1
Willpower Depletion and Hand Hygiene in Emergency Medicine
By
Daniel Wurzelmann
A Master’s Paper submitted to the faculty of the University of North Carolina at Chapel Hill
in partial fulfillment of the requirements for the degree of Master of Public Health in
the Public Health Leadership Program
Chapel Hill
2012
Advisor
Date
Second Reader
2
Table of Contents:
Abstract of Master’s Paper 3
Systematic Review:
Abstract 4
Manuscript 5
Tables 19
Figures 21
Appendix 22
References 23
Research Design Paper:
Abstract 27
Manuscript 28
Figures 39
Tables 43
3
Abstract of Master’s Paper
Psychology research suggests that willpower functions like a muscle and tires with use;
as willpower is depleted, we have less available for other, unrelated tasks that also require
willpower. Recent research has found that people demonstrate declines in performance in various
areas as they work hard without breaks. To date, there is minimal research investigating evidence
of willpower decline in a medical context. One candidate as a metric for finding evidence of
willpower decline is hand hygiene. Performance of hand hygiene requires conscious mental
effort on the part of the physician, suggesting it is subject to willpower depletion. Evidence
suggests that the low hand hygiene rates in medicine are responsible for nosocomial infections.
This paper consists of two distinct parts: a systematic review and an original manuscript
describing plans for an observational research study. The systematic review assesses the current
literature on hand hygiene to determine whether there is evidence of a willpower depletion effect
by examining hand hygiene rates and performance in the beginning and end of a shift. This
review found only three studies that met inclusion criteria. Although these studies did suggest
some mild effect of willpower depletion, all three studies were subject to significant limitations
related to measurement of time or hand hygiene.
The original manuscript lays out a design for an observational study of hand hygiene,
comparing hand hygiene rates in the beginning and end of a shift. It is to take place in an
Emergency Department and will use criteria for of hand hygiene indications defined by the
World Health Organization. If the study finds evidence of willpower depletion in hand hygiene,
it suggests that other areas in medicine may be at risk of declining performance over the course
4
Systematic Review Abstract:
Introduction: Hand hygiene practice among physicians has been consistently poor and intractable
in the face of improvement efforts. One potentially contributing factor is depletion of willpower,
which would be expected to present as declining hand hygiene performance over a shift of work.
The goal of this paper is to systematically review hand hygiene literature to determine if any
decline in hand hygiene performance has been noted over the course of a shift.
Methods: Medline and Web of Science were searched for studies examining a correlation
between hand hygiene and time, and a separate search for systematic review articles examining
the relationship between time and hand hygiene was also conducted to identify additional
articles. To be included, articles must have assessed hand hygiene practice at different times of
day. Articles meeting criteria for inclusion were graded for quality by evaluating risk of
measurement bias.
Results: Three studies met inclusion criteria, but only one was specifically designed to compare
hand hygiene performance at the beginning and end of the shift. Although the studies suggested
some decline of hand hygiene during a shift, all studies had methodological limitations that
prevented robust assessment of evidence of willpower depletion.
Conclusion: There currently is insufficient research to assess whether willpower depletion
manifests itself as declining hand hygiene performance over the course of a shift. Further
research into performance variation over the course of a shift may provide valuable insight into
5
Introduction:
A recent study found that for prisoners who committed equivalent crimes, the time of day
at which the prisoner’s case was heard was one of the most important factors in determining
whether the prisoner was granted parole by a judge.1 Prisoners whose similar cases were heard at
the beginning of the day or after a refreshing snack break had about a 65% chance of parole.
Chances of parole declined sharply thereafter, reaching a low of about 10% for comparable cases
heard just before scheduled snack breaks and just before finishing for the day.
The authors attribute this surprising discrepancy to a phenomenon dubbed “decision
fatigue,” suspecting that the judges became mentally fatigued after making repeated decisions,
and then tended to make the convenient choice of denying parole rather than grapple with the
difficult decision to grant parole, even though cases were alike. Decision fatigue is a form of
willpower depletion in that decision making is one of various types of tasks that can deplete
one’s supply of self-control, which is required to perform effortful tasks. Research has found that
willpower or self-control is like a muscle: it tires with use, but can be restored to full
functionality after a break,2 which is why the parole judges invested greater consideration of
cases heard at the beginning of the day or after breaks. Various classes of activities have been
found to exhaust willpower. Examples of such activities include cognitive processes, volition,
and social processing, as well as controlling one’s emotions, attention, impulses, and thoughts.3
Some of these taxing activities are frequently repeated tasks among medical
professionals, such as making patient care decisions or controlling emotions while dealing with
difficult patients. The strength model of self-control predicts that use of willpower in any task
6
if they are different in nature.2,4 It would therefore be expected that as medical professionals
work through the day, often with limited breaks, their supply of self-control would gradually
decline.
If health care providers are suspected to experience willpower depletion, the next step is
identify easily measurable areas of performance that are likely to show evidence of decline
during a shift. One such task likely subject to supply of self-control is hand hygiene, which
involves controlling one’s thoughts to remember to clean hands before and after seeing a patient
or performing certain care tasks. There is strong evidence that many of the 1.7 million
nosocomial infections per year in the United States5 are related to poor hand hygiene.6, 7 Despite
this evidence, hand hygiene rates have remained low among health care providers, with one
systematic review finding a median adherence of 40% for all health care workers, and among
physicians, the rate has consistently been found to be lower, with the same systematic review
finding a median compliance rate of 32%.8
Examining hand hygiene through the perspective of willpower depletion may help to
shed some light on why many interventions to improve hand hygiene rates have generally been
unsuccessful9 and hand hygiene rates have remained low. This systematic review seeks to
evaluate the current literature to determine whether there is presently any evidence of declining
hand hygiene performance over the course of a shift of medical work, consistent with the model
of willpower depletion.
Methods
7
PubMed and Web of Science were searched for studies including the following
keywords: fatigue, mental fatigue, workload, tired, tiredness, sleeplessness, daytime, end of shift,
beginning of shift, night shift, sleep deprivation, evening shift, morning shift, handwashing, hand
washing, hand hygiene, hand disinfection, and hand decontamination. Details of the search
strategies are shown in Appendix 1. Based on this initial search, it became clear that the
relationship between time and hand hygiene, particularly with regards to the time into the shift,
was rarely assessed as a primary outcome, and if time was assessed at all, it was not often
included in the title or even the abstract of most articles. Because search engines use keywords,
titles, and abstracts but not full text to retrieve relevant articles, another search was then
performed to identify systematic review articles that assessed the literature for factors affecting
hand hygiene in order to manually extract any studies assessing a relationship of hand hygiene
and time. This search for systematic reviews was conducted on PubMed using the MeSH term
“handwashing” and limiting the search to systematic reviews in English. Both searches were
limited to English language studies published and indexed on the search databases before May 1,
2012.
