Management of Chronic Tension-Type
Headache With Tricyclic Antidepressant
Medication, Stress Management Therapy,
and Their Combination
A Randomized Controlled Trial
Kenneth A. Holroyd, PhD Francis J. O’Donnell, DO Michael Stensland, MS Gay L. Lipchik, PhD Gary E. Cordingley, MD, PhD Bruce W. Carlson, PhDT
ENSION-TYPE HEADACHES OF-ten occur every day or nearly every day in individuals who seek treatment,1-3 but
head-aches must occur 15 or more days per month for at least 6 months to meet In-ternational Headache Society diagnos-tic criteria for chronic rather than epi-sodic tension-type headache.4The 1-year
prevalence rate for chronic tension-type headache in the general popula-tion is about 3% in women and 1.5% in men,5,6with just less than half of those
with chronic tension-type headache re-porting headache-related impairment in work performance. Chronic tension-type headaches are a risk factor for the overuse of analgesic medications and thus the development of analgesic abuse headaches.2,4,6,7Continuous headaches
and frequent comorbid psychiatric or an-algesic use problems often render chronic tension-type headaches diffi-cult to manage in primary practice.1,2,8,9
Tricyclic antidepressants are the pri-mary drug therapy for chronic tension-type headache, with amitriptyline hy-drochloride the first-line treatment.2,9-12
However, recent trials have reported little (#30%) or no improvement in chronic tension-type headaches13-15with
amitriptyline. Additional information is therefore needed to confirm the ben-efits of this widely used medication for chronic tension-type headache.
Author Affiliations:Department of Psychology (Drs Holroyd, Lipchik, and Carlson and Mr Stensland) and College of Osteopathic Medicine (Dr Cordingley), Ohio University, Athens; and Headache Treatment and Re-search (Drs Holroyd, O’Donnell, and Lipchik) and Or-thoNeuro (Dr O’Donnell), Westerville, Ohio. Dr Lip-chik is now with St Vincent Health Center, Erie, Pa.
Corresponding Author and Reprints:Kenneth A. Hol-royd, PhD, 225 Porter Hall, Athens, OH 45701 (e-mail: [email protected]).
Context Chronic tension-type headaches are characterized by near-daily head-aches and often are difficult to manage in primary practice. Behavioral and pharma-cological therapies each appear modestly effective, but data are lacking on their sepa-rate and combined effects.
Objective To evaluate the clinical efficacy of behavioral and pharmacological thera-pies, singly and combined, for chronic tension-type headaches.
Design and Setting Randomized placebo-controlled trial conducted from August 1995 to January 1998 at 2 outpatient sites in Ohio.
Participants Two hundred three adults (mean age, 37 years; 76% women) with diagnosis of chronic tension-type headaches (mean, 26 headache d/mo).
Interventions Participants were randomly assigned to receive tricyclic antidepres-sant (amitriptyline hydrochloride, up to 100 mg/d, or nortriptyline hydrochloride, up to 75 mg/d) medication (n=53), placebo (n=48), stress management (eg, relaxation, cognitive coping) therapy (3 sessions and 2 telephone contacts) plus placebo (n=49), or stress management therapy plus antidepressant medication (n=53).
Main Outcome Measures Monthly headache index scores calculated as the mean of pain ratings (0-10 scale) recorded by participants in a daily diary 4 times per day; num-ber of days per month with at least moderate pain (pain rating$5), analgesic medica-tion use, and Headache Disability Inventory scores, compared by intervenmedica-tion group. Results Tricyclic antidepressant medication and stress management therapy each pro-duced larger reductions in headache activity, analgesic medication use, and headache-related disability than placebo, but antidepressant medication yielded more rapid im-provements in headache activity. Combined therapy was more likely to produce clinically significant ($50%) reductions in headache index scores (64% of participants) than antidepressant medication (38% of participants;P=.006), stress management therapy (35%;P=.003), or placebo (29%;P=.001). On other measures the combined therapy and its 2 component therapies produced similar outcomes.
Conclusions Our results indicate that antidepressant medication and stress man-agement therapy are each modestly effective in treating chronic tension-type head-aches. Combined therapy may improve outcome relative to monotherapy.
JAMA. 2001;285:2208-2215 www.jama.com
Behavioral therapies, primarily re-laxation, biofeedback, and cognitive be-havior (stress management) therapies appear to be effective in managing ten-sion-type headache.16-24However,
tri-als of behavioral therapies tri-also have methodological shortcomings: results typically have not been reported spe-cifically for participants with chronic tension-type headache and few trials have included placebo controls.25
Ad-ditional information is thus needed to confirm the effectiveness of behav-ioral therapy for chronic tension-type headache. The possibility that behav-ioral therapy can enhance outcomes ob-tained with antidepressant medica-tion (AM) also needs to be evaluated.13,24
This study was intended to evaluate the separate and combined effects of tri-cyclic antidepressant (amitriptyline and nortriptyline hydrochloride) medica-tion (AM) and brief stress manage-ment therapy (SMT) for chronic ten-sion-type headache.
