R E S E A R C H
Open Access
Outcome assessment of a triangular clinic as a
harm reduction intervention in Rajaee-Shahr
Prison, Iran
Rahim Taghizadeh Asl
1†, Babak Eshrati
2, Colleen Anne Dell
3*†, Kelli Taylor
4†, Parviz Afshar
5,
Mohammad Kamali
6and Ali Mirzazadeh
7Abstract
Background:Transmission of the human immunodeficiency virus (HIV) among incarcerated injection drug users (IDU) is a health epidemic in the Islamic Republic of Iran. Triangular clinics (TCs) were established in prisons as a harm reduction measure to decrease the risk of HIV transmission and other blood-borne infections. The objective of this study was to assess the immediate outcomes of one TC among male IDUs in Iran’s Rajaee-Shahr prison. Methods:This study was conducted in two stages between 2003 and 2005. In the preparatory stage, focus group data was collected to update the prison’s TC education and medical interventions and construct the self-report questionnaire. In stage two, 150 male IDUs were recruited in a closed cohort study design to assess the immediate outcome of the TC. Participants were measured at baseline and followed up to six months to measure their drug use, attitude toward and knowledge of high risk behaviours, serological conversion for HIV, HBV and HCV, and engagement in risky behaviors. The TC outcomes were determined through random urine analysis testing, a self-administered questionnaire and behaviour report cards, and viral infection testing.
Results:The findings of the urine analyses indicated a minimal yet consistent decrease in drug use over the six months. The pre and post- self-administered questionnaire data relayed a modest change in IDU risky behaviours associated with sexual practices; this was greater in comparison to the knowledge and attitude measures. It was determined that age may have a detrimental effect as may viral infections (HIV and HBV) on knowledge, attitude and behavior change. Both education and employment may have a protective effect. Data collected from the self-report behaviour cards similarly showed a modest reduction in high risk practices. At the six month follow-up, only one case became HIV positive, 9 HCV and 17 HBV.
Conclusions:Considering that HIV is concentrated among Iranian prisoners who inject drugs at a high level, the results of this study indicate that TCs are a possible effective intervention. However, many prisoners continued with risky behaviors even if they were participating in harm reduction measures, such as methadone maintenance therapy.
Keywords:Triangular clinic, Injection drug use, HIV/AIDS, Health belief model
* Correspondence:[email protected] †Equal contributors
3
Department of Sociology & School of Public Health, University of Saskatchewan, Saskatoon, Saskatchewan, Canada
Full list of author information is available at the end of the article
Background
To address the IDU and HIV epidemic we need “to break the silence and change attitudes of prisoners and policy makers and [have] collaboration all around”.
-Dr. Afshar, Director General of Health Services for the Iranian Prison Organization at the 2004 International AIDS Conference.
With a population of over 75 million people in Iran, the number of individuals abusing drugs is estimated to be over one million, with approximately 200,000 to 300,000 injection drug users (IDU) [1,2]. At present, the human immunodeficiency virus (HIV) is highly concen-trated among IDUs [3]. Over the past several years there has been an increase in HIV cases originating from sexual transmission in the general population [3], however, the large majority of new cases (65-79%) remain among IDU’s sharing needles [3-5]. With a growing proportion of young people making up the Iranian population and an increase in the availability of drugs, including a mounting relation-ship between amphetamine-type stimulant use and high risk sexual practices, the country is vulnerable to an in-crease in the number of new drug users, including those engaged in injecting and other high risk behaviours [5]. In turn, there is potential for a dramatic increase in the prevalence of HIV, as well as the hepatitis B virus (HBV) and hepatitis C virus (HCV) [6]. The most recent (2012) United Nations AIDS progress report by the Islamic Republic of Iran acknowledged that if the current HIV epidemic among IDUs is left unattended, it has the poten-tial to turn into a generalized population epidemic [3].
Acknowledging the direct linkage between IDU and the spread of HIV, Iran committed to attempts to con-trol the spread of the disease at the 2003, 2008 and 2011 United Nations General Assembly Special Sessions on HIV/AIDS. The latest data relay that “[m]easures taken over the past ten years have successfully slowed the pro-gression of the epidemic among injection drug users”, but the HIV rate among IDUs remains at around 15% and varies across the country [3]. A surveillance survey in 2010 in Iran further revealed that“among those who had injected drugs over the last month, 36.9% had used a non-sterile needle, and 12.6% had practiced shared injection” [7]. Controlling the spread of HIV within Iranian penitentiaries is a particular concern with their concentration of IDUs as well as high risk behaviours. Foremost, the majority of incarcerated IDUs, some HIV positive, will reintegrate back into their communities, and this is a particular concern for the spread of HIV and other transmitted diseases [8].