Article selection:
Articles were reviewed by titles first, and then by abstract if necessary. To be included,
studies must have been published in peer-reviewed journals, used prospective observational
designs, and compared hand hygiene performance at different times of the day. In addition to
examining hand hygiene at different times of the day, studies must have evaluated for change in
performance of hand hygiene within the course of a shift. Only studies published in English were
8
scanned article titles and then read abstracts of relevant articles. The reviewer was not masked to
names of investigators or publication during assessment.
Data extraction:
One author [DW] reviewed all studies, extracting information on how hand hygiene
compliance was defined and measured, the type of health care worker (HCW) studied, setting of
the study, time frames assessed, and study results.
Quality assessment:
Because only observational research was included in this review, studies were assessed
primarily for measurement bias to determine whether measurements of hand hygiene rates in
included studies were equal, reliable and valid. Studies were assessed for methods of measuring
hand hygiene, definition of hand hygiene opportunity, training of hand hygiene observer,
inter-rater reliability where applicable, and whether observation was covert. For each study, this
combination of factors were considered as a whole to estimate how accurately hand hygiene rates
were measured, and then a quality rating of poor, fair, or good was given to each study.
Results
Search Results:
The initial search for observational studies assessing a relationship between hand hygiene
and time provided 102 citations for review, including 33 from PubMed and 69 different citations
from Web of Science. A second search to find systematic reviews assessing factors affecting
9
reviews were deemed relevant. Of these five reviews, only one systematic review8 was found to
assess the relationship of time and hand hygiene, but this source provided an additional six
citations for review. While reviewing literature on hand hygiene, one additional article10 was
incidentally found to include assessment of time and hand hygiene and was also included in the
review process although it did not come up in any systematic searches, most likely because it did
not mention time in the title or abstract.
Of the total of 109 citations found, titles and abstracts were scanned and 94 citations were
removed from consideration due to irrelevance. A flow chart of the review process is found in
Figure 1. The reviewer examined the full text of the remaining 15 articles and two more were
removed from consideration; one did not assess the relationship of time and hygiene11 and the
other was an assessment of contact precautions rather than hand hygiene.12
Of the remaining 13 studies, ten10, 13-21 only assessed hand hygiene performance by
comparing rates in different shifts, such as hand hygiene rate for the night shift compared to the
day shift. This type of comparison does not allow for evaluation of evidence of decision fatigue
and so these studies were also excluded, leaving three studies22-24 for final inclusion in this
review. Table 1 shows data extraction and evidence from each study, while Table 2 shows how
the quality rating for each study was derived.
Study Characteristics:
Lipsett 2001
10
The Lipsett study was conducted in a 14-bed surgical intermediate care unit of a teaching
hospital in the United States. Hand hygiene habits of various health care workers were assessed,
including nurses (68.0% of total observations), and nursing support personnel (21.4%), and
physicians (10.6%). Four different time frames were compared: 7am-11am, 11am-3pm,
3pm-7pm, and 7pm-11pm. The article text does not indicate if these times corresponded with the
beginning or end of shifts for any of the health care workers.
Results
This study found no statistically significant difference in hand hygiene rates between the
four time periods measured. The 7am-11am period had hand hygiene compliance of 46%;
11am-3pm had compliance of 43%; 11am-3pm-7pm had compliance of 44%; and 7pm-11pm had compliance
of 42%.
Quality
The Lipsett study used hand hygiene criteria established by Larson25 and Rotter.26 The authors describe “three trained unidentified individuals” as the observers of hand hygiene, but do
not specify who these individuals are. The training took place in a pilot trial, during which the
authors also mention that “reliability of observers was assessed and confirmed,” however they do
not provide any details or offer inter-rater reliability statistics. Hospital staff were unable to
identify those doing hand hygiene observation, but staff were aware of the ongoing research
project.
Overall assessment of quality of data gathered is fair. Many details of the observers and
11
staff were aware of a hand hygiene research project, it is unlikely that this knowledge had much
effect on hand hygiene given the difficulties of increasing hand hygiene rates.9
Evidence of Decision Fatigue or Willpower Decline
This study is not well designed to assess for evidence of decision fatigue as manifested
by hand hygiene rates for several reasons. One limitation is that the study does not explicitly
assess hand hygiene rates over the course of a shift. It is likely that many workers do arrive in the
early morning and finish work in the afternoon, and so some decline in hand hygiene rates would
be expected from the 7am-11am observation period compared to the 11am-3pm observation
period. This difference, however, was small (46% vs 43%) and not statistically significant.
Because this study included a mixture of health care personnel, some may come into work at
different times or experience other factors that affect willpower, making it difficult to compare
time periods assessed by this study. The study did not control for other variables that may
deplete willpower in analyzing hand hygiene rates. Another drawback of this study is that
physicians, who make many medical decisions in a day and may thereby be more subject to
additional mental fatigue, made up only a small proportion of this study (10.6% of observations).
A final limitation of this study is that the quality of measurement of hand hygiene rates is only of
fair quality, due to lack of information about details of methodology.
Chudleigh 2005
Design
The Chudleigh study examined quality of hand hygiene in the neonatal intensive care
units (NICU) of six hospitals. Unlike other studies, this one evaluated hand hygiene technique
12
nurses. Hand hygiene technique was intentionally assessed five times for each nurse at the
beginning and end of shifts, both standard 8-hour shifts and long 12-hour shifts.
Results
For the long 12-hour shift, the study reports that nurses were significantly more likely to
spend over 10 seconds decontaminating their hands at the beginning of the shift than at the end
of the shift although exact figures are not provided. Additionally, more surfaces of the hand were
decontaminated at the beginning of long shifts than at the end, and hand drying was also better at
the beginning rather than end of long shifts. However no such differences were found for the
beginning and end of the 8-hour shift.
Quality
The researchers developed their own scoring system for evaluating hand hygiene
technique. No mention was made of whether this scoring system was validated. One research
assistant collected all of the data, but there was no mention of training for data collection or any
pilot period. Furthermore, it was not explicitly stated whether hand hygiene observation was
covert or not; however, wording of the article suggests that data collection was not discreet.
The overall quality rating given to this study is poor. Evaluating hand hygiene technique
presents many challenges and validation and reliability of the scoring instrument is important to
establish. The scoring instrument included variables such as hand hygiene product, duration of
cleansing, number of surfaces of the hand cleaned, water tap use, hand drying, and bin use.
Accurately documenting all of these variables for a single event within a short period of time
may be difficult. It is unclear whether the observer had knowledge of the expected results of the
13
appear to control for whether a nurse was using hand sanitizer or washing hands in the analysis
of time spent cleaning hands. This variable is especially important to control for as there could
be variation in time between washing compared to using hand sanitizer.
Evidence of Decision Fatigue or Willpower Decline
This study does find significant differences between hand hygiene performance at the
beginning and end of long shifts, which is evidence consistent with a decline in willpower.
However, the lack of any significant difference at the beginning and end of standard 8-hour shifts
does not support the willpower hypothesis. It is possible that the extra four hours of nursing work
are required in order to see a noticeable change in performance, or perhaps the metric of hand
hygiene technique is not sensitive enough to notice a change for shorter shifts. However, the
most significant limitation of this study is concern for measurement bias, as discussed in the
Quality section. While the study may have uncovered evidence of declining willpower over the
course of a shift, more rigorous methodology is needed to verify these results.
