Published online 2016 January 23. Research Article
Prevalence of Traumatic Dental Injuries to Anterior Teeth of 12-Year-Old
School Children in Kashmir, India
Tasneem S. Ain,
1,*Ravishankar Lingesha Telgi,
1Saima Sultan,
2Pradeep Tangade,
1Chaitra
Ravishankar Telgi,
2Amit Tirth,
1Sumit Kumar Pal,
1Owais Gowhar,
3and Vaibhav Tandon
11Department of Public Health Dentistry, Mahatma Jyotiba Phule Rohilkhand University, Bareilly, India 2Departments of Pedodontics, Mahatma Jyotiba Phule Rohilkhand University, Bareilly, India
3Departments of Oral and Maxillofacial Pathology, Mahatma Jyotiba Phule Rohilkhand University, Bareilly, India
*Corresponding author: Tasneem S. Ain, Department of Public Health Dentistry, Kothiwal Dental College & Research Centre, Moradabad, India; Department of Public Health Dentistry, Mahatma Jyotiba Phule Rohilkhand University, Bareilly, India. Tel: +91-8494044261, Fax: +59-12452996, E-mail: khantasneemdr@gmail.com
Received 2014 October 16; Revised 2015 May 26; Accepted 2015 September 12.
Abstract
Background: Traumatic dental injuries to anterior teeth are a significant public health problem, not only because their prevalence is relatively high, but also because they have considerable impact on children’s daily lives. Traumatic dental injuries (TDIs) cause physical and psychological discomfort, pain and other negative impacts, such as tendency to avoid laughing or smiling, which can affect social relationships.
Objectives: This study aimed to assess the prevalence of traumatic dental injuries to anterior teeth among 12-year-old school children in Kashmir, India.
Patients and Methods: A cross-sectional study was conducted in private and government schools of India among 1600 schoolchildren aged 12 years. In addition to recording of the type of trauma (using Ellis and Davey classification of fractures, 1970), over jet, Angle’s molar relation and lip competence were also recorded. The socioeconomic status and academic performance of the study subjects were registered. The data obtained were compiled systematically and then statistically analyzed. The statistical significance for the association between the traumatic injury and the variables was analyzed using the chi-square test. Logistic regression was used to identify potential risk predictors of TDIs.
Results: The overall prevalence of TDI to anterior teeth was found to be 9.3%. The TDI to anterior teeth in male was more than female, but the difference was statistically nonsignificant (P < 0.01). Falls and sports were the most common causes of trauma in the present study. The highest potential risk factor for the occurrence of trauma was over jet. Academic performance was found to be significantly associated to TDI to anterior teeth, when analyzed in a multiple regression model.
Conclusions: It was concluded that the prevalence of traumatic dental injuries was 9.3%. Traumatic dental injuries among children exhibit complex interaction between the victims’ oral conditions and their behavior. Therefore, prevention should consider a number of characteristics such as oral predisposing factors, environmental determinants and human behavior. It is recommended that specific and proper public places for leisure and sports activities, with impact-absorbing surfaces around the items on which children are most likely to fall, should be provided.
Keywords: Traumatic Dental Injuries, Schools, Risks
Copyright © 2016, Kashan University of Medical Sciences. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non-Commercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/) which permits copy and redistribute the material just in noncommercial usages, provided the original work is properly cited.
1. Background
Injuries during childhood have been considered a glob-al public heglob-alth problem and injuries have become the primary cause of death and disability of human beings (1). It has been estimated that in 2000, 12% of the burden of disease and 9% of deaths worldwide were due to inju-ries (2).
The prevalence of traumatic dental injuries (TDIs) to anterior teeth among schoolchildren has been studied in different parts of the world by many researchers, and a wide range of variation has been found. In Asia and Af-rica, the prevalence of TDI to anterior teeth among ado-lescents ranges from 4% to 35% and 15% to 21%, respectively.
learning in affected children (7). Hence, such a negative impact of TDI cannot be underestimated, and it becomes the role of health professionals to elucidate the causes and risk factors of TDI, so as to prevent its occurrence.
To allow or implement the application of adequate pre-ventive actions for traumatic injuries, the knowledge of its risk factors is of utmost importance (8). Prevention of traumatic dental injuries will be possible only if it is based on reliable data relating to its prevalence, causes and risk factors. However, it is unfortunate that people are not aware of the risk factors and the ways to avoid traumatic dental injuries. Also, some dentists and health professionals do not give much importance to the pre-vention of dental trauma and are more concerned about the treatment aspects (9).
In most of the previous studies, increased over jet, in-competent lip coverage and maxillary incisor protrusion have been reported to have an association with the occur-rence of traumatic dental injuries (8, 10). There are com-plex interactions of these oral risk factors with the envi-ronmental factors and individual behaviors. All these risk factors together highlight the complexity of the etiology of dental trauma.
In Kashmir, being a hilly area, there is an additional risk of traumatic dental injuries due to falls on uneven ter-rain. Moreover, the climatic conditions, such as snowfall, can increase the probability of trauma, as children may fall while walking or playing on the slippery roads and playgrounds. A review of the literature reveals that there are no previous studies conducted regarding traumatic dental injuries in Kashmir, India.
2. Objectives
Therefore, a cross-sectional study was conducted to esti-mate the prevalence of traumatic dental injuries to ante-rior teeth among 12-year-old schoolchildren in Kashmir, India.
3. Patients and Methods
A cross-sectional survey was carried out in private and public schools of Kashmir, India to assess the prevalence of traumatic dental injuries to anterior teeth among 12-year-old schoolchildren.
The sample size calculation was done on the basis of a prevalence of 50% in order to obtain the largest sample size (mentioned in Health Research Methodology, WHO; 2nd Edition, 2001), as there were no previous studies con-ducted in the state. At a confidence interval level of 95% and with an allowable error of 5%, the sample size was es-timated to be 1600.
A multistage sampling was adopted for selection of students so that they represented the population of 12-year-old schoolchildren of Kashmir, India. In the first stage, the Kashmir division was divided into four zones; Northeast, Northwest, Southeast and Southwest. From each zone, one district was selected in which two private
and two public schools were chosen randomly, using the criteria of a minimum number of 100 students of age 12 years old studying in each school. In the second stage, all 12-year-old children in these schools who fulfilled the eli-gibility criteria, were examined to make the final sample of 1600 subjects. All those students who were 12 years old, willing to participate and were permanent residents of Kashmir, India were included in the study. Students, who were mentally or physically disabled and those who were not present on the days of oral examinations were excluded from the study.
A single examiner was calibrated in the department of Public Health Dentistry, Kothiwal Dental College and Research Centre, Moradabad. Kappa statistics were ap-plied to compute the intra-examiner reliability and it was found to be satisfactory at a Kappa coefficient of 0.81.
Subjects were asked about their demographic data by the investigator, and the responses were recorded in a pre-structured proforma. To categorize the subjects based on their socioeconomic status, they were inter-viewed to determine the education and occupation of the family head, monthly family income and total num-ber of memnum-bers in their family. Their responses were cross-verified with school records. An updated Kuppas-wami’s Classification 2012 was used for determining the socioeconomic status. The student’s teacher was asked about the academic performance and as to how they rated the student’s performance in academics. The rat-ings were categorized on 5-point Likert scale as excellent, good, fair, poor or very poor. Students were examined by one calibrated examiner for traumatic dental injuries us-ing a mouth mirror and explorer. The Ellis and Davey clas-sification of fractures (1970) was used to assess the type of tooth fracture. Subjects who were found to have traumat-ic dental injury were interviewed for details of the injury event. Subjects were checked for overjet using the Com-munity Periodontal Index (CPI) probe, as mentioned in the 1997 WHO basic oral health survey guidelines. Lip seal was examined by visual inspection to categorize children as having competent or incompetent lips. Angle’s molar relationship was recorded to classify the subjects as hav-ing Class I, Class II and Class III molar relation.
Data analysis included descriptive statistics (frequency distribution). The statistical significance for the asso-ciation between the traumatic injury and gender, socio-economic status, academic performance, malocclusion, overjet and lip competence was obtained using the Chi-Square test. The level of significance was set at P ≤ 0.05. Logistic regression was used to identify potential risk predictors of traumatic dental injuries at a level of sig-nificance of P < 0.15.
3.1. Ethical Consideration
Permis-sion for carrying out the study in the public and private schools of Kashmir was obtained from the Directorate of School Education, Kashmir.
4. Results
Out of total 1600 students, 767 (47.9%) were male and 833 (52.1%) were female. The prevalence of TDI was found to be 9.3% (5.06% male and 4.25% female). It was slightly higher in male than female, but the difference was found to be statistically non-significant (P < 0.10). The most common cause of trauma was falls (42.2%) followed by sport injuries (22.81%) (Table 1). Type I (68.45%) fracture was the most common type of tooth fracture found
(Ta-ble 2) and among all anterior teeth, the most commonly involved teeth were right maxillary central incisors (Ta-ble 3). Among those children with > 3 mm over jet, 17.1% were affected by trauma, while 3.6% of children with ≤ 3 mm overjet showed TDI to anterior teeth (Table 4).
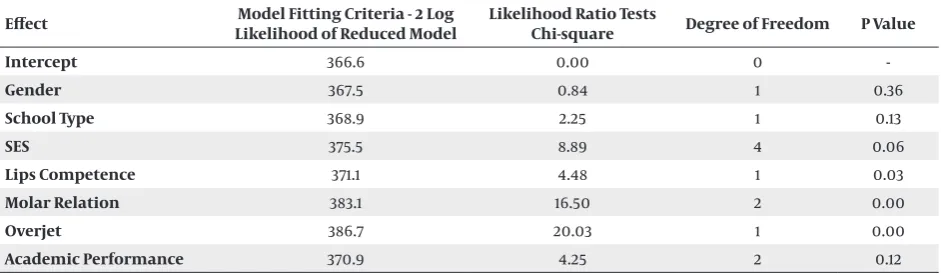
In multiple logistic regression analysis, it was observed that the highest potential risk factor for occurrence of TDI, was overjet followed by molar relation and lip in-competence. These three variables showed a highly signif-icant association to TDI. Academic performance and so-cioeconomic status also showed a statistically significant association to traumatic dental injuries when analyzed in the multiple logistic regression model (Table 5).
Table 1. Distribution of Traumatized Subjects According to Causea
Serial No. Cause of Trauma Percentage of Children
1 Falls 63 (42.2)
2 Sports 34 (22.81)
3 Unknown 24 (16)
4 Accidents 15 (10.06)
5 Collisions 7 (4.69)
6 Violence 3 (2.01)
7 Biting 3 (2.01)
aData are represent as No. (%).
Table 2. Traumatic Dental Injuries According to Type of Traumaa
Serial No. Type (Ellis and Davey classification of fractures) Affected Children
1 Type I 102 (68.45)
2 Type II 37 (24.8)
3 Type III 7 (4.6)
4 Type IV 1 (0.67)
5 Type V 1 (0.67)
6 Type VIII 1 (0.67)
aData are represent as No. (%).
Table 3. Traumatic Dental Injuries According to Tooth/Teeth Fractureda
Tooth/Teeth Fractured Involved Students
Right Maxillary Central Incisors 91 (61.07)
Right and Left Maxillary Central Incisors 15 (10.06)
Left Maxillary Central Incisors 40 (26.84)
Left Maxillary and Mandibular Central Incisors 1 (0.67)
Left Mandibular Central Incisors 1 (0.67)
Right and Left Mandibular Central Incisors 1 (0.67)
Table 4. Traumatic Dental Injuries According to Overjet, Lip Coverage, Molar Relation, Socio-Economic Status and School Typea,b
Risk Factor Examined Affected by Fracture P
Overjet, mm 0.001
Less than 3 mm 921 (57.6) 33 (3.6) ≥ 3 mm 679 (42.4) 116 (17.1)
Lip coverage 0.001
Competent 1301 (81.3) 71 (5.45) Incompetent 299 (18.7) 78 (26.08)
Molar relation 0.001
Class I 1262 (78.5) 69 (5.46) Class II 306 (19.1) 80 (26.14)
Class III 3 (2) 0 (0)
Socioeconomic status ≤ 0.024
Upper (I) 342 (21.5) 35 (10.2) Upper Middle (II) 476 (29.8) 28 (5.9) Middle Lower (III) 236 (14.8) 25 (10.6) Lower Upper Lower (IV) 350 (21.9) 35 (10.2) Lower (V) 196 (12.2) 26 (13.3)
School type ≤ 0.82
Public 844 (52.8) 80 (9.5) Private 756 (47.2) 69 (9.1)
aData are represent as No (%). bLevel of significance at P ≤ 0.05.
Table 5. Regression Analysis of Different Variables in Relation to Traumatic Dental Injuries to Anterior Teetha
Effect Likelihood of Reduced ModelModel Fitting Criteria - 2 Log Likelihood Ratio Tests Chi-square Degree of Freedom P Value
Intercept 366.6 0.00 0
-Gender 367.5 0.84 1 0.36
School Type 368.9 2.25 1 0.13
SES 375.5 8.89 4 0.06
Lips Competence 371.1 4.48 1 0.03
Molar Relation 383.1 16.50 2 0.00
Overjet 386.7 20.03 1 0.00
Academic Performance 370.9 4.25 2 0.12
aLevel of significance at P < 0.15.
5. Discussion
Out of a total of 1600 school children of 12 years of age examined in Kashmir, India, 149 (9.3%) subjects had trau-matic dental injuries to anterior teeth. A review of the literature has shown that there is a wide variation in TDI to anterior teeth among children in Africa, Asia, Europe, the Middle East and America; ranging from 4% to 58% (11). This variation in the prevalence of TDI has been related to many factors such as the study design, sample size, sam-pling procedure, diagnostic criteria, limited age-groups, geographic differences and study locations (8).
dif-ference found in TDI among girls and boys; this finding was similar to other previous studies (13, 14), which might be due to societal changes, including an increase in the participation of girls in sports, which can lead to trauma.
In the present study, children attending the public schools had more TDI to anterior teeth than those at-tending the private schools, but the difference was not found to be statistically significant (P ≤ 0.82). More TDIs were reported in public schools than the private schools in several previous studies (15, 16). This might be due to the better facilities and more favorable socio-environ-mental conditions (especially for sports) at the private schools (17). Public schools probably have more children per classroom, resulting in overcrowding, and hence, a predisposition to TDIs. Moreover, the children studying in public schools are usually from poor families, so they lack appropriate supervision, which might be a risk fac-tor for their TDIs. On the contrary, more traumatic dental injuries were seen in children attending private schools in the study conducted in San Domingo, Dominican Re-public (18). This might be due to the fact that the students in private schools that were studied had more facilities, such as swimming pools, skates and skids, and different types of contact sports, and thus, they were more prone to traumatic dental injuries.
In the present study, the socioeconomic stratification was done based on Kuppuswamy’s Socio-Economic Sta-tus Scale (revised in 2012). The socioeconomic staSta-tus gives an idea of whether health services and facilities can be af-forded or not. As Kuppuswamy’s socioeconomic status is calculated by a summation of education, occupation and income, the value system for a particular level of educa-tion and occupaeduca-tion can be predicted. It is an important tool in hospital and population-based research in India, which was first proposed in 1971 (19). An updated version of the Kuppuswamy Scale was used because of the in-crease in the price index (this scale being consumer price index based) (20).
In the present study, the highest prevalence (13.3%) of traumatic dental injuries to anterior teeth was found in the children from the lowest socioeconomic status families. This finding was in agreement with some of the previous studies in which it was reported that lower socioeconomic groups were more prone to TDIs (15, 21), while few studies reported a higher prevalence of TDI among the highest socioeconomic groups (22, 23). One of the studies found a higher TDI prevalence in the middle class group (24). As the same socioeconomic pattern is not shared by different countries, this might explain the reason for the conflicting figures found by different researchers. Moreover, very few studies have included so-cioeconomic status in their reports.
In the present study, the most common cause of trauma was due to falls, followed by sports. This finding was in ac-cordance with many previous studies, wherein they have mentioned that this is of special importance for health policy makers seeking to establish prevention strategies
to reduce traumatic or facial injuries (25, 26). The main activities that caused children to fall were playing, cy-cling, running and other leisure activities at home and at schools. As the present study was conducted in Kashmir, in which the snow-covered roads and playgrounds in-crease the chances for children to fall; hence, that might be the reason for falls being one of the most common cause for TDI. Moreover, the uneven terrain increases the likelihood of trauma among school children of Kashmir, it being a hilly area. The third most important cause was of unknown origin. The likely cause for this could be that the present study was retrospective in nature and several children could not recall the origin of their trauma. It might also be explained by the fact that as the trauma was not so severe, enamel fractures being more prevalent, it was possible that some children did not remember the circumstances of the traumatic event when they were in-terviewed. This finding was in accordance with the ous studies (26, 27). Contrary to this, in some of the previ-ous studies (28), violence has been attributed to being the most common cause of dental trauma. This might be due to the fact that falls is a broad category and includes sev-eral causes such as falls due to pushing, which is a minor form of violence. So, in the present study this might be ex-plained by the fact that minor forms of violence were not specified by the students, and hence, might have been categorized as falls.
The Ellis classification of fractures of anterior teeth has been used in many previous studies (29, 30) for record-ing dental trauma. Use of a simple classification, e.g., Ellis and Davey classification of fractures (1970) (31), was preferred over other classifications, as injuries to the al-veolar socket and fractures of jaws or gingival lacerations were not evaluated in the present study. Using this clas-sification was easy and allowed the rapid recording of reliable data.
cases. Protrusion of maxillary anterior teeth is the most common feature in Class II Div1 malocclusion, so they are more vulnerable to traumatic dental injuries. These find-ings corroborate with earlier findfind-ings (10, 13).
In the present study, a higher prevalence of TDI was found in those children having an incisal overjet ≥ 3 mm (P < 0.01) and those with incompetent lip closure (P < 0.001), and the differences were found to be statistically significant. These findings corroborated with the findings of various previous studies (10, 12). In some studies (10), the overjet > 3–3.5 mm is believed to be the meaning of protru-sion, but in others (12), it is considered when the overjet > 5.0 mm, Such differences in the explanation of overjet makes it difficult to compare the results of various stud-ies. The results of the present study support previous find-ings in which it has been found that lip incompetence de-creases the incisor protection, and thus, leaves the incisors more vulnerable to trauma (27). Children with inadequate lip coverage were found to be more prone to TDI to ante-rior teeth. This finding was in agreement with many previ-ous studies (12, 13, 27, 34). Competent lips provide a cush-ion and protective effect, and hence, lip incompetence increases the likelihood of trauma (27).
The present study included the student’s academic performance as per their class teacher. It was found that those students, who were rated as excellent for their aca-demics by their teachers, experienced the least traumatic dental injuries, while those who were fair in their studies accounted for a greater number of traumatic dental inju-ries. In multiple logistic regression analysis, the academ-ic performance of the children showed a signifacadem-icant asso-ciation with traumatic dental injuries to anterior teeth.
Various researchers have found that the academic per-formance of the students is influenced by many factors such as their socioeconomic status, aggressive behavior, the environment of classrooms, the physical activity of child and so on (35). Warren et al. believed that social scenarios are responsible for the deviation of students towards using aggressive behavior. They indicated that if an individual utilizes their aggression in a constructive direction, then the negative impact of aggression, which includes physical acts of violence that lead to harming or injuring other person, may not be a cause of the harm (35). Loveland et al. found that higher levels of aggression may have a negative impact on academic performance as the students may remain absent, being unable to deal with the stressors of school life (36). Injuries, especially dental injuries, have been associated with behavioral and emotional risk factors (37).
According to DeGarmo e t al., children’s academic per-formance improves with good parenting, which has been in turn associated with socioeconomic status (37). Unfortunately, the converse is also true; children’s school performance is hampered by negative parenting, which is related to the persistent stress of poverty. Parents who are struggling just to stay afloat tend to work extra hours, odd shifts, or multiple jobs, and hence, are not able to
provide proper supervision for their children as they are short of time and energy. These deficits have been linked with higher levels of externalizing behaviors and poor academic achievement by such children (38). Socioeco-nomic status and aggressive behavior has been corre-lated with academic performance. As the occurrence of traumatic dental injuries has been found to have an as-sociation with socioeconomic status and behavior, it can be assumed that academic performance and TDI are cor-related to each other, as well.
The reviewed studies showed associations between den-tal problems of children and their school performance (3, 35). According to Pourat et al., students who are unable to attend school due to dental problems miss the pros-pect of learning, which impairs their academic perfor-mance (7). A study conducted in Kerala, India, showed a considerable correlation between TDI and whether or not the good marks achieved by students in school were important. Children, who considered that good marks at school were not important, experienced twice the risk of TDIs when compared to those children for whom achiev-ing good marks was important (39).
Traumatic dental injuries among children exhibit a complex interaction between the victim’s oral conditions and their behavior. Therefore, prevention should consid-er a numbconsid-er of charactconsid-eristics such as oral predisposing factors, environmental determinants and human behav-ior. It is recommended that specific and proper public places for leisure and sports activities, with impact-ab-sorbing surfaces around the items on which children are most likely to fall, should be provided. Moreover, proper monitoring and supervision by the parents and teachers is necessary to avoid TDIs among children.
The prevalence of TDI can be reduced if the potential risk factors are identified in time and strategies are di-rected at behavioral, environmental and societal changes and implemented by the health policy makers.
5.1. Sample Size Estimation
The sample size was calculated using the following for-mula:
(1)
n
=
(
pqE1.96
)
2where, n = minimum sample size; p = maximum expect-ed prevalence; q = 1 - p; E = Margin of sampling error toler-ated (allowable error);
For this survey:
(2)
n
=
4
×
0.52.5×0.52=
1600
Footnotes
Authors’ Contribution:Tasneem S. Ain, Ravishankar Lingesha Telgi and Saima Sultan have done the data col-lection in schools, created the study concept, and the 1st draft of the paper. Pradeep Tangade, Chaitra Ravishankar Telgi, Amit Tirth designed the study and contributed in preparation of recording the proforma. Sumit Kumar Pal, Owais Gowhar contributed to the final draft of the paper after critical evaluation. Vaibhav Tandon contributed in analyzing the data.
Financial Disclosure:There are no financial interests related to the material in the manuscript.
Funding/Support:There was no financial and material support taken for this research work.
References
1. Mock C, editor. Guidelines for essential trauma care. World Health Organization; 2004.
2. World Health Organization. Injuries, and Violence Prevention Dept. The injury chart book: A graphical overview of the global burden of injuries. World Health Organization; 2002.
3. Gupta S, Kumar-Jindal S, Bansal M, Singla A. Prevalence of trau-matic dental injuries and role of incisal overjet and inadequate lip coverage as risk factors among 4-15 years old government school children in Baddi-Barotiwala Area, Himachal Pradesh, India. Med Oral Patol Oral Cir Bucal. 2011;16(7):e960–5. [PubMed: 21743405]
4. Cortes MI, Marcenes W, Sheiham A. Impact of traumatic inju-ries to the permanent teeth on the oral health-related quality of life in 12-14-year-old children. Community Dent Oral Epidemi.
2002;30(3):193–8. [PubMed: 12000342]
5. Andreasen JO, Andreasen FM. Textbook and color atlas of trau-matic injuries to the teeth. Copenhagen: Munksgaard. 1993:216–56. 6. Marcenes W, Alessi ON, Traebert J. Causes and prevalence of trau-matic injuries to the permanent incisors of school children aged 12 years in Jaragua do Sul, Brazil. Int Dent J. 2000;50(2):87–92. [PubMed: 10945187]
7. Pourat N, Nicholson G. Unaffordable dental care is linked to fre-quent school absences. UCLA Cen H Pol Rese. 2009.
8. Traebert J, Almeida IC, Marcenes W. Etiology of traumatic den-tal injuries in 11 to 13-year-old schoolchildren. Oral H Prev Dent.
2003;1(4):317–23. [PubMed: 15643760]
9. Carvalho Rocha MJ, Cardoso M. Traumatized permanent teeth in Brazilian children assisted at the Federal University of Santa Catarina, Brazil. Dent Traumatol. 2001;17(6):245–9. doi: 10.1034/j.1600-9657.2001.170601.x. [PubMed: 11766090]
10. Patel MC, Sujan SG. The prevalence of traumatic dental injuries to permanent anterior teeth and its relation with predisposing risk factors among 8-13 years school children of Vadodara city: An epi-demiological study. J Indian Soc Pedod Prev Dent. 2012;30(2):151–7. doi: 10.4103/0970-4388.99992. [PubMed: 22918101]
11. Glendor U. Epidemiology of traumatic dental injuries-a 12 year review of the literature. Dent Traumatol. 2008;24(6):603–11. doi: 10.1111/j.1600-9657.2008.00696.x. [PubMed: 19021651]
12. Ravishankar TL, Kumar MA, Ramesh N, Chaitra TR. Prevalence of traumatic dental injuries to permanent incisors among 12-year-old school children in Davangere, South India. Chin J Dent Res.
2010;13(1):57–60. [PubMed: 20936193]
13. Kumar A, Bansal V, Veeresha KL, Sogi GM. Prevalence of traumatic dental injuries among 12- to 15-year-old schoolchildren in amba-la district, Haryana, India. Oral Health Prev Dent. 2011;9(3):301–5. [PubMed: 22068187]
14. Adekoya-Sofowora CA, Adesina OA, Nasir WO, Oginni AO, Ugboko VI. Prevalence and causes of fractured permanent incisors in 12-year-old suburban Nigerian schoolchildren. Dent Traumatol.
2009;25(3):314–7. doi: 10.1111/j.1600-9657.2008.00704.x. [PubMed: 19302204]
15. Soriano EP, Caldas AF, Goes PS. Risk factors related to trau-matic dental injuries in Brazilian schoolchildren. Dent Trauma-tol. 2004;20(5):246–50. doi: 10.1111/j.1600-9657.2004.00246.x. [PubMed: 15355382]
16. Soriano EP, Caldas AF, Carvalho MVDD, Amorim Filho Hde A. Prevalence and risk factors related to traumatic dental injuries in Brazilian schoolchildren. Dent Traumatol. 2007;23(4):232–40. doi: 10.1111/j.1600-9657.2005.00426.x. [PubMed: 17635357] 17. Carvalho ML, Moyses SJ, Bueno RE, Shimakura S, Moyses ST. A
geographical population analysis of dental trauma in school-Children aged 12 and 15 in the city of Curitiba-Brazil. BMC Health Serv Res. 2010;10:203. doi: 10.1186/1472-6963-10-203. [PubMed: 20624321]
18. Garcia Godoy FM. Prevalence and distribution of traumatic in-juries to the permanent teeth of dominican children from pri-vate schools. Community Dent Oral Epidemiol. 1984;12(2):136–9. [PubMed: 6584264]
19. Kuppuswamy B. Socio-economic status scale. New Delhi: Mana-sayan. 1962;40.
20. Kumar BPR, Dudala SR, Rao AR. Kuppuswamy’s socio-economic status scale–a revision of economic parameter for 2012. Int J Res Dev Health. 2013;1(1):2–4.
21. Malikaew P, Watt RG, Sheiham A. Prevalence and factors associ-ated with traumatic dental injuries (TDI) to anterior teeth of 11-13 year old Thai children. Community Dent Health. 2006;23(4):222–7. [PubMed: 17194069]
22. Bendo CB, Scarpelli AC, Vale MP, Araujo Zarzar PM. Correla-tion between socioeconomic indicators and traumatic dental injuries: A qualitative critical literature review. Dent Trauma-tol. 2009;25(4):420–5. doi: 10.1111/j.1600-9657.2009.00803.x. [PubMed: 19519857]
23. Grimm S, Frazao P, Antunes JL, Castellanos RA, Narvai PC. Den-tal injury among Brazilian schoolchildren in the state of Sao Paulo. Dent Traumatol. 2004;20(3):134–8. doi: 10.1111/j.1600-4469.2004.00238.x. [PubMed: 15144443]
24. Fakhruddin KS, Lawrence HP, Kenny DJ, Locker D. Etiology and en-vironment of dental injuries in 12- to 14-year-old Ontario school-children. Dent Traumatol. 2008;24(3):305–8. doi: 10.1111/j.1600-9657.2007.00548.x. [PubMed: 18410389]
25. Franca Caldas A, Burgos MEA. A retrospective study of traumatic dental injuries in a Brazilian dental trauma clinic. Dental Trauma-tology. 2001;17(6):250–3. doi: 10.1034/j.1600-9657.2001.170602.x. [PubMed: 11766091]
26. Chopra A, Lakhanpal M, Rao N, Gupta N, Vashisth S. Traumatic dental injuries among 12-15-year-old-school children in panch-kula. Arch Trauma Res. 2014;3(1):e18127. doi: 10.5812/atr.18127. [PubMed: 25032172]
27. Govindarajan M, Reddy VN, Ramalingam K, Durai KS, Rao PA, Prabhu A. Prevalence of traumatic dental injuries to the ante-rior teeth among three to thirteen-year-old school children of Tamilnadu. Contemp Clin Dent. 2012;3(2):164–7. doi: 10.4103/0976-237X.96819. [PubMed: 22919215]
28. Marcenes W, al Beiruti N, Tayfour D, Issa S. Epidemiology of trau-matic injuries to the permanent incisors of 9-12-year-old school-children in damascus, Syria. Endod Dent Traumatol. 1999;15(3):117– 23. [PubMed: 10530154]
29. Tangade PS. The prevalence of anterior teeth fracture and its re-lation to malocclusion in 12 and 15 year old school children Bel-gaum City, India. J Oral Health Commun Dent. 2007;1:7–11. 30. Kaur A, Mohindroo A, Thakur G, Ahlawat B. Anterior tooth
trau-ma: A most neglected oral health aspect in adolescents. Ind J Oral Sci. 2013;4(1):31. doi: 10.4103/0976-6944.118532.
31. Young EP, Ellis RB, Lake BD, Patrick AD. Tay-sachs disease and related disorders: Fractionation of brain N-acetyl-beta-hexos-aminidase on DEAE-cellulose. FEBS Lett. 1970;9(1):1–4. [PubMed: 11947613]
32. Nik Hussein NN. Traumatic injuries to anterior teeth among schoolchildren in Malaysia. Dent Traumatol. 2001;17(4):149–52. [PubMed: 11585139]
S0103-64402010000200011. [PubMed: 11585139]
34. Singh G, Garg S, Damle SG, Dhindsa A, Kaur A, Singla S. A study of sports related occurrence of traumatic orodental injuries and associated risk factors in high school students in north In-dia. Asian J Sports Med. 2014;5(3):e22766. doi: 10.5812/asjsm.22766. [PubMed: 25520762]
35. Warren P, Richardson DS, McQuillin S. Distinguishing among nondirect forms of aggression. Aggress Behav. 2011;37(4):291–301. doi: 10.1002/ab.20394. [PubMed: 21480293]
36. Loveland JM, Lounsbury JW, Welsh D, Buboltz WC. The valid-ity of physical aggression in predicting adolescent academ-ic performance. Br J Educ Psychol. 2007;77(Pt 1):167–76. doi: 10.1348/000709905X79563. [PubMed: 17411493]
37. Degarmo DS, Forgatch MS, Martinez JCR. Parenting of divorced mothers as a link between social status and boys' academic out-comes: Unpacking the effects of socioeconomic status. Child Dev.
1999;70(5):1231–45. doi: 10.1111/1467-8624.00089. [PubMed: 10546342] 38. Hsueh J, Yoshikawa H. Working nonstandard schedules and
variable shifts in low-income families: Associations with pa-rental psychological well-being, Family functioning, and child well-being. Dev Psychol. 2007;43(3):620–32. doi: 10.1037/0012-1649.43.3.620. [PubMed: 17484575]
![DESIGN, SYNTHESIS, MOLECULAR DOCKING AND EVALUATION OF ANTIMICROBIAL ACTIVITY OF 4 AMINO N [(4 OXO 2 (PHENYLAMINO) 4H CHROMEN 3 YL) METHY LENE]BENZENESULFONAMIDE AND THEIR DERIVATIVES](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)