METHODS
Participants
Participants were recruited from pri-mary practice referrals and by local ad-vertisements at 2 outpatient sites. In-clusion criteria were age between 18 and 65 years and receipt of an Interna-tional Headache Society diagnosis of chronic tension-type headache4at 2
separate evaluations. Exclusion crite-ria were: International Headache Soci-ety diagnosis of analgesic-abuse head-aches4; current use of AM or other
prophylactic medication for head-ache, or regular ($15 d/mo) use of anx-iolytic medication; current psycho-therapy; current or planned pregnancy or breastfeeding; medical contraindi-cation to amitriptyline; migraine head-ache more than 1 day a month; pain dis-order (eg, arthritis) other than headache as primary pain problem; psychiatric (eg, suicide risk) or medical disorder requiring immediate treatment; and fail-ure to complete baseline diary record-ings of headache activity and medica-tion use. All participants provided written informed consent according to
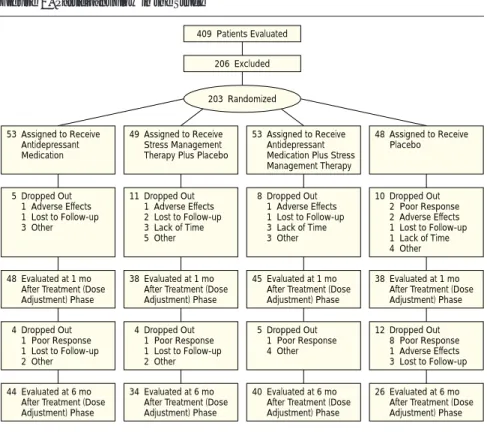
procedures approved by the Ohio Uni-versity Human Subjects Committee. Study Design and Treatments After completing the baseline assess-ment that included 1 month of head-ache and medication diary recordings, participants were randomly assigned in blocks of 4 participants to 4 treatments (FIGURE1): AM, placebo, SMT plus pla-cebo, and SMT plus AM. The AM and placebo therapies were administered in a standard double-blind fashion. Treat-ment conditions were blinded only for the medication component and not for the administration of SMT. This trial was conducted between August 1995 and January 1998.
Each treatment protocol required 3 clinic visits and 2 telephone contacts during the 2-month treatment (dose ad-justment) phase, during which SMT was administered and the medication dose was adjusted. Clinic visits were sched-uled at weeks 1, 4, and 8 of this treat-ment (dose adjusttreat-ment) phase; tele-phone contacts were scheduled at the beginning of weeks 3 and 7. In the
sub-sequent 6-month evaluation phase, clinic visits were scheduled 1, 3, and 6 months following completion of the treatment (dose adjustment) phase. The 1- and 6-month evaluations included review of 1 month of daily headache and medica-tion diaries, neurological evaluamedica-tion, and psychosocial testing. The 3-month evaluation included only medication checks and brief evaluation.
Tricyclic Antidepressant Medica-tion and Placebo.In this double-blind protocol, we attempted to maximize the efficacy and tolerability of AM by using a low starting dose and recommended target doses for the treatment of chronic tension-type headache,11,26-29by
treat-ing participants who were unable to tol-erate amitriptyline with nortriptyline and by use of an adherence intervention
de-signed to increase AM adherence.30
Treatment was initiated with 1 lead-in capsule of medication to be taken at bed-time (12.5 mg of amitriptyline hydro-chloride or matched placebo) and in-creased to 3 regular (25 mg or matched placebo) capsules by week 6, as toler-ated. At week 8, dose level was
stabi-Figure 1.Participant Flow in the Study
409 Patients Evaluated 53 Assigned to Receive Antidepressant Medication 49 Assigned to Receive Stress Management Therapy Plus Placebo
53 Assigned to Receive Antidepressant Medication Plus Stress Management Therapy 48 Assigned to Receive Placebo 4 Dropped Out 1 Poor Response 1 Lost to Follow-up 2 Other 4 Dropped Out 1 Poor Response 1 Lost to Follow-up 2 Other 5 Dropped Out 1 Poor Response 4 Other 12 Dropped Out 8 Poor Response 1 Adverse Effects 3 Lost to Follow-up 48 Evaluated at 1 mo
After Treatment (Dose Adjustment) Phase
38 Evaluated at 1 mo After Treatment (Dose Adjustment) Phase
45 Evaluated at 1 mo After Treatment (Dose Adjustment) Phase
38 Evaluated at 1 mo After Treatment (Dose Adjustment) Phase
44 Evaluated at 6 mo After Treatment (Dose Adjustment) Phase
34 Evaluated at 6 mo After Treatment (Dose Adjustment) Phase
40 Evaluated at 6 mo After Treatment (Dose Adjustment) Phase
26 Evaluated at 6 mo After Treatment (Dose Adjustment) Phase 5 Dropped Out 1 Adverse Effects 1 Lost to Follow-up 3 Other 11 Dropped Out 1 Adverse Effects 2 Lost to Follow-up 3 Lack of Time 5 Other 8 Dropped Out 1 Adverse Effects 1 Lost to Follow-up 3 Lack of Time 3 Other 10 Dropped Out 2 Poor Response 2 Adverse Effects 1 Lost to Follow-up 1 Lack of Time 4 Other 206 Excluded 203 Randomized
lized at the highest tolerated level. If a participant did not tolerate the first medication, at least 2 regular capsules (50 mg) of amitriptyline hydrochlo-ride or matched placebo, and, in the treating neurologist’s (F.J.O., G.E.C.) judgment was unimproved, the patient was switched (with blindness main-tained) to the second medication, nor-triptyline, or matched nortriptyline pla-cebo for participants who had been receiving placebo. Participants initially received a single 25-mg nortriptyline hy-drochloride capsule or matched pla-cebo. The dose was increased at the next visit to 2 capsules (50 mg) as tolerated. At week 8, the dose was stabilized at the highest tolerated level. In the evalua-tion phase, an increase to 4 capsules of amitriptyline hydrochloride (100 mg) or matched placebo or to 3 capsules of nor-triptyline hydrochloride (75 mg) or matched placebo was allowed.