Cheng 2011
Design
This study took place in a 6-bed neurosurgical intensive care unit. The study focused on
21 subjects, 17 of whom were nurses (81%), along with 3 physiotherapists and 1 healthcare
assistant. No physicians were included in the study. Unlike the previous studies, which used
human observers, the Cheng study utilized an electronic monitoring system, and assessed hand
hygiene in two-hour intervals throughout the day. These two-hour intervals did not match up
14
Results
Only one of the two-hour intervals had a significantly different rate of hand hygiene
compliance than the others. The period from 12pm-2:00pm had significantly lower compliance
(21.3%) than all other periods of the day. Other periods ranged from a high of 47.8% compliance
from 2:00am to 4:00am to a low of 32.7% compliance from 8:00am to 10:00am. For reasons that
are not explained, no data were reported for 4am-6am (end of night shift).
Quality
This study used an electronic hand hygiene monitoring system to collect data on hand
hygiene compliance. Electronic sensors were set up at the patient bed and also at hand hygiene
stations. Health care workers wearing an electronic badge are detected when they approach a
patient bed or activate a soap or alcohol dispenser. This system is designed to detect hand
hygiene opportunities before and after touching a patient; however, it cannot detect other
instances in which hand hygiene is required, such as after moving from a contaminated area on a
patient (e.g. urinary catheter) to a clean area (e.g. IV site).
This electronic monitoring system was tested and calibrated in a pilot trial before collecting
useable data. An infection control nurse was trained using the WHO “5 Moments of Hand
Hygiene”27
to assess validity of the electronic monitoring system. The observer conducted four
20-minute observations during one week, all which happened between 10:00am and 11:15am. In
order to assess accuracy of the electronic monitoring system, the observer also only counted
hand hygiene opportunities before and after touching a patient. Results from the human observer
and electronic observer were substantially different, with the infection control nurse noting 69
15
only detected 48 hand hygiene opportunities from 13 health care workers during the same
observation period. The nurse observer found 95.6% hand hygiene compliance while the
electronic system counted 88.9% hand hygiene compliance. A kappa value for inter-rater
reliability was not reported.
The quality rating given to this study is poor due to high risk for measurement error.
There was not strong agreement between the infection control nurse and electronic monitoring
system, which appeared to miss many hand hygiene opportunities despite using the same criteria.
The reliability and precision of the electronic system was not convincingly established. Another
shortcoming was the small sample used for validation with a human observer; only observing
four times for 20 minutes each during a window of 10:00am to 11:15am leaves monitoring data
for most of the day without validation. It is conceivable that that certain times of the day may
have different levels of traffic in patient rooms and that sensitivity of the electronic instrument
may vary, particularly when multiple health care workers are in the room.
Evidence of Decision Fatigue or Willpower Decline
This study did not directly assess hand hygiene performance at the beginning and end of
shifts, making it difficult to assess for evidence of decision fatigue. However, the authors did
provide information on when shifts start and end, allowing for some evaluation. The morning
shift, from 6:30am-1:45pm can be roughly correlated with the 6:00am to 8:00am interval as the
beginning of the shift and the 12:00pm-2:00pm interval as the end of the shift. Hand hygiene
compliance did decrease from 39.5% to 21.3% over this time period, a statistically significant
change. However, the afternoon shift, from 1:45pm-8:45pm did not show any similar significant
16
intervals. One possible reason for the lack of significant decline is that these intervals are only
assessing a six-hour difference, rather than the eight-hour difference in the morning shift.
Another factor that could be contributing is that it is unclear if all health care workers in the
study had the exact same shift schedule, or if the reported shifts are only for nurses, who made
up 81% of the study population. As the day goes on, it is more likely that shifts of different
professionals are staggered and a mixture of fresh and tired health care workers are seeing
patients, which could contribute to inconsistent hand hygiene rates. Additionally, the hand
hygiene rates are not adjusted for other variables that might affect hand hygiene, such as
workload, which could also contribute to noise in the data. Unfortunately, assessing the night
time shift for evidence of willpower depletion is not possible because no compliance data were
reported for the 4:00am to 6:00am time interval.
Although there is some evidence of waning willpower manifesting itself as declining
hand hygiene in the morning shift, it was not observed in the afternoon shift. Another limitation
of this study was the significant potential for measurement bias; it is difficult to feel confident
that the electronic system was consistently measuring all hand hygiene opportunities and
cleansings to calculate accurate compliance data.
Discussion:
The major finding of this systematic review is that there is currently insufficient research
to conclusively assess whether willpower depletion manifests itself as declining hand hygiene
performance over the course of a shift of medical work. The most significant reason for the lack
17
the beginning and end of shifts. Only the Chudleigh 2005 study intentionally compared and
analyzed hand hygiene practice in the beginning and end of the shift, whereas the two other
studies included in this review were not designed to assess performance across the shift and
evidence of decline could only be roughly inferred from what limited data were collected. There
is some suggestion of willpower depletion in the studies assessed, but more purposeful study of
the topic is needed.
A significant limitation of this systematic review is that it was very difficult to locate
studies that assess hand hygiene compliance with respect to some proxy measure of willpower
depletion, such as time since the beginning of a shift. The initial PubMed and Web of Science
searches only unveiled 10 of the 15 articles that met criteria for full text review, with four other
articles coming from a hand search of a systematic review and another article discovered
incidentally. Of the three articles that met final inclusion criteria, only the Lipsett 2001 study was
not retrieved by the search strategy and instead found via a hand search of a systematic review.8
Because the Lipsett article did not find a statistically significant difference, the authors did not
mention analysis by units of time in the title, abstract, or keywords, which is why it didn’t appear
in search results.
Some potential exists that other undiscovered studies failed to find statistically significant
results by unit of time and thus were not retrieved by the search strategy. However, it seems
improbable that any unfound studies exist that would provide high quality evidence for or against
willpower depletion in hand hygiene practices given the imprecise measurement of time in the
studies that were found. Additionally, willpower research did not take off until the late 1990s and
was not widely applied to areas outside psychology laboratories until the mid-2000s, so it is
18
Hand hygiene practice makes for a useful dependent variable in that it can be relatively
easily studied and has been linked to nosocomial infections.6, 7 A recent study found that the
number of colonies of bacteria on nurses’ hands significantly increased pre-shift to post-shift,28 suggesting that nurses’ hands become dirtier and potentially more dangerous as a shift wears on.
If nurses or other health care workers have more infectious hands and are less likely to clean
them at the end of shifts, this combination could lead to more hospital acquired infections.
