International Journal of Emerging Technology and Advanced Engineering
Website: www.ijetae.com (ISSN 2250-2459, ISO 9001:2008 Certified Journal, Volume 3, Issue 2, February 2013)
1
High Reliability and Informatics Tools: PKC Software in
Primary Care
Robert R. Weaver
11
University of Ontario Institute of Technology, Health Sciences, Oshawa, Canada
Abstract - Growing concern about patient safety and healthcare quality has led some to borrow principles of reliability from industries with exceptional records of safety and reliability. Enhancing the quality of clinical decisions is fundamental to quality improvement. This paper argues that commitment to reliability enables the effective deployment of informatics tools that are, in turn, essential for elevating the reliability and quality of clinical decisions. To illustrate, it describes the use of “knowledge coupling” decision support tools in an innovative family practice committed to high reliability. The tools thoroughly define patients’ complexity, couple this complexity with formal knowledge, and present a range of options available to guide decisions. This investigation shows how informatics tools embedded within a high reliability organization can enhance the reliability of the decision making process, and improve the quality of healthcare decisions.
Keywords-- Clinical decision support systems; high reliability organizations; informatics; primary health care; quality improvement
I. INTRODUCTION
At least since the Institute of Medicine sounded the alarm identifying significant variation in the quality of care delivered to patients, efforts have been made to bring changes to healthcare that advance the reliability with which it is practiced.1,2 In the current system there are few
mechanisms in place to ensure safety and reliability in decision making and care. The autonomous physician retains broad latitude in the exercise of judgment in managing patients, while conditions under which they exercise this judgment and make decisions have become increasingly challenging. Patients’ problems are more and more complex and variable than before, while the time available to manage them is more limited.3-7 Further, the
options for managing problems are numerous, changing, and difficult to keep up with. It is not surprising, therefore, that differences in local and regional practice conditions, idiosyncratic training and knowledge, evolving collective knowledge, clinical uncertainty, and broad clinical discretion would yield substantial practice variation.8-11
With a greater variety and complexity of patients and options available to manage them, and the underutilization of information tools, the quality of care too often suffers.2
Under these circumstances, it is no surprise that the outcomes of this process range from the very best to the very unsafe, while most fall everywhere in between.
Leaving the task of reliably applying current knowledge to increasingly complex patients within the confines of a fifteen minute office visit is a set-up for mediocrity in health care. Continuing this practice will only yield similar results. To address issues surrounding inconsistencies in quality, health care now looks to other industries that demonstrate high levels of safety and reliability – e.g., naval and commercial aviation, electric grid management, nuclear power.12-15 Five principles characterize high
reliability organizations16:
1. Preoccupation with failure: persistent wariness of
unexpected events to potentially preclude them from arising;
2. Reluctance to simplify: deliberate challenging of a
reductionist, incomplete, or stereotypic picture of the situation derived from received wisdom, past experience, or a limited initial assessment;
3. Sensitivity to operations: exchanging information to
obtain a broader picture of the current reality, irrespective of expectations or likelihoods;
4. Commitment to resilience: capacity to recover from
setbacks, learn from mistakes, adapt to new challenges, and improve effectiveness of actions;
5. Deference to expertise (not experts): willingness of
people and organizations to by-pass traditional status hierarchies and migrate decisions (often downward) to the person best able to make them.
Applying these principles in ambulatory settings presents additional challenges, as practitioners face the widest range of patient problems and, therefore, must draw upon the broadest scope of formal medical knowledge. Yet, it is in ambulatory settings where healthcare can do the most good for patients, where problems can be addressed at the earliest possible time, and where high quality decisions most greatly impact the health of individuals and the healthcare system at large.17,18 Nonetheless, cognitive
International Journal of Emerging Technology and Advanced Engineering
Website: www.ijetae.com (ISSN 2250-2459, ISO 9001:2008 Certified Journal, Volume 3, Issue 2, February 2013)
2
Combining patient complexity and the vast corpus of formal knowledge readily overwhelms the human mind. Computer tools are necessary to access and apply formal medical knowledge to patients’ complex problems, and to raise the reliability and quality of routine decisions.II. METHODS
This investigation uses a case study approach to examine the routine deployment of informatics tools in primary care.23 The study purposively selected an innovative family
practice (FP) that routinely uses informatics tools to support clinical decisions.24 Specificially, the FP is
distinctive among primary care practices in its embrace of the “knowledge coupling” approach to patient care and the PKC® informatics tools that embody it.25,26 This approach
uses computer tools to define the complexities of the patient’s condition and to “couple” the array of patient-specific findings with the diagnostic and management options available to address it. Further, the FP is atypical in its emphasis on high reliability, and its use of high reliability principles.15-16, 27 Thus, the FP combines a
commitment to reliability and the use of informatics decision aids to offer an important alternative to the conventional approaches to primary care likely to reproduce the quality and safety problems we aim to alleviate.
The analysis relies on observations made at the FP, informal discussions with clinical and office staff about the employment of PKC tools and the commitment to reliability, ongoing interactions with the physician who leads the practice, leadership statements expressed in practice documents, and an understanding of the philosophy and principles of the Knowledge Coupling approach. The investigation asks: How are PKC tools integrated into everyday practice? How does their deployment affect reliability? How compatible are reliability principles with the knowledge coupling approach and the tools that embody it?
III. RESULTS
High reliability is not a state an organization achieves, but an aspiration reinforced by leadership on an ongoing basis. Reliability principles permeate the FP’s leadership statements (e.g., its Mission and Vision, Principles of Practice document), its training and staff recruitment procedures, and the everyday awareness of staff and clinical practitioners.24 This commitment is key to fostering
a culture of safety and reliability in health care,28-31 and
central to integrating PKC tools into routine practice. For the FP the tools reinforce high reliability principles.
The practice divides clinical decision making process into two stages: (1) the knowledge coupling stage where collective knowledge is “coupled” with patient-specific findings to elicit a range of plausible guidance (diagnostic or management) options, and (2) the judgment stage where patient values, resources, and circumstances are taken into account to select which option is most suitable.
The knowledge coupling stage further divides into three
steps to enable consistent application of the most current and comprehensive knowledge.
Step 1. Choosing what data to collect from the patient
Normally, judgment regarding what patient data to collect remains with the practitioner. The flaws associated with this are well documented, highly problematic, and form the insecure basis upon which decisions usually are made.19-22 This task is removed from the clinical setting
entirely, and undertaken by builders, not users, of PKC tools (e.g., professionals, researchers, medical librarians).32
The a priori identification of data to collect from patients with a problem enables the development team to thoroughly review the literature and consult with experts to assess the utility of specific information, in combination with other information, for decision making. Decisions about what data to collect from patients who present a particular problem are embedded in the tools and automatically invoked each time a Coupler is run. In addition to the thoroughness this approach offers, it pre-empts problems associated with personal biases, memory lapses, or lack of time available to consider possibly relevant information to collect. When it comes to making choices regarding what data to collect, the problem of poor reliability and inconsistency, in effect, disappears when using the tool.
Step 2. Collecting data
International Journal of Emerging Technology and Advanced Engineering
Website: www.ijetae.com (ISSN 2250-2459, ISO 9001:2008 Certified Journal, Volume 3, Issue 2, February 2013)
3
By the time the patient even sees the primary provider an extensive patient history has been collected, laboratory results and vital data have been entered, and an initial database has been created. This enables primary care providers – the MDs or the Nurse Practitioner – to focus attention more directly on the patient’s problem. The provider reviews the data with the patient, and makes whatever corrections are required. Finally, the provider conducts the physical assessment as suggested by the Coupler. The broad-ranging patient-specific data collected presents a more complete and nuanced picture of the patient’s condition than otherwise would be available. PKC tools reinforce the “reluctance to simplify” that characterizes high reliability organizations.Step 3. Coupling patient-specific findings with formal medical knowledge
Once the initial database is compiled, the software couples the patient’s findings with the formal knowledge. Positive findings, in effect, “vote” for various guidance options presented. A diagnostic or management option is shown if one or more patient-specific findings lend support to it, irrespective of its prevalence or frequency of use. Probabilities can be considered later, as the results of the coupling process form the foundation for the decision made during stage two.
In stage two, the judgment stage, patients and providers assess the pros and cons of various diagnostic or management options and decide which seems most suitable. This is not automated. In cases where patient-specific findings and diagnostic or management options coalesce around a single option, the decision effectively makes itself. When the patient’s uniqueness is exposed, however, the match is often imperfect and two or more options may seem plausible. Patients and providers negotiate this ambiguity in deciding among options. Not all patients contribute equally in this process. Medicine’s cultural authority lead many to defer to the professional.33
Nonetheless, presenting the pros and cons of the various options enables a high level of patient involvement in considering their unique circumstances and values in clinical decisions, particularly when it comes to management decisions.
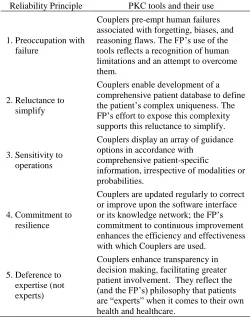
[image:3.612.318.568.172.489.2]Table I summarizes the compatibility between principles of high reliability organizations and the philosophy and application of PKC tools.
TABLE I
Compatibility Between Reliability Principles and the Philosophy and Application of PKC Tools
Reliability Principle PKC tools and their use
1.Preoccupation with
failure
Couplers pre-empt human failures associated with forgetting, biases, and reasoning flaws. The FP’s use of the tools reflects a recognition of human limitations and an attempt to overcome them.
2.Reluctance to
simplify
Couplers enable development of a comprehensive patient database to define the patient’s complex uniqueness. The FP’s effort to expose this complexity supports this reluctance to simplify.
3.Sensitivity to
operations
Couplers display an array of guidance options in accordance with
comprehensive patient-specific
information, irrespective of modalities or probabilities.
4.Commitment to
resilience
Couplers are updated regularly to correct or improve upon the software interface or its knowledge network; the FP’s commitment to continuous improvement enhances the efficiency and effectiveness with which Couplers are used.
5.Deference to
expertise (not experts)
Couplers enhance transparency in decision making, facilitating greater patient involvement. They reflect the (and the FP’s) philosophy that patients are “experts” when it comes to their own health and healthcare.
IV. DISCUSSION AND CONCLUSION
The FP’s commitment permeates the organization’s philosophy and practice principles, and is reinforced and encouraged in its everyday practice from the leadership on down.28-31 Various aspects of health care benefit from this
International Journal of Emerging Technology and Advanced Engineering
Website: www.ijetae.com (ISSN 2250-2459, ISO 9001:2008 Certified Journal, Volume 3, Issue 2, February 2013)
4
Further, Couplers help clinicians preempt problems associated with misspecifying events that otherwise result from complete dependence on personal judgment to manage patient complexity and uniqueness. Most important, the FP’s use of Couplers demonstrates how to structure the decision making process to form a sound, transparent basis upon which decisions can be made.This paper focuses on the process of decision making rather than its outcomes. It assumes that gaining a more complete and detailed picture of the patient’s current condition than is possible using the usual, discretionary approach generates a firmer foundation for decision making. It also assumes that the use of the tools complement rather than preclude the involvement of less tangible “intuitions” often seen as central to the “art” of medicine. Importantly, however, the more precise, complete, and explicit definition of the inputs to decision making the tools generate enables a more adequate assessment of the outcomes of decisions than is possible using the traditional approach. Irrespective of these outcomes, the transparency of the process permits continuous improvement of both human and information systems.
Using computer tools to achieve high reliability faces considerable challenges, however. Standards of performance in primary care remain ill-defined. The tolerance level for patient safety is socially constructed, and constrained by economic, regulatory, and legal conditions.8
While the political fallout of adverse events when they occur in the nuclear or aviation industries is broad and dramatic, this is less so in health care. When patients experience the effects of unsafe, unreliable, and mediocre or poor quality care, they usually do so privately, not publicly. And patients, vulnerable and disempowered to begin with, remain mainly a disparate collection of individuals, not an organized group with political clout.34
Public concern regarding the reliability and quality of decisions competes for attention with other values such as cost and access. While the realities of primary care might cry out for the adoption and use of decision support tools, these very realities leave little opportunity for individual practitioners struggling to manage an increasingly complex practice and clientele to even consider alternative practice designs that incorporate decision support tools. Under these conditions habitual modes of organizing and practicing in primary care easily become self-perpetuating.
Further, clinicians place paramount value on retaining clinical autonomy and authority, and the KC approach may be perceived as threatening to it.35-37 This might result from
misperceptions regarding what adopting this approach means with respect to clinical discretion.
To enhance reliability and to form a sound foundation for decision making, discretion during stage one is largely removed. As discussed, this is done to manage the overwhelming information processing task that practitioners face within the confines of a busy, fast-paced primary care context. The output of this stage, however, offers a broader range of options to consider than is available without using computer tools. When it matters most, the use of Couplers afford greater latitude in decision making than is available without them.
As the Institute of Medicine correctly points out, asking individuals to work harder or longer will do little to improve the quality of care. Quality is a property of a system so quality improvement requires change at the system level. Such change likely will come from health care leaders committed to enhancing reliability, safety, and quality. Increasingly these leaders look to learn from other industries adopting principles of high reliability. Weed’s longstanding vision for transforming health care is entirely compatible with these principles. The FP recognizes the central importance of reliability for health care safety and quality, and its achievements result from deliberately designing its operations to exploit the power of Couplers to define the complexity of each patient, to align this complexity with vast formal knowledge, and to integrate the tools into routine decision making. The FP’s commitment to reliability underlies the deployment of these tools, and demonstrates the feasibility of this vision and of high reliability in primary care. Leaders would do well to look to the FP as a concrete model for reform in health care.
ACKNOWLEDGMENTS
The author wishes to thank Dr. Charles Burger, Paula Eaton, and everyone in his practice for the insight and help provided in discussions of the work process at the patient-centred, high reliability family practice they all aim to produce. I also thank the Health Sciences Faculty at the University of Ontario Institute of Technology for its support for this research.
REFERENCES
[1] Kohn LT, Corrigan, JM, Donaldson MS. 1999. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press..
[2] Committee on Quality of Health Care in America. 2001. Crossing the Quality Chasm: A New Health System for the Twenty-First Century. Washington, DC: National Academy Press.
International Journal of Emerging Technology and Advanced Engineering
Website: www.ijetae.com (ISSN 2250-2459, ISO 9001:2008 Certified Journal, Volume 3, Issue 2, February 2013)
5
[4] Safford MM, Allison JJ, and Kiefe CI. 2007. Patient complexity: More than comorbidity. The vector model of complexity. Journal of General Internal Medicine. 22(3): 382-90.
[5] Peek C. 2009. Integrating care for persons, not only diseases. Journal of Clinical Psychology in Medical Settings 16(1): 13-20.
[6] Blaum CS, Cigolle CT, Boyd C, et al. 2010. Clinical complexity in middle-aged and older adults with diabetes: The health and rtirement study. Medical Care 48(4): 327-34.
[7] Abbo ED, Qi Z, Zelder M, and Huang ES. 2008. The increasing number of clinical items addressed during the time of adult primary care visits. Journal of General Internal Medicine 23(12): 2058-65. [8] Davis P, Gribben B, Scott A, Lay-Yee R. 2000. The “supply
hypothesis” and medical practice variation in primary care: testing economic and clinical models of inter-practitioner variation. Social Science & Medicine 50(3): 407-18.
[9] Wennberg JE. 1984. Dealing with practice variations: A proposal for action. Health Affairs 3(2): 6-32.
[10] Wennberg DE. and Wennberg JE. 2003. Addressing variations: Is there hope for the future? Health Affairs (Jul-Dec): 3-614-7. [11] Sirovich B, Gallagher PM, Wennberg DE, and Fisher ES. 2008.
Discretionary decision making by primary care physicians and the cost of U.S. health care. Health Affairs 27(3): 813-23.
[12] Schulman PR. 2004. General attributes of safe organisations. Quality and Safety in Health Care 13(suppl 2): ii39-ii44.
[13] Pronovost PJ, Berenholtz SM, Goeschel CA, et al. 2006. Creating high reliability in health care organizations. Health Services Research 41(4p2): 1599-1617.
[14] Nemeth C and Cook R. 2007. Reliability versus resilience: what does healthcare need? Human Factors and Ergonomics Society Annual Meeting Proceedings, Health Care 621-5.
[15] Sutcliffe, K.M., 2011. High reliability organizations (HROs). Best Practice & Research Clinical Anaesthesiology 25(2): 133-44. [16] Weick KE and Sutcliffe KM. 2007. Managing the Unexpected:
Resilient Performance in an Age of Uncertainty (Second Edition). San Francisco, CA: John Wiley & Sons, Inc,.
[17] Starfield B, Leiyu S, and Macinko J. 2005. Contribution of primary care to health systems and health. Milbank Quarterly 83(3): 457-502. [18] Friedberg MW, Hussey PS. and Schneider EC. 2010. Primary Care: A critical review of the evidence on quality and costs of health care. Health Affairs 29(5): 766-72.
[19] Tversky A. and Kahneman D. 1974. Judgment under uncertainty: heuristics and biases. Science 185: 1124-31.
[20] Elstein AS, Shulman LS, and. Spraska SA. 1978. Medical Problem Solving and Analysis of Clinical Reasoning. Cambridge, MA: Harvard University Press.
[21] Dawes R. 1988. Rational Choice in an Uncertain World. New York: Harcourt Brace Jovanovich.
[22] Groopman J. 2007. How Doctors Think. New York: Houghton Mifflin Company.
[23] Berg BL. 2007. Qualitative Research Methods for the Social Sciences, Sixth Edition. New York: Pearson.
[24] Burger C. 2010. The use of problem-knowledge couplers in a primary care practice. The Permanente Journal 14(1): 47-50. [25] Weed LL. 1991. Knowledge Coupling: New Premises And New
Tools For Medical Care And Education. New York: Springer-Verlag.
[26] Weed L. and Weed L. 2011. Medicine in Denial. Creative Commons Attribution 3.0 Unported License.
[27] Wilson KA, Burke CS, Priest HA, Salas E. 2005. Promoting health care safety through training high reliability teams. Quality and Safety in Health Care 14(4): 303-309.
[28] Reason J. 2000. Human error: models and management. BMJ 320(7237): 768-770.
[29] Khatri N, Brown GD, and Hicks LL. 2009. From a blame culture to a just culture in health care. Health Care Management Review 34(4): 312-322.
[30] Leape L, Berwick D, Clancy C, et al. 2009. Transforming healthcare: a safety imperative. Quality and Safety in Health Care 18(6): 424-8.
[31] Dugan DP, Mick SS, Scholle SH, Steidle EF, Goldberg DG. 2011. The relationship between organizational culture and practice systems in primary care. Journal of Ambulatory Care Management 34(1): 47-56.
[32] PKC Corporation. 2003. Construction and maintenance of
Problem-Knowledge Couplers®, http://www.pkc.com/papers/content.pdf.
PKC Corporation (first accessed February 2, 2009).
[33] Starr P. 1982. The Social Transformation of American Medicine: The Rise of a Sovereign Profession and the Making of a Vast Industry. New York: Basic Books, Inc.
[34] Venkatapuram, S., 2011. Health Justice: An Argument from the Capabilities Approach. Malden, MA: Polity Press.
[35] Weaver RR. 2002. Resistance to computer innovation: Knowledge Coupling in clinical practice. SIGCAS Comput. Soc 32(1): 16-21. [36] Carlson P. 2004. The European health divide: a matter of financial or
social capital? Social Science & Medicine 59(9): 1985- 92. [37] Weaver RR. 2010. A Knowledge Coupling approach to knowledge
translation: Implications for decision making and patient empowerment. The International Journal of Interdisciplinary Social Sciences 5(7): 73-83.
Address for Correspondence
Robert R. Weaver, Professor, Health Sciences, 2000 Simcoe Street N. , University of Ontario Institute of Technology, Oshawa,