Stress Management Therapy.A psy-chologist or counselor administered SMT in three 1-hour sessions at the same 3 clinic visits used for medica-tion dose adjustments. This primarily home-based treatment teaches both re-laxation and cognitive coping skills for preventing and managing stress and headaches.24,31In the first treatment
ses-sion, instruction manuals and audio-tapes32that guide the acquisition and
application of stress management skills at home were reviewed, and deep muscle relaxation training of 16 muscle groups33,34was introduced. At the
sec-ond treatment session, active cogni-tive coping35-37 or problem solving
techniques37-39for preventing and
man-aging headache-related stresses were in-troduced. At the third treatment ses-sion, the application of relaxation and cognitive coping skills to pain manage-ment was covered and the partici-pant’s experience with the headache management skills in the previous 2 months was reviewed. For partici-pants receiving SMT, the week 3 and 7 telephone contacts were used for both the medication adherence intervtion and the correcintervtion of problems en-countered in the application of behav-ioral headache management skills.
Measures
Participants recorded headaches and the use of analgesic and study medication in a daily diary.24,40-42Headache
activ-ity was recorded 4 times a day using an 11-point rating scale with 5 anchors that ranged from 0, which indicated no pain, to 10, which indicated extremely pain-ful or “I can’t do anything when I have a headache.” Diary recordings were ob-tained during the 1-month baseline phase, during the 2-month treatment (dose adjustment) phase, and, in months 1 and 6 of the 6-month evalu-ation phase.
The primary outcome measure was the headache index. The headache in-dex was the mean of all diary ratings for a 1-month period, and it provides a mea-sure of overall headache activity.24,40
Sec-ondary outcome measures were the number of days per month with a head-ache of at least moderate severity (pain rating$5),3analgesic medication
con-sumption (number of pills weighted by analgesic potency),40,43and
headache-related disability as assessed by the Head-ache Disability Inventory.44,45The
pri-mary end point for all measures was the 6-month evaluation (Figure 1). Psycho-physiological, psychodiagnostic, and psychosocial measures also were col-lected to address different questions. Data from these latter measures will be reported elsewhere.
Hypotheses and Statistical Analysis The study was designed to: (1) con-firm that AM alone and that SMT alone are more effective than placebo; (2) de-termine whether either AM or SMT is more effective than the other; and (3) determine whether the combination therapy is more effective than either AM or SMT.
Planned comparisons were con-ducted to examine each hypothesis . All analyses were conducted on the intent-to-treat sample of all 203 randomized participants with the last data point car-ried forward for dropouts. For the con-tinuous measures, after adjusting for baseline scores, F tests were used to evaluate each of 5 planned compari-sons, 1 for each hypothesis. For the
categorical headache measure, the pro-portion of participants showing clini-cally significant improvement (de-fined as a 50% or greater reduction in headache index scores46), Fisher exact
tests were used. A modified Bonfer-roni procedure47was used to control the
familywise type I error rate for the 5 comparisons at .05. One-tailed tests were used to compare AM and SMT with placebo; 2-tailed tests were used to compare active treatments.
We usedx2and Fisher exact tests to
determine whether the proportion of dropouts varied among the 4 treat-ment groups. Analyses of covariance and log-linear analyses were con-ducted to determine whether the effec-tiveness of the treatments varied by study site or for participants who received and did not receive a comor-bid migraine diagnosis. It did not. All analyses were conducted using SPSS Inc, Chicago, Ill.
The planned 200 subjects provided a power of 0.77 to detect a 0.75 differ-ence in headache index scores and power of 0.69 to detect a difference of 4 in at least moderately severe head-ache-days per month, differences that were judged to be meaningful.
RESULTS
Participant Characteristics
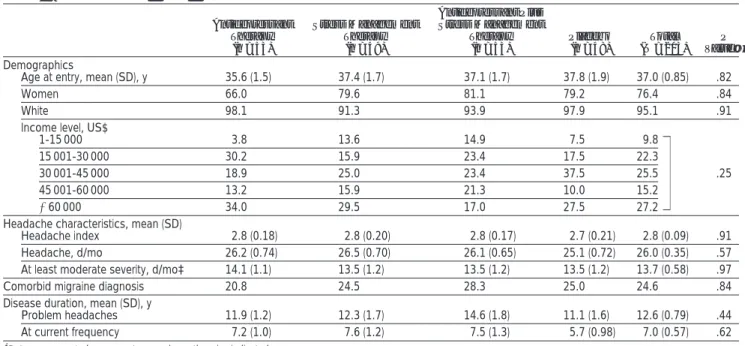
Demographic and clinical characteris-tics for the 203 participants are given inTABLE1. Sixty-three percent of par-ticipants recorded daily or near-daily
headaches ($25 headache d/mo). Of
the 203 participants, 160 (79%) re-ported having previously consulted a physician specifically for headache problems. However, 79 (49%) of these individuals werelapsed consulters,48
de-fined as not having consulted a physi-cian in at least 6 months despite per-sistent headache problems.
Attrition
Participant flow through the trial is dis-played in Figure 1. There were 206 ex-cluded participants: 54 chose not to be evaluated for the study or did not com-plete the pretreatment evaluation; 53 did not receive a primary diagnosis of
chronic tension-type headache or received a diagnosis of
analgesic-abuse headaches4 at the baseline
evaluation; 26 experienced migraines more than 1 day a month; 19 were using AM, other prophylactic head-ache medication, or anxiolytics regu-larly ($15 d/mo); 31 presented with a medical or psychiatric disorder that required referral; 10 were currently receiving psychotherapy; 6 were preg-nant or planned a pregnancy; 6 had a pain disorder other than headache as their primary pain problem; and 1 had a medical contraindication to amitriptyline.
