ARTICLE
Psychological Differences Between Children With and
Without Soiling Problems
Carol Joinson, PhDa, Jon Heron, PhDa, Ursula Butler, MRCPCHb, Alexander von Gontard, MDc, the Avon Longitudinal Study of Parents and Children Study Team
aDepartment of Community Based Medicine, Unit of Perinatal and Paediatric Epidemiology, University of Bristol, Bristol, United Kingdom;bSheffield Children’s Trust, Sheffield, United Kingdom;cDepartment of Child and Adolescent Psychiatry, Saarland University Hospital, Homburg, Germany
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVES.Previous studies, based on clinic samples, report that childhood soiling is
associated with behavior problems and reduced self-esteem. This population-based study investigates the prevalence of psychological problems associated with child-hood soiling.
METHODS.A total of 8242 children aged 7– 8 years born to mothers in the United
Kingdom– based Avon Longitudinal Study of Parents and Children were studied. Parents completed postal questionnaires assessing common childhood emotional and behavioral problems, and children were asked questions at a research clinic concerning their behavior, friendships, bullying, and self-esteem. The rate of psychological problems was compared in children who soil frequently (once a week or more), those who soil occasionally (less than once a week), and those with no soiling problems (controls). Analyses were adjusted for developmental delay, gender, sociodemographic background, and stressful life events.
RESULTS.Children who soil were reported by their parents to have significantly more
emotional and behavioral problems compared with children who do not soil. Children who soil frequently had significantly more problems than those who soil occasionally. The rate of attention and activity problems, obsessions and compul-sions, and oppositional behavior was particularly high in frequently soiling chil-dren. Children with soiling problems reported significantly higher rates of involve-ment in overt bullying (as both perpetrator and victim) and antisocial activities compared with controls.
CONCLUSIONS.The current study finds significantly higher rates of behavior and
emotional problems, bullying, and antisocial activities in children who soil com-pared with those who do not soil. Children who soil frequently are more likely to have these problems than those who soil occasionally.
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-1773
doi:10.1542/peds.2005-1773
Key Words
child behavior, incontinence, encopresis, constipation, psychological impact
Abbreviations
DSM-IV—Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition
ALSPAC—Avon Longitudinal Study of Parents and Children
DAWBA—Development and Well-Being Assessment
SPPC—Self-Perception Profile for Children WISC-III—Wechsler Intelligence Scale for Children III
SEN—special educational needs
Accepted for publication Oct 21, 2005 Address correspondence to Carol Joinson, PhD, Avon Longitudinal Study of Parents and Children, Department of Community Based Medicine, Unit of Perinatal and Paediatric Epidemiology, 24 Tyndall Ave, Bristol BS8 1TQ, United Kingdom. E-mail: carol.joinson@bristol. ac.uk
S
OILING IS Acommon childhood problem presenting to pediatric, psychiatric, and psychological settings and has a significant impact on children’s social and emotional functioning and on the family.1,2Constipationis the underlying cause of soiling in⬃80% of children.3,4
Currently, theDiagnostic and Statistical Manual for Mental Disorders, Fourth Edition(DSM-IV)5uses the term
enco-presis to describe fecal soiling, defining it as the repeated passage of feces in inappropriate places, with a frequency of at least once a month for 3 months in children aged
ⱖ4 years and in the absence of a physical cause.
How-ever, this definition has not been universally adopted, leading to wide variation in the reported prevalence figures for soiling (4.1% of children aged 5– 6 years and
1.6% of children aged 11–12 years6; 1.5–7.5% of
chil-dren aged 6 –12 years7; and 2.4% of boys and 0.7% of
girls aged 7 years8).
Psychological factors have often been implicated in the development of soiling. An early study reported that children who soil are more anxiety prone, less self-assured, less tolerant of demands, and less able to control
aggression compared with control children.9 A recent
population-based study reported that psychosocial prob-lems were far more common among children who soil
than among controls.6The majority of studies, based on
clinic samples, report an increased rate of behavior
prob-lems in children who soil compared with controls.10–16
Two studies report that the overall severity of behavior problems in children who soil is below that found in
children referred to clinics for behavior problems.2,17
Self-esteem levels have also been investigated, with 2 studies reporting reduced self-esteem in children who
soil compared with controls,18,19whereas another found
no difference between soiling and nonsoiling children.14
Overall, the results of previous studies provide evi-dence for an association between soiling and psycholog-ical problems (mostly behavior problems and reduced self-esteem). However, the generalizability of the find-ings is limited, because all but 16of the studies are based
on relatively small clinic samples, and some do not in-clude a suitable comparison group of children without soiling problems (or include only a small control group). Another limitation is that most of the findings of previ-ous studies are based on parental reports of psychologi-cal problems in their children. Only 3 studies have included reports from children (on self-esteem lev-els),14,18,19but there are no studies asking children about
problems with behavior, friendships, and bullying.
The present study, based on a population of ⬎8000
children, is an investigation of the psychological prob-lems associated with soiling in children aged⬃7.5 years. Based on reports from parents and children, the study compares the rate of problems with emotions, behavior, self-esteem, bullying, and friendships in children who soil compared with children who do not soil.
METHODS
Participants
The Avon Longitudinal Study of Parents and Children
(ALSPAC)20is an ongoing population-based study
inves-tigating a wide range of environmental and other influ-ences on the health and development of children. Preg-nant women resident in the former Avon Health Authority in southwest England with an estimated date of delivery between April 1, 1991, and December 31, 1992, were invited to take part, resulting in a cohort of 14 541 pregnancies and 13 971 children alive at 12 months of age. The primary source of data collection was via self-completion questionnaires administered at 4 points during the antenatal period, then at regular in-tervals after birth. More detailed information on the ALSPAC study is available on the Web site www.alspac. bris.ac.uk. The representative nature of the ALSPAC sample has been investigated by comparison with the
1991 National Census data of mothers with infants⬍1
year of age who were residents in the county of Avon. The ALSPAC sample had a slightly greater proportion of mothers who were married or cohabiting, who were owner-occupiers, and who had a car in the household. The study had a smaller proportion of ethnic minority mothers. Ethical approval for the study was obtained from the ALSPAC ethics committee and the local ethics committees of United Bristol, Southmead, and Frenchay Health Care Trusts.
Measures
Parents (or Main Carer)
A self-report questionnaire, administered when children
were⬃91 months of age, contained questions
concern-ing how often the child usually soils durconcern-ing the day, with the following options: (1) never; (2) less than once a week; (3) approximately once a week; (4) 2 to 5 times a week; (5) nearly every day; and (6) more than once a day. Children who soiled were split into 2 groups: “fre-quent” (ie, those who soiled once a week or more) and “occasional” (ie, those who soiled less than once a week). Also included in the 91-month questionnaire was the Development and Well-Being Assessment
(DAWBA),21composed of questions relating to a number
of common emotional and behavioral disorders in chil-dren occurring in the present and recent past.
Child
Children were invited to attend a clinic in which they were interviewed using the following schedules: (1) a modified version of the Bullying and Friendship
Inter-view Schedule22indicating whether or not the child had
Children Questionnaire23; (3) a reduced (12 item)
ver-sion of Harter’s Self-Perception Profile for Children (SPPC)24composed of global self-worth (items 2, 4, 6, 8,
10, and 12) and scholastic competence subscales (items 1, 3, 5, 7, 9, and 11); and (4) 5 questions from the Cambridge Hormones and Moods Project Friendship
Questionnaire25 to rate children’s happiness with their
friendships. Because of the sensitive nature of some of the questions, children were required to post their re-sponse in either a “yes” or “no” box. The interviewer could not see which box was chosen, and stressed that all of the answers would be confidential. Scores on the SPPC and the Friendship Questionnaire are continuous, but to aid comparison with the rest of the analyses, they were dichotomized so that children with the lowest scores on the SPPC (lowest self-esteem) and those with the highest scores on the Friendship Questionnaire (least happy with friendships) were in the top quartile.
Analysis
A 2 test was used to compare the rate of DSM-IV
psychiatric disorders derived from the DAWBA in chil-dren who soil (frequently or occasionally) and in a con-trol group composed of children with no daytime soiling problems. The small numbers of children meeting DSM-IV criteria for psychiatric disorders in the ALSPAC study population (see Appendix 1) precluded a multiva-riable regression analysis. Because of the low rate of DSM-IV disorders in the current study, additional anal-yses were conducted using a set of dichotomous out-come variables derived from the lists of symptoms in the DAWBA relating to each psychiatric disorder. This per-mitted a more rigorous multivariable analysis of the association of soiling with emotional and behavior prob-lems with adjustments for confounding variables. A scription of how all of the outcome variables were de-rived from the lists of symptoms in the DAWBA, their prevalence in the study population, and the prevalence of the child-reported problems are provided in Appen-dices 1 and 2.
The rate of problems reported in the clinic-based in-terviews of the children was also compared in the soiling and nonsoiling groups, and the analyses were adjusted for the effect of confounding variables, including devel-opmental delay (Wechsler Intelligence Scale for
Chil-dren III [WISC-III] IQ ⬍ 7026 or statement of special
educational needs), gender, stressful life events, and family sociodemographic background (home ownership status, car ownership, crowding, mother’s education, mother’s age, parity, and marital status, mainly derived from questionnaires administered during the antenatal period).
In the multivariable models, missing data on
con-founding variables resulted in a loss of ⬃10% of the
sample when the fully adjusted models were derived. To correct for any bias in the final adjusted estimates
be-cause of dropout, a missing data imputation technique
was used (missing imputation for chained equations27
using the procedure in Stata (Stata Corp, College Sta-tion, TX) known as “ice.”28Imputation was restricted to
confounding variables (no imputation of the outcome or the soiling exposure variable was performed).
RESULTS
The questionnaire was sent to 11 021 families, and 8242 questionnaires were returned (in 98% of cases, the re-spondent was the mother of the study child). The rate of responding to this questionnaire did not seem to be related to soiling. Reports of soiling in a previous ques-tionnaire given at 78 months were not related to the rate of response to the current questionnaire (of those soiling at 78 months, 86.2% returned the 91-month question-naire compared with 86.3% of those who were not soiling).
There were 117 (1.4%) children who soiled in the day once a week or more (81 males, 36 females; age range: 91–105 months; median: 91 months). Another 448 (5.4%) children soiled in the day less than once a week (287 males, 161 females; age range: 91–108 months; median: 91 months). The control group con-sisted of 7673 children with no soiling problems (3868 males, 3805 females; age range: 90 –111 months; me-dian: 91 months). Males comprised significantly more of
the group that had soiling problems (2 ⫽ 46.65;P ⬍
.001).
Of the original cohort, 6162 with information on level of soiling attended the 8-year clinic for the child assess-ment including 5741 (74.8%) of the children with no soiling problems, 340 (75.9%) of those with occasional soiling problems, and 81 (69.2%) of those with frequent soiling problems. There is no evidence to suggest a dif-ference in clinic attendance within the soiling group (2
⫽2.21;P⫽.331).
There were 276 children who were classified as hav-ing developmental delay, either by havhav-ing a WISC-III IQ
⬍ 70 or by having been issued with a statement of
special educational needs (SEN). WISC-III IQ was as-sessed in the 8-year clinic, and a full measure was only available for 5542 of the 8242 children in the study sample, and so the statement of SEN was used as proxy to highlight children without a WISC-III measurement. For the children with both indicators, children with an SEN were, on average, 21 points lower in WISC-III IQ, suggesting that SEN is a suitable proxy for developmen-tal delay in this sample. Of the children who soil fre-quently, 24 (20.5%) fit the criteria for developmental delay compared with 31 (6.9%) of children who soil occasionally and 221 (2.9%) of the children with no soiling problems (2⫽129.3;P⬍.001).
Table 1 shows the results of the2tests comparing the
occasion-ally) compared with those with no soiling problems. Many of the cells were sparse, and, hence, little can be concluded with any confidence from these figures. Table 2 shows the rate of emotional and behavioral problems reported by parents (from the symptom-based dichoto-mous outcome variables derived from the DAWBA) and child-reported problems (from the clinic-based assess-ments) in children who soil (frequently or occasionally) and in children with no soiling problems.
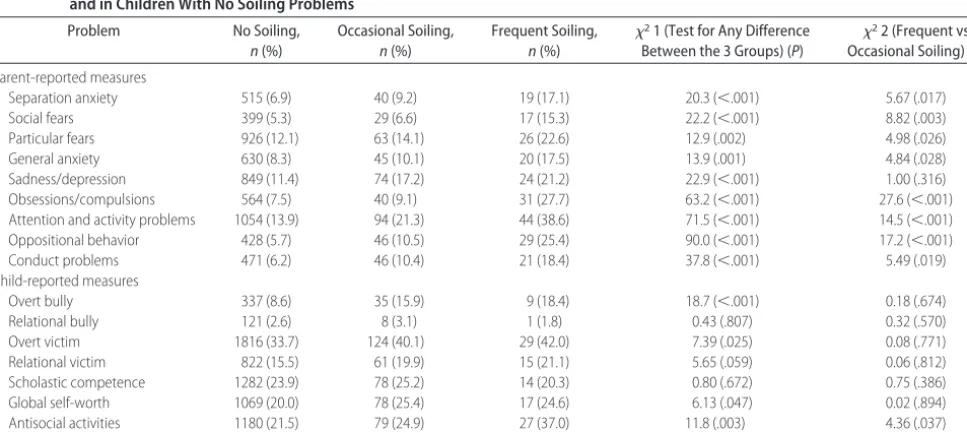
The results show a significantly higher rate of all of the parent-reported emotional and behavioral problems in children who soil compared with those who do not soil. There is also an effect of frequency of soiling, with children who soil frequently having significantly more problems than those who soil occasionally (with the exception of sadness/depression, where the slight in-crease for children who soil frequently is not signifi-cantly greater than that for children who soil occasion-ally). Significant differences in the child-reported
measures were also found, with higher rates of overt bullying (both bully and victim), low global self-worth (borderline significant), and antisocial activities (signifi-cantly higher in frequent compared with occasional soil-ing) in children who soil compared with controls.
Table 3 shows the odds ratios and 95% confidence intervals for the analyses with the parent-reported mea-sures derived from the DAWBA, as well as the results from the clinic-based assessment of the children. The unadjusted model indicates the odds ratios associated with each psychological problem for children who soil (frequent or occasional) compared with controls, with no adjustment for the effects of confounding variables. The other columns indicate the odds ratios after adjust-ing for developmental delay (adjusted 1) and then fur-ther adjusting for gender, sociodemographic back-ground, and stressful life events (adjusted 2).
The results from the unadjusted model (Table 3) show significantly higher odds of parent-reported psy-TABLE 1 Rates of DSM-IV Psychiatric Disorders in Children Who Soil Frequently (Once a Week or More)
or Occasionally (Less Than Once A Week) and in Children With No Soiling Problems
Disorder No Soiling,
n(%)
Occasional Soiling,
n(%)
Frequent Soiling,
n(%)
2(P)
Separation anxiety 58 (0.8) 6 (1.3) 5 (4.3) 18.6 (⬍.001)
Social phobia 20 (0.3) 0 (0) 2 (1.7) 10.3 (.006)
Specific phobia 73 (1.0) 9 (2.0) 5 (4.3) 16.2 (⬍.001)
Generalized anxiety disorder 34 (0.4) 3 (0.7) 4 (3.4) 20.8 (⬍.001)
Any depressive disorder 33 (0.4) 5 (1.1) 3 (2.6) 14.2 (.001)
Obsessive-compulsive disorder 9 (0.1) 1 (0.2) 0 (0) 0.534 (.766)
Any ADHD disorder 145 (1.9) 18 (4.0) 10 (9.2) 36.0 (⬍.001)
Oppositional-defiant disorder 142 (1.9) 14 (3.1) 13 (11.9) 56.6 (⬍.001)
Conduct disorder 42 (0.5) 3 (0.7) 2 (1.8) 3.19 (.203)
ADHD indicates attention-deficit/hyperactivity disorder.
TABLE 2 Rates of Psychological Problems in Children Who Soil Frequently (Once a Week or More) or Occasionally (Less Than Once A Week) and in Children With No Soiling Problems
Problem No Soiling,
n(%)
Occasional Soiling,
n(%)
Frequent Soiling,
n(%)
21 (Test for Any Difference
Between the 3 Groups) (P)
22 (Frequent vs
Occasional Soiling) (P)
Parent-reported measures
Separation anxiety 515 (6.9) 40 (9.2) 19 (17.1) 20.3 (⬍.001) 5.67 (.017)
Social fears 399 (5.3) 29 (6.6) 17 (15.3) 22.2 (⬍.001) 8.82 (.003)
Particular fears 926 (12.1) 63 (14.1) 26 (22.6) 12.9 (.002) 4.98 (.026)
General anxiety 630 (8.3) 45 (10.1) 20 (17.5) 13.9 (.001) 4.84 (.028)
Sadness/depression 849 (11.4) 74 (17.2) 24 (21.2) 22.9 (⬍.001) 1.00 (.316)
Obsessions/compulsions 564 (7.5) 40 (9.1) 31 (27.7) 63.2 (⬍.001) 27.6 (⬍.001)
Attention and activity problems 1054 (13.9) 94 (21.3) 44 (38.6) 71.5 (⬍.001) 14.5 (⬍.001)
Oppositional behavior 428 (5.7) 46 (10.5) 29 (25.4) 90.0 (⬍.001) 17.2 (⬍.001)
Conduct problems 471 (6.2) 46 (10.4) 21 (18.4) 37.8 (⬍.001) 5.49 (.019)
Child-reported measures
Overt bully 337 (8.6) 35 (15.9) 9 (18.4) 18.7 (⬍.001) 0.18 (.674)
Relational bully 121 (2.6) 8 (3.1) 1 (1.8) 0.43 (.807) 0.32 (.570)
Overt victim 1816 (33.7) 124 (40.1) 29 (42.0) 7.39 (.025) 0.08 (.771)
Relational victim 822 (15.5) 61 (19.9) 15 (21.1) 5.65 (.059) 0.06 (.812)
Scholastic competence 1282 (23.9) 78 (25.2) 14 (20.3) 0.80 (.672) 0.75 (.386)
Global self-worth 1069 (20.0) 78 (25.4) 17 (24.6) 6.13 (.047) 0.02 (.894)
Antisocial activities 1180 (21.5) 79 (24.9) 27 (37.0) 11.8 (.003) 4.36 (.037)
TABLE 3 Odds Ratios (95% CIs) for Reported Psychological Problems in Children With Frequent and Occasional Soiling Adjusting for Developmental Delay, Gender, Sociodemographic Background and Stressful Life Events
Problem, Frequency of Soiling (Reference Group⫽No Soiling)
Unadjusted Model
Adjusted 1 (Developmental Delay)
Adjusted 2 (⫹Gender, Sociodemographic Background,aand Stressful Life Events)
Parent-reported Separation anxiety
Occasional 1.38 (0.98–1.93) 1.33 (0.94–1.86) 1.26 (0.89–1.79)
Frequent 2.80 (1.69–4.62) 2.44 (1.46–4.07) 2.15 (1.27–3.66)
P ⬍.001 .001 .009
Social fears
Occasional 1.26 (0.85–1.86) 1.13 (0.76–1.67) 1.05 (0.71–1.57)
Frequent 3.24 (1.91–5.48) 2.32 (1.33–4.04) 2.06 (1.18–3.62)
P ⬍.001 .011 .041
Particular fears
Occasional 1.19 (0.91–1.57) 1.15 (0.87–1.52) 1.19 (0.90–1.57)
Frequent 2.12 (1.36–3.30) 1.87 (1.19–2.93) 1.92 (1.22–3.04)
P .002 .017 .011
General anxiety
Occasional 1.25 (0.91–1.72) 1.20 (0.87–1.66) 1.20 (0.87–1.66)
Frequent 2.35 (1.44–3.84) 2.07 (1.25–3.40) 1.91 (1.14–3.18)
P .001 .011 .030
Sadness/depression
Occasional 1.62 (1.25–2.10) 1.58 (1.22–2.05) 1.64 (1.26–2.14)
Frequent 2.10 (1.33–3.32) 1.92 (1.21–3.05) 1.93 (1.20–3.09)
P ⬍.001 ⬍.001 ⬍.001
Obsessions/compulsions
Occasional 1.23 (0.88–1.73) 1.11 (0.79–1.57) 1.07 (0.76–1.51)
Frequent 4.73 (3.10–7.23) 3.56 (2.28–5.56) 3.17 (2.01–5.00)
P ⬍.001 ⬍.001 ⬍.001
Attention/activity problems
Occasional 1.68 (1.33–2.13) 1.54 (1.20–1.97) 1.46 (1.14–1.88)
Frequent 3.90 (2.66–5.71) 2.88 (1.19–4.35) 2.63 (1.72–4.01)
P ⬍.001 ⬍.001 ⬍.001
Oppositional behavior
Occasional 1.95 (1.42–2.69) 1.76 (1.27–2.44) 1.70 (1.22–2.37)
Frequent 5.67 (3.68–8.75) 4.13 (2.60–6.54) 3.50 (2.18–5.64)
P ⬍.001 ⬍.001 ⬍.001
Conduct problems
Occasional 1.75 (1.27–2.41) 1.70 (1.23–2.34) 1.72 (1.24–2.38)
Frequent 3.40 (2.10–5.11) 2.99 (1.83–4.89) 2.67 (1.61–4.44)
P ⬍.001 ⬍.001 ⬍.001
Child-reported Overt bully
Occasional 2.01 (1.38–2.93) 2.01 (1.37–2.93) 1.86 (1.26–2.75)
Frequent 2.39 (1.15–4.97) 2.39 (1.15–4.96) 1.75 (0.82–3.77)
P ⬍.001 P⬍.001 .003
Overt victim
Occasional 1.32 (1.04–1.67) 1.31 (1.04–1.66) 1.26 (0.99–1.59)
Frequent 1.43 (0.88–2.31) 1.39 (0.86–2.25) 1.20 (0.73–1.97)
P .025 .033 .133
Relational victim
Occasional 1.35 (1.01–1.80) 1.34 (1.01–1.80) 1.39 (1.04–1.86)
Frequent 1.46 (0.82–2.59) 1.44 (0.81–2.56) 1.48 (0.83–2.64)
P .061 .068 .042
Scholastic competence
Occasional 1.07 (0.83–1.40) 1.06 (0.82–1.39) 1.06 (0.81–1.39)
Frequent 0.81 (0.45–1.46) 0.78 (0.43–1.41) 0.73 (0.40–1.33)
P .672 P⫽.638 .526
Global self-worth
Occasional 1.37 (1.05–1.78) 1.34 (1.03–1.75) 1.32 (1.01–1.72)
Frequent 1.31 (0.75–2.28) 1.22 (0.70–2.13) 1.14 (0.65–2.00)
P .048 .079 .122
Antisocial activities
Occasional 1.21 (0.93–1.57) 1.20 (0.92–1.56) 1.08 (0.83–1.42)
Frequent 2.14 (1.32–3.45) 2.05 (1.27–3.33) 1.65 (1.01–2.71)
P .003 .006 .117
Friendship score
Occasional 1.04 (0.78–1.40) 1.01 (0.76–1.36) 1.01 (0.75–1.35)
Frequent 1.27 (0.73–2.21) 1.18 (0.67–2.07) 1.11 (0.63–1.96)
P .688 .846 .937
chological problems in children who soil compared with controls (higher odds in children who soil frequently). Adjusting for developmental delay (adjusted 1) resulted in a large reduction in the odds ratios associated with social fears, obsessions/compulsions, attention and activ-ity problems, and oppositional behavior in frequently soiling children. Adjusting for the other confounding variables (gender, sociodemographic background, and stressful life events) had, in general, only a minor effect on the odds ratios. After the fully adjusted models had been fitted, the hypothesis of equality between the 2 soiling groups was formally tested for each outcome in turn. In a number of cases, the odds of a positive out-come were found to be significantly higher in the fre-quently soiling compared with the occasionally soiling children. These were social fears (borderline significant,
P ⫽.041), obsessions and compulsions (P⬍ .001),
at-tention and activity problems (P ⫽ .017), and
opposi-tional behavior (P⫽.011).
In the unadjusted models for the child-reported mea-sures (Table 3), the odds of being a perpetrator or a victim of overt bullying and engaging in antisocial activ-ities were significantly greater in children who soil com-pared with controls. In the final adjusted models, the effect of most confounders on the estimates was negli-gible with the exception of the overt bullying variables (bully and victim) and antisocial activities where adjust-ment for gender resulted in a small reduction in the odds ratios (these problems were more common in boys irre-spective of soiling).
DISCUSSION
The present study, based on a large epidemiologic
sam-ple of ⬃8000 children, was an investigation into the
psychological problems associated with soiling. The find-ings are important, not only because they show a signif-icantly higher rate of emotional and behavioral problems reported by parents of children with soiling problems compared with those without, but also because there were significantly more problems in children who soil frequently (once a week or more) compared with those who soil occasionally (less than once a week). Particu-larly striking were the significantly higher rates of atten-tion and activity problems, obsessions and compulsions, and oppositional behavior reported by parents of chil-dren who soil frequently compared with those who soil occasionally. The only other population-based study of psychological problems in children who soil, although not using standardized questionnaires, also reported significantly higher rates of emotional and behavioral
problems in children who soil.6 These results provide
evidence for an association between soiling and psycho-logical problems, even in nonclinical samples.
In comparison to previous studies of childhood soil-ing, which are mainly based on parental reports of psy-chological problems, the current study also included
reports from children about bullying, behavior, self-es-teem, and friendships. In particular, this is the first study in which children who soil are significantly more likely to report being victims or perpetrators of overt bullying behaviors (eg, name-calling and physical aggression) and antisocial activities (eg, aggression toward people and animals and destruction of property) than children with no soiling problems. The increased rates of bullying and antisocial activities reported by children who soil concur with the parental reports of oppositional and conduct problems, because these behaviors are often related.
Children were also asked questions about self-esteem in the current study, but there was no strong evidence for reduced self-esteem in children who soil compared with children with no soiling problems (global self-worth scores were slightly reduced in soiling compared with nonsoiling children). Previous studies comparing children’s reports of self-esteem levels have either found reduced self-esteem in those who soil18,19 or no
differ-ence in self-esteem level.14These equivocal findings may
be because of the self-report measure used or because of a tendency for children to deny experiencing problems or to underestimate their severity in self-reports.14
How-ever, the way in which children in this study were asked sensitive questions in the interview (by posting their responses in either a yes or no box that the interviewer could not see) should have helped to minimize any such problems.
Overall, there were fewer significant group differ-ences between the soiling and nonsoiling groups on the measures reported by the children compared with those reported by parents. It is possible that the findings were compounded by a bias in parental rating, with parents of children who soil viewing their children more nega-tively, perhaps because of the unpleasant nature of the problem or the belief that the soiling is intentional.15
Another possible explanation for the difference in the rate of problems reported by parents and children is that parents were asked about different issues (emotional and behavioral problems) compared with children (bul-lying, friendships, and self-esteem), which may imply that children with soiling have distinct psychological problems.
It is well known that children with developmental delay are at heightened risk for behavior problems and mental disorder.29,30In the current study, adjusting for
developmental delay led to a reduction in the odds ratios for the parent-reported psychological problems, with the largest reductions found for social fears, obsessions/com-pulsions, attention and activity problems, and opposi-tional behavior. However, even after adjusting for de-velopmental delay, the association of these problems with soiling remained highly significant.
girls.6,9,31–33 In addition, there was also an association
between soiling and having highly stressful life events. As a consequence, there were modest reductions in the regression estimates for soiling after adjusting for these variables.
Adjusting for the effect of confounding variables re-lating to sociodemographic status had a negligible effect on the relationship between soiling and psychological problems in this study suggesting that these variables do not represent underlying risk factors for psychological problems in the study population. This is in agreement with a recent population-based study reporting that dif-ferences in behavioral and emotional problems between soiling and nonsoiling children remained even after cor-rection for sociodemographic factors.6
The majority of studies of psychological problems in children who soil have included only a very small num-ber of children with nonretentive soiling (where there is no evidence of constipation) compared with those with retentive soiling (where there is evidence of constipa-tion). Only 2 studies compare children with retentive and nonretentive soiling, and they report no difference in the rate of behavior problems between the 2
groups.10,13 Comparison of retentive and nonretentive
types of soiling was not possible in the present study because of a number of concerns with the constipation measure that was used. These concerns were mostly because of the fact that the constipation measure was not based on clinical assessment but on parental reports of whether or not their child had suffered from consti-pation in the past 12 months. This may have resulted in the low rate of constipation found in children who soil the present study (19.4% of those soiling less that once a week, 31.3% of those soiling once a week, and 46.4% of those soiling twice a week or more). It is possible that parents of children who soil in the present study under-reported the presence of constipation, because, unless the child has seen a health professional for their soiling problem, parents might be unaware that the child is constipated. However only a small proportion of chil-dren see a doctor for soiling problems,6and this is
pos-sibly because parents are unaware that soiling is a con-dition for which they could seek medical advice.
There are also potential weaknesses associated with the parent-reported measure of soiling used in the cur-rent study. First of all, there is no information on the quantity of feces lost in the underwear. Some parents included a note in the questionnaire to clarify their response to the soiling question, for example, child has soiled his/her pants only because of diarrhea or pants were soiled because of insufficient cleaning after defeca-tion. It was reassuring to see that in cases such as these, parents did not place their children in the soiling cate-gory.
The fact that parents in the present study were not asked about the duration of soiling is another potential
weakness of the soiling measure. According to DSM-IV5
and the Rome II criteria,34soiling should be present for
ⱖ3 or ⱖ2 months as published in a recent article.35
However, rates of soiling measured at a previous time point in the ALSPAC data suggest that soiling is a per-sistent problem in these children (of the children who were soiling at 91 months, 83.2% of those soiling once a week or more, and 54.5% of those soiling less than once a week were also reported to be soiling at 78 months).
Another weakness of the study is that the small num-bers of children who met DSM-IV criteria for psychiatric disorders prevented an adequate multivariable statistical analysis using the proper diagnoses derived from the DAWBA. Instead, the study compared children on the rate of symptoms of behavioral and emotional disorders. Although this had the advantage of permitting a more rigorous multivariable statistical analysis, the impact of the symptoms in terms of resultant distress and interfer-ence with family life, learning, friendships, and leisure activities was not considered. The fact that children can have symptoms of disorders but are not necessarily sig-nificantly impaired by them means that the rate of par-ent-reported psychological problems may have been overestimated in the present study. However, in deriving the dichotomous outcome variables based on reported symptoms of psychiatric disorders, only the children with the most “severe” symptoms (children who were reported to have suffered from the symptoms the most often or a lot more than others of the same age) were included in the group with emotional or behavioral problems.
It is also possible that, in the present study, symptom categories may not be independent and that the psycho-logical problems identified in children who soil are indi-cators of comorbid psychiatric disorders. For example, attention and activity problems and oppositional behav-ior often occur together, as do anxiety and depression. In the present study, there was some overlap between do-mains in the DAWBA, but of the children who were reported to have behavioral or emotional problems,
many (⬃70%) had symptoms in only 1 domain.
There is also a potential difficulty associated with the DAWBA being given as a self-report questionnaire in that parents might mistake symptoms of 1 disorder for another. However, the lists of symptoms in the DAWBA that were used to derive the dichotomous outcome vari-ables for the current study were composed of closed questions, for example, “Has he/she ever worried about sleeping alone?” and “Is he scared of dentists or doc-tors?” Such a format means that there is minimal op-portunity for misinterpretation.
than those who defaulted. However, there does not seem to be a relationship between dropout and soiling, and controlling for sociodemographic variables had only a negligible effect on the regression estimates. Because sociodemographic variables are good predictors of attri-tion, this would lead us to infer that there is not a great deal of bias present in our final adjusted models and that the results can be generalized to the ALSPAC population as a whole.
As with all cross-sectional studies, it is unclear whether the psychological problems found in the present study are a cause or a consequence of soiling. Early studies suggest that emotional and behavior
prob-lems are a primary cause,36,37whereas other approaches
view behavior problems as secondary to soiling.38In the
majority of children, it is hypothesized that childhood constipation is the result of a painful experience, such as the passage of hard stools.39The presence of significant
behavior problems in children who soil does not neces-sarily mean that a child should be treated in a psychiatric setting. Successful treatment in a pediatric setting often results in a resolution or reduction of behavioral diffi-culties and other psychological problems.15,40,41
There is likely to be a complex interrelationship of biological, dietary, neurologic, psychological, and ge-netic factors involved in causal mechanisms related to soiling. Future plans include longitudinal studies looking at the association between soiling and the development of psychological problems, particularly in relation to toi-let training, parental child-rearing practices, child’s tem-perament, and early stresses, and to determine the in-teraction of these factors in the persistence of a child’s incontinence.
ACKNOWLEDGMENTS
A grant to support this research was given by the Big Lottery Fund to the charity Education and Resources for Improving Childhood Continence, and the study was conducted in collaboration with ALSPAC. Financial sup-port for the establishment of the ALSPAC cohort was provided by the Medical Research Council, the Well-come Trust, the United Kingdom Department of Health, Department of the Environment, Department for Edu-cation and Skills, National Institutes of Health, and a variety of medical research charities and commercial companies. The ALSPAC study is part of the World Health Organization–initiated European Longitudinal Study of Pregnancy and Childhood.
We are extremely grateful to all the families who participate in ALSPAC and to the midwives for their cooperation and help in recruitment. The whole AL-SPAC study team comprises interviewers, computer technicians, laboratory technicians, clerical workers, re-search scientists, managers, and volunteers who con-tinue to make the study possible.
REFERENCES
1. Bernard-Bonnin AC, Haley N, Belanger S, Nadeau D. Parental and patient perceptions about encopresis and its treatment.J Dev Behav Pediatr.1993;14:397– 400
2. Gabel S, Hegedus AM, Wald A, Chandra R, Chiponis D. Prev-alence of behavior problems and mental health utilization among encopretic children: implications for behavioral pediat-rics.J Dev Behav Pediatr.1986;7:293–297
3. Levine MD. Children with encopresis: a descriptive analysis.
Pediatrics.1975;56:412– 416
4. Molnar D, Taitz LS, Urwin OM, Wales JKH. Anorectal manom-etry results in defecation disorders. Arch Dis Child. 1983;58: 257–261
5. American Psychiatric Association.Diagnostic and Statistical Man-ual of Mental Disorders: DSM-IV. 4th ed. Washington, DC: Amer-ican Psychiatry Press; 1995
6. van der Wal MF, Benninga MA, Hirasing RA. The prevalence of encopresis in a multicultural population.J Pediatr Gastroenterol Nutr.2005;40:345–348
7. Doleys DM, Schwartz MS, Ciminero AR. Elimination problems: enuresis and encopresis. In: Mash EJ, ed.Behavioral Assessment of Childhood Disorders.New York, NY: Guildford Press; 1981 8. Lukeman D. Mainly children: childhood enuresis and
encopre-sis. In: Getliffe K, Dolman M, eds. Promoting Continence: A Clinical and Research Resource. London, United Kingdom: Bal-liere Tindall; 1997
9. Bellman M. Studies on encopresis.Acta Paediatr Scand. 1996; 170:1–151
10. Benninga MA, Buller HA, Heymans HS, Tytgat GN, Taminiau JA. Is encopresis always the result of constipation?Arch Dis Child.1994;71:186 –193
11. Loening-Baucke VA, Cruikshank B, Savage C. Defecation dy-namics and behavior profiles in encopretic children.Pediatrics.
1987;80:672– 679
12. Johnston BD, Wright JA. Attentional dysfunction in children with encopresis.J Dev Behav Pediatr.1993;14:381–385 13. Benninga MA, Voskuijl WP, Akkerhuis GW, Taminiau JA,
Buller HA. Colonic transit times and behavior profiles in chil-dren with defecation disorders.Arch Dis Child.2004;89:13–16 14. Cox DJ, Morris JB Jr, Borowitz SM, Sutphen JL. Psychological
differences between children with and without chronic enco-presis.J Pediatr Psychol.2002;27:585–591
15. Young MH, Brennen LC, Baker RD, Baker SS. Functional encopresis: symptom reduction and behavioral improvement.
J Dev Behav Pediatr.1995;16:226 –232
16. Wald A, Hinds JP, Caruana BJ. Psychological and physiological characteristics of patients with severe idiopathic constipation.
Gastroenterology.1989;97:932–937
17. Friman PC, Mathews JR, Finney JW, Christophersen ER, Lei-bowitz JM. Do encopretic children have clinically significant behavior problems?Pediatrics.1988;82:407– 409
18. Landman GB, Rappaport L, Fenton T, Levine MD. Locus of control and self-esteem in children with encopresis.J Dev Behav Pediatr.1986;7:111–113
19. Owens-Stively JA. Self-esteem and compliance in encopretic children.Child Psychiatry Hum Dev.1987;18:13–21
20. Golding J, Pembrey M, Jones R. ALSPAC: the Avon Longitu-dinal Study of Parents and Children. I.Study methodology. Pae-diatr Perinat Epidemiol.2001;15:74 – 87
21. Goodman R, Ford T, Richards H, Gatward, R, Meltzer, H. The Development and Well-Being Assessment: description and initial validation of an integrated assessment of child and adolescent psychopathology.J Child Psychol Psychiatr.2000;41:645– 655 22. Woods S, Wolke D. Does the content of anti-bullying policies
23. Loeber R, Stouthamer-Loeber M, Van Kammen WB, Far-rington DP. Development of a new measure of self-reported antisocial behavior for young children: Prevalence and reliabil-ity. In: Klein M, ed.Cross-National Research in Self-Reported Crime and Delinquency. Boston, MA: Kluwer-Nijhoff; 1989:203–225 24. Harter S.The Construction of the Self: A Developmental Perspective.
London, United Kingdom: Guildford Press; 1999
25. Goodyer I, Wright C, Altham PME. Recent achievements and adversities in anxious and depressed school age children.
J Child Psychol Psychiatr.1990;31:1063–1077
26. Weschler D.Manual for the Weschler Intelligence Scale for Children. 3rd ed. San Antonio, TX: Psychological Corporation; 1991 27. van Buuren S, Boshuizen HC, Knook DL. Multiple imputation
of missing blood pressure covariates in survival analysis.Stat Med.1999;18:681– 694
28. Royston P. Multiple imputation of missing values: update.Stata J.2005;5:188 –201
29. Bregman JD. Current developments in the understanding of mental retardation. Part II: Psychopathology.J Am Acad Child Adolesc Psychiatry.1991;30:861– 872
30. Dykens EM. Psychopathology in children with intellectual dis-ability.J Child Psychol Psychiatry.2000;41:407– 417
31. Hansen A, Hansen B, Dahm TL. Urinary tract infection, day wetting and other voiding symptoms in seven- to eight-year-old Danish children.Acta Paediatr.1997;86:1345–1349 32. Rutter M, Tizard J, Whitmore K.Education, Health and
Behav-iour. London, United Kingdom: Longman; 1970
33. Golding J, Tissier, G. Soiling and wetting. In: Butler NR, Gold-ing J, eds.From Birth to Five: A Study of the Health and Behaviour of Britain’s 5-Year-Olds. Oxford, United Kingdom: Pergamon Press; 1986:64 –79
34. Voskuijl W, Heijmans J, Heijmans H, Taminiau J, Benninga MA. Use of Rome II criteria in childhood defecation disorders: applicability in clinical and research practice.J Pediatr.2004; 145:213–217
35. Benninga M, Candy DC, Catto-Smith, et al. The Paris Consen-sus on Childhood Constipation Terminology (PACCT) Group.
J Pediatr Gastroenterol Nutr.2005;40:273–275
36. Halpern WI. The treatment of encopretic children.J Am Acad Child Psychiatry.1977;16:478 – 499
37. Bemporad JR, Kresch RA, Asnes R, Wilson A. Chronic neurotic encopresis as a paradigm of a multifactorial psychiatric disor-der.J Nerv Ment Dis.1978;166:472– 479
38. Gabel S.Fecal Soiling, Chronic Constipation and Encopresis: Behavioral Problems in Childhood.New York, NY: Grune Stratton Inc; 1981: 214 –228
39. Loening-Baucke. Chronic constipation in children. Gastroenter-ology.1993;105:1557–1564
40. van der Plas RN, Benninga MA, Redekop WK, Taminiau JA, Buller HA. Randomised trial of biofeedback training for enco-presis.Arch Dis Child.1996;75:367–374
APPENDIX 1 Prevalence in the Study Population of DSM-IV Disorders, the Symptom-Based Outcome Variables (and a Description of How They Were Derived From the DAWBA), and the Child-Reported Problems
DSM-IV Diagnosis Outcomes for Current Study
Disorder Derived From DAWBA
Prevalence in ALSPAC Study Population, %
Outcome Variables Derived From
DAWBA
Derivation of Dichotomous Outcome Variables From List of Symptoms in DAWBA and Examples of Items in DAWBA
Relating to Each Outcome
Prevalence in ALSPAC Study Population, %
Separation anxiety 0.8 Separation anxiety Any separation anxiety symptom(s) “a lot more than others” compared with “no more than others” or “a little more than others,” for example, has he/she worried about sleeping alone?
7.2
Social phobia 0.3 Social fears Any social fears “a lot” compared with “none,” “a little,” or “hasn’t done this in the last month,” for example, has he/she been afraid of meeting new people?
5.5
Specific phobia 1.1 Particular fears Any particular fears “a great deal” compared with “quite a lot,” “only a little” or “not at all,” for example, is he/she scared of the dark?
12.4
Generalized anxiety disorder
0.5 General anxiety Any of the worries “often” compared with “sometimes” or “not at all,” for example, does he/she worry a lot about schoolwork, homework, or tests/examinations?
8.5
Any depressive disorder
0.5 Sadness/ depression Any mood symptoms compared with none, for example, did he/she think about death a lot?
11.8
Obsessive-compulsive disorder
0.1 Obsessions/ compulsions
Any of the behaviors “sometimes” or “often” compared with “none,” for example, checking things (doors, ovens, locks, etc), excessive cleaning (handwashing, toothbrushing, etc).
7.8
Any ADHD disorder 2.1 Attention and activity problems
Any attention/activity problems “a lot more than others” compared with “a little more than others” or “none,” for example, does he/she often fidget? Is he/she easily distracted?
14.6
Oppositional-defiant disorder
2.1 Oppositional behavior Any of the behaviors “a lot more than others” compared with “no more than others” or “a little more than others,” for example, has he/she had severe temper tantrums?
6.2
Conduct disorder 0.6 Conduct problems Any of the behaviors “definitely/often/ more than once” compared with “none” or “perhaps”/“sometimes”/“once only,” for example, has he/she bullied or threatened people?
6.6
APPENDIX 2 Prevalence of Child-Reported Problems in the Study
Population
Problem %
Overt bullying 9.1
Relational bullying 2.6
Overt victim 34.1
Relational victim 15.8
Low scholastic competence 23.9 (score range⫽6–24;ⱕ14⫽low score) Low global self-worth 20.3 (score range⫽6–24;ⱕ16⫽low score Unhappy with friendships 18.0 (score range⫽0–15;ⱖ6⫽high score)
DOI: 10.1542/peds.2005-1773
2006;117;1575
Pediatrics
Longitudinal Study of Parents and Children Study Team
Carol Joinson, Jon Heron, Ursula Butler, Alexander von Gontard and the Avon
Psychological Differences Between Children With and Without Soiling Problems
Services
Updated Information &
http://pediatrics.aappublications.org/content/117/5/1575
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/117/5/1575#BIBL
This article cites 32 articles, 7 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/gastroenterology_sub Gastroenterology
ub
http://www.aappublications.org/cgi/collection/psychosocial_issues_s Psychosocial Issues
http://www.aappublications.org/cgi/collection/medical_home_sub Medical Home
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2005-1773
2006;117;1575
Pediatrics
Longitudinal Study of Parents and Children Study Team
Carol Joinson, Jon Heron, Ursula Butler, Alexander von Gontard and the Avon
Psychological Differences Between Children With and Without Soiling Problems
http://pediatrics.aappublications.org/content/117/5/1575
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.