A 2006 study by Zamani et al. reported that 94% of IDUs in Iran have been incarcerated at least once in their lifetime. Among them, 28% reported using injec-tion drugs at least once within the prison; of these, 82% reported using a shared injection device, with 36% of
these individuals being HIV-positive [9]. A 2007 study by the same authors found that in their site-specific study of Karaj Central prison [10] in Iran, 42% of pris-oners reported to use intravenous drugs before their incarceration. A more recent 2013 study, reporting on 2009 data from a sample of 27 Iranian prisons, con-cluded that the prevalence of HIV among the prisoner population is 2.1%, and 8.1% among those who have a his-tory of IDU [3]. They also found that only 24% of pris-oners reported condom use during their last vaginal/anal sexual encounter in prison, 12.9% reported being tattooed while incarcerated, and only one in five had sufficient knowledge of the routes of HIV transmission and pre-ventative measures [8]. Such high risk behaviours among prisoners both before and during their incarceration have turned Iranian prisons into highly prospective environ-ments for acquiring HIV.
In response, triangular clinics (TCs) surfaced in Iranian prisons at the turn of the 21st century [11] as part of a co-ordinated, country-wide approach to the dual epidemic of HIV and IDU [12]. Iran has a long-standing commitment to supply reduction efforts, that is, largely enforcement ef-forts that aim to disrupt the manufacturing and distribu-tion of drugs, with a history of severe punishment for drug dealing. This coincides with the correctional system’s harsh and overcrowded prison conditions, detainment of political dissidents, and carrying out of prisoner execu-tions. However, with a high rate of IDU and an emerging HIV health epidemic, coupled with lessons learned from other countries, demand reduction efforts that focus on treatment and prevention were introduced to reduce indi-viduals’needs for drugs. Harm reduction clinics initiated in the community; these are drop-in centres in drug-ridden neighborhoods where former drug abusers assist with offering“needles, methadone, treatment for sexually transmitted diseases, AIDS tests and other medical care to their peers” [13]. The clinics transitioned into triangular clinics in the prison environment and similarly offer harm reduction measures. Both clinic types were embraced as both pragmatic and progressive in consideration of the country’s general conservative social climate [11,14]. In fact, Iran’s concept of the TC is largely unique across the globe [15]. In Canada and the United states, for example, the prison systems do not offer needle exchange even though IDU in these systems too is a concern; it is fre-quently a part of the fabric of prison life [16].
quality of life and empowerment of affected citizens [15]. These aims support the Health Belief Model (HBM) and its focus on informing beliefs (knowledge) and attitudes to eventually change behaviour, and specifically within the HV/AIDS field. “Within a harm reduction context, the HBM provides a systematic framework for examining the reasoning behind an individual’s choice to decrease, main-tain or increase their high risk behaviour”[17]. It is well established in the prevention and treatment literature that handing out clean needles in isolation from other support services, for example, is inadequate for sustainable behav-iour change [18].
The TCs provide a variety of harm reduction services in-cluding counseling, education, referral services, and treat-ment such as methadone maintenance therapy (MMT) [19]. For example, MMT is currently available to opioid-dependent prisoners in over half of the 230 prisons and correctional settings in Iran [10]. With the introduction of TCs and MMT, the total number of prisoners taking part in methadone therapy increased from 100 in 2002 to more than 25,000 in 2009 [1,20]. Since their introduction they have also expanded to address STIs in addition to HIV/ AIDS. However, still, relatively little research has been undertaken to assess the outcome of TC’s on behavior change. The aim of this study is to assess the immediate outcome of a TC on behavior change among injection drug users incarcerated in Rajaee-Shahr prison in Iran. Drawing on available data, the outcome indicators include (1) drug use, (2) change in attitude toward and belief about (knowledge) high risk behaviours, (3) serological conversion (HIV, HCV and HBV), and (4) engagement in risky behaviors (e.g., syringe exchange, condom use).
Methods
Setting and sample
In order to assess the immediate outcome of the TC as a health intervention in an Iranian prison, this study funded by the World Health Organization was under-taken in Rajaee-Shahr prison between 2003 and 2005. The lapse in time between the data collection and publi-cation of this paper in part reflects the detailed process for data release in the country. Ethics for the study was granted from the World Health Organization, Special Programme for Research and Training in Tropical Dis-eases, and the Iran Prisons Organization ethics commit-tee. Rajaee-Shahr prison is located 70 km northwest of Tehran (Iran’s capital) in the city of Karaj, has an inmate population of approximately 3,200 individuals, and is one of the most crowed and harsh prison environments in the country [12,20].
The study sample was a closed cohort of 150 incarcer-ated male injection drug users; the first 150 prisoners who voluntarily registered in the study were included. Given the conservative environment of the Iranian correctional
facility, this was deemed the best method to solicit partici-pation and is similar to how other topic sensitive studies have been carried out in the prison system [8]. In order to be eligible for selection, individuals must: (1) have been imprisoned for more than four months, (2) not have been diagnosed with a psychiatric disorder, (3) not have previ-ously accessed the TC or other harm reduction services in the prison, and (4) be an injection drug user and willing to take part in MMT. Verbal informed consent was acquired from all study participants. For individuals with low liter-acy, a designated and trained staff member was available to confidentially assist with the prisoners’participation in the study.
