Measuring the
“
Triple Aim
”
in Transition Care:
A Systematic Review
abstract
BACKGROUND AND OBJECTIVES: Without adequate support, adoles-cents transitioning from the pediatric to the adult health care system are at increased risk for poor health outcomes. Numerous interven-tions attempt to improve this transition, yet few comprehensively eval-uate efficacy. To advance evaluation methods and ultimately the quality of transition services, it is necessary to understand the current state of health care transition measurement. This study examines and catego-rizes transition measures by using the “Triple Aim” framework of experience of care, population health, and cost of care.
METHODS:Ovid Medline and the Cumulative Index to Nursing and Allied Health Literature were searched for articles published between 1995 and 2013. Two reviewers independently screened studies and included those that evaluated the impact of a health care transition intervention. Measures were subsequently classified according to population health, experience of care, and costs of care.
RESULTS:Of the 2282 studies initially identified, 33 met inclusion cri-teria. Population health measures were used in 27 studies, with disease-specific measures collected most frequently. Fifteen studies measured cost, most often service utilization. Eight studies measured experience of care, with satisfaction assessed most commonly. Only 3 studies examined all 3 domains of the“Triple Aim.” Transition interventions described in the gray literature were not reviewed.
CONCLUSIONS: Transition programs are inconsistently evaluated in terms of their impact on population health, patient experience, and cost. To demonstrate improvement in the transition from pediatric to adult health care, a more robust and consistent set of measures is needed.Pediatrics2014;134:e1648–e1661
AUTHORS:Megan Prior, BA,a,bMargaret McManus, MHS,a
Patience White, MD, MA,aand Laurie Davidson, MLIS, MEdb
aThe National Alliance to Advance Adolescent Health, Washington,
District of Columbia; andbGeorgetown University School of
Medicine, Washington District of Columbia
KEY WORDS
adolescent, transition to adult care, population health, patient experience, cost of care, evaluation, quality improvement
ABBREVIATIONS
AHRQ—Agency for Health Care Research and Quality DM—diabetes mellitus
HbA1C—hemoglobin A1C
IHI—Institute for Health Care Improvement
Ms Prior developed the review protocol, completed the data collection, carried out the initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript; Ms McManus conceptualized the study, resolved data collection discrepancies, reviewed the initial analyses, and revised the manuscript; Dr White resolved data collection discrepancies and revised the manuscript; Ms Davidson developed the review protocol, designed the search strategy, drafted the literature review methods, and reviewed thefinal manuscript; and all authors approved thefinal manuscript as submitted and agree to be accountable for all aspects of the work.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-1704
doi:10.1542/peds.2014-1704
Accepted for publication Sep 24, 2014
Address correspondence to Megan Prior, BA, The National Alliance to Advance Adolescent Health, 1015 18th St, NW, Ste 300, Washington, DC 20036. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:This study was supported by cooperative agreement U39MC25729 HRSA/MCHB (“Transition Services in Adolescent Health—Healthy and Ready to Work”). The authors of this article are responsible for its contents. No statement in this article should be construed as the official position of the Health Resources and Services Administration or the Maternal and Child Health Bureau.
Movement from the pediatric to the adult health care system is a facet of every youth’s transition to independence. While learning to manage their own medical care, many adolescents also must change providers. Decline in health over this period is pervasive: increasing obesity,1sickle cell disease complications,2
and renal transplant loss3are among the
many documented poor health outcomes encountered during the transition to young adulthood. These outcomes are often the result of preventable lapses in adherence,4 follow-up,5 and insurance
coverage.6
Preventing adverse outcomes during transition requires support, especially for youth with special health care needs. In 2011, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians jointly developed a report on transition that includes a set of specific clinical activities recom-mended for all youth beginning at age 127; yet, national data reveal that most
youth do not receive needed transition services.8
A variety of interventions have been used to improve health care transition support, but the evaluation of these interventions is limited. The Agency for Healthcare Research and Quality (AHRQ) recently noted that it is difficult to de-termine which transition interventions are most effective because of their limited evidence base.9Yet, there is an
ever-increasing demand to demon-strate impact. Demonstrating the im-pact of transition interventions requires a comprehensive measurement strategy with an underlying framework.
One such framework is the“Triple Aim,” a conceptual model that has been used to determine the impact of the medical home10 and to guide the redesign of
pediatric practice.11Developed by the
Institute for Health Care Improvement (IHI), the Triple Aim is organized around 3 interdependent goals: (1) improve
the individual experience of health care, (2) improve the health of pop-ulations, and (3) reduce the per capita costs of care.12Starting in 2011 with
the enactment of the Affordable Care Act, the Department of Health and Hu-man Services published its National Strategy for Quality Improvement in Health Care by using the Triple Aim to guide development and measurement across the department.13 Framing
transition measurement in terms of these 3 linked goals aligns transition interventions with system-wide improve-ments in health care.
To elucidate the current state of tran-sition measurement, this systematic review identified published measures used to evaluate transition. These measures are categorized within the Triple Aim framework. By understanding how transition interventions have mea-sured their impact on experience of care, population health, and cost, a more unified approach for evaluating health care transition interventions can be developed.
METHODS
Literature Search
Ovid Medline and the Cumulative Index to Nursing and Allied Health Literature databases were searched to identify English-language articles with abstracts published between January 1995 and November 2013. The search used a combination of medical subject head-ings and keywords. Search terms were divided into 3 groups: population (eg, adolescent), transition (eg, transition to adult care), and study design (eg, evaluation study). The Boolean phrase
“AND”was used between groups and the phrase“OR”was used within groups. The full Medline search strategy is available (Supplemental Table 4). In addition, ref-erence lists of relevant review articles were scanned for applicable studies. All results were compiled and duplicates were removed.
