Abstract...1
Introduction...3
Table 1. Factors Related to Sub-Optimal Feeding Practices...8
Methods...9
Table 2. Focused Research Question for Review...11
Results...13
Figure 1. Summary of Article Review...14
Table 3. Characteristics of Included Studies...15
Table 4. Results of Studies Measuring Breastfeeding...19
Table 5. Results of Studies Measuring Introduction to Solid Foods...21
Discussion...22
Conclusions...27
Acknowledgments...28
References...29
Appendices...32
Appendix 1. Search Strategy...32
Appendix 2. Quality Assessment...33
Table A1. Critical Appraisal Tool...33
Figure A1. USPSTF Criteria for Rating Strength of Evidence...35
1 Abstract
Introduction: Initiating and maintaining breastfeeding during infancy and delayed introduction of solid foods are associated with superior health outcomes in children. American mothers currently fall short of reaching national guidelines of exclusive breastfeeding until 6 months, when solid foods are recommended in addition to breastfeeding until 1 year of age. A dearth of education about optimal infant feeding practices may contribute to mothers’ lack of adherence to these guidelines. Determining the most effective sources of information and advice that
influence mothers’ feeding decisions may offer an opportunity to develop maternal education materials and programs to increase breastfeeding initiation, duration, and delayed introduction of solid foods in the United States.
Methods: This systematic review searched PubMed for articles from 1995-present regarding sources of information and advice for mothers of infants (0-2 years old) and their associations with 1) breastfeeding initiation and/or duration and 2) introduction of solid foods. Studies were divided according to “passive” (media, unsolicited advice or opinions) or “active” (interventions or educational programs) sources of information. Randomized and non-randomized controlled trials and cohort studies were included in analysis and rated for quality as individual studies and in aggregate. Results were synthesized qualitatively.
Results: From 294 abstracts, 40 full text articles were reviewed and 14 met eligibility criteria. 11 evaluated breastfeeding, 2 evaluated solid food introduction, and 1 study evaluated both
3 Introduction
Infant Feeding Practices and Child Health Outcomes
During infancy, mothers’ and caregivers’ feeding practices play an important role in a child’s future health status. Initiating and maintaining breastfeeding during infancy is associated with superior outcomes, including a lower risk of overweight or obesity in later childhood. An Icelandic prospective cohort study of 154 infants found that formula-feeding and shorter duration of breastfeeding before 6 months are associated with faster weight gain and higher BMI at six years of age.1,2 Early introduction of solid foods is found to further exacerbate the relationship between formula feeding and increased BMI.2 A meta-analysis of risk factors for overweight or obesity during childhood resulted in similar findings; children who are “ever breastfed” as infants are significantly less likely to be overweight than children who are never breastfed as infants.3 In addition, lengthening the duration of breastfeeding results in better outcomes. One study
compared durations of breastfeeding and found that infants who were breastfed for 6 months were significantly less likely to be overweight at 2 years of age than infants who were breastfed for 3 months.4
4 systematic review for the Nordic Nutrition Recommendations found evidence that breastfeeding during infancy is associated with slower weight gain during infancy, less inflammatory bowel disease, higher developmental scores in children, and slightly lower blood pressure and cholesterol levels during adulthood.9
Association between early weight gain and later weight
There is also evidence that obesity during childhood has negative health consequences later in life. An examination of 2 prospective cohort studies of children followed into adulthood (one in the U.S. and one in Finland) found that youth with metabolic syndrome (defined for this study as any 3 components of low HDL, high triglycerides, high glucose, high blood pressure, or high BMI) were significantly more likely to have high carotid artery intima-media thickness and type 2 diabetes mellitus as adults.10 A systematic review conducted with evidence from 2002-2010 found that 4 of 5 included studies showed a significantly increased risk of premature mortality in adulthood among those who were overweight or obese in childhood or adolescence. Additionally, all included studies that reported on morbidity found significantly increased risk of diabetes, hypertension, ischemic heart disease, and stroke in adulthood among obese and overweight children and adolescents.11 Promoting adherence to guidelines for exclusive breastfeeding and introduction of solid foods may be one approach to decreasing a child’s risk of overweight and obesity, and thus negative health consequences later in life.
Infant Feeding Practice Guidelines
5 any other solids or liquids with the exception of vitamins. The AAP elaborates on their solid food introduction guideline by recommending 2-3 “healthy snacks” per day after 9 months of age.13
Adherence to Guidelines
Actual adherence to these nutritional guidelines is poor in the United States. Data from the CDC’s 2011 and 2012 National Immunization Survey report that 76.5% of U.S. infants were “ever breastfed,” and only 16.4% of infants were exclusively breastfed at 6 months of age as guidelines recommend, suggesting that other modes of feeding are widespread prior to 6
months. 24.2% of breastfed infants received formula supplementation within the first few days of age.14 The National Immunization Survey data are based on a landline telephone survey
conducted by the CDC, and thus has a large potential for error.14 Mothers who do not own a landline telephone are not represented in the survey data, and as use of landline telephones continues to decrease in the United States, the representativeness of the study significantly diminishes. If for some reason mothers who are less likely to breastfeed are also less likely to own a landline telephone, the NIS may even overestimate the percentage of infants ever breastfed and exclusively breastfed at different ages.
Adherence to the guideline regarding solid food introduction is even lower. A study published in 2008 using data from the Infant Feeding Practices Study II (IFPS II) found that 21% of mothers introduced solid foods before 4 months of age, with just 7% of mothers introducing solids after 6 months as recommended. Additionally, 20% of the mothers introduced juice before 6 months of age.15 Many parents introduce solid foods early by adding cereal to their baby’s bottle.16 Whether this action is included in measures of solid food introduction has the potential to underestimate the number of parents actually introducing solid foods prior to 6 months.
6 than half of the original study participants were able to complete all 10 questionnaires.17 This large attrition rate may limit the external validity of the results and, again, may overestimate the percent of mothers introducing solid foods later, as parents adhering to guidelines may be more likely to respond to the survey.
The Healthy People 2020 objectives include targets of 81.9% of infants ever breastfed, 25.5% exclusively breastfed through 6 months, and reduction of the proportion of breastfed infants who receive formula supplementation to 14.2%.14 According to the data presented above, the U.S. has yet to achieve these goals and in some cases has a fair amount of work to do to reach them. In fact, the NIS and IFPS II may even over-estimate the percentage of infants breastfed and introduced to solid foods at optimal times.