Beyond hand hygiene, willpower depletion offers a new psychological paradigm for
assessing variations in medical practice, such as rates of admissions and medical errors, ordering
expensive imaging tests, prescribing medications, and much more. Investigating these various
areas of practice for evidence of willpower depletion will require precise data on timing of
events and carefully controlling for a litany of other variables. Although there are challenges to
evaluating willpower depletion in the real-world clinical setting, it holds great potential for
19
Table 1: Evidence Table
Author Year Types of HCW
studied Location Time frames assessed
Results (percent compliant on HH opportunities)
Evidence of Decline in Performance over
Course of Shift
Lipsett 2001
68% nurses, 21% nursing support personnel, 11% physicians teaching hospital, surgical intermediate 7am-11am; 11am-3pm; 3pm-7pm; 7pm-11pm
No significant difference: 7am-11am: 46%; 11am-3pm: 43%; 3pm-7pm: 44%; 7pm-11pm: 42%
Not statistically significant
Chudleigh 2005 100% nurses
multiple hospitals; NICU's only
assessed nurses at beginning and end of shifts; standard (8 hr) and long (12 hr) shifts included
Nurses spent significantly more time cleaning hands at beginning than at end of a long (12hr) shift. No significant difference was found for a standard (8 hr) shift. Yes
Cheng 2011
81% nurses, 14% physiotherapists, 5% health care assistants
neurosurgical ICU
assessed in two-hour intervals from 6am through 4am.
No significant difference between morning, afternoon, and night shifts. However, 12pm-14:00 interval (at end of first shift) had significantly lower compliance than rest of day: 12:00 to 14:00 (21.3%); 0:00 to 2:00 (38.9%) 2:00 to 4:00 (47.8%); 6:00 to 8:00 (39.5%, 95%); 8:00 to 10:00 (32.7%, 95%); 10:00 to 12:00 (37.6%); 14:00 to 16:00 (37.1%); 16:00 to 18:00 (35.0%); 18:00 to 20:00 (39.3%). No data were reported for 4am-6am (end of night shift).
20
Table 2: Study Quality
Author Year Criteria or Definition of Hand Hygiene Opportunity
Hand Hygiene Observer(s)
Training for HH Observer Covert Observation? Interrater Reliability (if applicable) Quality Rating: (good, fair, poor) Lipsett 2001
Criteria established by Larson (1995) and Rotter (1996)
3 "trained unidentified individuals"
trained in pilot trial
"unidentifie d" observers, but staff aware of the project
"reliability of observers assessed and confirmed" in a pilot trial, but no specifics given Fair
Chudleigh 2005
Developed evaluative criteria for quality of handwashing rather than evaluating rate of hand hygiene. Criteria not validated. one research assistant, not specified none mentioned unclear;
unlikely NA Poor
Cheng 2011
Before and after touching patient noted with electronic monitoring with observer validation.
infection control nurse
21
22
Appendix 1:
PubMed Search strategy:
("Fatigue"[Mesh] OR fatigue[ti] OR "Mental Fatigue"[Mesh] OR "Workload"[Mesh] OR
workload[ti] OR "Personnel Staffing and Scheduling"[Mesh] OR staffing[ti] OR "Sleep
Disorders, Circadian Rhythm"[Mesh] OR sleeplessness[ti] OR sleep[ti] OR daytime[tw] OR
"end of shift"[tw] OR "change of shift*"[tw] OR "shift change*"[tw] OR "night shift*"[tw] OR
"sleep deprivation"[tw] OR "evening shift*"[tw] OR “morning shift*”[tw]) AND
("Handwashing"[Mesh] OR "hand washing"[ti] or handwashing[ti] or "hand hygiene"[ti] OR
"hand disinfection"[ti] OR “hand decontamination”[ti]) Filters: English
Web of Science Search Strategy:
TS= ((Fatigue OR Mental Fatigue OR Workload OR tired OR tiredness OR sleeplessness OR
daytime OR end of shift OR beginning of shift OR night shift OR sleep deprivation OR evening
shift OR morning shift) AND (Handwashing OR hand washing OR hand hygiene OR hand
23
REFERENCES
1. Danziger S, Levav J, Avnaim-Pesso L. Extraneous factors in judicial decisions. Proc Natl
Acad Sci U S A. 2011;108(17):6889-6892. doi: 10.1073/pnas.1018033108.
2. Muraven M, Baumeister RF. Self-regulation and depletion of limited resources: Does
self-control resemble a muscle?. Psychol Bull. 2000;126(2):247-259.
3. Baumeister RF, Vohs KD, Tice DM. The strength model of self-control. Current directions in
psychological science. 2007;16(6):351-355.
4. Hagger MS, Wood C, Stiff C, Chatzisarantis NL. Ego depletion and the strength model of
self-control: A meta-analysis. Psychol Bull. 2010;136(4):495-525. doi: 10.1037/a0019486.
5. Klevens RM, Edwards JR, Richards CL,Jr, et al. Estimating health care-associated infections
and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122(2):160-166.
6. Larson E. A causal link between handwashing and risk of infection? examination of the
evidence. Infect Control. 1988;9(1):28-36.
7. Larson E. Skin hygiene and infection prevention: More of the same or different approaches?.
Clin Infect Dis. 1999;29(5):1287-1294. doi: 10.1086/313468.
8. Erasmus V, MSc, Daha T, Brug H, PhD, et al. Systematic review of studies on compliance
with hand hygiene guidelines in hospital care • . Infection Control and Hospital Epidemiology.
24
9. Gould DJ, Moralejo D, Drey N, Chudleigh JH. Interventions to improve hand hygiene
compliance in patient care. Cochrane Database Syst Rev. 2010;(9)(9):CD005186. doi:
10.1002/14651858.CD005186.pub3.
10. Venkatesh AK, Pallin DJ, Kayden S, Schuur JD. Predictors of hand hygiene in the
emergency department. Infect Control Hosp Epidemiol. 2011;32(11):1120-1123. doi:
10.1086/662374.
11. MacDonald A. Performance feedback of hand hygiene, using alcohol gel as the skin
decontaminant, reduces the number of inpatients newly affected by MRSA and antibiotic costs. J
Hosp Infect. 2004;56(1):56-63.
12. Afif W. Compliance with methicillin-resistant staphylococcus aureus precautions in a
teaching hospital. Am J Infect Control. 2002;30(7):430-433.
13. Lund S, Jackson J, Leggett J, Hales L, Dworkin R, Gilbert D. Reality of glove use and
handwashing in a community hospital. Am J Infect Control. 1994;22(6):352-357.
14. Watanakunakorn C, Wang C, Hazy J. An observational study of hand washing and infection
control practices by healthcare workers. Infection Control and Hospital Epidemiology.
1998;19(11):pp. 858-860.
15. Pittet D, Mourouga P, Perneger TV, and the Members of the Infection Control Program.
Compliance with handwashing in a teaching hospital. Annals of Internal Medicine.
25
16. Sharir R, Teitler N, Lavi I, Raz R. High-level handwashing compliance in a community
teaching hospital: A challenge that can be met!. J Hosp Infect. 2001;49(1):55-58. doi:
10.1053/jhin.2001.1049.
17. Santana SL, Furtado GH, Coutinho AP, Medeiros EA. Assessment of healthcare
professionals' adherence to hand hygiene after alcohol-based hand rub introduction at an
intensive care unit in sao paulo, brazil. Infect Control Hosp Epidemiol. 2007;28(3):365-367. doi:
10.1086/510791.