Inclusion and Exclusion Criteria Several criteria had to be met to be included in this systematic review (Supplemental Table 5). Studies that met inclusion criteria were limited to those describing an intervention for adolescents transferring from pediat-ric to adult outpatient health care. Studies aimed at patients with and without chronic conditions (physical, mental, and developmental) were in-cluded, whereas those looking at den-tistry were excluded. Studies that met inclusion criteria needed to evaluate preintervention and postintervention data or compare the intervention group with a comparison group. Both pro-spective and retropro-spective data were accepted. Studies that reported exclu-sively qualitative data or that did not include a sample size were excluded.
Study Selection
Titles and abstracts were screened by 1 reviewer. Only articles that described an outcome of a health care transition intervention were further reviewed. Two reviewers then read the full text of the selected articles and screened them using an inclusion criteria checklist (Supplemental Table 5). A third and fourth reviewer resolved disagreements.
Risk of Bias Assessment
Because the primary interest of this review was identifying measures and not evaluating outcomes, the quality of the articles was not formally assessed. Thus, measures used in a study with a small sample size were considered as important as measures used in a larger study.
Data Extraction
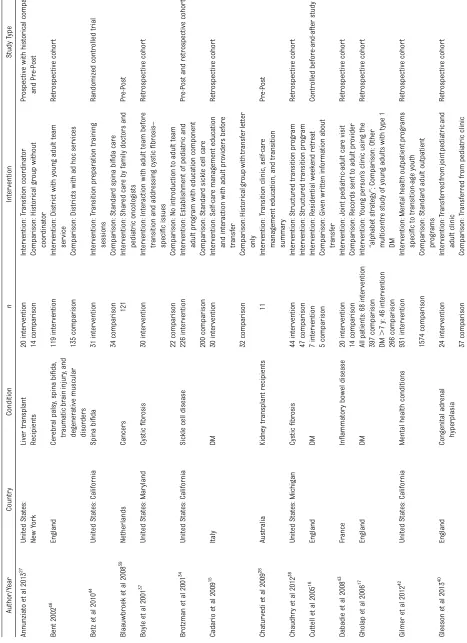
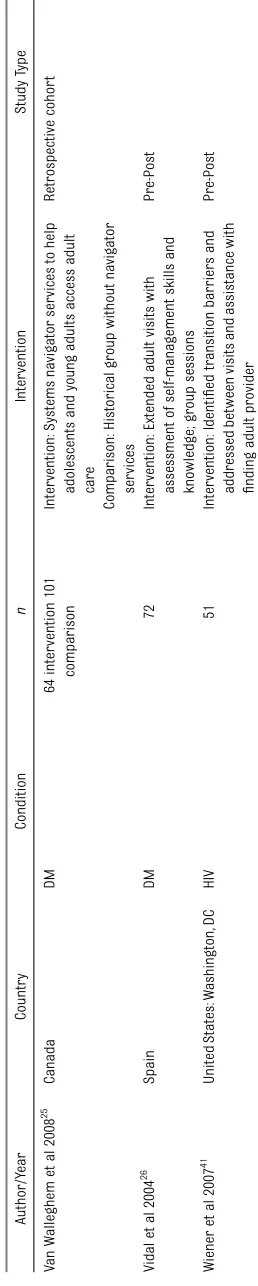
the number of subjects (n) were reported; nis defined as the number of partic-ipants for whom outcome data were obtained. Unless noted, n refers to youth or young adults. To add context to the measures, a brief description of the transition intervention and the study type also are reported (Table 1).
Data Synthesis and Analysis The transition measures in each article were then categorized according to the framework of the“Triple Aim.”To guide the categorization of transition mea-sures within the domains of experience, population health, and cost, IHI’s“Guide to Measuring the ‘Triple Aim,’”14 and
AHRQ’s“Early Evidence on the Patient-Centered Medical Home”10were used.
As shown in Fig 1, each measure was further categorized within the 3 Triple Aim domains consistent with IHI and AHRQ’s example measures. Experience of care measures were split into satis-faction and barriers to care. Population health measures were organized into adherence to care/guidelines, disease-specific outcomes, mortality, patient-reported outcomes (eg, quality of life, functional status), self-care skills, and process of care. Cost measures were classified according to service use, gaps in care (eg, missed appointments, time without a primary care provider), and cost per patient.
Measures or survey instruments de-veloped by study authors, as opposed to validated tools, are noted. Study results, noted as improvement or deterioration in the Triple Aim, also are summarized as reported by the authors of each article. When reporting on utilization, increased outpatient visits were reported as cost-effective and emergency visits and in-patient visits as not cost-effective.
