http://dx.doi.org/10.4236/health.2016.89089
A Health Impairment Process of Sickness
Presenteeism in Norwegian Physicians:
The Mediating Role of Exhaustion
Sylvi Thun1, Lise T. Løvseth2
1Department of Psychology, Norwegian University of Science and Technology (NTNU), Trondheim, Norway
²Department of Research and Development, Division of Psychiatry, St Olav’s Hospital, Trondheim, Norway
Received 4 May 2016; accepted 12 June 2016; published 15 June 2016
Copyright © 2016 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/
Abstract
Although work factors have been associated with both presenteeism and exhaustion among hos-pital physicians, we lack knowledge on the dynamic relationship between demands in the work context and presenteeism and how this can be mediated by symptoms of exhaustion when con-trolling for job resources. The objective of this study is to examine a health impairment process of presenteeism among university hospital physicians. A cross-sectional survey of 545 university hospital physicians in Norway was conducted. Variables included in the model were presenteeism, exhaustion, work-family conflict, role conflict, social support and control over work pace. Findings from structural equation modeling indicated that exhaustion mediates the relationship between job demands and presenteeism. Job resources had no direct effect on presenteeism in the hy-pothesized model. The variables in the study explained 17% of the variance in presenteeism. The study is one of the first to demonstrate that the relationship between job demands and presentee-ism is mediated by exhaustion when controlling for job resources. The results highlight the im-portance of considering the link between health symptoms and job demands to reduce the nega-tive effects of presenteeism.
Keywords
Sickness Presenteeism, Exhaustion, Job Demands, Job Resources, JD-R Theory
1. Introduction
exhaus-tion as a symptom of burnout [1]-[4] and attend work despite their own ill-health, a phenomenon termed sick-ness presenteeism [5]-[8]. Though exhaustion and presenteeism have been associated with similar work and personal factors, only a few studies have indicated a relationship between these health behaviors [8]-[10]. We also lack studies that examine the dynamic relationship between these factors and their relative contribution to a health impairment process manifested by exhaustion and presenteeism. This knowledge is vital to initiate inter-ventions that can reduce both exhaustion and unwanted presenteeism among physicians. An important step is to examine how exhaustion mediates the relationship between factors in the work context and presenteeism within an established model of occupational stress such as the Job-Demand-Resources (JD-R) model.
A recent meta-analysis on the correlates of presenteeism concluded that significant contributors are job de-mands and perceived stress, negative relational experiences, positive attitudes, and lack of personal and job re-sources [11]. This is concordant with studies that show a high rate of sickness presence and low sickness ab-sence among professionals with high job demands and those who report that their skills and tasks are difficult to allocate to others [12], such as physicians in academic medicine [5] [6] [13]. Their high demands at work com-bined with family responsibilities can compromise sufficient self-care, restitution, and rest [14] which in turn can contribute to exhaustion and presenteeism. Work tasks in the healthcare service may also stimulate presen-teeism because of high work engagement or professional obligations [11]. To understand better the dynamic re-lationship between work characteristics, exhaustion, and presenteeism it is vital to examine these associations in an occupation that manifests high prevalence of presenteeism such as that of hospital physicians [5] [8].
The JD-R model is a theoretical model of occupational stress that conceptualizes the relationship between employee well-being and job performance. The theory is based on the assumption that all working environments constitute job demands and job resources [15] [16]. Job resources are defined as the physical, social, and organ-izational features of work that can reduce job demands and are functional in achieving work goals [17]. In con-trast, job demands refer to psychological, social, physical, or organizational features of the job that require sus-tained personal effort and are related to some psychological and/or physiological costs [18]. These include a va-riety of distinct variables that constitute role demands (e.g., role conflict), time demands (e.g., long hours, shift work) and relational demands (e.g., work-family conflict) [11]. The JD-R theory states that the dynamic rela-tionship between job demands and resources triggers either a health impairment process or a motivational process. Accordingly, the current study emphasizes that job demands are the most important predictors of occu-pational strain such as exhaustion which in turn predict job performance whereas resources are the most impor-tant predictor of work engagement [16] [19]. In contrast to studies that have examined the direct relationship between work factors and presenteeism, the current study suggests that job demands can have an effect on well-being and indirectly influence performance. Considering the health impairment process, we examine if presenteeism as a sign of strain is directly ameliorated by job demands or indirectly through exhaustion as a me-diator of presenteeism.
As emotional exhaustion may develop as a consequence of demanding cognitive, affective, and physical strain [20] it can mediate the health impairment process manifested by presenteeism among physicians. Al-though studies have confirmed a relationship between presenteeism and exhaustion [8] [9], research on the spe-cific link between these two behaviors is inconclusive. One study has suggested that emotional exhaustion is an important target when the aim is to reduce presenteeism [21]. Others suggest a reciprocal relationship between presenteeism and exhaustion because exhausted employees most likely mobilize “compensation strategies” while they attend work when ill [9]. The current study examines the relative influence of different work de-mands on physicians’ exhaustion which in turn can contribute to presenteeism.
Attending work while ill can be regarded as controversial as it can pose high health risks to the person and the patients. However, certain job demands pose high attendance pressure that contributes to presenteeism among physicians [7]. An important job demand that influences psychosocial work climate and generates job-related strain is role conflict [22]. Role conflict is the result of a lack of congruent expectations and demands from other people in the workplace and increases exhaustion [23].
A work-family conflict can contribute to presenteeism when work demands force work attendance on behalf of staying home to care a sick child or workers’ personal need for restitution, leisure, and rest [30].
In contrast to job demands, job resources such as control over work pace are relevant factors to control for in the health impairment process of presenteeism. Control over work pace refers to the subject’s perceived control of time and pace in his or her work [31]. Employees who manifest high presenteeism often work under condi-tions characterized by time pressure. Despite their poor health they still make a considerable effort to carry out their work duties [32]. It is important to have control over work pace [33] and to get adequate rest to recover and recharge psychologically and physically after demanding efforts at work [34] [35]. In a very demanding job, the decision to be absent or present will vary with work pace [36].
Another important resource in research on presenteeism is social support. Social support refers to perceptions that one has access to helpful relationships of varying quality or strength [37]. Presenteeism is associated with supervisor support and subjective health [38]. Support from colleagues is important for well-being and buffers the negative effects of work stress [39]. It is important to investigate the relative importance of job resources in relation to presenteeism to increase knowledge on how employees respond to the strains of being sickness present [40]. Though job control and social support are regarded as the most important job resources to coun-terweigh job demands in that workers who experience “being in control” and have a supportive workplace will be less likely to feel pressure to attend when ill [11]. Studies have examined the relative influence of job control and social support on presenteeism [38] [41]-[44].
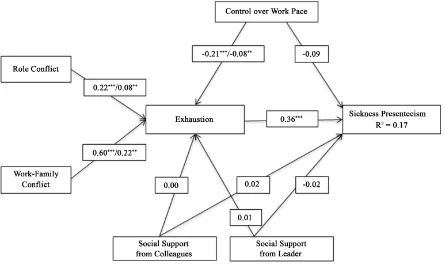
The objective of this study is to examine the dynamic relationship between different job demands and presen-teeism mediated by exhaustion by simultaneously controlling job resources such as control over work pace and social support. This contributes to presenteeism literature by investigating the mediating effect of the em-ployee’s health symptoms in the relationship between different job demands and presenteeism, and we control for the two most salient job resources when investigating the health impairment process. According to the JD-R model and the above-mentioned empirical work, the hypotheses of this study are (illustrated inFigure 1):
Hypothesis 1. Exhaustion is positively related to sickness presenteeism.
Hypothesis 2a. Role conflict is positively related to exhaustion and sickness presenteeism.
[image:3.595.94.539.420.685.2]Hypothesis 2b. Work-family conflict is positively related to exhaustion and sickness presenteeism.
Hypothesis 3a. Exhaustion positively mediated the positive relationship between work-family conflict and sickness presenteeism when controlling for control over work pace and social support.
Hypothesis 3b. Exhaustion positively mediated the positive relationship between role conflict and sickness presenteeism when controlling for control over work pace and social support.
Hypothesis 4. Control over work pace and social support is negatively related to sickness presenteeism.
2. Method
2.1. Participants and Procedure
This study included data from all participants in a study concerning work-related health, organizational culture, and working conditions among physicians in a Norwegian university hospital conducted from February to May 2012. The participants received a letter containing a personal link to a web-based questionnaire and were asked to provide their responses anonymously. The survey was conducted in English. The inclusions criteria were em-ployment as full-time or part-time physicians actively working at the time of data collection. The project was approved by the administration of the hospital, the union representatives of the physicians at the hospital, and the Regional Ethics Board. In addition to a short oral presentation given in organizational forums, all partici-pants received a letter with a description of the study. All physicians voluntarily participated and completed the informed consent form that was required for participation in the study. The total response rate was 71.8% (N = 545/759). Of these responses, 45% (n = 245) were female physicians. A response analysis showed that the sam-ple was representative according to age, gender, and position.
2.2. Measures
The questionnaire contained 123 items concerning education, work-related health, organizational culture, and working conditions. The study was based on a selection of variables relevant to the current foci and included presenteeism, exhaustion, role conflict, work-family conflict, control over work pace, social support from col-leagues, and social support from supervisors.
2.2.1. Sickness Presenteeism
The item “Have you gone to work with an illness in a situation where you would have recommended a patient to stay home? How often has this happened during the last 12 months?” measured sickness presenteeism [6]. The response was rated “none” (1), “once” (2), “2-4 times” (3) and “more than five times” (4).
2.2.2. Exhaustion
Exhaustionwas measured by a miniature version of the Oldenburg Burnout Inventory [20]. Exhaustion (α = 0.73) was measured by five items, and the response scale ranged from 1 = “totally agree” to 4 = “totally disagree”. “After my work, I now need more time to relax than in the past to become fit again” was one item measuring exhaustion. The index included both positively and negatively worded items. The positive and negative items were presented in random order, and the negatively worded items were reversed.
2.2.3. Role Conflict
The three items measuring role conflict were derived from the General Nordic Questionnaire for Psychological and Social Factors at Work (QPS Nordic) [45]. The role conflict questions consisted of items about conflicts between demands and resources, conflicting requests, and conflicts between the subject’s expectations and ex-ternal demands [31]. For example, “Do you receive incompatible requests from two or more people?” was measured from 1 = “very seldom or never” to 5 = “very often or always”. The alpha of this scale (α = 0.68) cor-responded to the validation data on QPS Nordic [46].
2.2.4. Work-Family Conflict
2.2.5. Control over Work Pace
The items for the variable “control over work pace” were derived from QPS Nordic [45]. Control over work pace consisted of four items (α = 0.83), and the response ranged from “very seldom or never” (1) to “very often or always” (5). The items are about setting work pace, deciding the length and time of breaks, and setting work-ing hours (flexitime) [31]. The alpha of the scale corresponded to the validation data on QPS Nordic [46].
2.2.6. Social Support
Social support was measured by the item “How much can people as listed below be relied upon for support when things get tough at work?” [47] [48]. The item was rated with references to the immediate supervisor and the physicians’ colleagues (in their work unit), respectively. Responses were on a five-point scale ranging from “not at all” (1) to “very much” (5). A high score for each item of support indicated high levels of support.
2.3. Analysis
A confirmatory factor analysis (CFA) using IBM SPSS AMOS version 22 evaluated the outcome data. We per-formed structural equation modeling (SEM) to test our hypothesized model (Figure 1) based on criteria includ-ing: 1) root-mean-square error of approximation (RMSEA) of 0.06 or less indicating good fit; 2) a comparative fit index (CFI) equal to or greater than 0.95; and 3) standardized root mean square residual (SRMR) of 0.08 or less [49].
Missing value analysis was conducted with the maximum likelihood (ML) estimation in IBM SPSS Statistics version 22. We investigated modification indices of the measurement model and co-varied some of the error terms on a theoretical basis. A bootstrapping procedure with bias-corrected intervals was conducted to test the indirect effects. This used 1000 bootstraps and a 95% confidence interval. The assumptions for performing SEM in AMOS were satisfactory. A curve estimation for all the relationships in the model showed that they were suf-ficiently linear. The assumption of no multicollinearity was confirmed.
3. Results
3.1. Descriptive Statistics
Table 1shows details of the constructs and associated items. The model fits for the confirmatory factor analyses (measurement model) are reported as a note inTable 1. Physicians scored a mean of 3.09 on the question “Have you gone to work with an illness in a situation where you would have recommended a patient to stay home?”. Information on the descriptive statistics, correlation, and squared correlations (R2) between the variables is pre-sented inTable 2.
3.2. The Measurement Model
The measurement model (Table 1) demonstrated a good fit to the data: χ2 (114) = 231.16, p < 0.001, a good-ness-of-fit index (GFI) of 0.956, a CFI of 0.963, a Tucker-Lewis Index (TLI) of 0.951, an SRMR of 0.043, and an RMSEA of 0.043 [49] [50]. As shown inTable 1, the Cronbach’s alpha and composite reliability coefficients (CR) of the multiple-item measures displayed good internal consistency. Further support for convergent validity as well as discriminant validity was indicated by composite reliability coefficients greater than the recommend-ed 0.7 and average variance extractrecommend-ed (AVE) estimates meeting the critical value of 0.5 [50]. For one measure, the alpha was a little below the commonly accepted threshold of 0.70. However, this is considered acceptable for measures that have a small number of items [51]. Two variables had AVE values below the critical value of 0.5, indicating some validity concerns.
3.3. Results of the Testing of Hypotheses
Hypothesis 1 that exhaustion was positively related to presenteeism was confirmed (β = 0.36, p < 0.001). Pear-son correlational analysis confirmed Hypothesis 2, indicating a positive relationship between job demands and exhaustion, and job demands and presenteeism. Of the job demands, work-family conflict demonstrated strong-est relationship with both presenteeism (r = 0.28, p < 0.01) and exhaustion (r = 0.55, p < 0.01) (seeTable 2).
Table 1. Measurement model. Result of confirmatory factor analysis for all study measures.
Construct and Indicators Mean (M)
Standard Deviation
(SD)
Standardized Beta (β)
Average Variance Extracted
(AVE)
Composite Reliability
(CR)
Cronbach’s Alpha (α)
Sickness presenteeism
Have you gone to work with an illness in a situation where you would have recommended
a patient to stay at home?
3.09 1.06
How often has this happened
during the last 12 months? 2.47 0.89
Exhaustion 0.35 0.72 0.73
There are days when I already feel tired
before I go to work (r) 2.69 0.75 0.63 After my work, I now need more time to
relax than in the past to become fit again (r) 2.41 0.77 0.62
I can stand the pressure of my work very well 2.10 0.63 0.45
After my work, I usually still feel totally
fit for my leisure activities 2.54 0.71 0.60
After my work, I usually feel worn out and weary (r) 2.55 0.76 0.63
Role Conflict 0.41 0.68 0.68
Do you have to do things that
you feel should be done differently? 2.76 0.92 0.56 Are you given assignments without
adequate resources to complete them? 2.77 1.01 0.68 Do you receive incompatible requests
from two or more people? 2.31 0.98 0.67
Work-family Conflict 0.64 0.86 0.84
When I get home from work I am often too frazzled to
participate in family activities/responsibilities (r) 2.23 0.69 0.86 I am often so emotionally drained when I get home from
work that it prevents me from contributing to my family (r) 2.03 0.72 0.79 Because of all the pressures at work, sometimes when
I come home I am too stressed to do the things I enjoy (r) 2.41 0.78 0.82
Work Pace 0.57 0.84 0.83
Can you set your own work pace? 2.72 1.08 0.65 Can you decide yourself when
you are going to take a break? 3.06 1.09 0.89 Can you decide the length of your break? 2.80 1.06 0.89
Can you set your own working hours? 1.99 1.18 0.53
Social Support Leader How much can people as listed below be relied on for support when things get tough at work? Immediate superior
3.59 1.23
Social Support Colleagues How much can people as listed below
be relied on for support when things get tough at work? Physician colleagues in your work unit
4.01 0.99
Note: Fit Indices: χ2 = 231.16, df = 114, p < 0.001, χ2/df = 2.028, GFI = 0.956, CFI = 0.963, SRMR = 0.043, TLI = 0.951, RMSEA = 0.043, PCLOSE
Table 2. Means (M), Standard Deviations (SD), and correlations (Pearson’s r) for the sample (N = 545).
Mean (M)
Standard
Deviation (SD) 1 2 3 4 5 6 7
1. Sickness Presenteeism 2.47 0.89 0.17
2. Exhaustion 2.21 0.68 0.30**
0.62
3. Role Conflict 2.61 0.76 0.17** 0.30** -
4. Work-Family Conflict 2.22 0.63 0.28** 0.55** 0.32** -
5. Work Pace 2.46 1.05 −0.25** −0.28** −0.19** −0.17** -
6. Social Support Leader 3.59 1.23 −0.14** −0.23** −0.24** −0.29** 0.22** -
7. Social Support Colleagues 4.01 0.99 −0.12** −0.24** −0.19** −0.32** 0.19** 0.48** -
Note: **p < 0.01. R² of dependent variables in bold.
one SD increased presenteeism by 0.22 SD mediated by exhaustion. There was also an effect of role conflict on presenteeism mediated by exhaustion (β = 0.08, p < 0.01). Hypothesis 3 was supported. We examined the indi-rect effects based on bootstrapped confidence intervals to test the mediation hypotheses. The indiindi-rect effects were confirmed at the 95% level of significance.
There was a negative correlation between presenteeism and work pace (r = −0.25, p < 0.01), presenteeism and social support from leader (r = −0.14, p < 0.01), and presenteeism and social support from colleagues (r = −0.14, p < 0.01). In the SEM analysis where we controlled for job resources there was no direct association between the job resources and presenteeism (seeFigure 1). In addition, control over work pace had a negative indirect effect on presenteeism; however, this was not hypothesized (β = −0.08, p < 0.01). Hypothesis 4 that job resources were negatively related to presenteeism was partly confirmed.
The health impairment process of presenteeism was confirmed, and the hypothesized model had a good fit to the data (χ2
(116) = 231.23, p < 0.001, GFI = 0.956, CFI = 0.964, SRMR = 0.043, TLI = 0.953, and RMSEA = 0.043). The results confirmed direct effects between exhaustion and presenteeism. In addition to mediating ef-fects of variables in the model (Figure 1), the explained variance of presenteeism was 17% (Table 2).
4. Discussion
The results of this study confirmed a positive relationship between presenteeism and exhaustion, and that ex-haustion mediates the relationship between job demands and presenteeism. The results support the occurrence of a health impairment process and contribute to the existing literature by simultaneously looking at different kinds of job demands in relation to presenteeism and how this relationship is mediated by exhaustion. We found that job demands can have an indirect association with presenteeism. This indicates that a mere focus on a reduction of either job demands or exhaustion can be inadequate in the reduction of presenteeism. It is important to focus on both factors simultaneously to reduce presenteeism [9] [21] [40]. The study also highlights the importance of the JD-R model as a framework of occupational stress for understanding the process of presenteeism.
The JD-R model suggests that job demands make people exhausted and burned out, and that it is important to gain resources in demanding jobs [17] [18]. The findings of this study confirm the relation between job demands and exhaustion, and contribute to the JD-R literature by applying presenteeism as a job performance variable. Although limited by the cross-sectional design, the current results are in concordance with the existing literature that suggests a reciprocal relationship between exhaustion and presenteeism [8] [9] [21]. However, there is a need for more longitudinal studies examining this specific causal relationship.
scope of correlates of presenteeism beyond the typical psychosocial and structural job demands in future re-search. The current results also show that exhaustion mediated the relationship between role conflict and pre-senteeism in that role conflict through high symptoms of exhaustion increased prepre-senteeism. Experiencing con-flicting demands can cause attendance pressures which in turn increase symptoms of exhaustion and presentee-ism.
Contrary to our hypothesis, the current study found no support for a relationship between job resources and presenteeism. In the literature, the effects of social support on presenteeism are contradictory [38] [41]-[43] and it remains unclear when and what aspects of presenteeism are affected by social support. However, the current study examined the health impairment process of the JD-R model, suggesting that a supportive work context would decrease presenteeism. It could be beneficial to examine a motivational path between job resources and presenteeism [11] as presenteeism has been associated with resources, work engagement, and work joy [52]. An increased understanding of the complexity of presenteeism, and the association between presenteeism and job resources, may be important for preventing long-term ill-health. Future studies should investigate if the motiva-tional path affects presenteeism and health in the long term.
4.1. Strengths and Limitations
In contrast to some studies on presenteeism the operational definition of the current study is specific and con-textual. The physicians were asked to consider themselves as patients and relate to situations and conditions where they would have recommended a patient to stay home. The measure of presenteeism used in this study was defined as a period of 12 months and may be prone to recall bias. Changing the time frame of the question by asking the participants to provide their responses according to the prevalence of presenteeism at the last 3, 6, 9 and 12 months can prevent recall bias. Some scholars emphasize the development of a more detailed and ob-jective measure of presenteeism in preference to a single item measure [9] [53] [54]. Firstly, as presenteeism is a subjective state that can be undetectable for others, studies of this phenomenon must rely on self-report, as only the individual knows if he or she attend work sickness present [30]. To prevent different definition of presentee-ism it is important to define the phenomenon to participants as in the current study. Secondly, a single-item question and self-reports are shown to be a valid measure of presenteeism [55] [56]. The study confirms similar results on prevalence of presenteeism among physicians, which indicates validity of the current results for the current population of physicians [6]-[8].
The strength of the current study is its high response rate. However, the study is cross-sectional. Longitudinal data including self-reports and objective register data are better suited to confirm causal relationships between the variables in the current model. This would also enable a model that can identify a possible reciprocal rela-tionship between exhaustion and presenteeism. In addition, the antecedents of presenteeism can be heterogene-ous across occupations and reduce the generalizability of the current findings. However, many work environ-ments are characterized by high and often conflicting demands, role conflicts, responsibilities, and workload. Although this study focuses on physicians in academic medicine, we believe that the findings are relevant for work environments and occupations that share the same characteristics of high demands and high presenteeism.
4.2. Practical Implications
5. Conclusion
A significant contribution of this study is its demonstration that the relationship between job demands and pre-senteeism is mediated by a health variable. The significance of relational demands highlights the importance of extending the scope of correlates of presenteeism beyond the typical job demands in future research. Job de-mands, exhaustion, and job resources explained 17% of the variance of presenteeism and supported the impor-tance of looking at work characteristics mediated through exhaustion. The current study tested these assump-tions in terms of the health impairment process. However, it is important to explore these relaassump-tionships through a motivational path that emphasizes that presenteeism can have positive antecedents and effects on health and well-being.
Acknowledgements
The authors are grateful to the physicians who participated in this study and to the HOUPE Study Research Group. They would also like to thank Professor Per Øystein Saksvik for his review of the manuscript and helpful suggestions.
References
[1] Arigoni, F., Bovier, P.A. and Sappino, A.P. (2010) Trend of Burnout among Swiss Doctors. Swiss Medical Weekly,
140, w13070. http://dx.doi.org/10.4414/smw.2010.13070
[2] Houkes, I., Winants, Y., Twellaar, M. and Verdonk, P. (2011) Development of Burnout Over Time and the Causal Or-der of the Three Dimensions of Burnout among Male and Female GPs. A Three-Wave Panel Study. BMC Public Health, 11, 13. http://dx.doi.org/10.1186/1471-2458-11-240
[3] Peterson, U., et al. (2008) Burnout and Physical and Mental Health among Swedish Healthcare Workers. Journal of Advanced Nursing, 62, 84-95. http://dx.doi.org/10.1111/j.1365-2648.2007.04580.x
[4] Prins, J.T., et al. (2010) Burnout and Engagement among Resident Doctors in the Netherlands: A National Study. Medical Education, 44, 236-247. http://dx.doi.org/10.1111/j.1365-2923.2009.03590.x
[5] McKevitt, C., Morgan, M., Dundas, R. and Holland, W.W. (1997) Sickness Absence and ‘Working through’ Illness: A Comparison of Two Professional Groups. Journal of Public Health Medicine, 19, 295-300.
http://dx.doi.org/10.1093/oxfordjournals.pubmed.a024633
[6] Rosvold, E.O. and Bjertness, E. (2001) Physicians Who Do Not Take Sick Leave: Hazardous Heroes? Scandinavian Journal of Public Health, 29, 71-75. http://dx.doi.org/10.1177/14034948010290010101
[7] Sendèn, M.G., Løvseth, L.T., Schenck-Gustafsson, K. and Fridner, A. (2013) What Makes Physicians Go to Work While Sick: A Comparative Study of Sickness Presenteeism in Four European Countries (HOUPE). Swiss Medical Weekly, 143, 1-6.
[8] Thun, S., Fridner, A., Minucci, D. and Løvseth, L.T. (2014) Sickness Present with Signs of Burnout: The Relationship between Burnout and Sickness Presenteeism among University Hospital Physicians in Four European Countries. Scan-dinavian Psychologist, 1, e5.http://psykologisk.no/sp/2014/11/e5/
[9] Demerouti, E., Le Blanc, P.M., Bakker, A.B., Schaufeli, W.B. and Hox, J. (2009) Present But Sick: A Three-Wave Study on Job Demands, Presenteeism and Burnout. Career Development International, 14, 50-68.
http://dx.doi.org/10.1108/13620430910933574
[10] Lu, L., Cooper, C.L. and Lin, H.Y. (2013) A Cross-Cultural Examination of Presenteeism and Supervisory Support. Career Development International, 18, 440-456. http://dx.doi.org/10.1108/CDI-03-2013-0031
[11] Miraglia, M. and Johns, G. (2015) Going to Work Ill: A Meta-Analysis of the Correlates of Presenteeism and a Dual- Path Model. Journal of Occupational Health Psychology, No Pagination Specified.
[12] Gustafsson, K. and Marklund, S. (2014) Associations between Health and Combinations of Sickness Presence and Ab-sence. Occupational Medicine, 64, 49-55. http://dx.doi.org/10.1093/occmed/kqt141
[13] Grinyer, A. and Singleton, V. (2000) Sickness Absence as Risk-Taking Behaviour: A Study of Organisational and Cultural Factors in the Public Sector. Health, Risk & Society, 2, 7-21. http://dx.doi.org/10.1080/136985700111413 [14] Fridner, A. (2004) Career Paths and Career Patterns among Physicians with a Ph.D. Ph.D. Thesis, Uppsala University,
Uppsala.
[15] Bakker, A.B. and Demerouti, E. (2014) Job Demands-Resources Theory. In: Chen, P.Y. and Cooper, C.L., Eds., Work and Wellbeing: A complete Reference Guide, John Wiley & Sons, New York, 1-28.
[16] Bakker, A.B., Demerouti, E. and Sanz-Vergel, A.I. (2014) Burnout and Work Engagement: The JD-R Approach. An-nual Review of Organizational Psychology and Organizational Behavior, 1, 389-411.
http://dx.doi.org/10.1146/annurev-orgpsych-031413-091235
[17] Demerouti, E., Bakker, A.B., Nachreiner, F. and Schaufeli, W.B. (2001) The Job Demands-Resources Model of Bur-nout. Journal of Applied Psychology, 86, 499-512. http://dx.doi.org/10.1037/0021-9010.86.3.499
[18] Demerouti, E., Bakker, A.B., de Jonge, J., Janssen, P.P.M. and Schaufeli, W.B. (2001) Burnout and Engagement at Work as a Function of Demands and Control. Scandinavian Journal of Work Environment & Health, 27, 279-286. http://dx.doi.org/10.5271/sjweh.615
[19] Bakker, A.B. and Demerouti, E. (2007) The Job Demands-Resources Model: State of the Art. Journal of Managerial Psychology, 22, 309-328. http://dx.doi.org/10.1108/02683940710733115
[20] Demerouti, E., Bakker, A.B., Vardakou, I. and Kantas, A. (2003) The Convergent Validity of Two Burnout Instru-ments. European Journal of Psychological Assessment, 19, 12-23.
http://dx.doi.org/10.1027//1015-5759.19.1.12
[21] De Vroome, E.M.M., Smulders, P.G.W. and Houtman, I.L.D. (2010) Longitudinal Study on the Determinants and Consequences of Presenteeism. Gedrag & Organisatie, 23, 194-212.
[22] Kalliath, T. and Morris, R. (2002) Job Satisfaction among Nurses: A Predictor of Burnout Levels. Journal of Nursing Administration, 32, 648-654. http://dx.doi.org/10.1097/00005110-200212000-00010
[23] Piko, B.F. (2006) Burnout, Role Conflict, Job Satisfaction and Psychosocial Health among Hungarian Health Care Staff: A Questionnaire Survey. International Journal of Nursing Studies, 43, 311-318.
http://dx.doi.org/10.1016/j.ijnurstu.2005.05.003
[24] Allen, T.D., Herst, D.E.L., Bruck, C.S. and Sutton, M. (2000) Consequences Associated with Work-to-Family Conflict: A Review and Agenda for Future Research. Journal of Occupational Health Psychology, 5, 278-308.
http://dx.doi.org/10.1037/1076-8998.5.2.278
[25] Kahn, R.L., Wolfe, D.M., Quinn, R.P., Snoek, J.D. and Rosenthal, R.A. (1964) Organizational Stress: Studies in Role Conflict and Ambiguity. John Wiley, Oxford.
[26] Van Steenbergen, E.F., Kluwer, E.S. and Karney, B.R. (2014) Work-Family Enrichment, Work-Family Conflict, and Marital Satisfaction: A Dyadic Analysis. Journal of Occupational Health Psychology, 19, 182-194.
http://dx.doi.org/10.1037/a0036011
[27] Carlson, D.S., Kacmar, K.M. and Williams, L.J. (2000) Construction and Initial Validation of a Multidimensional Measure of Work-Family Conflict. Journal of Vocational Behavior, 56, 249-276.
http://dx.doi.org/10.1006/jvbe.1999.1713
[28] Greenhaus, J.H. and Beutell, N.J. (1985) Sources of Conflict between Work and Family Roles. Academy of Manage-ment Review, 10, 76-88.
[29] Innstrand, S.T., Langballe, E.M., Espnes, G.A., Falkum, E. and Aasland, O.G. (2008) Positive and Negative Work- Family Interaction and Burnout: A Longitudinal Study of Reciprocal Relations. Work & Stress, 22, 1-15.
http://dx.doi.org/10.1080/02678370801975842
[30] Johns, G. (2011) Attendance Dynamics at Work: The Antecedents and Correlates of Presenteeism, Absenteeism, and Productivity Loss. Journal of Occupational Health Psychology, 16, 483-500. http://dx.doi.org/10.1037/a0025153 [31] Dallner, M., et al. (2000) Validation of the General Nordic Questionnaire (QPSNordic) for Psychological and Social
Factors at Work. NORD, Copenhagen
[32] Dellve, L., Hadzibajramovic, E. and Ahlborg Jr., G. (2011) Work Attendance among Healthcare Workers: Prevalence, Incentives, and Long-Term Consequences for Health and Performance. Journal of Advanced Nursing, 67, 1918-1929. http://dx.doi.org/10.1111/j.1365-2648.2011.05630.x
[33] Løvseth, L.T., Fridner, A., Jónsdóttir, L.S., Marini, M. and Linaker, O.M. (2013) Associations between Confidentiality Requirements, Support Seeking and Burnout among University Hospital Physicians in Norway, Sweden, Iceland and Italy (the HOUPE Study). Stress and Health, 29, 432-437. http://dx.doi.org/10.1002/smi.2479
[34] Meijman, T.F. and Mulder, G. (1998) Psychological Aspects of Workload. In: Drenth, P.J.D. and Thierry., H., Eds., Handbook of Work and Organizational Psychology, Hove, Psychology Press. 5-33.
[35] Lu, L., Peng, S.-Q., Lin, H.Y. and Cooper, C.L. (2014) Presenteeism and Health over Time among Chinese Employees: The moderating Role of Self-Efficacy. Work & Stress, 28, 165-178.
[36] Johns, G. (2010) Presenteeism in the Workplace: A Review and Research Agenda. Journal of Organizational Behavior,
31, 519-542. http://dx.doi.org/10.1002/job.630
[38] Caverley, N., Cunningham, B.J. and MacGregor, J.N. (2007) Sickness Presenteeism, Sickness Absenteeism, and Health Following Restructuring in a Public Service Organization. Journal of Management Studies, 44, 304-319. http://dx.doi.org/10.1111/j.1467-6486.2007.00690.x
[39] Wallace, J.E. and Lemaire, J. (2007) On Physician Well Being—You’ll Get by with a Little Help from Your Friends. Social Science & Medicine, 64, 2565-2577. http://dx.doi.org/10.1016/j.socscimed.2007.03.016
[40] Deery, S., Walsh, J. and Zatzick, C.D. (2014) A Moderated Mediation Analysis of Job Demands, Presenteeism, and Absenteeism. Journal of Occupational and Organizational Psychology, 87, 352-369.
http://dx.doi.org/10.1111/joop.12051
[41] Hansen, C.D. and Andersen, J.H. (2008) Going Ill to Work—What Personal Circumstances, Attitudes and Work-Re- lated Factors Are Associated with Sickness Presenteeism? Social Science & Medicine, 67, 956-964.
http://dx.doi.org/10.1016/j.socscimed.2008.05.022
[42] Johansson, G. and Lundberg, I. (2004) Adjustment Latitude and Attendance Requirements as Determinants of Sickness Absence or Attendance. Empirical Tests of the Illness Flexibility Model. Social Science & Medicine, 58, 1857-1868. http://dx.doi.org/10.1016/S0277-9536(03)00407-6
[43] Jourdain, G. and Vezina, M. (2014) How Psychological Stress in the Workplace Influences Presenteeism Propensity: A test of the Demand-Control-Support Model. European Journal of Work and Organizational Psychology, 23, 483-496. http://dx.doi.org/10.1080/1359432X.2012.754573
[44] Kivimäki, M., et al. (2005) Working While Ill as a Risk Factor for Serious Coronary Events: The Whitehall II study. American Journal of Public Health, 95, 98-102. http://dx.doi.org/10.2105/AJPH.2003.035873
[45] Lindström, K. (2000) User’s Guide for the QPS Nordic: General Nordic Questionnaire for Psychological and Social Factors at Work. Copenhagen
[46] Wannström, I., Peterson, U., Asberg, M., Nygren, A. and Gustavsson, P. (2009) Psychometric Properties of Scales in the General Nordic Questionnaire for Psychological and Social Factors at Work (QPS): Confirmatory Factor Analysis and Prediction of Certified Long-term Sickness Absence. Scandinavian Journal of Psychology, 50, 231-244.
http://dx.doi.org/10.1111/j.1467-9450.2008.00697.x
[47] Hellesøy, O.H. (1985) Work Environment Statfjord Field. Work Environment, Health and Safety on a North Sea Oil Platform. Universitetsforlaget, Bergen.
[48] Løvseth, L.T. (2011) The Subjective Burden of Confidentiality. Ph.D. Thesis, Faculty of Medicine, Department of Neuroscience, Norwegian University of Science and Technology, Trondheim.
[49] Hu, L. and Bentler, P.M. (1999) Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6, 1-55.
http://dx.doi.org/10.1080/10705519909540118
[50] Tabachnick, B.G. and Fidell, L.S. (2013) Using Multivariate Statistics. Pearson, Boston.
[51] Cortina, J.M. (1993) What Is Coefficient Alpha? An Examination of Theory and Applications. Journal of Applied Psychology, 78, 98-104. http://dx.doi.org/10.1037/0021-9010.78.1.98
[52] Johansen, V., Aronsson, G. and Marklund, S. (2014) Positive and Negative Reasons for Sickness Presenteeism in Norway and Sweden: A Cross-Sectional Survey. BMJ Open, 4, e004123.
http://dx.doi.org/10.1136/bmjopen-2013-004123
[53] Baker-McClearn, D., Greasley, K., Dale, J. and Griffith, F. (2010) Absence Management and Presenteeism: The Pres-sures on Employees to Attend Work and the Impact of Attendance on Performance. Human Resource Management Journal, 20, 311-328. http://dx.doi.org/10.1111/j.1748-8583.2009.00118.x
[54] Johns, G. (2012) Presenteeism: A Short History and a Cautionary Tale. In: Houdmont, J., Stavroula, L. and Sinclair, R.R., Eds., Contemporary Occupational Health Psychology: Global Perspectives on Research and Practice, John Wi-ley & Sons, Chichester, 204-220. http://dx.doi.org/10.1002/9781119942849.ch12
[55] DeSalvo, K.B., Bloser, N., Reynolds, K., He, J. and Muntner, P. (2006) Mortality Prediction with a Single General Self-Rated Health Question. Journal of General Internal Medicine, 21, 267-275.
http://dx.doi.org/10.1111/j.1525-1497.2005.00291.x
[56] Johns, G. and Miraglia, M. (2015) The Reliability, Validity, and Accuracy of Self-Reported Absenteeism from Work: A Meta-Analysis. Journal of Occupational Health Psychology, 20, 1-14. http://dx.doi.org/10.1037/a0037754