At the 1-month evaluation, the number of dropouts did not differ among the 4 treatment groups (Figure 1). However, by the 6-month evalua-tion, differential dropout was observed across treatment groups (P=.01), with significantly lower attrition from the
AM (P= .002) and AM plus SMT
(P=.04) groups than from the placebo group. Attrition because of a poor treatment response was especially high with placebo, with participants in the placebo group 5.6 times more likely to discontinue the study than
partici-pants in the active treatment groups (P= .006). After their exit from the study, participants who terminated treatment because of a poor treatment response or inability to tolerate medi-cation generally requested additional treatment for their headaches. All such participants from the placebo group (n = 13) requested additional treat-ment. This was provided without charge for 9 months.
Dosing and Protocol Adherence At the 1-month evaluation, 84 (90%) of the 93 participants in the 2 active medication groups were taking ami-triptyline hydrochloride (3 at 25 mg, 8 at 50 mg, 73 at 75 mg) and 9 were tak-ing nortriptyline hydrochloride (3 at 25 mg, 6 at 50 mg). At the 6-month evalu-ation 70 (83%) of the 84 participants were taking amitriptyline hydrochlo-ride (3 at 25 mg, 14 at 50 mg, 44 at 75 mg, 9 at 100 mg) and 14 were taking nortriptyline hydrochloride (4 at 25 mg, 9 at 50 mg, 1 at 75 mg).
Daily diary recordings indicated that at least 90% of participants were ad-herent for 80% or more days in the 4 months, where diaries were collected
following the initiation of medication therapy. Neurologists (F.J.O., G.E.C.) rated at least 95% of participants as at least 90% adherent at the 4 neurologi-cal visits following the initiation of medication treatment. Adherence with the SMT protocol also was high. At the completion of SMT participants re-ported in a computer assessment that, on average, they had completed 15 of 17 (range, 3-17) workbook chapters and audiotapes and had attempted to use 9 of the 11 (range, 4-11) headache management strategies that had been presented.
Outcome
FIGURE2shows that all 3 active treat-ments, but not the placebo, yielded im-provements in headache activity by the 6-month evaluation, but improve-ment occurred more rapidly with AM than with SMT. At the 6-month evalu-ation, the AM and SMT groups each showed significantly larger reduc-tions in headache index scores than the placebo group. However, improve-ment was more rapid in the AM group than in the SMT group because the AM group showed larger reductions in
Table 1.Demographic and Clinical Characteristics* Antidepressant Therapy (n = 53) Stress Management Therapy (n = 49) Antidepressant Plus Stress Management Therapy (n = 53) Placebo (n = 48) Total (N = 203) P Value† Demographics
Age at entry, mean (SD), y 35.6 (1.5) 37.4 (1.7) 37.1 (1.7) 37.8 (1.9) 37.0 (0.85) .82
Women 66.0 79.6 81.1 79.2 76.4 .84
White 98.1 91.3 93.9 97.9 95.1 .91
Income level, US$
1-15 000 3.8 13.6 14.9 7.5 9.8
15 001-30 000 30.2 15.9 23.4 17.5 22.3
30 001-45 000 18.9 25.0 23.4 37.5 25.5 .25
45 001-60 000 13.2 15.9 21.3 10.0 15.2
.60 000 34.0 29.5 17.0 27.5 27.2
Headache characteristics, mean (SD)
Headache index 2.8 (0.18) 2.8 (0.20) 2.8 (0.17) 2.7 (0.21) 2.8 (0.09) .91 Headache, d/mo 26.2 (0.74) 26.5 (0.70) 26.1 (0.65) 25.1 (0.72) 26.0 (0.35) .57 At least moderate severity, d/mo‡ 14.1 (1.1) 13.5 (1.2) 13.5 (1.2) 13.5 (1.2) 13.7 (0.58) .97 Comorbid migraine diagnosis 20.8 24.5 28.3 25.0 24.6 .84 Disease duration, mean (SD), y
Problem headaches 11.9 (1.2) 12.3 (1.7) 14.6 (1.8) 11.1 (1.6) 12.6 (0.79) .44 At current frequency 7.2 (1.0) 7.6 (1.2) 7.5 (1.3) 5.7 (0.98) 7.0 (0.57) .62 *Data are presented as percentages unless otherwise indicated.
†Results fromx2analyses on discrete variables and analyses of variance for continuous variables. ‡Pain rating$5 on an 11-point rating scale (0-10).
headache index scores than the SMT group at the 1-month evaluation (TABLE2). The combined AM plus SMT treatment group and the SMT and AM treatment groups all showed similar im-provements in headache index scores at the 6-month evaluation, but head-ache index scores improved more rap-idly in the AM plus SMT treatment group than in the SMT only group. A greater proportion of participants in the AM plus SMT group (34 [64%] of 53) also showed clinically significant ($50%)46reductions in headache
in-dex scores compared with only 20 (38%) of 53 in the AM group (P=.006), 17 (35%) of 49 in the SMT group (P= .003), and 14 (29%) of 48 in the placebo group (P= .001).
Improvements in secondary out-come measures paralleled improve-ments in headache index scores with only 2 exceptions. For the “days of at least moderate pain” variable, improve-ment was not significantly more rapid in the AM plus SMT than in the SMT only group; for Headache Disability In-ventory scores, improvements were equally rapid in all 3 active treatment groups (Figure 2B, 2C, and 2D and Table 2).
The differential dropout rate of par-ticipants who complained of a poor treatment response from the placebo group renders a completor analysis biased because unimproved partici-pants were differentially removed from the placebo group in this analysis.