18. Traore O, Hugonnet S, Lubbe J, Griffiths W, Pittet D. Liquid versus gel handrub
formulation: A prospective intervention study. Crit Care. 2007;11(3):R52. doi: 10.1186/cc5906.
19. Duggan JM, Hensley S, Khuder S, Papadimos TJ, Jacobs L. Inverse correlation between
level of professional education and rate of handwashing compliance in a teaching hospital.
Infection Control and Hospital Epidemiology. 2008;29(6):pp. 534-538.
20. Venkatesh AK, Lankford MG, Rooney DM, Blachford T, Watts CM, Noskin GA. Use of
electronic alerts to enhance hand hygiene compliance and decrease transmission of
vancomycin-resistant enterococcus in a hematology unit. Am J Infect Control. 2008;36(3):199-205. doi:
10.1016/j.ajic.2007.11.005.
21. Sahay S, Panja S, Ray S, Rao BK. Diurnal variation in hand hygiene compliance in a tertiary
level multidisciplinary intensive care unit. Am J Infect Control. 2010;38(7):535-539. doi:
26
22. Lipsett PA. Handwashing compliance depends on professional status. Surgical infections.
2001;2(3):241-245.
23. Chudleigh J, Fletcher M, Gould D. Infection control in neonatal intensive care units. J Hosp
Infect. 2005;61(2):123-129. doi: 10.1016/j.jhin.2005.02.017.
24. Cheng VCC, Tai JWM, Ho SKY, et al. Introduction of an electronic monitoring system for
monitoring compliance with moments 1 and 4 of the WHO "my 5 moments for hand hygiene"
methodology. Bmc Infectious Diseases. 2011;11:151. doi: 10.1186/1471-2334-11-151.
25. Larson EL. APIC guideline for handwashing and hand antisepsis in health care settings. Am J
Infect Control. 1995;23(4):251-269.
26. Rotter M. Hand washing and hand disinfection. In: Mayhall C, ed. Hospital Epidemiology
and Infection Control. Baltimore: Williams and Wilkins; 1996:1052-1068.
27. Pittet D, Allegranzi B, Boyce J. The world health organization guidelines on hand hygiene in
health care and their consensus recommendations. World Health. 2009;30(7):611-622.
28. Findik UY, Otkun MT, Erkan T, Sut N. Evaluation of handwashing behaviors and analysis of
27
Research Design Abstract:
Introduction & Background: Willpower acts like a muscle and tires with use. It is expected that
effortful tasks will show declining performance as willpower is depleted. We expect that rates of
hand hygiene among emergency room physicians will decrease over the course of a shift.
Methods: Attending physicians will be recruited to participate in a study monitoring their
“interactions” in the emergency room. Two medical student observers will shadow the
physicians for the first two and last two hours of their shift, covertly recording hand hygiene
compliance using the WHO “5 Moments of Hand Hygiene” criteria. Additionally, the students
will record the physicians’ total interactions and interruptions as potential mediating variables.
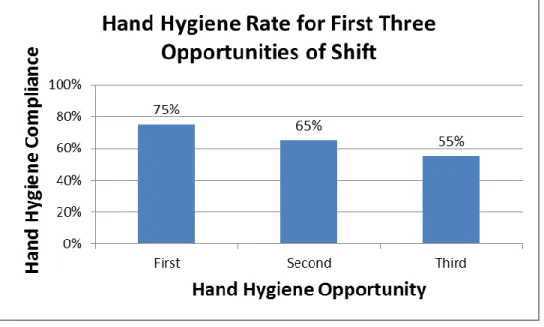
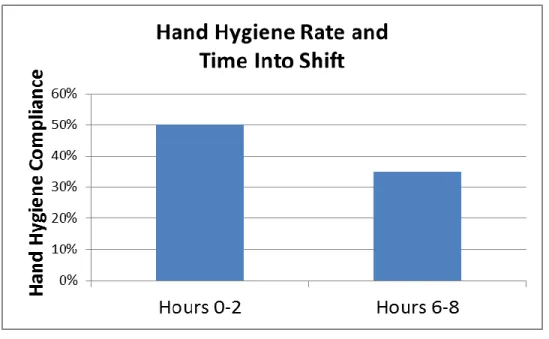
Anticipated Results: We expect that hand hygiene will demonstrate a significant decline from the
first two and last two hours of the shift. The study will be powered to detect a 15% difference
from 50% to 35% compliance. We also expect a more marked decrease in hand hygiene
compliance from the first three hand hygiene opportunities of the shift compared to the last three
hand hygiene opportunities.
Discussion: If this study does find that hand hygiene rates falls in a manner consistent with
willpower depletion, then it raises the question of whether willpower depletion is also harming
28
Introduction & Background:
Psychology research suggests that willpower or self-control is like a muscle - it tires with
use, but can be restored to full functionality after a break.1 Further experiments have
demonstrated that decision making is one strenuous task that depletes willpower, and as a person
makes repeated effortful decisions without a break, the person will demonstrate signs of
declining willpower and decision-making ability, a phenomenon captured in a term called
“decision fatigue.” 2
One recent example was a study that found that prisoners coming up for parole had a
wide range in likelihood of being paroled depending on the time of day that their cases were
heard, controlling for other variables. Prisoners whose cases were heard at the very beginning of
the day or right after judges returned from a break had about a 65% chance of receiving parole,
but the chance of being paroled dropped sharply thereafter, approaching a 10% chance just
before judges took a break.3 The authors suspect that the judges became mentally fatigued after
making repeated decisions, and then tended to make the convenient choice of denying parole
rather than grapple with the difficult decision to grant parole.
Given the dramatic potential consequences of declining willpower, we have decided to
search for evidence of decision fatigue in a medical context. We have selected the Emergency
Department as the setting due to its high cognitive demand on physicians.4 We plan to focus on
attending physicians as they have the final say in making decisions regarding patient care, and
evidence suggests that those burdened with final decision making power are the most subject to
29
There are many ways of measuring willpower depletion, from how long participants
tolerate pain or attempt to solve difficult math problems,2 to how likely they are to choose the
default option when choosing features on cars or suits.5 Self-control is defined as occurring
when a person has to exert control by the self over the self.1 Baumeister et al has proposed that
tasks requiring self-control can be organized into several spheres, such as controlling emotions,
attention, impulses, thoughts, cognitive processes, choice and volition, and social processing.6
The strength model of self-control predicts that use of willpower in any sphere will deplete a
common pool of willpower, leaving less self-control available for other tasks, even if they are in
a different sphere, a prediction supported by a recent meta-analysis.7 Hand hygiene likely falls
into the category of thought control; the physician must try to remember to clean his or her hands
before and after touching patients, before performing sterile procedures, or after contact with
bodily fluids. Previous studies of willpower in thought control have depleted willpower by
asking participants to avoid thinking of something, such as a “white bear”8,9; however, we expect that attempting to control thoughts to remember think of something, such as cleaning one’s
hands, will similarly be subject to willpower.