Discrepancies in Adherence
The literature suggests that adherence to feeding guidelines is related to many factors, including education, race, work status, and even geographic location (Table 1). Less
breastfeeding may be somehow ingrained in American culture. “Less acculturated” groups such as immigrant Hispanic children with immigrant parents are more likely to be breastfed than “more acculturated” groups – especially American black children with American-born black mothers.18 Formula supplementation is especially high among black mothers.19
Low-income mothers are also less likely to breastfeed and more likely to introduce solid foods before 6 months, and sometimes even before 4 months.20,21 Low income women who perceive their child as “fussy” are more likely to introduce solids before the recommended age.22 An analysis of complementary feeding practices reported in the IFPS II found that introducing solid foods prior to 4 months and feeding juice before 6 months were significantly inversely associated with the mother’s education level.23
7 study on state-to-state discrepancies in breastfeeding rates found that adjusting for income, race, and other demographics actually decreased the discrepancies between states, but large disparities still existed due to differences in legislation protecting breastfeeding between states.24
The work culture and maternity leave in the United States is different than in other developed countries. Working mothers practice shorter durations of exclusive breastfeeding, especially in states without legislation to encourage workplace breastfeeding.25 A study of state breastfeeding laws found that, in 2010, 23 of the 50 states had enacted laws to protect a mother’s right to express milk during the workday. The Patient Protection and Affordable Care Act of 2010 includes a provision for “reasonable break time” for mothers to pump breast milk, but it has some exceptions and is open to interpretation. Even with overall increases in initiation of breastfeeding since the 1970s, the ability of mothers to exclusively breastfeed for 6 months or more may be limited by the work environment.25 In other developed countries, the provision of paid maternity leave, legislation supporting breastfeeding in the workplace, and support staff such as health visitors in the U.K. offer additional sources of support and information about infant feeding guidelines that most American women do not find. Consequently, breastfeeding initiation and duration rates are higher in other countries that guarantee breastfeeding support in the workplace through legislation, such as the U.K. and Australia.26
The healthcare system can also make it difficult for mothers to learn about the guidelines for infant feeding. Access to healthcare is varied in the United States, but among those who do have access, primary care providers have limited time for appointments to discuss a multitude of topics. One study of active fellows of the AAP found that 65% recommended exclusive breastfeeding past 1 month and only 37% recommended breastfeeding for 1 year.27 A lack of current knowledge about breastfeeding benefits and support exists among busy,
8 Table 1. Factors Related to Sub-Optimal Feeding Practices
Average and Higher-Income Women
All Women Lower-Income Women
Time (full-time/high-demanding jobs without
legislation to protect breastfeeding)
American-born Low income
Minority race Low educational attainment Younger age Perceive child as “fussy” Lack of paid maternity
leave/legislation to protect breastfeeding in workplace
WIC participation (formula provided)
Living in Southern state
Mothers’ Barriers and Sources of Support
Given a possible lack of guidance and support from healthcare providers and employers, American mothers often turn to other sources for information and advice on how to feed their child during infancy. Mothers cite the need to return to work, fear, and provision of formula through the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) as reasons they do not exclusively breastfeed for the recommended period of time.29 Mothers repeatedly state in qualitative studies that they feel there is a lack of accessible information and support to initiate and sustain breastfeeding and proper timing of solid food introduction.30-32 Some mothers who lack formal sources of information rely on their own experience or the advice of family members, who may advise them to supplement feeding with formula or solid foods at an early age because the baby is not “chubby” enough or because it is simply the cultural norm.33-35 Multiple other sources are available for mothers to receive conflicting information about feeding, including advertisements, magazines, and the Internet.
These sources of information may play an integral role in a mother’s decision-making process regarding how she chooses to feed her infant. Knowing how different sources of information and advice affect mothers’ feeding styles may help elucidate ways in which
9 sub-optimal feeding practices, working to intervene or provide education at these critical points may help spread awareness of feeding guidelines. Eliciting reasons for choosing and
implementing different feeding practices will be paramount in determining how to change these practices to increase the proportion of infants who are exclusively breastfed.
Thus, the aim of this review was to determine how different sources of information and advice influence infant feeding practices. More specifically, I will examine whether (1)
breastfeeding initiation and/or duration and (2) timing of introduction of solid foods differ between “passive” and “active” sources of information and advice used by mothers or caregivers of infants (children less than two years old).
Methods
Research Question
A preliminary review of the literature elicited two main outcomes studied in regards to infant feeding practices: (1) initiation and/or duration of breastfeeding and (2) timing of introduction of solid foods. The main sources of information studied in the literature can be divided into 5 main categories: peer counselors, nurses (includes RNs and lactation
consultants), physicians, relatives/friends, and media (includes Internet, books, DVDs, etc.). Additionally, studies ranged from “passive” sources of information (media, brochures,
unsolicited advice or encouragement from relatives, friends, or healthcare providers) to more “active” interventions to provide information (face to face meetings and education with peer counselors, lactation consultants, physicians, and nurses). Based on these findings, I decided on two key questions:
10 ● KQ2: For parents and caregivers of children less than 2 years old, does introduction of
solid foods before 6 months differ between “passive” and “active” sources of information or advice?
Study inclusion criteria
I included studies from 1995-present to capture the Internet as a relevant source of information or advice for caregivers (Table 2). I included systematic and non-systematic reviews, randomized controlled trials, non-randomized controlled trials, prospective and retrospective cohort studies. I excluded cross-sectional and qualitative studies, due to the lack of causal relationships and outcomes that can be identified from these studies. No previous systematic or non-systematic reviews were found that answered my study question, however one relevant review provided studies included in the final selection.36
I chose to include only studies from the United States. While much of the evidence base for infant nutrition practices comes from other developed countries, such as Australia and the U.K., large differences exist in the health system, provision of maternity leave, and resources available to new mothers that may render studies from these countries inapplicable to the United States. For example, 70% of mothers in the U.K. cite health visitors as their main source of information for feeding during the postnatal period.37 There is no equivalent of a health visitor that is available to most mothers in the United States, thus studies from other developed countries with different sources of information and different maternity leave practices were deemed inapplicable.
11 A timeline from birth to two years was considered, as global guidelines recommend breastfeeding up to 2 years of age as tolerated by mother and infant.12 Thus, I wished to capture breastfeeding duration up to 2 years if possible.
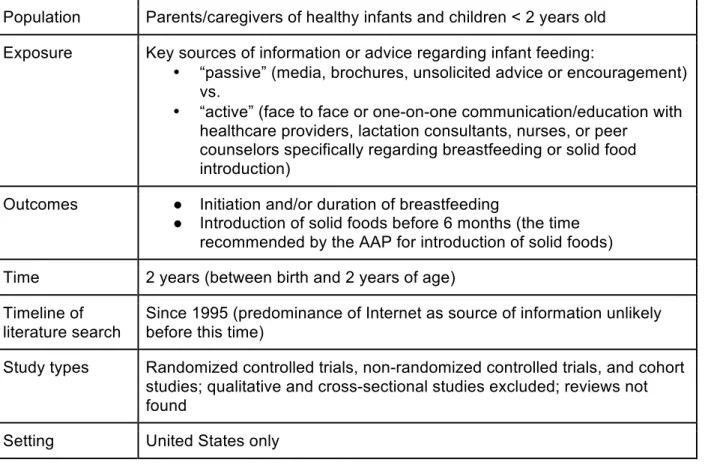
Table 2. Focused Research Question for Review
Population Parents/caregivers of healthy infants and children < 2 years old Exposure Key sources of information or advice regarding infant feeding:
• “passive” (media, brochures, unsolicited advice or encouragement) vs.
• “active” (face to face or one-on-one communication/education with healthcare providers, lactation consultants, nurses, or peer
counselors specifically regarding breastfeeding or solid food introduction)
Outcomes ● Initiation and/or duration of breastfeeding
● Introduction of solid foods before 6 months (the time recommended by the AAP for introduction of solid foods) Time 2 years (between birth and 2 years of age)
Timeline of literature search
Since 1995 (predominance of Internet as source of information unlikely before this time)
Study types Randomized controlled trials, non-randomized controlled trials, and cohort studies; qualitative and cross-sectional studies excluded; reviews not found
Setting United States only
Search Strategy
12 duration of breastfeeding OR timing of introduction of solid foods were included and other
outcomes (such as intent to breastfeed) were excluded.
Articles that did not specifically elicit sources of information or advice for
mothers/caregivers were excluded. For example, several studies looked at sources of support during infant feeding. This was excluded as an independent variable because it implies either agreement (support) or disagreement (lack of support) with the mothers’ own decision to breastfeed or introduce solid foods and may not imply any actual influence on the decision-making process. Articles deemed to fit criteria based on abstract review were then examined in full-text independently (by the same reviewer).
Quality Assessment and Synthesis of Evidence
I assessed individual study quality using the following criteria: risk of bias (internal validity), analysis, precision, and applicability (external validity). A standardized critical appraisal template served as the basis for quality assessment for individual articles (Appendix 2, Table A1). Subsequently, I prescribed an overall quality rating of each article according to the gestalt of the critical appraisal template.
The strength of evidence from the aggregate of all included studies was examined for each key question using the USPSTF criteria (Appendix 2, Figure A1). I used the USPSTF system because the criteria are a thorough and standardized way to evaluate the evidence base.