Ef-fect sizes for active treatments were smaller when calculated from end point data than from completor data, sug-gesting end point data yielded a more conservative estimate of treatment ef-fect size than completor data. Never-theless, completor analysis revealed the same results at the 6-month evalua-tion as did the end point analysis, with 2 exceptions on secondary outcomes: in the completor analysis the SMT group and the placebo group did not differ significantly on the weighted an-algesic-use variable; also, the AM group and the placebo group did not differ sig-nificantly on headache disability scores. When 2 imputation procedures (im-putation of either the treatment group mean or the mean of previous data points for the participant) were used to replace missing headache index data at the 6-month evaluation, instead of car-rying actual end point data forward, the results from both analyses were the same as the end point analysis. Adverse Effects
Among 187 participants who com-pleted at least the first dose adjust-ment session, 78 (80%) of 97 partici-pants who received AM and 27 (30%) of 90 participants who received pla-cebo reported adverse effects (P=.001). Of 9 reported adverse effects caused by AM (dry mouth, drowsiness, weight gain, dizziness, sweating, constipa-tion, abdominal pains, nervousness, in-creased appetite), only dry mouth and drowsiness were reported by more than 10% of participants in either treat-ment group; 51 participants (53%) in the AM group reported dry mouth vs 12 (13%) in the placebo group (P=.001) and 43 participants (44%) in the AM group reported drowsiness vs 10 (11%) in the placebo group (P= .001).
COMMENT
To our knowledge, this is the first pla-cebo-controlled trial to examine the separate and combined effects of be-havioral and drug therapies for a chronic headache disorder. Results in-dicate that AM and SMT, alone and in combination, are effective in reducing
Figure 2.Mean Headache Activity, Medication Use, and Disability Scores
Placebo Stress Management Therapy
Antidepressant Medication Plus Stress Management Therapy Antidepressant Medication 3.0 1.0 0.5 1.5 2.0 2.5 0 Headache Index
Mean Headache Index Scores
A B Days of at Least Moderate Pain
10 8 6 4 2 12 14 0 At Least Moderately Sever e Headache, d/mo 45 20 25 30 35 40 15 0 1 2 3 4 5 6 Month
Headache Disability Inventory
2 1 Baseline Treatment (Dose Adjustment) Evaluation Analgesic Medication Use Scores
C D Headache Disability Inventory Scores 50 10 20 30 40 0 0 1 2 3 4 5 6 Month W
eighted Analgesic Use
2 1 Baseline Treatment (Dose Adjustment) Evaluation
A, Headache index is calculated as mean of daily pain ratings (range, 0-10) over a 1-month period. B, A day of at least moderate pain is indicated by a rating of$5 (scale, 0-10). C, A medication score of 40, for example, could reflect intake of 40 pills per month of simple or combined nonprescription analgesic (weight, 1), 20 pills per month of prescription-strength nonsteroidal anti-inflammatory agents (weight, 2), or 13.3 pills per month of a compound (eg, butalbital containing) analgesic (weight, 3). In A-D, error bars indicate SEs.
chronic tension-type headaches, anal-gesic medication consumption, and headache-related disability. All 3 ac-tive treatments produced improve-ments in each of these variables, while chronic tension-type headaches proved unresponsive to even 8 months of clinical attention and treatment with placebo. However, reductions in head-ache activity and in analgesic medica-tion consumpmedica-tion (but not headache-related disability) occurred more rapidly with AM than with SMT. In addition, observed reductions in headache ac-tivity were clinically meaningful but were only moderate in magnitude. For example, each of the active treatments reduced the average number of days of at least moderately severe headache pain by half, from about 14 days to fewer than 7 days a month.
These results provide needed em-pirical support for the use of tricyclic AM
in the management of chronic tension-type headaches.13Although
amitripty-line dose levels did not differ apprecia-bly in this study compared with previous studies that reported negative or mar-ginal findings,13,14our medication
pro-tocol did include a brief adherence in-tervention30and did permit substitution
of a second tricyclic antidepressant. Al-though our results provide clear sup-port for the efficacy of tricyclic AM in the management of chronic tension-type headaches, specific findings may not gen-eralize to treatment protocols that do not include these features. In spite of the positive results observed with tricyclic AM, only about one third of partici-pants in the AM-only treatment group recorded substantial ($50%) reduc-tions in headache activity.
Brief SMT also effectively reduced chronic tension-type headache activ-ity, producing improvements in
head-ache activity, use of analgesic medica-tion, and headache-related disability comparable to improvements ob-served with AM alone. However, im-provements in headache activity and in analgesic medication use with SMT were not fully evident until the 6-month evaluation, probably because ac-quired stress-management skills must be applied for several months before they have an affect on daily or almost daily headaches. Our results provide the first evidence that chronic tension-type headaches are responsive to be-havioral therapy but suggest that there may be a time lag before the full-treatment response is evident. Brief SMT thus appears to offer a viable alterna-tive to AM. Nonetheless, mono-therapy with brief SMT also produced substantial ($50%) reductions in head-ache activity in only about one third of participants.
Table 2.Planned Comparisons Testing Differences in Effectiveness of Treatments at 1-Month and 6-Month Evaluations* 1-Month Evaluation 6-Month Evaluation
F Value† PValue‡
Mean Difference§
(95% CI) F Value PValue
Mean Difference (95% CI) Headache index AM vs placebo 20.95 .001\ 1.00 (0.57 to 1.43) 14.30 .001\ 0.92 (0.44 to 1.41) SMT vs placebo 4.20 .02\ 0.46 (0.02 to 0.89) 10.08 ,.01\ 0.79 (0.30 to 1.28) AM plus SMT vs AM 0.01 .91 0.02 (−0.39 to 0.44) 0.29 .59 0.13 (−0.34 to 0.60) AM plus SMT vs SMT 6.86 ,.01\ 0.57 (0.14 to 1.00) 1.17 .28 0.26 (−0.22 to 0.74) SMT vs AM 6.28 .01\ −0.54 (−0.97 to −0.12) 0.30 .58 −0.13 (−0.61 to 0.35) At least moderately severe headache, d/mo
AM vs placebo 20.88 .001\ 6.0 (3.4 to 8.6) 12.26 .001\ 5.0 (2.2 to 8.0) SMT vs placebo 3.57 .03 2.5 (−0.1 to 5.2) 12.51 .001\ 5.1 (2.3 to 8.0) AM plus SMT vs AM 0.93 .34 −1.2 (−3.8 to 1.3) 0.01 .94 0.1 (−2.6 to 2.8) AM plus SMT vs SMT 2.95 .09 2.3 (−0.3 to 4.8) 0.00 .98 0.0 (−2.8 to 2.8) SMT vs AM 7.08 ,.01\ −3.5 (−6.1 to −0.9) 0.01 .92 0.1 (−2.7 to 2.9) Weighted analgesic use
AM vs placebo 11.85 .001\ 17.7 (7.6 to 27.8) 12.41 .001\ 18.0 (7.9 to 28.1) SMT vs placebo 0.11 .37 −1.7 (−12.0 to 8.6) 5.14 .01\ 11.8 (1.5 to 22.1) AM plus SMT vs AM 0.39 .54 −3.1 (−13.0 to 6.8) 0.23 .63 −2.4 (−12.2 to 7.5) AM plus SMT vs SMT 10.16 ,.01\ 16.3 (6.2 to 26.4) 0.57 .45 3.8 (−6.2 to 13.9) SMT vs AM 14.42 .001\ −19.4 (−29.5 to −9.3) 1.49 .22 −6.2 (−16.2 to 3.8) Headache Disability Inventory score
AM vs placebo 6.38 ,.01\ 7.3 (1.6 to 12.9) 5.69 ,.01\ 6.9 (1.2 to 12.6) SMT vs placebo 6.29 ,.01\ 7.3 (1.6 to 13.0) 9.91 .001\ 9.3 (3.5 to 15.1) AM plus SMT vs AM 0.72 .40 2.4 (−3.1 to 7.9) 2.07 .15 4.1 (−1.5 to 9.6) AM plus SMT vs SMT 0.67 .41 2.3 (−3.3 to 7.9) 0.34 .56 1.7 (−4.0 to 7.3) SMT vs AM 0.01 .99 0.1 (−5.6 to 5.7) 0.69 .41 2.4 (−3.3 to 8.0) *CI indicates confidence interval; AM, antidepressant medication; and SMT, stress management therapy.
†F value for comparison. Degrees of freedom for each test is 198, except for Headache Disability Inventory, for which degrees of freedom are 197 due to 1 missing data point. ‡Pvalue for contrast. Two contrasts containing placebo are 1-tailed; all others are 2-tailed. Values,.001 are reported as .001.
§Difference in adjusted (for baseline score) means.
The combination of AM plus STM produced clinically significant reduc-tions in headache activity in a greater proportion of participants than either AM or STM alone. Almost two thirds of participants treated with the com-bined treatment, but a little more than one third of participants in the AM or STM groups, showed clinically signifi-cant ($50%) reductions in headache in-dex scores. Although this finding suggests that combined therapy can im-prove outcomes relative to mono-therapy, it must be qualified by the fact that no significant advantage for com-bined therapy was observed on other outcome variables.
Methodological limitations of this trial need to be kept in mind when in-terpreting these results. Although this is the largest trial that has compared the effectiveness of drug and nondrug therapies for chronic tension-type head-ache, this trial did not have power to detect small treatment effects.49
Rela-tively high attrition also was ob-served, especially for participants treated with placebo, who were likely to exit the trial because of a poor trement response. No previous trial has at-tempted to maintain a placebo control group for as long as 8 months; thus, it is probably not surprising that partici-pants seeking relief from daily head-aches requested alternate treatment be-fore they went 8 months with no relief. Attrition did not differ significantly across the 3 active treatment groups but ranged from 17% to 31% at the final as-sessment.
Primary analyses were conducted us-ing all randomized participants, carry-ing end point data forward. Alternate analyses using data from only the par-ticipants who completed the 6-month evaluation and using 2 alternate meth-ods of imputing missing data for drop-outs yielded similar results. The con-vergence of results from different analyses increases confidence in the findings, but it cannot eliminate the possibility that dropouts biased the es-timates of treatment effects. It has been argued that administration of psycho-logical treatment with placebo
im-pairs the effectiveness of psychologi-cal therapy by reducing participants’ involvement in psychological treat-ment.50Although empirical support for
this contention is limited,51if this is true,
our findings would underestimate the effectiveness of SMT. Finally, partici-pants with a comorbid pain disorder as a primary presenting problem, with fre-quent comorbid migraines, or with a di-agnosis of analgesic-abuse headaches were excluded to allow evaluation of the effects of treatment specifically on chronic tension-type headaches. Re-sults thus cannot be readily general-ized to participants with these comor-bid medical problems. Future studies conducted in primary practice set-tings might thus examine outcome as a function of comorbid disorders.
Author Contributions:Study concept and design: Hol-royd, O’Donnell, Lipchik, and Cordingley.
Acquisition of data:Holroyd, O’Donnell, Stensland, Lipchik, and Cordingley.