We hypothesize that decision fatigue will manifest itself as declining rates of hand
hygiene over the course of a shift in the Emergency Department. Hand hygiene rates among
physicians are lower than other health care workers, with an estimated median compliance of
32% for every hand hygiene opportunity according to a recent systematic review.10 Given the
poor hand hygiene rates, this act does not occur automatically, and instead appears to require
conscious effort on the part of the physician, making it a good candidate as a metric for
self-control. The relationship of time of day and hand hygiene has been studied before with mixed
30
been studied as a correlate of hand hygiene rates. Examining whether hand hygiene rates decline
during the course of a shift may also provide new insight as to why physicians consistently have
lower hand hygiene rates than other health care workers.
There are several other factors that have been shown to correlate with willpower
depletion that we will monitor in this study, including effort, perceived difficulty, negative
affect, subjective fatigue, and blood glucose levels.7 Although we will not monitor blood
glucose, we will ask about food and drink intake, and monitor for periods of relaxation while at
work, which have also been shown to restore willpower.11
Another metric for estimating willpower depletion is the number of interruptions and
interactions that the physician experiences over the course of the shift; busier shifts are correlated
with poorer hand hygiene.10 We therefore plan to track physicians’ interruptions and interactions
as these may mediate effects of willpower depletion on hand hygiene. Lastly, we expect that
hand hygiene rates will be influenced by some patient-level factors, such as whether a patient is
on contact precautions or has symptoms suggestive of a communicable infection and plan to
track these metrics as well.
Methods:
Study Participants:
We plan to recruit a minimum of 14 attending physicians (“attendings”) from the
University of North Carolina at Chapel Hill (UNC) Department of Emergency Medicine.
31
to the attendings’ electronic mail listserve. Attendings will then be contacted by a medical
student observer to set up observation sessions; attendings will be able to opt out of the study at
any time. Any attendings who participated in the design or approval of this project will not be
permitted to participate as knowledge of the study metrics may alter their behavior during
observation. In the event that we are unable to recruit 14 attending physicians, we plan to recruit
nurse practitioners (NPs) who work in the ED until we have 14 total subjects. The NPs will be
recruited in the same manner and treated in the same ways as the attending physicians.
Design:
In this observational study, two medical students [DW and MLP] will be shadowing
attendings to document their interactions and hand hygiene habits during a shift of work in the
UNC Emergency Department. We will attempt to select shifts for observation in such
proportions that our sample approximates the distribution of shifts in a typical week in the
Emergency Department. However, our first priority is shadowing the pool of participating
physicians broadly and equally to minimize effects of individual differences among physicians,
and our selection of shifts may therefore be limited by the fact that some physicians only work in
certain areas of the ED or certain shifts.
The observers will email attendings 1 week prior to a shift to request to shadow. If the
physician agrees to participate, the student will arrive to the shift, obtain written informed
consent from the physician, and then shadow the physician. The data collectors will quietly
follow the physicians to all locations except the restroom and in any instances in which the
32
herself and then return four hours later to collect data for the last two hours of the eight-hour
shift. Breaking up the shift into two-hour segments will allow us to capture data from the
beginning and end of the shift to assess hand hygiene rates without creating too much of a time
burden on the data collectors. At the end of the shift, the student observer will also ask the
physician a few questions to assess mood, fatigue, difficulty of shift, and enjoyment of shift.
After all data collection is complete, all participating physicians will be thanked and
emailed a debriefing document and a brief end-of-study survey to assess knowledge of and
attitudes towards hand hygiene.
Sample size:
Based on prior studies, we estimate hand hygiene compliance by these criteria will be
approximately 30-50%. Given this low initial compliance, we hope to capture an average
difference of 15% between the first two and last two hours of a shift. We have powered our study
to identify a 15% difference between 50% and 35%, with a power of 80% and a 1-tailed alpha of
0.05, estimating an effect size of 1.5. Using these parameters, we estimate that we will need 210
hand hygiene opportunities each in the first two and last two hours of a shift, for a total of 420
hand hygiene observations. At an estimated rate of 5 hand hygiene opportunities per 2 hours of
observation, we expect to shadow about 42 shifts total. Because we will be shadowing at least 14
ED physicians, we plan on shadowing each approximately 3 times.
Measurement tools:
Medical student observers will use the 2009 WHO criteria for hand hygiene
33
Technical Reference Manual,13” which is a guide for training health care personnel to determine
hand hygiene rates, as well as other training materials from the WHO, including video hand
hygiene scenarios. The students will engage in a practice observation session for further training,
and their inter-rater reliability will be determined by double-shadowing three additional shifts.
Further shifts may be double-shadowed if greater precision in the kappa value is needed.
Definitions for monitoring interruptions and interactions in the Emergency Department
are based upon a task analysis study performed in an academic emergency department.14
Interruptions will be defined as an event that shifts the attention of the attending for less than a
minute and does not cause the attending to switch tasks. Examples include a nurse saying hello
to the attending who is writing a patient note or the attending hitting “ignore” on an incoming
cell phone call. More complicated interruptions that last over 1 minute or result in an attending
changing to another activity will be defined as breaks in task. Examples include being called
away from note writing to see a patient or answering an incoming phone call.
Several moderating variables to be assessed in this study require definition. Signs of
contagiousness are any elements in the history or chief compliant of a patient that suggested a
contagious illness or increased likelihood of becoming contaminated by germs after examining
the patient. This information will only be gathered by direct observation of patient encounters by
the observer and will not include review of medical records or follow-up. Examples of signs of
contagiousness will include a history of diarrhea, cold symptoms, or abscess within the last 24
hours. Other symptoms such as rash or vomiting will be considered contagious if the clinical
picture supports an infectious etiology, but the judgment will be made by the observer and err on
34
Similarly, whether a patient is at increased risk of infection will be based on chief
compliant and history. Examples of classification of being at increased risk of infection include
open wounds, use immunosuppressive drugs, or HIV+ patients with poor disease control.
Lastly, presence of a bad smell in the room will be subjectively assessed by the observer.
Analysis:
Data will be doubly-entered into a MS Access database by both data collectors and then
cross-checked in order to ensure accuracy of entry. Data will then be analyzed using Stata
(StataCorp, College Station, Texas).
Anticipated Results:
We expect that fourteen attendings will participate in the study and will be shadowed
three times each for a total of 42 shifts shadowed. Figures 1 and 2 demonstrate our expectation
that hand hygiene adherence for the first three hand hygiene opportunities of the shift will be
substantially greater than hand hygiene adherence for the last three hand hygiene opportunities of
the shift. Expected values for hand hygiene compliance in the first two and last two hours of the
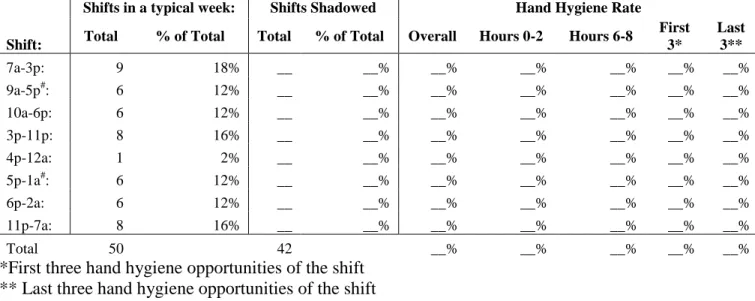
shift are shown in Figure 3. A summary of which shifts were shadowed and a breakdown of hand
hygiene compliance by shift will appear in Table 1.