13 Results
Results of Evidence Search
I reviewed 294 abstracts and 40 full-text articles based on the criteria described above. 14 studies met all eligibility criteria. Of these, 11 evaluated the initiation and/or duration of breastfeeding as the outcome, 2 looked at timing of introduction of solid foods as the outcome, and 1 study included both outcomes. Main reasons for exclusion at the full-text review stage were using “intent to breastfeed” rather than actual breastfeeding practices as the outcome and lack of inclusion of specific sources of information and/or advice as independent variables (Figure 1).
Included Studies
The studies included varied in terms of population studied, measurement, and
exposures. The independent variables measured as sources of information or advice ranged from self-reported sources of influence (such as family, members, friends, partners, or healthcare providers) to specific interventions including WIC peer counselor programs, home visitation programs, educational videos, and educational handouts provided at the doctor’s office. The outcomes measured were also heterogeneous: initiation of breastfeeding was measured at different times (any breastfeeding during first year, breastfeeding within first 4 weeks, exclusive breastfeeding vs. any breastfeeding) and timing of solid food introduction was measured before 3 months, before 4 months, or before 6 months. For a summary of the
characteristics of included studies, please see Table 3.
14 Figure 1. Summary of Article Review
in person or in a one-on-one setting. These studies either measured a one-time or unstructured “active” source of information or measured a multi-contact, more intensive “active” source. The “active” sources included classes or regular education from peer counselors, nurses, lactation consultants, physicians, or WIC counselors. I ranked included studies on a level from 1 to 3, with “1” representing the studies that measured “passive” sources of information, “2”
15 Table 3. Characteristics of Included Studies
Author & Year
Population Exposure Comparator Outcomes Study Design
Studies of Breastfeeding
Level 1 Studies Odom et al.
201338 2,041 mothers from 2005-2007 IFPS II Family members’ and healthcare providers’ opinion on infant feeding
None Initiation of
breastfeeding at 4 weeks PP
Prospective cohort
Racine et al. 200939
1,322 women from Healthy Steps for Young Children National Evaluation from birth to 33 months PP
Doctors’ encouragement of and information given about breastfeeding, education about breastfeeding through WIC
None Breastfeeding
cessation during first 12 months PP
Prospective cohort
Rhodes et al. 200840
256 American Indian women living in Minnesota
Advice to breastfeed from woman’s mother and/or partner
None Breastfeeding
initiation and
duration to 6 and/or 12 weeks PP
Prospective cohort
Level 2 Studies Campbell et
al. 201441
3,070 low-income mothers from Texas WIC Infant Feeding Practices Survey (IFPS) in 2009
WIC peer counselor who provided advice and information on breastfeeding either before pregnancy, during pregnancy, or both
No peer counselor exposure
Initiation of breastfeeding
Retrospective cohort
Chen et al. 201242
2,586 women from IFPS II who reported “ever breastfed”
Education sources about breastfeeding and breast pump use Compared “classes/support groups”, “media”, various healthcare providers, WIC, relatives/friends Duration of
breastfeeding in 2 categories; “short” (<2 months) and “long” (>2 months)
Prospective cohort
Reifsnider & Eckhart 199743
31 WIC participants in rural Oklahoma
Prenatal nutrition education at WIC + breastfeeding education class
Prenatal nutrition education only
Breastfeeding incidence and days of duration
16 Author &
Year
Population Exposure Comparator Outcomes Study Design
Level 3 Studies Sandy et al.
200944
238 Latina mothers in NYC
Program with information about infant feeding from “family support workers”
Educational books/pamphlets
Breastfeeding (any & exclusive) in first week
Randomized controlled trial
Petrova et al.
200945 104 in WIC program One-on-one breastfeeding education sessions from lactation consultant: 2 prenatal, 1 in-hospital, f/u at 1 wk, 1 mo., and 2 mos.
Standard WIC
breastfeeding services
Breastfeeding in 1 week, 1 month, 2 months, and 3 months
Randomized controlled trial
Betzold et al.
200746 33 women recruited from prenatal clinic in CA
Educational handouts distributed at prenatal and well child visits; doctors giving information about breastfeeding at each visit
None In-hospital
exclusivity of breastfeeding and duration of exclusive breastfeeding Quasi-experimental
Pugh et al.
199847 60 primiparous women 2 home visits from RN + lactation consultant telephone call
1 home visit from RN without structured program Days of breastfeeding Randomized controlled trial
Brent et al.
199548 108 from a predominantly low-income, inner-city prenatal clinic and maternity ward
Prenatal lactation consultation, in-hospital consultation, outpatient follow-up at 1 week and at each f/u visit in first year
No lactation consultant Incidence and duration of breastfeeding
Randomized controlled trial
Studies of Breastfeeding AND Introduction of Solid Foods
Level 2 Studies Scheinmann
et al. 201049 272 Latina women recruited from WIC clinics in NYC
Educational, bilingual 25-min. DVD with
information about “appropriate feeding behaviors”
No DVD; usual WIC care
Initiation of
breastfeeding AND timing of
introduction of solid foods
17 Author &
Year
Population Exposure Comparator Outcomes Study Design
Studies of Solid Foods
Level 1 Studies Clayton
et al. 201350
1334 women from IFPS II Advice from friends, family members, and healthcare providers
None Introduction of solid foods earlier than 4 months
Prospective cohort
Level 3 Studies Black et
al. 200151
121 first-time, low-income Black mothers <18 years old recruited from urban hospitals
Home visit by peer educators and videotape made by adolescent mothers, every other week for 1 year focusing on complementary feeding
No
intervention
Introduction of solid foods earlier than 3 months
18 Quality of Included Individual Studies
A full assessment of the quality of each individual study is shown in Appendix 2, Table
A2. All but 3 of the studies were assigned an overall quality rating of “Poor,” with one study48
judged to be between “Fair” and “Poor” and 2 studies45,51 rated as “Fair.” None of the included
studies rated as “Good” quality based on internal validity, analysis, precision, and external
validity. Many studies used the Infant Feeding Practices Study II (IFPS II) as the source of data,
which afforded a large sample size but the prospective cohort design and consumer opinion
sampling limited the studies in terms of selection bias and measurement bias. Many of the other
studies lacked external validity due to limited sample size and/or limitation to a single
geographic region, race, or income level that is not representative of all United States mothers.
Results of Included Studies
Key Question 1: Breastfeeding Initiation and/or Duration
The results of included studies that measured initiation and/or duration of breastfeeding
are displayed in Table 4. Most studies found at least one source of information or advice
statistically significantly associated with a breastfeeding outcome, but measurement of initiation
or a specific duration of breastfeeding was highly variable. For studies that measured passive
sources of information38-40, advice or opinions shared by the infant’s father were most strongly
associated with either initiating breastfeeding or discontinuing breastfeeding if the father
preferred formula feeding only. Interventions to provide education and encouragement for
breastfeeding, for the most part, increased breastfeeding outcomes. Peer counselor contact
was associated with greater odds of initiating breastfeeding41 and greater odds of exclusive
breastfeeding in the first week.44 Multi-contact lactation consultant education was associated
with longer duration of breastfeeding in one study48 but not statistically significantly associated
19 sources of information seemed to be similar to ORs for breastfeeding outcomes of
single-contact or less structured interventions or “active” sources, although comparison is difficult given
differences in breastfeeding outcomes measured.