RESULTS
Results of the Literature Search We identified 2282 articles and reviewed the full text of 104; 33 articles met
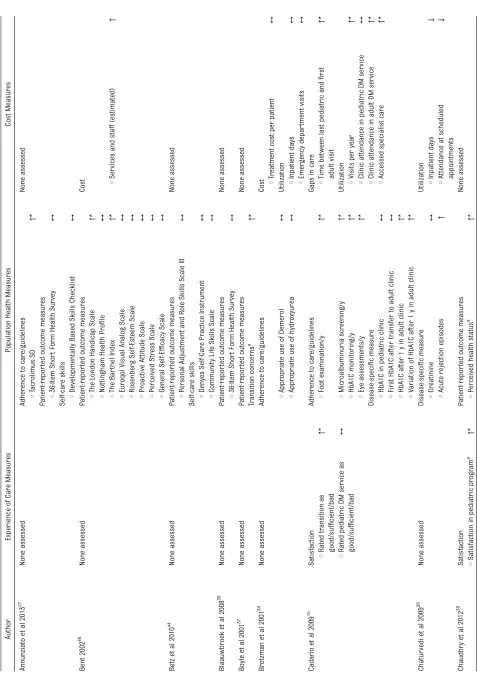
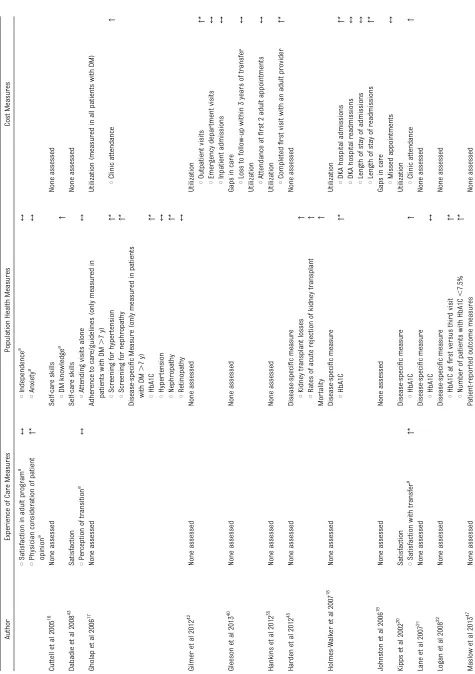
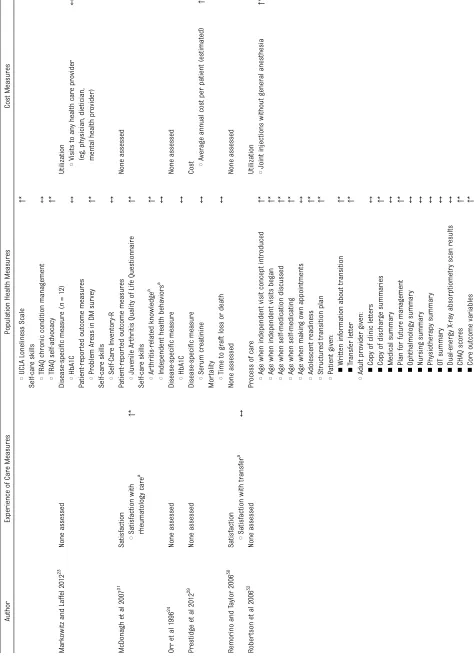
in-clusion criteria and were selected for the review (Fig 2). The characteristics of these articles are presented in Table 1. The transition evaluation measures, cate-gorized within the Triple Aim framework, are presented in Table 2.
Study Characteristics
The selected articles evaluated the impact of a variety of transition inter-ventions for youth with specific chronic conditions. Study designs were primarily pre-post or retrospective, and sample sizes were typically,100.
Study Populations
Thirteen studies were conducted in the United States and the remaining 18 studies took place in Canada, Europe, or Australia. All 33 studies examined transition in the context of a specific medical condition as opposed to ex-amining transition for all youth with or without chronic conditions. Twelve studies evaluated programs for patient with diabetes mellitus (DM),15–264 for
transplant recipients,27–30 3 each for
those with arthritis31–33and sickle cell
disease,34–362 for patients with cystic
fibrosis,37,38and 1 study each for those
with cancers,39congenital adrenal
hy-perplasia,40 HIV,41 mental health
con-ditions,42inflammatory bowel disease,43
spina bifida,44and kidney failure.45One
study looked at a combination of patients with traumatic brain injury, cerebral palsy, spina bifida, and degenerative muscular disorders.46No study included
youth with developmental disabilities, and only 1 examined the impact of the transition intervention on youth with a wide variety of chronic conditions.47
Although several studies reported qual-itative data or surveys from parents, only 1 study surveyed parents before and after the transition intervention.33
Study Design
Sample sizes ranged from 10 to 2502, with nearly a third of the studies en-rolling#20 in their intervention group.
Fourteen studies collected data before and after the intervention, but lacked a comparison group. Most studies with comparison groups used a retrospec-tive design. Only 1 study was a ran-domized controlled trial.44
Transition Interventions
Although this review does not focus on the specific components of transition interventions, a brief description of each study can be found in Table 1 to provide a context for the measures that were reviewed. Transition inter-ventions were diverse, and their study methodologies were reported on with varying levels of detail. Several inter-ventions consisted of 1 visit, whereas others took place over the course of multiple years. Staff involvement ranged from a single transition coordinator to joint meetings between pediatric and adult teams. Some studies focused on preparing adolescents to manage their own health care, whereas oth-ers sought to improve transfer to adult providers.
Health Care Transition Measures The measures used to evaluate health care transition interventions were widely variable. All domains of the Triple Aim were examined, although only 3 studies assessed all domains of the Triple Aim (Table 3).15,20,25
Population Health
Population health measures were used more than twice as frequently as the other 2 Triple Aim domains. In the 27 studies that included these measures, disease-specific outcomes, patient-reported outcomes, and self-care skills were examined most commonly. Measures that were used less frequently included adherence to care, mortality, and process of care.
was the disease-specific measure used most commonly.