Table 2 will provide a breakdown of hand hygiene compliance by the five WHO
indications for hand hygiene. Table 3 will offer a breakdown of hand hygiene compliance by
factors considered to potentially be moderating variables. Figure 4 will show the rate of hand
35
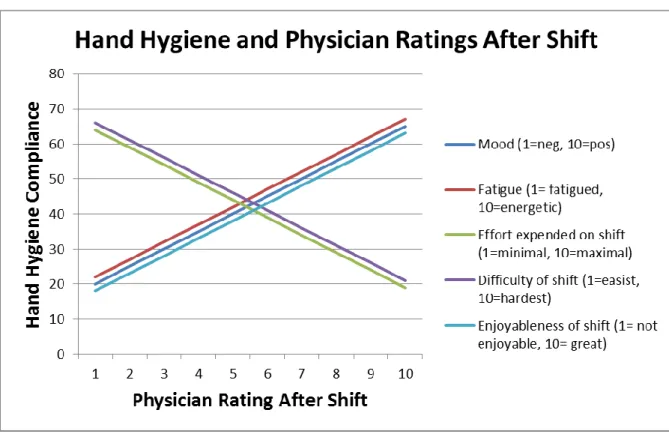
the course of an observation session. Figure 5 will demonstrate the expected effect of mood,
fatigue, effort expended on shift, difficulty of shift, and enjoyableness of shift on hand hygiene
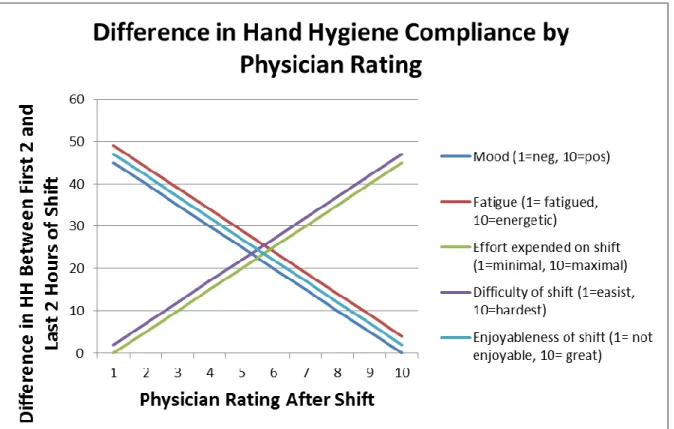
compliance. Similarly, Figure 6 shows the expected difference in hand hygiene rate of the first
two and last two hours of the shift as related to physician ratings of mood, fatigue, effort
expended on shift, difficulty of shift, and enjoyableness of shift on hand hygiene compliance.
Discussion:
We anticipate that the main finding from this study will be declining rate of hand hygiene
over the course of the shift of work, consistent with the model of willpower depletion or decision
fatigue. The significance of such a finding would not only include a potentially higher likelihood
of contracting a hospital acquired infection late into a physician’s shift, but also would suggest
that there are other aspects of physician performance that may gradually decline during work
without physicians’ awareness. Declining willpower could affect medical errors, admission rates,
interactions with staff, or ordering laboratory and imagining tests. Even a variance of 10-15% in
rates of admission or medical imaging due to willpower depletion could have significant health
and financial consequences for individual patients and the health care system.
There are possible alternate explanations for an apparent decline in hand hygiene rate
over the course of a shift. One explanation is that the busyness of shift may vary at different
times of the day, and high activity levels are associated with poorer hand hygiene adherence.
There are essentially three types of shifts at the medical center under study: morning to afternoon
shifts, afternoon to night shifts, and overnight shifts. The mornings may start off slowly and pick
36
poorer rates later in the day. The afternoon to night shifts, however, should generally
demonstrate the inverse pattern and by starting off busy and being less hectic at the end,
countering the momentum from the morning shift. To account for these potential variances that
could affect hand hygiene, our measurements of interruptions to the physician and interactions
by the physician may help to illuminate such patterns.
Another possible alternative explanation might be a different distribution of hand hygiene
indications in the first two and last two hours of the shift. Hand hygiene compliance before
patient contact is lower, with median compliance <20%, than after patient contact, which ranges
from 30-40% compliance.10 In the WHO criteria, there are two “before” contact indications: before patient contact and before a sterile task. There are three “after” indications: after body
fluid contact, after touching a patient, and after contact with patient surroundings, such as the
bed. It is possible that if more “after” indications occurred in the first two hours of a shift, then
the hand hygiene rate could be higher than the last two hours. This difference would be a
reflection of the distribution of the hand hygiene indications, but this would not necessarily
suggest indicate willpower depletion. Our analysis will assess the distribution of hand hygiene
indications in order to evaluate this possibility.
The WHO criteria also present a limitation to the study in that the different indications
do not equally capture likelihood of pathogen transmission. For instance, the “before sterile task”
category is very broadly defined as any interfacing with a mucus membrane, non-intact skin, or
invasive medical device. Thus, if a doctor washes her hands, performs a cardiac exam, and then
puts on gloves and palpates a patient’s tooth, the physician would only have 50% compliance:
The physician correctly performs hygiene before touching the patient for the cardiac exam, but
37
Likewise, if a physician washes his hands upon entering a room, only touches the patient bed,
and then leaves without performing hand hygiene, the compliance rate is 0%. No credit is given
for washing hands in the beginning because the physician did not touch the patient or perform a
sterile task; however, the physician is penalized for not performing hand hygiene after touching
immediate patient surroundings. A recent assessment of the WHO criteria found that it lacked a
strong scientific basis.15 While the hand hygiene criteria may not be accurately reflective of
potential for disease transmission, if applied consistently, these criteria should nonetheless be a
reasonable metric to assess evidence of decision fatigue. The hand hygiene indications with most
uncertainty in effectiveness can be removed from final analysis, leaving only the clearest
indications for hand hygiene, such as before and after touching a patient, which may offer a
better assessment of likelihood of acquiring hospital infections.
Another limitation of the study is potential for selection bias. During recruitment,
attendings will told that the study is about physician interactions in the Emergency Department.
Physicians who enjoy their jobs and are cheerful while performing them may be more likely to
enter the study than those who dislike their work and perform it with reluctance. Evidence on
willpower depletion shows that good mood and enjoyment of effortful work reduces the effect of
willpower depletion.7 It is possible that our study will include only those attendings who are least
susceptible to willpower depletion. If this scenario were to be true in our study, then it may prove
difficult to find performance differences between the beginning and end of the shift, or, these
differences may be underestimated.
A third concern as a possible threat to the validity of the study is the Hawthorne effect.