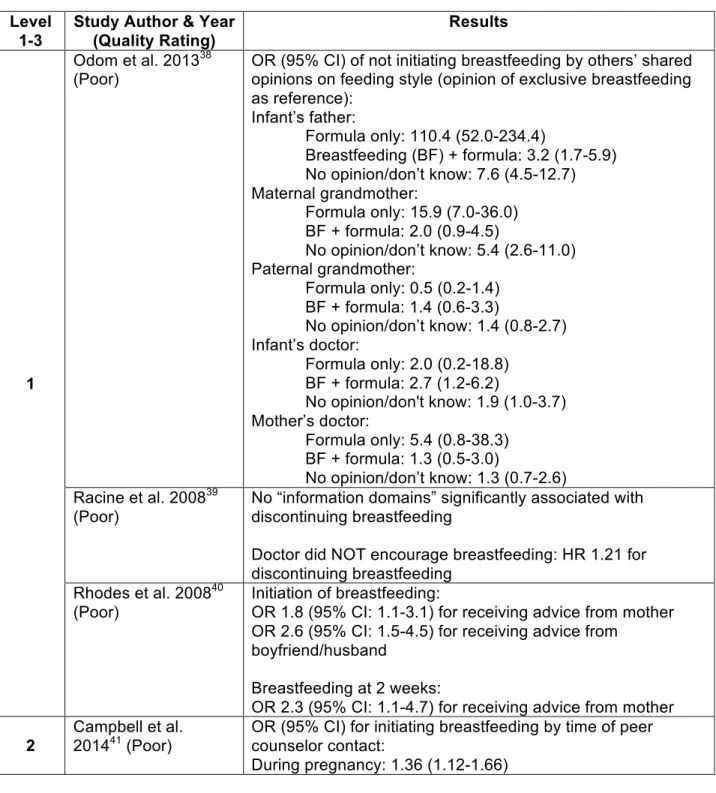
Table 4. Results of Studies Measuring Breastfeeding
Level 1-3
Study Author & Year (Quality Rating)
Results
1
Odom et al. 201338
(Poor)
OR (95% CI) of not initiating breastfeeding by others’ shared opinions on feeding style (opinion of exclusive breastfeeding as reference):
Infant’s father:
Formula only: 110.4 (52.0-234.4)
Breastfeeding (BF) + formula: 3.2 (1.7-5.9) No opinion/don’t know: 7.6 (4.5-12.7) Maternal grandmother:
Formula only: 15.9 (7.0-36.0) BF + formula: 2.0 (0.9-4.5)
No opinion/don’t know: 5.4 (2.6-11.0) Paternal grandmother:
Formula only: 0.5 (0.2-1.4) BF + formula: 1.4 (0.6-3.3)
No opinion/don’t know: 1.4 (0.8-2.7) Infant’s doctor:
Formula only: 2.0 (0.2-18.8) BF + formula: 2.7 (1.2-6.2)
No opinion/don't know: 1.9 (1.0-3.7) Mother’s doctor:
Formula only: 5.4 (0.8-38.3) BF + formula: 1.3 (0.5-3.0)
No opinion/don’t know: 1.3 (0.7-2.6) Racine et al. 200839
(Poor)
No “information domains” significantly associated with discontinuing breastfeeding
Doctor did NOT encourage breastfeeding: HR 1.21 for discontinuing breastfeeding
Rhodes et al. 200840 (Poor)
Initiation of breastfeeding:
OR 1.8 (95% CI: 1.1-3.1) for receiving advice from mother OR 2.6 (95% CI: 1.5-4.5) for receiving advice from
boyfriend/husband
Breastfeeding at 2 weeks:
OR 2.3 (95% CI: 1.1-4.7) for receiving advice from mother
2
Campbell et al.
201441 (Poor) OR (95% CI) for initiating breastfeeding by time of peer counselor contact:
20 In hospital: 2.06 (1.54-2.75)
After delivery: 1.85 (1.53-2.24)
During pregnancy + in hospital: 2.07 (1.51-2.84) During pregnancy + after delivery: 1.56 (1.30-1.88) In hospital + after delivery: 2.07 (1.51-2.83)
All 3 points: 2.00 (1.44-2.76) Chen et al. 201242
(Poor)
OR (95% CI) for breastfeeding for >2 months (compared to <2 months):
Classes/support groups: 1.85 (1.24-2.76) Non-significant findings:
Nurse: OR 0.80 (0.57-1.11)
Physician/PA: OR 1.11 (0.81-1.53) Lactation consultant: OR 0.92 (0.65-1.30) Friends/relatives: OR 1.29 (0.92-1.79) Nutritionist: 0.94 (0.53-1.68)
WIC: 0.99 (0.61-1.60) Media: 1.39 (0.97-2.01) Reifsnider & Eckhart
199743 (Poor)
Mean days of breastfeeding: Intervention group: 76.1 +/- 104.3 Control group: 29.5 +/- 43.6 Scheinmann et al.
201049 (Poor) % any breastfeeding at 3 months: Intervention group: 74.8%
Control group: 76.7% (N.S.)
% any breastfeeding at 6 months: Intervention group: 53.8%
Control group: 58.9% (N.S.)
3
Sandy et al. 200944 (Poor)
OR (95% CI) for intervention group vs. control group:
Any breastfeeding (ABF) in first week: 1.73 (0.88-3.40)
Exclusive breastfeeding (EBF) in first week: 1.92 (1.05-3.52)
Petrova et al. 200945
(Fair)
OR (95% CI) for intervention vs. control group:
EBF at 1 week: 1.66 (0.55-4.99) EBF at 1 month: 1.34 (0.41-4.42) EBF at 2 months: 1.70 (0.47 – 6.10) EBF at 3 months: 2.21 (0.42-11.7) Betzold et al. 200746
(Poor)
100% breastfeeding initiation 61% EBF while in-hospital 88% ABF at 3 months 73% ABF at 6 months 33% ABF at 12 months Pugh & Milligan
199847 (Poor)
Mean breastfeeding duration (days): Intervention group: 136.3
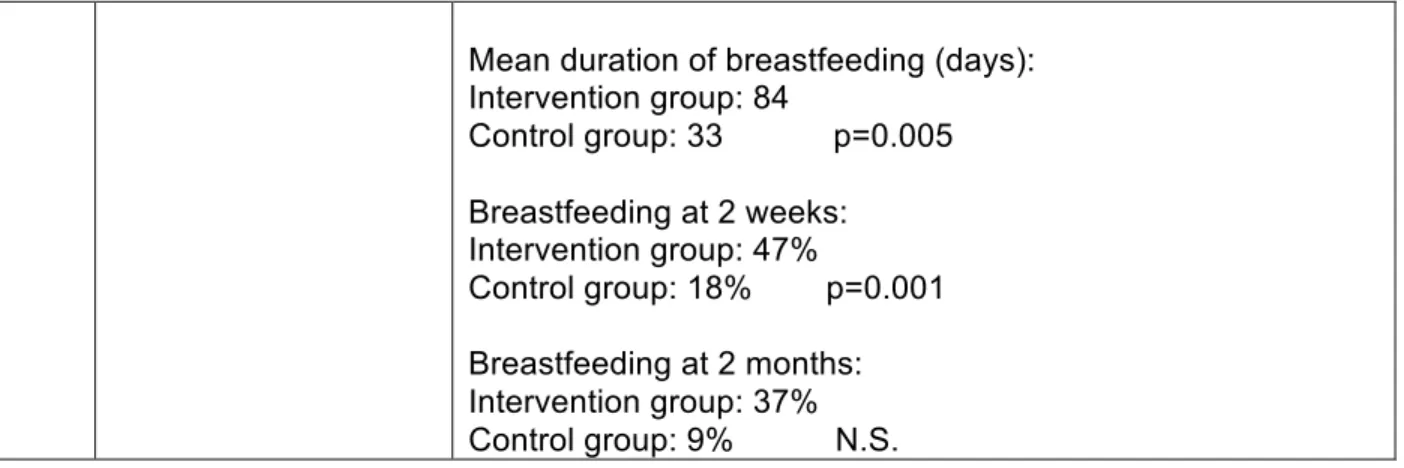
Control group: 88.3 Brent et al. 199548
(Fair to Poor)
21 Mean duration of breastfeeding (days):
Intervention group: 84
Control group: 33 p=0.005
Breastfeeding at 2 weeks: Intervention group: 47%
Control group: 18% p=0.001
Breastfeeding at 2 months: Intervention group: 37% Control group: 9% N.S.
Key Question 2: Solid Food Introduction
The results of studies that evaluated introduction to solid foods are shown in Table 5. In
these studies, a home visitation program by peer educators significantly delayed introduction of
solid foods after 3 months51, while advice from a healthcare provider to introduce solid foods
prior to 4 months was statistically significantly associated with introducing solid foods prior to 4
months.50 Only one of the studies measured introduction of solid foods before at the
recommended age, 6 months, and no significant difference was seen between the intervention
and control group.49
Table 5. Results of Studies Measuring Introduction to Solid Foods
Level 1-3
Study Author & Year (Quality Rating)
Results
1 Clayton et al. 201350
(Poor)
OR (95% CI) for introducing solid foods prior to 4 months if mother received advice from doctor of healthcare provider to introduce solid foods:
1.79 (1.15-2.80) 2 Scheinmann et al.
201049 (Poor)
Introduced solid foods before 3 months: Intervention group: 16.8%
Control group: 17.2% N.S.
Introduced solid food before 6 months: Intervention group: 28.7%
Control group: 29.5% N.S.
Average age at first solid foods (months): Intervention group: 5.2
22 3 Black et al. 200151
(Fair)
OR (95% CI) of introducing solid foods after 3 months: Intervention group: 3.8 (1.6-9.1)
Rating the of Body of Evidence
As discussed above, most studies achieved a “poor” quality rating. Studies are
heterogeneous in population characteristics, study designs, exposures, and outcome
measurements and thus are difficult to compare. 6 of the 14 studies used the most appropriate
and ideal research design (RCT) to evaluate certain sources of information compared to
controls, although many of these studies suffered design or measurement flaws. The body of
evidence generally is of low quality for this review, due to the fact that 11 of 14 studies were
rated as poor quality, with no good quality studies. The external validity similarly is low among
the included studies, with the largest samples from a non-nationally representative consumer
opinion panel (IFPS II) and most remaining studies from specific, non-representative
populations such as low-income women of a single race or predominantly high-income White
women. The results of the studies are inconsistent in that each looked at different variations of
exposures and measured breastfeeding or solid food outcomes in different ways. Likewise,
precision of the body of evidence is poor due to the heterogeneity of the included studies. Most
studies contained some evidence that the specific source of information or intervention studied
was associated with better breastfeeding or solid food outcomes, but again, the studies are so
variable in nature that comparison or synthesis of results is difficult.
Discussion
Summary of Results
In summary, 14 articles examining key sources of information or advice regarding
breastfeeding and solid food introduction displayed heterogeneous methods, measurement, and
23 information sources measured is too great to say with any certainty that “passive” or “active”
sources are superior to the others in terms of infant feeding outcomes. A consistent body of
evidence comparing different types and intensities of sources of information does not exist at
this time. In addition, although multi-contact peer counseling interventions showed improved
feeding outcomes in more than one study, the quality of the studies and general limitation of the
literature is too poor to conclude that multi-contact peer counseling is in fact the best source of
infant feeding information for mothers.
Current Practice
The USPSTF currently recommends interventions to promote and support breastfeeding
with a grade B recommendation.52 However, the specific types of interventions or information
sources that are the most effective are not known. Assuming that lack of education about
breastfeeding and optimal timing of solid food introduction is one reason for low rates of
breastfeeding to one year and introduction of solid foods after 6 months, knowing what types of
information and advice influence feeding the most are of great importance in educating mothers
about proper feeding for their infants.
As stated previously, the Healthy People 2020 goals aim for breastfeeding rates of
81.9% ever breastfed and 25.5% breastfeeding through 6 months.14 In order to achieve these
goals (and the goals that were not met in Healthy People 2010), evidence about the best way to
educate mothers is needed. Large, expensive programs such as weekly home visits for every
mother are likely not feasible. Thus, while these programs are valuable and research examining
high-intensity interventions adds to our knowledge of how to improve feeding for disadvantaged
women, knowing the effectiveness of more basic (described here as “passive”) sources of
information is important as well in order to reach the masses. Distributing the most effective and
available passive sources of information in clinic offices and other convenient locations could
24 personnel. This review attempted to discern the comparative effectiveness of different types and
intensities of sources of information. While this is, to our knowledge, the first attempt at a review
of sources of infant feeding information or advice, the current body of literature is insufficient to
determine the optimal mode of education for mothers of infants.
Limitations of this review
One potential limitation of this review is the search strategy and search terms used.
Finding MeSH terms that capture the variety of sources of information and advice available to
mothers is difficult, and it is likely that studies were missed. Consultation with a health sciences
librarian helped groom the search strategy but some relevant studies may not be indexed to the
search terms used.
Publication bias is quite possible given that most of the included studies found significant
associations between one or more sources of information and infant feeding outcomes. Thus,
studies conducted with negative results may not be published. However, it is important for us to
know what sources of information and advice do not increase breastfeeding rates so that time,
money, and other resources are not spent on programs that provide these sources of education.
Additionally, the heterogeneity of the studies led us to divide the studies somewhat
arbitrarily by “passive” and “active” sources of information, and, within the “active” sources, by
intensity of contact with the source. These divisions may be arbitrary for some but, given the
heterogeneity of the body of literature, some type of classification seemed necessary to attempt
to synthesize the results.
Limitations of the evidence
Obviously, there is a paucity of evidence regarding the effectiveness of certain sources
of information and their associations with infant feeding outcomes. The first problem is the great
25 measured within the studies. A need exists for comparison of multiple sources of information or
advice with one another in large, representative studies. The studies measured a range of
sources of information and interventions, from opinions and advice from family members and
healthcare providers, to weekly home visitation by peer counselors or lactation consultants, to
regular breastfeeding education by a physician. However, the Internet as a source of
information was noticeably left out from measurement of exposures in these studies. The
Internet offers the potential for a large variety of convenient, accessible information for mothers
and should be measured as a possible source of education. Standardization of the measures
used for breastfeeding initiation and duration are also needed.
The included studies did not measure feeding outcomes as adherence to national
guidelines (breastfeeding to six months or one year, introduction of solid foods after six months),
but rather included seemingly arbitrary measurements of feeding. For example, one study
measured breastfeeding after 1 week postpartum.44 The timing of assessment of breastfeeding
duration and introduction of solid foods was generally variable and inconsistent across studies.
The largest limitation of the evidence, however, is the quality of the included studies.
Most studies received a “poor” quality rating, due to multiple issues with both internal and
external validity. A body of evidence with such low certainty renders any magnitude of results
less meaningful; in this case, magnitude of results is unclear due to lack of measurement of
equal outcomes in the literature. However, even if the magnitude of results were consistent and
large across the studies, the poor quality of the body of evidence limits our ability to interpret the
results to make any recommendation regarding breastfeeding education.
Implications for Practice
The United States has much room for improvement in regards to breastfeeding rates
and introduction of solid foods at appropriate ages. The Healthy People goals repeatedly set
26 about the benefits of breastfeeding, optimal duration of breastfeeding, and optimal timing of
introduction of solid foods. Mothers may rely on a number of sources to learn about these
topics. Once the most effective, most reliable sources are confidently known, they can be
implemented into prenatal education, perhaps in the form of clinic visits, classes, or home visits.
Given the uncertainty regarding the base of evidence to date, the sources that should be
standardized in practice are unknown at this point. However, once the superiority of certain
sources are established, cost-effectiveness analysis could help determine the sources or modes
of education that are best suited to reach the masses in an affordable, sustainable way.
Implications for Research
This review points to the dire need for research comparing the effectiveness of different
sources of information or advice regarding infant feeding. While the IFPS II offers a large and
convenient sample to draw from, more RCTs comparing multiple sources of information are
needed. Our ability to compare different sources with each other is limited by the current
literature and trials comparing multiple sources to a control may help tease out the effectiveness
of each different source or intervention. Studies need to include the use of the Internet (both
reliable and unreliable websites) as a source of information to stay up to date with modern
information-seeking behavior.
Additionally, standardization of measurement of infant feeding outcomes is necessary in
order to draw evidence-based conclusions from further research about which sources of
information should be distributed to women. The current variation in measurement of
breastfeeding initiation, duration, and timing of introduction to solid foods renders results
synthesis difficult if not impossible. Standardizing outcome measurement to adherence to
national guidelines may increase future reviewers’ ability to compare studies to one another. In
addition, using standard definitions of “any breastfeeding” and “exclusive breastfeeding” are
27 As more literature emerges with better quality studies and more standardized measures
of exposures and outcomes, cost-effectiveness analysis should be used to determine which
sources are most feasible for implementation into practice. Expensive, intensive interventions
may be targeted to certain groups of women who are less likely to know about breastfeeding
and solid food recommendations. However, in order to feasibly reach a larger majority of women
and increase the chances of reaching the Healthy People 2020 goals, cost-effective measures
for educating women about infant feeding guidelines will be necessary.
Conclusions
A paucity of consistent, high-quality evidence exists regarding the best sources of
information and advice to educate mothers about infant feeding practices. Better quality studies
with more standardized measures of exposures and outcomes are needed to synthesize results
regarding modes of education for mothers. Once the best sources of information are assessed,
these can be implemented into practice in a cost-effective manner to improve adherence to
28 Acknowledgments
I would like to sincerely thank my advisor, Dr. Russell Harris, for all of his guidance and
assistance during this process and for teaching me the value of critical appraisal. I would also
like to thank my second reader, Dr. Kathy Andolsek, for helping Duke medical students navigate
this MPH program each year and for her continued support. Thank you to the directors and
registrar of the HC&P program, Dr. Anthony Viera, Dr. Sue Tolleson-Rinehart, and Ms. Sue
Robeson, for making this one of the best and most challenging academic years of my life and
for carrying on such a wonderful program. I am so grateful for all of the other wonderful MPH
students I met this year and the chance to learn with and be challenged by them.
29 References
1. Gunnarsdottir I, Schack-Nielsen L, Michaelsen KF, Sorensen TI, Thorsdottir I, NordNet Study Group. Infant weight gain, duration of exclusive breast-feeding and childhood BMI - two similar follow-up cohorts. Public Health Nutr. 2010 Feb;13(2):201-7.
2. Imai CM, Gunnarsdottir I, Thorisdottir B, Halldorsson TI, Thorsdottir I. Associations between Infant Feeding Practice Prior to Six Months and Body Mass Index at Six Years of Age. Nutrients. 2014 Apr 17;6(4):1608-17.
3. Weng SF, Redsell SA, Swift JA, Yang M, Glazebrook CP. Systematic review and meta-analyses of risk factors for childhood overweight identifiable during infancy. Arch Dis Child. 2012 Dec;97(12):1019-26.
4. Weyermann M, Rothenbacher D, Brenner H. Duration of breastfeeding and risk of overweight in childhood: a prospective birth cohort study from Germany. Int J Obes. 2006;30:1281-7.
5. Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2002;(1):CD003517.
6. Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2012 Aug 15;8:CD003517.
7. Dogaru CM, Nyffenegger D, Pescatore AM, Spycher BD, Kuehni CE. Breastfeeding and Childhood Asthma: Systematic Review and Meta-Analysis. Am J Epidemiol. 2014 Apr 11 [Epub ahead of print].
8. Debes AK, Kohli A, Walker N, Edmond K, Mullany LC. Time to initiation of breastfeeding and neonatal mortality and morbidity: a systematic review. BMC Public Health. 2013;13 Suppl 3:S19.
9. Hornell A, Lagstrom H, Lande B, Thorsdottir I. Breastfeeding, introduction of other foods and effects on health: a systematic literature review for the 5th Nordic Nutrition
Recommendations. Food Nutr Res [Internet]. 2013 Apr 12 [cited 2014 Apr 22];57. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3625706/
10. Magnussen CG, Koskinen J, Juonala M, Chen W, Srinivasan SR, Sabin MA, et al. A diagnosis of the metabolic syndrome in youth that resolves by adult life is associated with normalization of high carotid intima-media thickness and type 2 diabetes mellitus risk: the Bogalusa heart and cardiovascular risk in Young Finns studies. J Am Coll Cardiol. 2012 Oct 23;60(17):1631-9.
11. Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and
adolescence on morbidity and premature mortality in adulthood: a systematic review. Int J Obes. 2011 July;35(7):891-8.
12. World Health Organization [Internet]. WHO 2014 [last update unknown; cited 2014 April 19]. The World Health Organization's infant feeding recommendation. Available from:
http://www.who.int/nutrition/topics/infantfeeding_recommendation/en/
13. American Academy of Pediatrics. [last update unknown; cited 2014 April 19]. Infant - food and feeding. Available from: http://www.aap.org/en-us/advocacy-and-policy/aap- health-initiatives/HALF-Implementation-Guide/Age-Specific-Content/Pages/Infant-Food-and-Feeding.aspx#none
14. CDC National Center for Chronic Disease Prevention and Health Promotion Division of Nutrition, Physical Activity, and Obesity. Breastfeeding Report Card: United States 2013 [Internet]. Atlanta; July 2013 [cited 2014 April 22]. Available from:
http://www.cdc.gov/breastfeeding/pdf/2013breastfeedingreportcard.pdf
15. Fein SB, Grummer-Strawn LM, Raju TN. Infant feeding and care practices in the United States: results from the Infant Feeding Practices Study II. Pediatrics. 2008 Oct;122 Suppl 2:S25-7.
30 17. Fein SB, Labiner-Wolfe J, Shealy KR, Li R, Chen J, Grummer-Strawn LM. Infant
Feeding Practices Study II: Study Methods. Pediatrics. 2008 Oct 1;122(Suppl 2):S28-S35.
18. Singh GK, Kogan MD, Dee DL. Nativity/immigrant status, race/ethnicity, and
socioeconomic determinants of breastfeeding initiation and duration in the United States, 2003. Pediatrics. 2007 Feb;119 Suppl 1:S38-S46.
19. Wolf JH. Low Breastfeeding Rates and Public Health in the United States. Am J Public Health. 2003 Dec;93(12):2000-10.
20. Gross RS, Mendelsohn AL, Fierman AH, Hauser NR, Messito MJ. Maternal infant feeding behaviors and disparities in early childhood obesity. Child Obes. 2014 Apr;10(2):145-52.
21. Lynch S, Bethel J, Chowdhury N, Moore JB. Rural and urban breastfeeding initiation trends in low-income women in North Carolina from 2003 to 2007. J Hum Lact. 2012 May;28(2):226-32.
22. Wasser H, Bentley M, Borja J, Davis Goldman B, Thompson A, Slining M, Adair L. Infants perceived as “fussy” are more likely to receive complementary foods before 4 months. Pediatrics. 2011 Feb;127(2):229-37.
23. Fein SB, Labiner-Wolfe J, Scanlon KS, Grummer-Strawn LM. Selected complementary feeding practices and their association with maternal education. Pediatrics. 2008 Oct;122 Suppl 2:S91-7.
24. Kogan MD, Singh GK, Dee DL, Belanoff C, Grummer-Strawn LM. Multivariate analysis of state variation in breastfeeding rates in the United States. Am J Public Health. 2008 Oct;98(10):1872-80.
25. Murtagh L, Moulton AD. Working mothers, breastfeeding, and the law. Am J Public Health. 2011 Feb;101(2):217-23.
26. Heymann J, Raub A, Earle A. Breastfeeding policy: a globally comparative analysis. Bulletin of the World Health Organization. 2013;91:398-406.
27. Schanler RJ, O’Connor KG, Lawrence RA. Pediatricians’ practices and attitudes regarding breastfeeding promotion. Pediatrics. 1999;103(3).
28. Philipp BL, Merewood A, O’Brien S. Physicians and breastfeeding promotion in the United States: a call for action. Pediatrics. 2001 Mar;107(3):584-7.
29. Johnson AM, Correll A, Greene JF, Hein D, McLaughlin T. Barriers to breastfeeding in a resident clinic. Breastfeed Med. 2013 Jun;8(3):273-6.
30. Lewallen LP, Street DJ. Initiating and sustaining breastfeeding in African American women. J Obstet Gynecol Neonatal Nurs. 2010 Nov-Dec;39(6):667-74.
31. Horodynski M, Olson B, Arndt MJ, Brophy-Herb H, Shirer K, Shemanski R. Low-income mothers’ decisions regarding when and why to introduce solid foods to their infants: influencing factors. J Community Health Nurs. 2007 Summer;24(2):101-18.
32. Johnston ML, Esposito N. Barriers and facilitators for breastfeeding among working women in the United States. J Obstet Gynecol Neonatal Nurs. 2007 Jan-Feb;36(1):9-20. 33. Bentley M, Gavin L, Black MM, Teti L. Infant feeding practices of low-income,
African-American, adolescent mothers: an ecological, multigenerational perspective. Soc Sci Med. 1999 Oct;49(8):1085-100.
34. Heinig MJ, Ishkii KD, Banuelos JL, Campbell E, O’Loughlin C, Vera Becerra LE. Sources and acceptance of infant-feeding advice among low-income women. J Hum Lact. 2009 May;25(2):163-72.
35. Bunik M, Clark L, Zimmer LM, Jimenez LM, O’Connor ME, Crane LA, Kempe A. Early infant feeding decisions in low-income Latinas. Breastfeed Med. 2006 Winter;1(4):225-35.
31 Review and Meta-Analysis for the US Preventive Services Task Force. Annals of Family Medicine. 2003 July/Aug;1(2):70-78.
37. Gildea A, Sloan S, Stewart M. Sources of feeding advice in the first year of life: who do parents value? Community Pract. 2009 Mar;82(3):27-31.
38. Odom EC, Li R, Scanlon KS, Perrine CG, Grummer-Strawn L. Association of Family and Health Care Provider Opinion on Infant Feeding with Mother’s Breastfeeding Decision. J Acad Nutr Diet. 2013 Nov 5. pii: S2212-2672(13)01289-6.
39. Racine EF, Frick K, Guthrie JF, Strobino D. Individual net-benefit maximization: a model for understanding breastfeeding cessation among low-income women. Matern Child Health J. 2009 March;13(2):241-9.
40. Rhodes KL, Hellerstedt WL, Davey CS, Pirie PL, Daly KA. American Indian
breastfeeding attitudes and practices in Minnesota. Matern Child Health J. 2008 Jul;12 Suppl 1:46-54.
41. Campbell LA, Wan J, Speck PM, Hartig MT. Women, Infant, and Children (WIC) peer counselor contact with first time breastfeeding mothers. Public Health Nurs. 2014 Jan-Feb;31(1):3-9.
42. Chen PG, Johnson LW, Rosenthal MS. Sources of education about breastfeeding and breast pump use: what effect do they have on breastfeeding duration? An analysis of the Infant Feeding Practices Survey II. Matern Child Health J. 2012 Oct;16(7):1421-30. 43. Reifsnider E, Eckhart D. Prenatal breastfeeding education: its effect on breastfeeding
among WIC participants. J Hum Lact. 1997 Jun;13(2):121-5.
44. Sandy JM, Anisfeld E, Ramirez E. Effects of a prenatal intervention on breastfeeding initiation rates in a Latina immigrant sample. J Hum Lact. 2009 Nov;25(4):404-11. 45. Petrova A. Ayers C, Stechna S, Gerling JA, Mehta R. Effectiveness of exclusive
breastfeeding promotion in low-income mothers: a randomized controlled study. Breastfeed Med. 2009 Jun;4(2):63-9.
46. Betzold CM, Laughlin KM, Shi C. A family practice breastfeeding education pilot program: an observational, descriptive study. Int Breastfeed J. 2007 Mar 5;2:4. 47. Pugh LC, Milligan RA. Nursing intervention to increase the duration of breastfeeding.
Appl Nurs Res. 1998 Nov;11(4):190-4.
48. Brent NB, Redd B, Dworetz A, D’Amico F, Greenberg JJ. Breast-feeding in a low income population. Program to increase incidence and duration. Arch Pediatr Adolesc Med. 1995 Jul;149(7):798-803.
49. Scheinmann R, Chiasson MA, Hartel D, Rosenberg TJ. Evaluating a bilingual video to improve infant feeding knowledge and behavior among immigrant Latina mothers. J Community Health. 2010 Oct;35(5):464-70.
50. Clayton HB, Li R, Perrine CG, Scanlon KS. Prevalence and reasons for introducing infants early to solid foods: variations by milk feeding type. Pediatrics. 2013
Apr;131(4):e1108-14.
51. Black MM, Siegel EH, Abel Y, Bentley ME. Home and videotape intervention delays early complementary feeding among adolescent mothers. Pediatrics. 2001
May;107(5):E67.
52. US Preventive Services Task Force. Primary Care Interventions to Promote
32 APPENDICES
Appendix 1. Search Strategy
1. "Health Knowledge, Attitudes, Practice"[Mesh] OR knowledge[tw] OR belief*[tw] OR practice*[tw] OR opinion*[tw] OR attitude*[tw] OR reason*[tw] OR perception*[tw] OR thought*[tw] OR influence*[tw]
2. "Infant"[Mesh] OR infant*[tw] OR newborn* OR young child*[tw])
3. "Parents"[Mesh] OR parent*[tw] OR mother*[tw] OR father*[tw] OR caregiver*[tw] 4. "Feeding Behavior"[Mesh] OR feeding[tw] OR breastfeeding[tw]
5. decision making [mesh] OR decision*[tw] OR choice*[tw] OR behavior*[tw] 6. united states[mesh] OR united states[tw]
33 Appendix 2. Quality Assessment
35 Figure A1.
USPSTF Criteria for Rating Strength of Evidence
1. Do the studies have the appropriate research design to answer the key question(s)? 2. To what extent are the existing studies of high quality? (i.e., what is the internal validity?) 3. To what extent are the results of the studies generalizable to the general U.S. primary
care population and situation? (i.e., what is the external validity?)
4. How many studies have been conducted that address the key question(s)? How large are the studies? (i.e., what is the precision of the evidence?)
5. How consistent are the results of the studies?
6. Are there additional factors that assist us in drawing conclusions (e.g., presence or absence of dose-response effects, fit within a biologic model)?
From USPSTF Website:
http://www.uspreventiveservicestaskforce.org/uspstf07/methods/benefit.htm
36
Citation Potential for selection bias Potential for measurement bias Potential for confounding
Analysis Precision Overall internal validity External validity Overall Quality Rating Odom et al. 201338
Medium to High
Consumer opinion panel of 500,000 homes with pregnant women in third trimester; not nationally representative
We don't know the
characteristics of the 33% of women with incomplete data
Women in the IFPS II were more likely to be white, married, educated, and breastfed overall at higher rates than national averages High Measured provider and family members' opinions on infant feeding styles by asking for mothers' self-report, which could be inaccurate and relies totally on mothers' perception of the information providers gave
Did not explain how they measured breastfeeding and chose to use outcome of "never breastfed" meaning that those who did could fall into many categories of breastfeeding Medium Controlled for maternal age, race, parity, marital status, education, poverty, and WIC participation
Could be other factors related to the women who were able to fully complete the surveys that confound Adjusted for factors described previously
Report odds ratios of never breastfeeding for infant's father, maternal grandmother, paternal grandmother, doctor, and mother's doctor for opinions of
breastfeeding only, breastfeeding and formula, formula only, or don't know, using breastfeeding only as reference
Fair - wide confidence intervals
Poor
High potential for selection bias due to uncertainty of differences b/w group with incomplete data, high degree of measurement bias Fair
All U.S. women on a consumer opinion panel, but women were not nationally representative and were more likely to be married, white, and educated and had higher breastfeeding rates than the U.S. overall
37
Citation Potential for selection bias Potential for measurement bias Potential for confounding
Analysis Precision Overall internal validity External validity Overall Quality Rating Racine et al. 200839 High No information given on how sites selected or how those who enrolled may have been different from source population No explanation of mising data
Only included women who initiated
breastfeeding in the study, thus leaving out possible
disincentives for any woman who chose not to breastfeed High Measure breastfeeding as "any breastfeeding" which captures a wide variety of feeding types, from breastfed once to exclusively breastfed for a year
Reliance on maternal self-report for dis-incentives related to information and breastfeeding Medium Controlled for significant factors determined from literature, qualitative analyses, and experts However, only included women who ever breastfed Survival analysis with "event" classified as discontinuation of breastfeeding at X weeks
Controlled for 6 demographic variables found to be significantly associated with disincentives Full model included only those variables that were significant in each "domain" of disincentives Fair to High; small confidence intervals Poor
High potential for selection and measurement bias
Study design and analysis strategy is confusing - looking at "disincentives" and discontinuation of breastfeeding (negatively-connotated factors) rather than positively connotated factors such as sources of positive advice which is more consistent with previous literature Poor Low-income women only recruited from select clinics of the Healthy Steps National
Evaluation; don't have information about where they came from or whether source population is nationally representative
38
Citation Potential for selection bias Potential for measurement bias Potential for confounding
Analysis Precision Overall internal validity External validity Overall Quality Rating Rhodes et al. 200840 High Women recruited from 4 clinics; women who agreed to participate may be different from rest of population
High Measured sources of information/advice as perceived encouragement to breastfeed from different sources, which relies on mother's report and perceptions which could be inaccurate
Only studied mothers who had initiated
breastfeeding
No differentiation between types of breastfeeding (breastfeeds exclusively,
breastfeeds once a week with the rest formula, etc.)
Medium to High
Controlled statistically for attitudinal factors related to breastfeeding, some demographic variables
Did not control for age, previous breastfeeding experience, WIC recipient
Chi-squared tests for each separate variable
Logistic regression with odds ratios reported for initiation and duration of breastfeeding for each variable that was significant in Chi-squared analysis
Do not report OR past initiation for women who received advice from
boyfriend/husband and do not report OR past 2 weeks for women who received advice from mother Fair Confidence intervals reasonably narrow Poor Prospective cohort method with volunteer participants introduces selection bias; in addition basic characteristics of women who entered the study not fully
described
Measurement bias inherent in mother's perceptions and self-report and lack of definition of breastfeeding styles Poor Only American Indian women from 4 clinics in Minnesotra; narrow if any applicability to other U.S. populations
39
Citation Potential for selection bias
Potential for measurement bias
Potential for confounding
Analysis Precision Overall internal validity External validity Overall Quality Rating Campbell et al. 201441 High Poor description of how study population was recrutied (3,070 WIC-enrolled women at 1-year subcertification visit); no
description of how many women dropped out, why, or whether they were different from group who completed surveys No demographic comparison between group who received peer contact vs. group who did not
High
Measured breastfeeding by self-report and did not differentiate whether they used baby currently fed breastmilk or baby ever fed breastmilk as outcome measure Measured peer counselor contact pre-pregnancy, during hospitalization, and after baby was born by self-report when baby is 1 year old - high risk of recall bias
High
Again, no clear description of difference in demographics between control and intervention groups - no idea of differences in race, education, SES, language spoken, previous births, etc. between the two groups
Mothers may have interpreted actual WIC counselor as a peer counselor (no description of difference between the two)
% Breastfed and OR for peer counselor contact vs. no peer counselor contact during pregnancy, during hospitalization, and after birth Fair, large sample size Poor Poor description of sampling methods, handling of missing data, demographic characteristics of intervention vs. control groups, poor measurement of variables, unclear which outcome variable was used as main outcome
Fair
Large sample size in TX likely somewhat applicable to rest of U.S. but unclear whether WIC peer counselors are used or available in other states
40
Citation Potential for selection bias Potential for measurement bias Potential for confounding
Analysis Precision Overall internal validity External validity Overall Quality Rating Chen et al. 201242 Fair to High IFPS II again - same as above High Recall bias Poor measurement of education sources - asked retrospectively, only of women who ever breastfed
Low
Controlled for many factors including race/ethnicity, age, maternal education, marital status, residence in metropolitan area, income, WIC enrollment, Edinburgh postnatal depression score, intention to work within first year, prior breastfeeding experience, number of problems breastfeeding in first 2 weeks, use of breast bump, friends/relatives who breastfed Compared sources of education between "short duration" of breastfeeding (<2 months) and "long duration" of breastfeeding (> 2 months), reported as OR with short duration group as reference
Fair Poor
Controlled for many potential
41
Citation Potential for selection bias Potential for measurement bias Potential for confounding
Analysis Precision Overall internal validity External validity Overall Quality Rating Reifsnider & Eckhart 199743 High
Groups different at baseline -
experimental group younger, more likely to be
married, and more likely to be
multiparous then control group (authors report that groups are similar at baseline)
Participants not truly randomized
Desire to
breastfeed one of eligibility criteria - subjects in each group may be more likely to breastfeed than other women
High
Measured breastfeeding
duration indirectly, by waiting until mother asked for formula voucher at appointment and then asking for recall of time of
discontinuation
WIC clerks recorded information about breastfeeding, not blinded to study group assignment
Medium to High
Apparently
controlled for some variables using randomization, but age, marital status, and parity were not actually equal between groups at baseline
All participants indicated desire to breastfeed
Descriptive statistics only
N/A Poor
Selection, sample size, randomization, measurement, and analysis problems Poor
42
Citation Potential for selection bias Potential for measurement bias Potential for confounding
Analysis Precision Overall internal validity External validity Overall Quality Rating Sandy et al. 200944 Medium RCT study design should lower risk of selection bias, but randomization process and characteristics between exposed and unexposed groups not clearly explained
No description of differences with group that did not complete the study or how missing data were treated
High
Measured exposure as 1 or more prenatal visists; records likely accurate but did not classify exposed as being randomized to the intervention group but rather whether the exposure actually occurred
Breastfeeding measured by family support workers asking mothers questions about feeding style within first 7 days of birth; most were asked on 3rd day of birth; this gives very little information about how mothers are actually
breastfeeding their children over the long term Medium Controlled for many factors including age, parity, education, acculturation score, mother's contribution to family income, father involvement, hospital location, method of delivery
Did not control for previous
breastfeeding experience, income, work status, etc.
No ITT analysis
Calculated OR for any breastfeeding (ABF) and exclusive breastfeeding (EBF) within first week of birth for "exposed" vs. "unexposed" group (NOT for intervention vs. control group)
Lack of blinding for participants and for data collectors (FSWs knew whether woman was in intervention or control group when assessing breastfeeding status)
Fair Poor
Lack of blinding or ITT analysis
Lack of information about randomization, missing data handling, and differences between the intervention and control groups Controlled for many potential confounders Measuring breastfeeding only within first week
postpartum does not give us much information about likely long-term practices Poor Latina immigrant study sample with psychosocial risk factors for caregiving problems Most participants were Dominican immigrants living in NYC and eligible for a special home visitation program, likely not applicable to all U.S. women