Patient-reported health outcomes were measured in 12 studies, with quality of life measured most frequently in 5. All 5 of these studies used validated survey instruments. The 36-Item Short Form Health Survey, an instrument that measures social and physical func-tioning, pain, mental health, vitality, emotional and physical roles, and general perceived health was used in 2 studies.27,39The EuroQol, which measures
mobility, usual activities, pain/discomfort, and anxiety/depression, was used in 1 study.46 Validated disease-specific tools
for DM (Diabetes Quality of Life Ques-tionnaire) and arthritis (Juvenile Arthritis Quality of Life Questionnaire), which as-sess topics similar to the generic instru-ments but in a disease-specific manner, were used in 2 studies.26,31
Other patient-reported outcome mea-sures examined single topics associated with quality of life by using validated surveys. These included activities of daily living (Barthel Index46), stress
(Com-munity Life Skills Scale44and Perceived
Stress Scale46), loneliness (UCLA
Lone-liness Scale47), anxiety (State/Trait
Anx-iety Inventory41), psychosocial skills
(Personal Adjustment and Role Skills Scale,44 Proactive Attitude Scale,46 and
General Self-Efficacy Scale46), disability
(London Handicap Scale46), perceived
health status (Nottingham Health Pro-file46), and self-esteem (Rosenberg
Self-Esteem Scale46). Two additional
patient-reported outcome measures relied on disease-specific instruments that evaluated emotional distress caused by DM (Problem Areas in Di-abetes Questionnaire23) and
con-cerns in transitioning to adult sickle cell care (Sickle Cell Transfer Ques-tionnaire36).
The third most commonly used set of population health measures were those that evaluated self-care skills, used in 11 studies. Six of these studies used
validated instruments to evaluate changes in self-care abilities or knowledge. Of the validated instruments, several gauged a youth’s general understanding of medi-cal conditions, wellness, emergencies, medications, pharmacies, medical records, and insurance (eg, the Developmentally Based Skills Checklist,27 Denyes Self-Care
Practice Instrument,44 Transition
Readi-ness Assessment Questionnaire,47 and
Self-Care Inventory R23). As opposed
to assessing general self-care skills, 2 validated surveys asked disease-specific questions about sickle cell disease (Sickle Cell Disease Quiz36)
and DM (Diabetes Knowledge Question-naire 226).
Three other studies evaluated self-care skills by using project-specific surveys, rather than validated tools.16,31,41 One
survey asked about DM knowledge,16
another about general self-care skills and HIV-specific knowledge,41and the
third about self-medicating, independent visits, and arthritis knowledge.31The
remaining 3 studies that measured self-care skills did not use surveys but rather recorded patients’abilities to complete a task, such as attending a doctor visit alone,43carrying a
self-monitoring card,32or self-adjusting an
insulin dose.26
Adherence to care was measured in 4 studies. Three studies15,17,34examined
TABLE
1
Continued
Autho
r/Y
ear
Count
ry
Con
dition
n
Interv
ention
Stu
dy
Type
V
an
W
allegh
em
et
al
20
08
25
Canada
DM
64
int
ervention
101
compa
rison
Interv
ention:
Systems
na
vigato
r
services
to
help
adoles
cents
and
youn
g
adults
access
adult
car
e
Ret
rospecti
ve
cohor
t
Compa
rison:
Historica
l
gr
oup
withou
t
na
vigator
servic
es
Vid
al
et
al
2004
26
Spain
DM
72
Interv
ention:
Exten
ded
adult
visits
wit
h
asse
ssment
of
self-ma
nagem
ent
sk
ills
and
knowle
dge;
gr
oup
se
ssions
Pr
e-P
ost
Wien
er
et
al
2007
41
United
States:
W
ashingto
n,
DC
HIV
51
Interv
ention:
Ide
nti
fi
ed
tr
ansit
ion
barrier
s
and
add
resse
d
betwe
en
visits
and
assistanc
e
with
fi
nding
adult
pr
ovid
er
Pr
e-P
ost
FIGURE 1
receipt of recommended screenings or medications, and 1 study evaluated transplant recipients’ fluctuations in drug levels.27
Mortality was measured in 2 stud-ies,29,45 both of which evaluated the
impact of transition interventions on patients with kidney transplants.
Process of care measures were evalu-ated in only 1 study.32 This study
in-vestigated whether the intervention improved documentation of transition-related services in the medical chart, including the age when patients began having independent visits, receipt of a transfer letter by the family, and receipt of records by the future adult provider.
Experience of Care
Experience of care was evaluated in 8 of 33 studies, with almost all measuring
satisfaction with care.15,20,25,30–33,38,43
Barriers to care were measured in only 1 study.25
Of the 7 studies measuring patient satisfaction, 3 studies20,30,43 asked
specifically about transition services, whereas 3 studies31,33,38 asked about
satisfaction with care in general. One study asked about both areas.15 The
studies evaluating satisfaction with transition support most often assessed awareness of transfer policies, appro-priateness of transfer timing, and ex-tent of shared decision-making. Three studies assessed overall satisfaction with care. Two of these studies used the same survey instrument and evaluated practice management (eg, availability of appointments), provider character-istics, and clinical processes. This sur-vey also included a parent version,
which contained additional questions on availability of parent support. The third study assessing general satisfac-tion with care did not include the survey instrument in the published article.
The length and scope of survey instru-ments to measure satisfaction varied widely. Surveys were as simple as 1 question (asking the patient to rate transition as good, sufficient, or bad15)
and as complicated as a 22-item ques-tionnaire.31,33Each study conducted its
own project-specific survey as opposed to using an existing validated survey, and only 2 studies31,33 relied on the
same instrument, the Mind the Gap Scale, which has been subsequently validated for use in the juvenile idio-pathic arthritis population.49
Barriers to care were evaluated in only 1 study.25Patients were surveyed about
their difficulties finding providers, scheduling appointments, establishing relationships with an adult team, and feeling comfortable in a new health care system.
Cost
Cost measures, most often reported in terms of service utilization, were used in 15 of the 33 studies. Fewer studies examined gaps in care or per capita costs.
Thirteen studies measured the im-pact of transition interventions on service utilization, including primary care, hospital, emergency department, or other services (medication26 and
anesthesia32).
Gaps in care, defined as loss to follow-up over a specified period,25,40missed
appointments,19 and the time frame
between attendance in pediatric and adult clinics15 were evaluated in 4
studies.
Cost was evaluated in 3 studies. Two studies estimated the total costs of staff and services devoted to transition services,29,46whereas the third study34 FIGURE 2
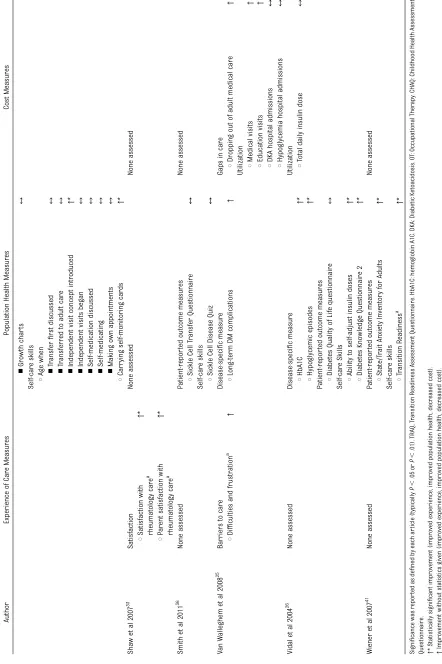
TABLE 2 Continued Autho r Experi ence of Car e Meas ur es P opu lation Health Measur es Cost Meas ur es n Gr owth char ts ↔ Self-car e sk ills s Age when n Tr ansfer fi rst discu ssed ↔ n Tr ansferr ed to adu lt ca re ↔ n Ind epend ent visi t concept intr oduced ↑ * n Ind epend ent visi ts began ↔ n Sel f-medication discu ssed ↔ n Sel f-medicating ↔ n Ma king own app ointm ents ↔ s Carr ying self-mo nitorin g car ds ↑ * Sha w et al 2007 33 Satisfact ion None as sessed Non e assess ed s Satis faction wit h rhe umatolog y car e a ↑ * s P ar ent satisfa ction with rhe umatolog y car e a ↑ * Smi th et al 20 11 36 None as sessed P atien t-r epo r te d outcome me asur es Non e assess ed s Sic kle Cel l Tr ansfe r Quest ionnai re ↔ Self-car e sk ills s Sic kle Cel l Dis ease Quiz ↔ V an W allegh em et al 20 08 25 Barriers to c a re Disease-speci fi c me asur e Gap s in car e s Dif fi cul ties and frustr ation a ↑ s Long-term DM complica tions ↑ s Dr opp ing out of adult me dical car e ↑ Utiliza tion s Medical visi ts ↑ s Educati on visits ↑ s DKA hospital adm issions ↔ s Hypoglycemia hospit al admissio ns ↔ Vid al et al 2004 26 None as sessed Disease-speci fi c me asur e Utiliza tion s HbA 1C ↑ * s Total daily ins ulin dos e ↔ s Hypo glycem ic epi sodes ↑ * P atien t-r epo r te d outcome me asur es s Diab etes Qualit y of Life que stionnai re ↔ Self-car e Ski lls s Abi lity to se lf-adjust insulin doses ↑ * s Diab etes Knowle dge Que stionnai re 2 ↑ * Wien er et al 2007 41 None as sessed P atien t-r epo r te d outcome me asur es Non e assess ed s Sta te/T rait Anxi ety Inventory fo r Adults ↑ * Self-car e sk ills s Tr ansition Readin ess a ↑ * Signi fi cance was repor ted as de fi ned by each ar ticle (typically P , .05 or P , .01). TRAQ, Tr ansition Readiness Assessment Questionnaire. HbA1C: hemoglobin A1C. D KA: Diabetic K etoacidosis. O T: Occupational Ther ap y. CHAQ: C hildhood Health Assessment
Questionnaire. ↑*
measured cost per capita for those with and without transition support.
DISCUSSION
This systematic review reveals that transition intervention studies mea-sure impact with little consistency and without a common measurement framework to comparatively judge transition outcomes. The Triple Aim provides an explicit conceptual model. However, most studies examine only 1 domain of the Triple Aim and are seldom using the same measure. Moreover, except for those evaluating quality of life and self-care skills, few instruments have been validated. The transitionfield of research is in its early stages of de-velopment, and new efforts are needed to establish a consensus on a core set of measures aligned with the Triple Aim framework.
When establishing transition measures, 2 considerations are important. Evaluation strategies should include measures that are, first, applicable to all youth, and, second, reasonably attributable to tran-sition interventions. The American Acad-emy of Pediatrics/American AcadAcad-emy of Family Physicians/American College of Physicians Clinical Report7 emphasizes
the importance of transition services for all adolescents, not just those with special health care needs. It is therefore impor-tant to establish a core set of measures that can be used to assess youth with and without chronic conditions. Although disease-specific measures may be of value, they cannot be used for compar-ison across diverse populations. Fur-ther, several measures identified by this
review pertain to care in general, as opposed to transition specifically. Qual-ity of life or satisfaction may be more appropriate to evaluate overall health care quality rather than the impact of a transition intervention. Measures that meet these 2 criteria (applicable to all youth and attributable to transition) are discussed later in this article, with recognition that they may be best used in conjunction with other measures tailored to specific diseases or research questions.
Population health evaluation strategies applicable to all youth and attributable to transition include self-care manage-ment and process of care measures. Several validated self-care assessment tools, such as the Transition Readiness Assessment Questionnaire (TRAQ)50and
the TRxANSITION Scale,51assess a wide
array of skills relevant to youth with and without chronic conditions. Process-of-care measures also can be used to evaluate transition interventions tar-geted at a broad population. The paucity of process measures found in this sys-tematic review is likely because many studies were published before the re-lease of the transition recommendations specified in the 2011 Clinical Report.7The
necessary components of transition de-lineated in this report were further translated into clinical tools referred to as the Six Core Elements, which include a transition policy, a method of tracking patients, a self-care assessment, a tran-sition plan, a transfer protocol, and a method to elicit consumer feedback.52
A newly developed process measure, the Health Care Transition Process
Mea-surement Tool, is available to monitor the implementation of these elements and can be used to evaluate the receipt of transition services by all youth.52This tool
has yet to be validated.
With respect to experience of care, several surveys are transition-specific. The 2009–2010 National Survey of Children with Special Health Care Needs asked parents 4 questions about receipt of transition assistance8;
how-ever, it is currently undergoing signifi -cant revisions. In addition, AHRQ has funded Boston Children’s Hospital to develop and test an adolescent self-reported quality measure. Finally, as part of the updated Six Core Elements, consumer transition feedback surveys were developed for use with youth, parents/caregivers, and young adults, although these instruments have not yet been validated.52
Cost indicators also can be specific to transition while remaining applicable to all youth. One such indicator is the use of primary care services by young adult patients. By measuring utilization longitudinally, researchers can corre-late transition processes with eventual cost outcomes into adulthood.
Achieving consensus on a core set of transition measures will require a careful, concerted effort involving clin-ical, consumer, and research expertise. To facilitate this process, AHRQ has de-fined specific attributes important for quality measurement.53 These include
importance of the measure, clinical logic, measure properties, and feasi-bility. Critical examination of each of these attributes will be important in developing a consensus. Several cur-rent efforts are noteworthy. AHRQ has commissioned a technical brief to de-scribe current transition practice and outcomes to provide a framework for future research.9 Additionally, The
Healthcare Transition Research Con-sortium has initiated a Delphi pro-cess with consumers and providers
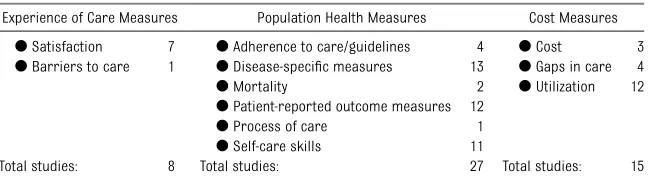
TABLE 3 Summary of Transition Intervention Measures
Experience of Care Measures Population Health Measures Cost Measures
dSatisfaction 7 dAdherence to care/guidelines 4 dCost 3
dBarriers to care 1 dDisease-specific measures 13 dGaps in care 4
dMortality 2 dUtilization 12
dPatient-reported outcome measures 12
dProcess of care 1
dSelf-care skills 11
to elicit potential health care transition measures.54
Once a core set of transition measures has been developed, sharing these with clinicians and researchers is essential. Practice-based research networks are a proven method for evaluating im-provement in primary care.55
Expand-ing fundExpand-ing support for transition research networks will allow mea-surement strategies to be imple-mented and tested among a broader group of youth. Building on the in-vestment in evaluation that the federal government, private foundations, and
health plans have made in the areas of medical home and transition from hos-pital to community-based settings, the field of pediatric to adult health care transition could benefit from similar leadership and support.
CONCLUSIONS
Health care transition evaluations as-sess Triple Aim impacts, but do so with little consistency. Seldom do transition interventions measure all 3 domains of the Triple Aim. A unified approach for evaluating health care transition should include broadly applicable measures
that evaluate patient and family experi-ence, population health, and cost. By evaluating the Triple Aim, successful health care transition interventions can be identified and implemented to benefit all youth.
ACKNOWLEDGMENTS
The authors are grateful to Katherine Rogers for her assistance reviewing methods and Daniel Beck for his assis-tance screening abstracts and revising the manuscript. We are also apprecia-tive of the support of our project officer Marie Mann.
REFERENCES
1. Lee H, Lee D, Guo G, Harris KM. Trends in body mass index in adolescence and young adulthood in the united states: 1959.J Adolesc
Health. 2011;49(6):601–608
2. Blinder MA, Vekeman F, Sasane M, Trahey A, Paley C, Duh MS. Age-related treatment patterns in sickle cell disease patients and the associated sickle cell complications and healthcare costs. Pediatr Blood
Can-cer. 2013;60(5):828–835
3. Andreoni KA, Forbes R, Andreoni RM, Phillips G, Stewart H, Ferris M. Age-related kidney
transplant outcomes: health disparities amplified in adolescence.JAMA Intern Med. 2013;173(16):1524–1532
4. Annunziato RA, Emre S, Shneider B, Barton C, Dugan CA, Shemesh E. Adherence and medical outcomes in pediatric liver trans-plant recipients who transition to adult services. Pediatr Transplant. 2007;11(6):
608–614
5. Devernay M, Ecosse E, Coste J, Carel JC. Determinants of medical care for young women with turner syndrome. J Clin
Endocrinol Metab. 2009;94(9):3408–3413
6. Goudie A, Carle AC. Ohio study shows that insurance coverage is critical for children with special health care needs as they tran-sition to adulthood. Health Aff (Millwood).
2011;30(12):2382–2390
7. Cooley WC, Sagerman PJ; American
Acad-emy of Pediatrics; American AcadAcad-emy of Family Physicians; American College of Physicians; Transitions Clinical Report Authoring Group. Supporting the health care transition from adolescence to adult-hood in the medical home.Pediatrics. 2011;
128(1):182–200
8. McManus MA, Pollack LR, Cooley WC, et al. Current status of transition preparation among youth with special needs in the united states. Pediatrics. 2013;131(6): 1090–1097
9. Agency for Healthcare Research and Quality. Evidence-based Practice Center Technical Brief Protocol: Transitions of Care for Children with Special Health Care Needs. Rockville, MD: AHRQ; Oct 2013
10. Peikes D, Zutshi A, Genevro J, Smith K, Parchman M, Meyers D. Early Evidence on the Patient-Centered Medical Home. Princeton, NJ: Mathematica Policy Research Feb 2012
11. Schor EL. Reshaping pediatric practice.
Pediatrics. 2013;131(2):201–203
12. Berwick DM, Nolan TW, Whittington J. The triple aim: care, health, and cost.Health Aff
(Millwood). 2008;27(3):759–769
13. US Department of Health and Human Services. Report to Congress: National Strategy for Quality Improvement in Health Care. Rockville MD: AHRQ; March 2011
14. Stiefel M, Nolan K. A Guide to Measuring the Triple Aim: Population Health, Experience of Care, and Per Capita Cost. IHI Innovation Series White Paper. Cambridge, MA: In-stitute for Healthcare Improvement; 2012
15. Cadario F, Prodam F, Bellone S, et al. Transition process of patients with type 1 diabetes (T1DM) from paediatric to the adult health care service: a hospital-based
approach.Clin Endocrinol (Oxf). 2009;71(3): 346–350
16. Cuttell K, Hilton D, Drew J. Preparation for
transition to adult diabetes services.Paediatr
Nurs. 2005;17(2):28–30
17. Gholap N, Pillai M, Virmani S, et al. The alphabet strategy and standards of care in young adults with type 1 diabetes. Br
J Diabetes Vasc Dis. 2006;6(4):168–170
18. Holmes-Walker DJ, Llewellyn AC, Farrell K. A transition care programme which improves diabetes control and reduces hospital admission rates in young adults with type 1 diabetes aged 15–25 years.
Diabetic Med. 2007;24(7):764–769
19. Johnston P, Bell P, Tennet H, Carson D. Audit of young people with type 1 diabetes transferring from paediatric to adult di-abetic services.Pract Diabetes Int. 2006;23 (3):106–108
20. Kipps S, Bahu T, Ong K, et al. Current methods of transfer of young people with type 1 diabetes to adult services.Diabetic
Med. 2002;19(8):649–654
21. Lane JT, Ferguson A, Hall J, et al. Glycemic control over 3 years in a young adult clinic for patients with type 1 diabetes.Diabetes
Res Clin Pract. 2007;78(3):385–391
22. Logan J, Peralta E, Brown K, Moffett M, Advani A, Leech N. Smoothing the transition from paediatric to adult services in type 1 diabetes.J Diabetes Nurs. 2008;12:328–338
23. Markowitz JT, Laffel LM. Transitions in care: support group for young adults with type 1 diabetes.Diabet Med. 2012;29(4):522–525
24. Orr DP, Fineberg NS, Gray DL. Glycemic control and transfer of health care among adolescents with insulin dependent
di-abetes mellitus.J Adolesc Health. 1996;18 (1):44–47
25. Van Walleghem N, Macdonald CA, Dean HJ.
for young adults with type 1 diabetes.Diabetes
Care. 2008;31(8):1529–1530
26. Vidal M, Jansa M, Anguita C, et al. Impact of a special therapeutic education pro-gramme in patients transferred from a paediatric to an adult diabetes unit.
Eu-ropean Diabetes Nursing. 2004;1(1):23–27
27. Annunziato RA, Baisley MC, Arrato N, et al. Strangers headed to a strange land? A pilot study of using a transition coordinator to improve transfer from pediatric to adult services.J Pediatr. 2013;163(6):1628–1633
28. Chaturvedi S, Jones CL, Walker RG, Sawyer SM. The transition of kidney transplant recipients: a work in progress. Pediatr
Nephrol. 2009;24(5):1055–1060
29. Prestidge C, Romann A, Djurdjev O, Matsuda-Abedini M. Utility and cost of a renal transplant transition clinic.Pediatr
Nephrol. 2012;27(2):295–302
30. Remorino R, Taylor J. Smoothing things over: The transition from pediatric to adult care for kidney transplant recipients.Prog
Transplant. 2006;16(4):303–308
31. McDonagh JE, Southwood TR, Shaw KL, British Society of Paediatric and Adolescent Rheumatology. The impact of a coordinated transitional care programme on adoles-cents with juvenile idiopathic arthritis.
Rheumatology. 2007;46(1):161–168
32. Robertson LP, McDonagh JE, Southwood TR, Shaw KL, British Society of Paediatric and Adolescent Rheumatology. Growing up and moving on. A multicentre UK audit of the transfer of adolescents with juvenile idio-pathic arthritis from paediatric to adult cen-tred care.Ann Rheum Dis. 2006;65(1):74–80
33. Shaw KL, Southwood TR, McDonagh JE, British Society of Paediatric and Adolescent Rheumatology. Young people’s satisfaction of transitional care in adolescent rheuma-tology in the UK. Child Care Health Dev. 2007;33(4):368–379
34. Brotzman AJ, Blake OA, Myers ML, et al. Vohs award winner: Southern California West Los Angeles Sickle Cell Medical Care Program. The Permanente Journal. 2001; 5(2):12–18
35. Hankins JS, Osarogiagbon R, Adams-Graves P, et al. A transition pilot program for adoles-cents with sickle cell disease.J Pediatr Health
Care. 2012;26(6):e45–e49
36. Smith GM, Lewis VR, Whitworth E, Gold DT, Thornburg CD. Growing up with sickle cell disease: a pilot study of a transition pro-gram for adolescents with sickle cell dis-ease.J Pediatr Hematol Oncol. 2011;33(5): 379–382
37. Boyle MP, Farukhi Z, Nosky ML. Strategies for improving transition to adult cysticfi -brosis care, based on patient and parent views.Pediatr Pulmonol. 2001;32(6):428–436
38. Chaudhry SR, Keaton M, Nasr SZ. Evaluation of a cysticfibrosis transition program from pediatric to adult care.Pediatr Pulmonol. 2013;48(7):658–665
39. Blaauwbroek R, Tuinier W, Meyboom-de Jong B, Kamps WA, Postma A. Shared care by paediatric oncologists and family doctors for long-term follow-up of adult childhood cancer survivors: a pilot study.
Lancet Oncol. 2008;9(3):232–238
40. Gleeson H, Davis J, Jones J, O’Shea E, Clayton PE. The challenge of delivering en-docrine care and successful transition to adult services in adolescents with con-genital adrenal hyperplasia: experience in a single centre over 18 years.Clin
Endo-crinol (Oxf). 2013;78(1):23–28
41. Wiener LS, Zobel M, Battles H, Ryder C. Transition from a pediatric HIV intramural clinical research program to adolescent and adult community-based care services: assessing transition readiness.Soc Work
Health Care. 2007;46(1):1–19
42. Gilmer TP, Ojeda VD, Fawley-King K, Larson B, Garcia P. Change in mental health ser-vice use after offering youth-specific versus adult programs to transition-age youths.
Psychiatr Serv. 2012;63(6):592–596.
43. Dabadie A, Troadec F, Heresbach D, Siproudhis L, Pagenault M, Bretagne JF. Transition of patients with inflammatory bowel dis-ease from pediatric to adult care.
Gas-troenterol Clin Biol. 2008;32(5 pt 1):451–
459
44. Betz CL, Smith K, Macias K. Testing the transition preparation training program: a randomized controlled trial.Intl J Child
Adolesc Health. 2010;3(4):595–607
45. Harden PN, Walsh G, Bandler N, et al. Bridging the gap: an integrated paediatric to adult clinical service for young adults with kidney failure.BMJ. 2012;344:e3718
46. Bent N, Tennant A, Swift T, Posnett J, Scuffham P, Chamberlain MA. Team approach versus ad hoc health services for young people with physical disabilities: a retrospective cohort study.Lancet. 2002;360(9342):1280–1286
47. Maslow G, Adams C, Willis M, et al. An evalu-ation of a positive youth development program for adolescents with chronic illness.J Adolesc
Health. 2013;52(2):179–185
48. Wiener LS, Kohrt BA, Battles HB, Pao M. The HIV experience: youth identified bar-riers for transitioning from pediatric to adult care.J Pediatr Psychol. 2011;36(2): 141–154
49. Shaw KL, Southwood TR, McDonagh JE, British Society of Paediatric and Adolescent Rheumatology. Development and pre-liminary validation of the ’mind the gap’ scale to assess satisfaction with transi-tional health care among adolescents with juvenile idiopathic arthritis. Child Care
Health Dev. 2007;33(4):380–388
50. Sawicki GS, Lukens-Bull K, Yin X, et al. Measuring the transition readiness of youth with special healthcare needs: vali-dation of the TRAQ–transition readiness assessment questionnaire. J Pediatr
Psy-chol. 2011;36(2):160–171
51. Ferris ME, Harward DH, Bickford K, et al. A clinical tool to measure the components of health-care transition from pediatric care to adult care: the UNC TR(x)ANSITION scale.
Ren Fail. 2012;34(6):744–753
52. National Alliance to Advance Adolescent Health. Got transition: Center for Health Care Transition Improvement. Available at: www.GotTransition.org. Accessed May 16, 2014
53. National Quality Measures Clearinghouse. Tutorials on quality measures: desirable attributes of a quality measure. Available at: www.qualitymeasures.ahrq.gov/tutorial/ attributes.aspx. Accessed June 3, 2014
54. Healthcare Transition Research Consor-tium. Annual spring meetings: Special In-terest Group on Health Care Transition. Available at: https://sites.google.com/site/ healthcaretransition/. Accessed June 3, 2014
DOI: 10.1542/peds.2014-1704 originally published online November 24, 2014;
2014;134;e1648
Pediatrics
Megan Prior, Margaret McManus, Patience White and Laurie Davidson
Measuring the ''Triple Aim'' in Transition Care: A Systematic Review
Services
Updated Information &
http://pediatrics.aappublications.org/content/134/6/e1648
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/134/6/e1648#BIBL
This article cites 13 articles, 3 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/transition_adult_care_
Transition to Adult Care
dicine_sub
http://www.aappublications.org/cgi/collection/adolescent_health:me
Adolescent Health/Medicine
sub
http://www.aappublications.org/cgi/collection/quality_improvement_
Quality Improvement
e_management_sub
http://www.aappublications.org/cgi/collection/administration:practic
Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2014-1704 originally published online November 24, 2014;
2014;134;e1648
Pediatrics
http://pediatrics.aappublications.org/content/134/6/e1648
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2014/11/19/peds.2014-1704.DCSupplemental
Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.