While under observation, it is likely that physicians will change their performance in various
38
study reduces risk of the Hawthorne effect in several ways. First, both the first two hours and last
two hours of the shift are observed in the same manner, and then compared to each other. Thus,
both comparison groups should experience about the same degree of change in physician
behavior due to observation and any differences between the beginning and end of the shift
should not be due to differences in being observed. Given the nature of the study design
observing the beginning and end of the shift, it will not be too difficult for physicians to infer
that we plan to compare the two time periods. In order to prevent physicians from trying to affect
study findings by altering certain aspects of their performance, they will be blinded to the
specific metrics under study, most importantly hand hygiene compliance.
There is great potential for applying the principle ideas of this study to other areas of
medicine. Assessing decision making and behavior through the lens of willpower depletion may
provide valuable insights into variations in medical practice and the clinical environment. The
highest value would be in assessing patient outcomes based on the point in time during the
physician’s shift a patient was treated; however, evaluating patient outcomes can present many
measurement challenges and great risk of confounding that may be difficult to control for. In the
short term, it may be easier to assess other intermediate outcomes such as rates of imaging or
admissions for specific injuries or illnesses to establish whether patterns consistent with decision
fatigue exist. For prospective observational studies, such as this one, measuring the time spent
and number of questions asked in evaluating patients and teaching residents over the course of
the shift could be also revealing of decision fatigue, and if so, might imply decreased quality of
care or teaching late in the shift. Much research remains to be done in understanding how
willpower depletion may manifest itself in real world circumstances outside of the psychology
39
Figures:
Note that data are not real and are provided to illustrate anticipated study findings.
Figure 1: Average Hand Hygiene Compliance for the First Three Opportunities of the Shift
40
Figure 3: Hand Hygiene Rate for the First Two Hours of a Shift vs Last Two Hours of a Shift
41
42
43
Tables:
Table 1: Hand Hygiene Compliance by Shift
Shifts in a typical week: Shifts Shadowed Hand Hygiene Rate
Shift: Total % of Total Total % of Total Overall Hours 0-2 Hours 6-8
First 3*
Last 3**
7a-3p: 9 18% __ __% __% __% __% __% __%
9a-5p#: 6 12% __ __% __% __% __% __% __%
10a-6p: 6 12% __ __% __% __% __% __% __%
3p-11p: 8 16% __ __% __% __% __% __% __%
4p-12a: 1 2% __ __% __% __% __% __% __%
5p-1a#: 6 12% __ __% __% __% __% __% __%
6p-2a: 6 12% __ __% __% __% __% __% __%
11p-7a: 8 16% __ __% __% __% __% __% __%
Total 50 42 __% __% __% __% __%
*First three hand hygiene opportunities of the shift ** Last three hand hygiene opportunities of the shift # Shifts on the D Side or “Fast Track”
Table 2: Hand Hygiene Compliance by WHO Indication
HH Indication
Total HH opportunitie
s:
Hours 0-2 Hours 6-8 Hand hygiene rate:
HH Opp's Proportio n HH Opp's Proportio n Hours 0-2 Hours 6-8 Overa ll Before patient
contact ___ ___ ___% ___ ___% ___% ___% ___%
Before sterile
task ___ ___ ___% ___ ___% ___% ___% ___%
After body
fluid contact ___ ___ ___% ___ ___% ___% ___% ___%
After patient
contact ___ ___ ___% ___ ___% ___% ___% ___%
After touching patient
surroundings ___ ___ ___% ___ ___% ___% ___% ___%
Column 1 of Table 2 displays the five WHO indications for hand hygiene (HH). Column 2 shows the total number of hand hygiene opportunities observed in the study for each of the five hand hygiene indications. In columns 3 and 4, the total of hand hygiene opportunities is broken down into those occurring in the first two and last two hours of the shift respectively.
44
Table 3: Hand Hygiene rates by moderating variables
Moderating Variable
Number of HH Opportunities
Overall HH Rate
Hours 0-2 Hours 6-8
Total Opp's
HH Rate
Total Opp's
HH Rate
New patient __ __% __ __% __ __%
Continued patient __ __% __ __% __ __%
On contact or other
precautions __ __% __ __% __ __%
Signs of
contagiousness __ __% __ __% __ __%
Patient at increased
risk of infection __ __% __ __% __ __%
Spanish-speaking
patient __ __% __ __% __ __%
Use of Interpreter __ __% __ __% __ __%
Noxious odor in
45
REFERENCES
1. Muraven M, Baumeister RF. Self-regulation and depletion of limited resources: Does
self-control resemble a muscle?. Psychol Bull. 2000;126(2):247-259.
2. Vohs KD, Baumeister RF, Schmeichel BJ, Twenge JM, Nelson NM, Tice DM. Making
choices impairs subsequent control: A limited-resource account of decision making,
self-regulation, and active initiative. J Pers Soc Psychol. 2008;94(5):883-898. doi:
10.1037/0022-3514.94.5.883.
3. Danziger S, Levav J, Avnaim-Pesso L. Extraneous factors in judicial decisions. Proc Natl
Acad Sci U S A. 2011;108(17):6889-6892. doi: 10.1073/pnas.1018033108.
4. Laxmisan AA. The multitasking clinician: Decision-making and cognitive demand during and
after team handoffs in emergency care. International journal of medical informatics (Shannon,
Ireland). 2007;76(11-12):801-811.
5. Levav J, Heitmann M, Herrmann A, Iyengar SS. Order in product customization decisions:
Evidence from field experiments. Journal of Political Economy. 2010;118(2):274-299.
6. Baumeister RF, Vohs KD, Tice DM. The strength model of self-control. Current directions in
psychological science. 2007;16(6):351-355.
7. Hagger MS, Wood C, Stiff C, Chatzisarantis NL. Ego depletion and the strength model of
self-control: A meta-analysis. Psychol Bull. 2010;136(4):495-525. doi: 10.1037/a0019486.
8. Burkley E. The role of self-control in resistance to persuasion. Person Soc Psychol Bull.
46
9. Tyler JM. In the eyes of others: Monitoring for relational value cues. Human Communication
Research. 2008;34(4):521-549.
10. Erasmus V, MSc, Daha T, Brug H, PhD, et al. Systematic review of studies on compliance
with hand hygiene guidelines in hospital care • . Infection Control and Hospital Epidemiology.
2010;31(3):pp. 283-294.
11. Tyler JM, Burns KC. After depletion: The replenishment of the self's regulatory resources.
Self and Identity. 2008;7(3):305-321.
12. World Health Organization. WHO Guidelines on Hand Hygiene in Health Care: First Global
Patient Safety Challenge: Clean Care is Safer Care. World Health Organization, Patient Safety;
2009.
13. World Health Organization. Hand hygiene technical reference manual. 2009.
14. Chisholm CD, Weaver CS, Whenmouth L, Giles B. A task analysis of emergency physician
activities in academic and community settings. Ann Emerg Med. 2011;58(2):117-122. doi:
10.1016/j.annemergmed.2010.11.026.
15. Chou DT, Achan P, Ramachandran M. The world health organization '5 moments of hand
hygiene': The scientific foundation. J Bone Joint Surg Br. 2012;94(4):441-445. doi: