, Rai SK, Lekhak B, Rai KR. Study of parasitic infection among children of Sukumbasi Basti in Kathmandu valley. Nepal Med Coll J. 2011;13(1):7-10.
15. Bhattachan B, Panta YB, Tiwari S, Thapa Magar D, Sherchand JB. Intestinal Parasitic Infection among School children in Chitwan district of Nepal. J Institute Med. 2015;37(2):79-84.
16. Kotiak S, Sharma M, Juyal D, Sharma N. Intestinal parasitic infection-intensity, prevalence and associated risk factors, a study in general population from the Uttarakhand hills. Int J Med Public Health. 2014;4:422-5.
17. Pradhan P, Bhandary S, Shakya PR, Acharya T, Shrestha A. Prevalence of intestinal parasitic infections among public school children in a rural village of Kathmandu Valley Nepal. Med Coll J. 2014;16:50-3.
18. Khadka SK, Kaphle PH, Gurung K, Shah Y, Sigdel M. Study of Intestinal Parasitosis among School Going Children in Pokhara, Nepal. JHAS. 2013;3:47-50.
19. Rai L, Saud B, Paudel G, Dhungana G. Prevalence of Intestinal Parasitic Infection among Rural Area School Children of Lokhim VDC, Nepal. J Microbiol Exp. 2017;4(1):00102.
20. Tandukar S, Ansari S, Adhikari N, Shrestha A, Gautam J, Sharma B, et al. Intestinal parasitosis in school children of Lalitpur district of Nepal. BMC. 2013;6:449.
21. Ishiyama S, Rai SK, Ono K, Uga S. A small-scale study on intestinal on parasitos in a remote village in Nepal. Nepal Med Coll J. 2004;5:28-30.
22. Shrestha A, Narayan KC, Sharma R. Prevalence of Intestinal Parasitosis among School Children in Baglung District of Western Nepal. Kathmandu Univ Med J. 2012;10:3-6.
23. Rai DR. Factors Associated with Intestinal Parasitic Infection among School Children in Rural Area of Kathmandu Valley, Nepal. Nepal Med Coll J. 2005;7(1);43-6.
transmitted helminthiasis. Asian Parasite Control Organ. 1983;2:89-103.
25. Suharijha I, Bintari R. Nail and dust examination for helminthic eggs in orphanages. In: Collected papers on the control of soil transmitted helminthiasis. Asian Parasite Control Organ.1983;6:59-61.
Cite this article as: Das RK, Mahato PK, Neupane P.