Analysis and interpretation of data:Holroyd, Stens-land, Cordingley, and Carlson.
Drafting of the manuscript:Holroyd, Stensland, and Carlson.
Critical revision of the manuscript for important in-tellectual content:Holroyd, O’Donnell, Stensland, Lip-chik, Cordingley, and Carlson.
Statistical expertise:Holroyd, Stensland, and Carl-son.
Obtained funding:Holroyd and Carlson.
Administrative, technical, or material support: Hol-royd, O’Donnell, Lipchik, and Cordingley.
Study supervision:Holroyd, O’Donnell, and Carlson.
Funding/Support:This work was funded by grant NS32374 from the National Institute of Neurological Disorders and Stroke, National Institutes of Health.
Acknowledgment:We thank Katherine Davis Rosen-balm, PhD, Douglas French, PhD, Kimberly Hill, MS, Jennifer Labus, MS, Peter Malinoski, MS, Adriana Meade, BA, Angela Nicolosi, MA, Carol Nogrady, BA, Cornelia Pinnell, PhD, France Talbot, PhD, and Sharon Waller, RN.
REFERENCES
1.Jensen R, Sandrini G. Symptomatology of chronic tension-type headache. In: Olesen J, Tfelt-Hansen P, Welch KMA, eds.The Headaches. 2nd ed. Philadel-phia, Pa: Lippincott Williams & Wilkins; 2000:627-634.
2.Schoenen J, Wang W. Tension-type headache. In: Goadsby PJ, Silberstein SD, eds.Headache. Boston, Mass: Butterworth-Heinemann; 1997:177-200.
3.Holroyd K, Stensland M, Lipchik G, Hill K, O’Donnell F, Cordingley G. Psychosocial correlates and impact of chronic tension-type headaches.Headache. 2000; 40:3-16.
4.Olesen JC for the Headache Classification Com-mittee of the International Headache Society. Classi-fication and diagnostic criteria for headache disor-ders, cranial neuralgias, and facial pain.Cephalalgia. 1988;8(suppl 7):1-96
5.Schwartz BS, Stewart WF, Simon MS, Lipton RB. A population-based study of the epidemiology of ten-sion-type headache.JAMA. 1998;279:381-383.
6.Rasmussen BK, Lipton RB. Epidemiology of tension-type headache. In: Olesen J, Tfelt-Hansen P, Welch KMA, eds.The Headaches. 2nd ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2000:545-550.
7.Granella F, Farina S, Malferrari G, Manzoni GC. Drug abuse in chronic headache: a clinico-epidemiologic study.Cephalalgia. 1987;7:15-19.
8.Diamond S, Dalessio DJ.The Practicing Physi-cian’s Approach to Headache. 4th ed. Baltimore, Md: Williams & Wilkins; 1992.
9.Couch JR. Medical management of recurrent ten-sion-type headache. In: Tollison CD, Kunkel RS, eds.
Headache Diagnosis and Treatment. Baltimore, Md: Wiliams & Wilkins; 1993:151-162.
10.Couch JR, G. M. Prophylactic pharmacotherapy. In: Olesen J, Tfelt-Hansen P, Welch MA, eds.The Headaches. New York, NY: Raven Press, Ltd; 1993.
11.Mathew NT, Bendtsen L. Prophylactic pharma-cotherapy of tension-type headache. In: Olesen J, Tfelt-Hansen P, Welch KMA, editors.The Headaches. 2nd ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2000:667-774.
12.Kunkel RS. Diagnosis and treatment of muscle con-traction (tension-type) headaches.Med Clin North Am. 1991;75:595-603.
13.Pfaffenrath V, Diener HC, Isler H, et al. Efficacy and tolerability of amitriptylinoxide in the treatment of chronic tension-type headache: a multi-centre con-trolled study.Cephalalgia. 1994;14:149-155.
14.Gobel H, Hamouz V, Hansen C, et al. Chronic ten-sion-type headache: amitriptyline reduces clinical head-ache-duration and experimental pain sensitivity but does not alter pericranial muscle activity readings.Pain. 1994;50:241-249.
15.Bendtsen L, Jensen R, Olesen J. A non-selective (amitriptyline), but not a selective (citalopram), sero-tonin reuptake inhibitor is effective in the prophylac-tic treatment of chronic tension-type headache.J Neu-rol Neurosurg Psychiatry. 1996;61:285-290.
16.Holroyd KA, Martin PR. Psychological treat-ments for tension-type headache. In: Olesen J, Tfelt-Hansen P, Welch KMA, eds.The Headaches. 2nd ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2000: 643-649.
17.Blanchard EB. Psychological treatment of benign headache disorders.J Consult Clin Psychol. 1992;60: 537-551.
18.Bogaards MC, ter Kuile MM. Treatment of re-current tension headache: a meta-analytic review.Clin J Pain. 1994;10:174-190.
19.Holroyd KA, Penzien DB. Client variables in the behavioral treatment of recurrent tension headache: a meta-analytic review.J Behav Med. 1986;9:515-536.
20.Blanchard EB, Appelbaum KA, Guarnieri P, et al. Two studies of the long-term follow-up of minimal-therapist contact treatments of vascular and tension headache.J Consult Clin Psychol. 1988;56:427-432.
21.Blanchard EB, Appelbaum KA, Guarnieri P, Mor-rill B, Dentinger MP. Five-year prospective follow-up on the treatment of chronic headache with biofeed-back and/or relaxation.Headache. 1987;27:580-583.
22.Blanchard EB. Long-term effects of behavioral treatment of chronic headache.Behav Ther. 1987; 23:375-385.
23. McCrory DC, Penzien DB, Hasselblad V, Gray RN. Evidence Report:Behavioral and Physical Treat-ments for Tension-Type and Cervicogenic Head-ache. DesMoines, Iowa: Foundation for Chiropractic Education and Research; 2001. No. 2085.
24.Holroyd KA, Nash JM, Pingel JD, Cordingley GE, Jerome A. A comparison of pharmacological (amitrip-tyline HCl) and nonpharmacological (cognitive-behavioral) therapies for chronic tension headaches.
J Consult Clin Psychol. 1991;59:387-393.
treat-ment of recurrent headache disorders.J Consult Clin Psychol. In press.
26.Silberstein SD, Lipton RB, Goadsby PJ. Head-ache in Clinical Practice. Oxford, England: Isis Medi-cal Media Ltd; 1998.
27.Solomon S. Psychotropic drug therapy for tension-type headaches. In: Olesen J, Shoenen J, eds. Tension-Type Headache: Classification, Mechanisms, and Treatment. New York, NY: Raven Press, Ltd; 1993.
28.Giammarco R, Edmeads J, Dodick D.Critical De-cisions in Headache Management. Hamilton, On-tario: BC Decker, Inc; 1998.
29.Robbins LD.Management of Headache and Head-ache Medications. 2nd ed. New York, NY: Springer; 2000.
30.Peveler R, George C, Kinmonth A, Cambell M, Thompson C. Effect of antidepressant drug counsel-ling and information leaflets on adherence to drug treatment in primary care: randomised controlled trial.
BMJ. 1999;319:612-615.
31.Tobin DL, Holroyd KA, Baker A, Reynolds RVC, Holm JE. Development and clinical trial of a minimal contact, cognitive-behavioral treatment for tension headache.Cogn Ther Res. 1988;12:325-339.
32.Holroyd KA, French DJ, Nash JM, Tobin DL, Ech-elberger-McCune RL. Stress management for tension headaches: a treatment program for controlling head-aches. Athens: Ohio University Headache Project; 1995.
33.Bernstein DA, Borkovec TD.Progressive Relax-ation Training: A Manual for the Helping Profes-sions. Champaign, Ill: Research Press; 1973.
34.Bernstein DA, Carlson CR. Progressive
relax-ation: abbreviated methods. In: Lehrer P, Woolfolk RL, eds.Principles and Practice of Stress Management. New York, NY: Guilford Press; 1993:53-85.
35.Holroyd KA, Andrasik F. A cognitive-behavioral approach to recurrent tension and migraine head-ache. In: Kendall PE, ed.Advances in Cognitive-Behavioral Research and Therapy. New York, NY: Aca-demic Press; 1982:276-320.
36.Beck AT. Cognitive approaches to stress. In: Le-hrer PM, Woolfolk RL, eds.Principles and Practice of Stress Management. New York, NY: Guilford Press; 1993:333-371.
37.Goldfried MR, Davison GC.Clinical Behavior Therapy. 2nd ed. New York, NY: John Wiley & Sons, Inc; 1994.
38.D’Zurilla TJ. Problem-solving training for effec-tive stress management and prevention.J Cogn Psy-chother. 1990;4:327-354.
39. D’Zurilla TJ. Clinical stress management. In: Nezu AM, Nezu CM, eds.Clinical Decision Making in Be-havior Therapy: A Problem-solving Perspective. Cham-paign, Ill: Research Press; 1989:371-400.
40.Blanchard EB, Andrasik F.Management of Chronic Headaches: A Psychological Approach. Elmsford, NY: Pergamon Press; 1985.
41.Blanchard EB, Andrasik F, Neff DF. Social valida-tion of the headache diary.Behav Ther. 1981;12:711-715.
42.McKee M. Headache diary. In: Tollison CD, Kunkel RS, eds.Headache Diagnosis and Treatment. Balti-more, Md: Williams & Wilkins; 1993:321-327.
43.Coyne L, Sargent J, Segerson J, Obourn R.
Rela-tive potency scale for analgesic drugs: use of psycho-physical procedures with clinical judgments. Head-ache. 1976;16:70-71.
44.Jacobson GP, Ramadan NM, Aggarwal SK, New-man CW. The Henry Ford Hospital Headache Disabil-ity Inventory (HDI).Neurology. 1994;44:837-842.
45.Jacobson GP, Ramadan NM, Norris L, Newman CW. Headache Disability Inventory (HDI): short-term test-retest reliability and spouse perceptions.
Headache. 1995;35:534-539.
46.Blanchard EB, Schwarz SP. Clinically significant changes in behavioral medicine.Behav Assess. 1988; 10:171-188.
47.Hochberg Y. A sharper Bonferroni procedure for multiple tests of significance.Biometrika. 1988;75: 800-802.
48.Edmeads J, Findlay H, Tugwell P, Pryse-Phillips W, Nelson RF, Murray TJ. Impact of migraine and ten-sion-type headaches on life-style, consulting behav-ior, and medication use: a Canadian population sur-vey.Can J Neurol Sci. 1993;20:131-137.
49.Cohen J.Statistical Power Analysis for the Be-havioral Sciences. Hillsdale, NJ: Lawrence Erlbaum As-sociates; 1988.
50.Hollon SD, DeRubeis J. Placebo-psychotherapy combinations: inappropriate representations of psy-chotherapy in drug-psypsy-chotherapy comparative tri-als.Psychol Bull. 1981;90:467-477.
51.Frank E, Kupfer DJ. Does a placebo tablet affect psychotherapeutic outcome? results from the Pitts-burgh study of maintenance therapies in recurrent de-pression.Psychother Res. 1992;2:102-111.