Data collection Stage one
The study was conducted in two stages: (1) the qualita-tive preparatory stage, and (2) the quantitaqualita-tive outcome testing stage. The first stage is addressed in detail in this paper and sets the necessary context for understanding the operation of a TC. In this preparatory stage, three focus groups were held. The groups were comprised of eight to ten men imprisoned in Rajaee-Shahr prison who were involved in high risk drug and sexual behaviors (e.g., needle sharing); all focus groups were held in Farsi language and lasted approximately two hours. The aim of this initial step in the study was to gather baseline un-derstanding about the target group’s knowledge, attitude, and practices related to IDU, HIV/AIDS, HBV, HCV, un-safe sexual practices, and other risky behaviors. These three foci reflect the Health Belief Model, which focuses on individuals’attitudes and beliefs in an attempt to ex-plain and predict health behaviors, in particular sexual and other high risk taking to prevent the transmission of HIV [19,21,22]. This data was used to review and revise the existing TC educational and medical interventions in Rajaee-Shahr prison as well as to construct the question-naire for the second step of the study – measuring im-mediate outcomes.
Stage two
psychology. The self-administered questionnaire was then tested for reliability among 40 randomly selected prisoners representative of the study target group imprisoned at Rajee-Shahr. With 34 responses, internal consistency of the questionnaire was measured with Cronbach’s Alpha test, and the outcome was greater than 74%.
In addition to the questionnaire, at pre-test each par-ticipant completed a personal history survey, a physical examination, testing for HIV, HBV and HCV viral infec-tion, STI testing, and urine analysis for drug residue. From this, physicians determined the medical needs of each participant and suggested various treatment options, including detoxification, STI counseling, and MMT. A health and education counseling session was held with each prisoner.
All 150 participants started MMT in groups of 5 to 10 (referred to as the attack phase). Throughout this phase, participants were closely monitored for several weeks in an isolated ward of the prison to minimize any unantici-pated effects of withdrawal and risks due to other drug use. The prescribed methadone dosage for each partici-pant was determined by a physician and accounted for the participant’s health status, drug use history, and other personal indexes. The daily dosage of methadone was between 80–125 mg. Following the attack phase, participants were relocated to the common ward of the prison where they received a maintenance dose of methadone (referred to as the loading phase). This phase was undertaken for a 6-month period, during which all participants received their daily dosage of methadone under the direct supervision of a trained health staff member. This marked the beginning of the outcome testing of the TC intervention.
After 6 months, the participants completed: (1) ran-dom urine analysis for opium/heroin residuals via thin-layer chromatography (TLC) to measure drug use, (2) the follow-up study questionnaire (to measure practice, knowledge, and attitude change), and (3) HIV, HBV, HCV viral infection testing. The study also issued and collected self-report behavior cards at four equal inter-vals over the 6 month period (at the end of months 2, 3, 4 and 5). The study benefited from applying these cards in two ways: to remind participants of the high risk for contracting viral infections (i.e., HIV, HBV, HCV) with risky behaviors (e.g., sharing sharp instruments such as a razor, tattooing, injecting drugs, sexual contact without using a condom), and to collect self-reported engage-ment in risky behaviours.
Results Participants
Of the 150 participants enrolled in the study, all re-ported to be of Iranian and Muslim descent, with 62% born in the province of Tehran. The mean age was
31.4 years (SD = 8.2). Only 21% graduated from high school or attended university, while 14% identified them-selves as illiterate. Eleven percent of participants reported being unemployed at their time of their incarceration. Fifty percent were single and had never been married, and of those that were married, 65 had children. The mean years of drug abuse was 10.97 (SD = 7.6) and the mean years of injection drug use was 5.39 (SD = 5.21). This translates into participants reporting to have spent, on average, a third of their lives abusing drugs (32% of life-time, SD = 17.08%), with engagement in injection drug use for approximately one-seventh of their lives (15.98% of lifetime, SD = 12.75%). A total of 103 participants com-pleted the full study.
More than 88% of the participants agreed to be tested for viral infections at the start of the study, of which 42.5% tested positive for HIV, 18.9% for HBV, and 75.9% for HCV. Ninety percent of participants were screened for sexually transmitted infections (gonorrhea and syph-ilis) and all were negative. A urinalysis was performed on 81% of participants; only one participant tested posi-tive and for a urinary tract infection. Although the find-ings of this study are unique to Rajaee-Shahr prison and therefore not directly transferable to other TCs in the Iranian correctional system, given the comparable con-text of HIV, IDU and incarceration across the country, they can provide important insight.
Stage one
The data collected in the qualitative preparatory stage of the study was systematically reviewed to recommend revisions to the current TC educational and medical in-terventions for high risk groups, primarily IDUs, in the prison (e.g., cultural adaption). They were originally de-veloped based on the best available knowledge at the time and this study was the first attempt to review the prisoner, staff and prison context for their implementa-tion. Attention was placed during this stage on prisoner behavior change. This stage was time intensive because all interventions needed to be compatible with prison rules and required staff education.
most popular and commonly injected drug among the prison population due to its ease of access, low cost, and efficiency.
Stage two
Drawing on available data, the outcome indicators include: (1) drug use, (2) change in attitude toward and belief about (knowledge) high risk behaviours, (3) serological conversion (HIV, HCV and HBV), and (4) engagement in risky behaviors (e.g., syringe exchange, condom use).
Drug use
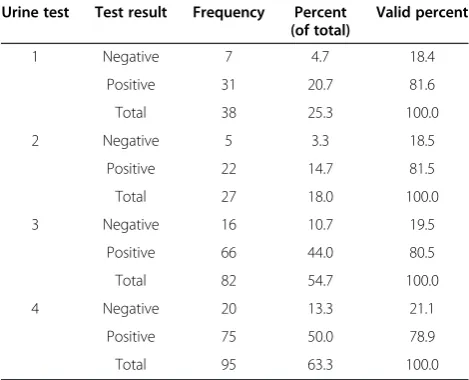
Throughout the TC intervention, random urine analysis using TLC was conducted to detect opium and heroin residuals, a strong indicator of injection drug use. Com-pliance was limited with only 64% of participants provid-ing samples at the four points. Positive drug results for opium and heroin were high, ranging from 78.9% to 81.6% of participants (see Table 1). The data does indicate a min-imal yet consistent decrease over time (from 81.6% to 78.9%), however, this was not significant (p = 0.982).
Practice, knowledge and attitude change
Analysis of the pre and post- self-administered question-naire data relayed that a change in IDU risky behaviours and associated sexual practices, although modest, was greater in comparison to knowledge and attitude (see Table 2) and also had the least respondent variability among the three components of the HBM. The results of a paired t-test (see Table 3) similarly revealed reduced engagement in risky practices following respondents’TC attendance (.000). Neither knowledge nor attitude ap-peared to be affected—positively or negatively.
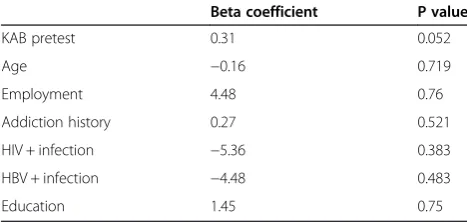
Applying multiple linear regression to examine a com-bined knowledge, attitude and behavior (KAB) score, the only significant determinant was the degree of knowledge, attitude and behaviour pre-test, adjusting for age, employ-ment, addiction history, viral infection status, and educa-tion. This may be partially explained by the size of the study population and the loss of follow-up participants. It can, however, be tentatively hypothesized that based on the coefficients a larger sample size may produce statis-tical significance.
Additional data analyses relayed that post-intervention KAB is significantly related to KAB at baseline (P = 0.05) (see Table 4). Further, individuals with positive test re-sults in HIV (Beta−5.36) and HBV (Beta−4.48) and also older in age (Beta −0.16 per 1 year increase in age) had acquired scores in KAB, although it was not statistically significant. Age may have an inverse effect on the KAB score as may viral infections (HIV and HBV). Both edu-cation and employment may have a positive effect.
HIV, HBV and HCV conversion
The findings of the questionnaire relaying a slight reduc-tion in IDU-related risky behaviour and this is consistent with the viral infection test results, which showed an increase in 1 HIV conversion, 21 HBV, and 9 HCV (see Figure 1). Although comparison data on conversions prior to the TC are not available, these findings are en-couraging among a high risk group of IDUs. Recall that at baseline 43% of respondents tested positive for HIV, 19% HBV and 76% HCV.
Table 1 Opium and/or heroin use during TC intervention
Urine test Test result Frequency Percent (of total)
Valid percent
1 Negative 7 4.7 18.4
Positive 31 20.7 81.6
Total 38 25.3 100.0
2 Negative 5 3.3 18.5
Positive 22 14.7 81.5
Total 27 18.0 100.0
3 Negative 16 10.7 19.5
Positive 66 44.0 80.5
Total 82 54.7 100.0
4 Negative 20 13.3 21.1
Positive 75 50.0 78.9
Total 95 63.3 100.0
Table 2 Practice, knowledge and attitude change
N Mean (% of maximum
achievable score)
Std. Deviation Percentage of mean score to maximum achievable score
Valid Missing Minimum Maximum
Knowledge pre-test 104 46 27.17 (0.69.6) 6.30 0 0.92
Knowledge post-test 53 97 27.63 (0.70.8) 5.29 0.45 0.89
Attitude pre-test 149 1 76.44 (0.73.5) 9.51 0.40 1.01
Attitude post-test 92 58 75.51 (0.72.6) 13.60 0.30 1
Practice pre-test 148 2 11.85 (0.59.2) 3.19 0.05 0.9
Risky practices
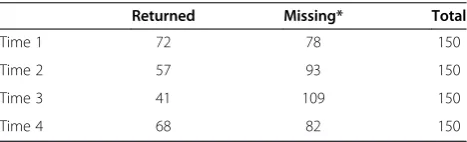
The completion rate for the self-report behaviour cards documenting the participants’high risk drug and sexual-related practices during the TC intervention was limited (see Table 5). Nonetheless, the data relay that over the course of the 6 month study, 53% of the study partici-pants remained free of any risky behaviour after two months of involvement in the intervention. Engagement in risky behavior increased throughout the 6 month period, with only 1.4% of the participants reporting be-ing risk-free after the total period of the study (i.e., 6 months) (see Table 6).
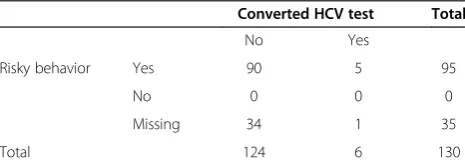
More specifically, focusing on HCV converted status because it had the highest initial viral infection rate among the prison population and therefore the greatest availability and accuracy of immediate test results, when risky practices at any of the four time points during the 6 month TC intervention were tested among participants who became HCV positive, the data collected on the self-report behavior cards showed that there was no sig-nificant difference between the risky behavior of con-verted cases and others (fisher’s exact test: 2sided = 1.00) (see Table 7).
Although not identified in the initial study design, two additional indicators of high risk behavior emerged as the study progressed. These were the frequency of ab-scess formation at the injection site, and the number of drug-related quarrels. According to informal clinical ob-servations and security records, there was no evidence of either of these issues among the study participants.
This again suggests that there was some reduction in risky behaviors.
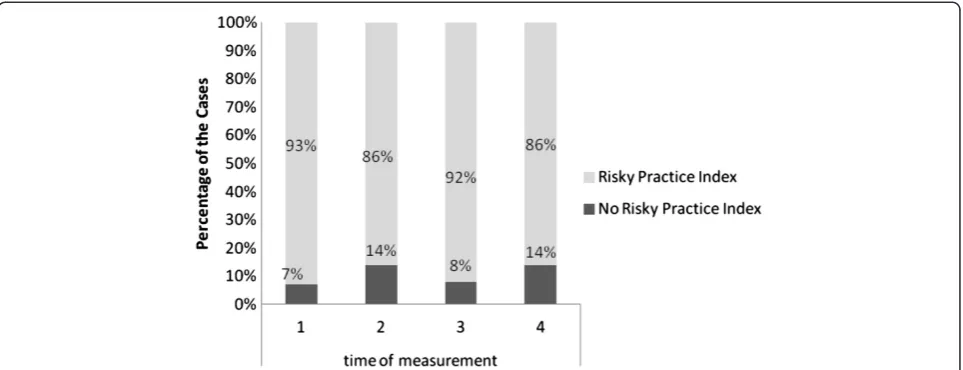
Risky practices index
In acknowledgement of the cultural taboo associated with intoxicant use in Iran and its potential impact on full dis-closure in the study, an index for participating in risky practices related to IDU was created through a combining of reported shared drug injection equipment and positive urine analysis. The findings relayed that 71% of partici-pants engaged in at least one high risk behaviour during the TC intervention, despite receiving the TC harm reduc-tion services. With 29% of the sample missing, it is un-known if any participants were totally free from risky behavior during the 6 month study period. Overall, par-ticipation in risky behaviour varied between 93% and 86% at the four reporting points over the course of the TC intervention (see Figure 2).
Discussion
The documented number of HIV cases in Iran increased 87% between 2001 and 2007 [23]. The vast majority of new cases were identified among IDUs [24-26]. The two key risk factors are imprisonment and the use of con-taminated injection equipment while incarcerated [9]. Likewise, recent studies of HCV among men incarcer-ated in Tehran, Iran identified a history of incarceration to be independently associated with HCV infection [27]. The same was found of HBV and sexually transmitted diseases [27,45]. The same cannot necessarily be applied to female prisoners in Iran [28]. A recent study of TCs in Hamadan province in Iran concluded that the estab-lishment of TCs is a starting point for organizing IDUs infected with HIV/AIDS to detect and address their dis-ease [29]. It is well established that there is a high preva-lence of high risk behaviors among IDUs [2], but there remains limited understanding about how to change the high risk behaviours of incarcerated individuals who in-ject drugs, including the immediate and long-term out-comes of TCs.
Although time consuming, it was critical that the first step in this study focused on generating knowledge about the prisoner population so that the existing Rajaee-Shahr TC educational and medical interventions could be appro-priately modified. For example, it was established that the low literacy level among the majority of prisoners who would access the TC needed to be considered in the avail-able written material. Offering services at the TC that are tailored to respond foremost to client needs is founda-tional to a harm reduction philosophy. It was also essential that baseline characteristics of the prisoner population were established to undertake step two of the study and the identification of outcome indicators, such as HIV, HCV and HBV status, which have been identified as Table 3 Pre and post-test impact of TC on practice,
knowledge and attitude
Variables Sig. (2-tailed)
Knowledge pre and post-test .937
Attitude pre and post-test .687
Behaviour pre and post-test .000
Combined knowledge, attitude and behavior pre and post-test
.419
Table 4 Knowledge, attitude and behaviour post-test association with independent factors
Beta coefficient P value
KAB pretest 0.31 0.052
Age −0.16 0.719
Employment 4.48 0.76
Addiction history 0.27 0.521
HIV + infection −5.36 0.383
HBV + infection −4.48 0.483
particularly problematic among individuals who inject drugs in Tehran, Iran [30].
The findings of this study relay that the immediate outcome of the TC in Rajaee-Shahr prison on behaviour change among injection drug users is modest. The prem-ise of the Health Belief Model–that individuals’attitudes and beliefs explain and predict health behaviors–did not support behaviour change over the six-month period. This does not mean, however, that the TC is ineffective. In fact, evidence to the contrary was concluded. It should also be kept in mind that Rajaee-Shahr prison is an institution in which individuals are sentenced for serious, long-term crimes and the volunteer sample for this study represents long-term, high risk IDUs. Consequently, the impact of harm reduction measures on knowledge and attitude may be minimal in the sort-term, even though some behavior was modified. A study by Shams et al. (2011) examined the impact of harm reduction approaches in Iranian prisons over a two year period and found there was not an immediate reduction (after one year/2007) in social behav-ior across the provincial institutions (e.g., self-harm, drug abuse, bullying), but that over the long-term (2 years/ 2008) there was [20].
Examining this study’s outcome indicators, it was con-cluded that introducing the TC intervention led to a minimal decrease in drug use (i.e., opium and heroin), although it did consistently decrease over the 6 month period. Once again, the high risk IDU prisoner popula-tion needs to be considered in interpreting this finding. This is a particularly important finding given that all participants in the study were prescribed MMT. Reasons for the participants’continued drug use while on MMT requires exploration, including whether it is in the indi-vidual’s best interest to be prescribed methadone. Future studies should investigate MMT dosage guidelines, means of distribution to combat diversion, and the source of
problematic drug use within the prison environment in order to provide the most effective TC harm reduction intervention.
Although the majority of participants continued their drug use, there was still some reported decrease in asso-ciated risky practices, although this was not sustained by the vast majority of participants over the six month intervention. With participants reporting long-term drug use, including IDU, it should not be expected that a swift change in behavior would occur. Although, a recent study of prisoners in Ghezel Hesar prison in Tehran, Iran found that“the rate of injecting in the prison unit…decreased drastically since introducing the MMT program” [31]. Further examination into the specifics of this intervention would be useful.
The corresponding absence of change in knowledge and attitude in the current study may in part be explained by the primary focus of the TC being on behaviour change, and the fact that individuals enrolled in the study may have already had altered beliefs and attitudes based on the preparatory stage of the study/at baseline. This finding may also suggest that access to harm reduction services, including MMT, has the potential to motivate prisoners to change their behavior without altering their current know-ledge or attitude. This is an important consideration to
Figure 1Viral infection status of study participants before and after TC intervention.
Table 5 Frequency of high risk practices on self-report behaviour cards
Returned Missing* Total
Time 1 72 78 150
Time 2 57 93 150
Time 3 41 109 150
Time 4 68 82 150
follow-up on, given that long-term change in high risk be-haviors, according to the Health Belief Model, requires change among all three components. This may in fact help to explain the lack of sustained behaviour change across the 6 month study period.
There was no difference found in engagement in risky behaviour among participants who became HCV posi-tive during the study and those that did not. This implies that a‘one size fits all’approach to practice change may not be warranted, which underpins the harm reduction philosophy of a TC. There is a need for much greater understanding about the intricacies of prisoners’ lives and their high risk drug use and sexual practice related behaviors [32].
It was also found that HIV and HBV positive status as well as older age may diminish change in knowledge, at-titude and practices. This may be explained by the feel-ing of hopelessness that may accompany a positive viral status and pessimism with older age. This is supported by the finding that the effect was stronger for HIV infec-tion. The opposite may be the case for participants with higher education and employment status. A 2010 survey of injection drug users in Iran similarly found that edu-cation greater than high school and permanent employ-ment were protective factors for HIV transmission [6].
The results of the current study suggest that existing interventions may not be as effective for extremely high risk groups like drug injecting prisoners who already are affected with viral infections and are well informed given their compromised health status; hence this may indicate the need for targeted interventions for specific groups [33].
It is well established that not enough is known about the high risk behaviors of IDUs in Iran, both generally
and particularly within prison sub-populations [31,34]. A baseline study of prisoners in Karaj Central prison, for example, found that injecting, in comparison to non-injecting drug-using prisoners, were more likely to have been tested for HIV infection [10]; this is useful informa-tion. In measuring the outcome of the TC, the current study only considered injection drug use and related risky practices. To further develop the TC, it would be useful to know more context-specific information, such as if the TC stimulates change in the extent to which drug users organize their lives around drug use, how much drug use is integrated into their lives, and the ways in which drug use negatively impacts other aspects of their health [35]. Related, it was determined that the most frequent viral infection among the participants was Hepatitis C. This is consistent with other studies of incarcerated groups [33], and should be given equivalent attention to HIV in the reduction measures being im-plemented within TCs.
Given the complex nature of this study, it has four key limitations. These may in part explain the absence of concrete findings. First, the attempt to measure both sex and non-sex related high risk behaviors in the conserva-tive social environment of a prison setting in Iran has extreme cultural and religious taboos. This may have translated into decreased levels of accuracy and compli-ance with reporting in the study. One means to address this was the development of a risky practices index (combined indicator of reported shared drug injection equipment and positive urine analysis results at the same sequence). In the future, the development of a less com-plex and lengthy questionnaire may want to be consid-ered, as well as observational reporting. Related, focus was paid to measuring prisoner behavior to the exclu-sion of considering the mutual role of staff in the TC and the prison environment (other than in the prepara-tory phase) in this study. Third, participant retention was a limitation of the study; it is anticipated that with an increased, non-punitive presence of the TC clinic within the prison environment as time progresses, pris-oners may be willing to report their IDU and associated risky practices. And fourth, the use of thin-layer chro-matography as the form of urine analysis in this study has potential problems in that it may produce incorrect conclusions; it can produce both a false positive and a Table 6 Timing of prisoners’practicing of risky behaviour
Interval End of month Total Engaged in risky behavior Lost Survival Std. error [95% Conf. Int.]
1 2 110 52 0 0.527 0.047 0.43 0.615
2 3 58 14 0 0.40 0.046 0.308 0.489
3 4 44 31 0 0.118 0.030 0.066 0.186
4 5 13 9 4 0.014 0.014 0.004 0.067
Table 7 Practicing of risky behaviors among participants who became HCV positive during the study
Converted HCV test Total
No Yes
Risky behavior Yes 90 5 95
No 0 0 0
Missing 34 1 35
false negative for various reasons, including the presence of drug metabolite-like chemicals in urine and human error. Although more expensive, more accurate tests may want to be applied in future studies.
Although the findings of this study are specific to Rajaee-Shahar prison in Tehran, Iran, it remains that the Iranian prisoner“population is under-served by HIV pre-vention services, as are the prison populations of many countries in the Middle East and Eastern Mediterranean regions” [12]. This recognition is transferable to other countries in the world. As the Iranian working group on drug treatment and rehabilitation in prison settings shared: “We believe that Iran with the unfortunately large addiction affliction has much to offer and in return is eager to learn when it comes to clinical interventions in drug abuse” [15]. Thus this study makes a contribu-tion to both understanding harm reduccontribu-tion practices within an Iranian prison and the international literature. As correspondent Ian Tanner writes forThe Majalla, an Arab magazine, “Despite the draconian policy towards punishing trafficking and the fact that treatment is not universally available, Iran’s drug policy is at the very least surprising, and perhaps even inspiring”[11].
Conclusion
The results of this study relay that the TC in Rajaee-Shahr prison had modest immediate impact (i.e., 6 months) in reducing high risk harmful behaviors among incarcerated IDUs. In its current form, it is unknown if the TC would bring about a sustainable, long-term reduction in harmful behaviors. This is particularly important considering the lack of significant change in knowledge and attitude re-lated to high risk practices; the three together comprise the Health Belief Model. Also, considering the large
number of missed cases at follow-up, it may further in-dicate the clinic’s benefits were either not evident or relevant to the participants. Past studies have shown that harm reduction initiatives are most effective when perceived benefit is high among participants [27]. Fu-ture research is required to determine the specific gaps in the current TC model.
In order to combat the HIV/AIDS epidemic in Iran, the results of this research must be considered not only in the context of the prison environment, but beyond to the general Iranian population [26]. The majority of the prisoners in Rajaee-Shahr prison will be released and will reintegrate into the general population where they have the potential to spread HIV and other viral infections [20]. We know from other studies that injection drug users engage in high risk behaviors outside the prison environment [2]. We also know that there is a need for practice and research-focused attention to be placed on the transition from prison to the community, and keep-ing up safe practices such as MMT. A recent study of HIV/AIDS in Iran emphasized “the need for intensified HIV prevention efforts with men who use drugs via in-jection and strengthened efforts to encourage the indi-vidual at risk to get tested for HIV” [26]. With a large number of IDUs filtering through the prison system in Iran, and the high rates of HIV, HBV and HCV, this may be an ideal catchment area. This is supported in other studies [36,37]; in the general Iranian community, people who wish to determine their HIV status are oftentimes prevented from doing so because of the sociocultural con-text. As a result, the impacts of the triangular clinic exam-ined in this study should be supported as one part of a broad, multi-faceted HIV/AIDS and other health behav-iour prevention strategy in the Islamic Republic of Iran.
Competing interests
The authors declare that they have no competing interests.
Authors’contributions
RTA and BE participated in the design of the study, collection of data, analysis and interpretation of data, drafting the article, and final approval of this version. CAD and KT participated in contextualizing the data, drafting the article, and final approval of this version. PA, MH and AM participated in reviewing drafts of this paper and final approval of this version. All authors read and approved the final manuscript.
Acknowledgements
This study was part of a larger study funded by the World Health Organization (IDNO: SGS03/67). The authors would like to acknowledge the World Health Organization for its financial support of the project. They would also like to acknowledge the cooperation of the Health Bureau of Iran Prisons Organization and personnel of the heath office of Rajaee-Shahr prison who made the prison and prisoners accessible to us, and kindly pro-vided us with access to assess their interventions. Dr (Ms) Marzieh Farnia, Director General of Health Bureau in Iran Prisons Organization and Dr (Ms) Joumana Hermes, Medical Officer of WHO-EMOR are specifically thanked for their review and comments on this article.
Author details
1World Health Organization, Tehran, Iran.2Arak University of Medical Science, Arak, Iran.3Department of Sociology & School of Public Health, University of Saskatchewan, Saskatoon, Saskatchewan, Canada.4Faculty of Medicine/ Medical School, University of Calgary, Calgary, Alberta, Canada.5Ministry of Welfare, Tehran, Iran.6Iran University of Medical Science, Tehran, Iran. 7
Institute for Health Policy Studies, School of Medicine, University of California, San Francisco, USA.
Received: 19 October 2011 Accepted: 3 December 2013 Published: 26 December 2013
References
1. Drug Control Bureau:Annual report of drug control.Tehran; 2001. 2. Momtazi S, Fallahnejad M, Shoghli A, Musavinasab N, Hajkarim B:Study of
high-risk behaviors among injecting drug users in Iran.InNational Institute of Drug Abuse Conference; 2009.
3. National AIDS Committee Secretariat, Ministry of Health and Medical Education:Islamic Republic of Iran AIDS Progress Report: On Monitoring of the United Nations General Assembly Special Session on HIV and AIDS; 2012. Retrieved from: http://www.unaids.org/en/dataanalysis/knowyourresponse/ countryprogressreports/2012countries/IRIran%20AIDS%20Progress%20Report %202012%20English%20final1_1.pdf.
4. Ministry of Health and Medical Education:HIV/AIDS in Iran (in Persian). Tehran; 2007.
5. Mirzazadeh A, Haghdoost A, Doostmohammadi P:Estimating the time trend of adjusted incidence of opioid dependency and multiple factors related to the lag time: backward calculation method.J Kerman Med Univ 2007,13(3):164–172.
6. Khajehkazemi R, Osooli M, Sajadi L, Karamouzian M, Sedaghat A, Fahimfar N, Safaie A, Mostafavi E, Haghdoost A-A:HIV prevalence and risk behaviours among people who inject drugs in Iran: the 2010 national surveillance survey.Sex Transm Infect2013:1–4. 10.1136/sextrans-2013-051204. 7. Khajehkazemi R, Osooli M, Sajadi L, Karamouzian M, Sedaghat A, Fahimfar N,
Safaie A, Mostafavi E, Haghdoost A-A:HIV Prevalence and risk behaviours among people who inject drugs in Iran: the 2010 National Surveillance Survey.Sex Transm Infect J2013:1–4. 10.1136/sextrans-2013-051204. 8. Navadeh S, Mirzazadeh A, Mehdi Gouya M, Farnia M, Alasvand R, Haghdoost
A-A:HIV prevalence and related risk behaviours among prisoners in Iran: results of the national biobehavioural survey.Sex Transm Infect2013:1–4. doi: 10.1136/sextrans-2013-051295.
9. Zamani S, Kihara M, Gouya M,et al:High prevalence of HIV infection associated with incarceration among community-based injecting drug users in Tehran, Iran.J Acquir Immune Defic Syndr2006,42:342–346. 10. Zamani S, Farnia M, Torknejad A, Alaei BA, Gholizadeh M, Kasaree F,
Ono-Kihara M, Oba K, Kihara M:Patterns of drug use and HIV-related risk behaviors among incarcerated people in a prison in Iran.J Urban Health 2010,87(4):603–616. doi:10.1007/s11524-010-9450-8.
11. Tanner I:The Lion Chases Away the Dragon: Iran’s drug treatment programs are among the world’s most progressive.The Majalla2013. Retrieved from: http://www.majalla.com/eng/2013/08/article55244942. 12. Farnia M, Ebrahimi B, Shams A,et al:Scaling up methadone maintenance
treatment for opioid-dependent prisoners in in Iran.Int J Drug Policy 2010,21:422–424.
13. Rosenberg T:An Enlightened Exchange in Iran.The New York Times: The Opinion Pages2010. Retrieved from: http://opinionator.blogs.nytimes.com/ 2010/11/29/an-enlightened-exchange-in-iran/.
14. Harrison F:Tackling Iran’s growing drugs problem.BBC News: Middle East 2004. Retrieved from: http://news.bbc.co.uk/2/hi/4054703.stm.
15. United Nations Office on Drugs and Crime:Triangular Clinic & Rehabilitation Centre.Iran; 2006. Retrieved from: http://www.unodc.org/treatment/en/ Iran_resource_centre_11.html.
16. Mehta D:AIDS prevention groups want prison needle programs to protect inmates, public.TV News, The Canadian Press2013. Retrieved from: http://www.ctvnews.ca/canada/aids-prevention-groups-want-prison-needle-programs-to-protect-inmates-public-1.1502466.
17. Eshrati B, Taghizadeh R, Dell CA, Afshar P, Millson PME, Kamali M, Weekes J: Preventing HIV transmission among Iranian prisoners: initial support for providing education on the benefits of harm reduction practices. Harm Reduct J2008,5:21.
18. Lenton S, Single E:The definition of harm reduction.Drug Alcohol Rev 1998,17:213–220.
19. Des Jarlais D:The public health paradigm for AIDS and the drug use: shifting the time frame.Br J Addict1990,85:348–349.
20. Shams A, Rabie N, Esmaili A, Baratvand M:The effect of the harm reduction approach in Iran’s prisons.IPEDR2011,20. Retrieved from: http://www.ipedr.com/vol20/37-ICHSC2011-M10018.pdf.
21. UNODC:World Drug Report Vienna: United Nations Office on Drugs and Crime; 2005.
22. Burrows D:Advocacy and coverage of needle exchange programs: results of a comparative study of harm reduction programs in Brazil, Bangladesh, Belarus, Ukraine, Russian Federation, and China.Cad Saude Publica2006,22:871–879.
23. UNAIDS:Report on the Global AIDS Epidemic Annex 1: HIV and AIDS estimates and data, 2007 and 2001.Geneva; 2008.
24. Razani N, Mohraz M, Kheirandish P,et al:HIV risk behavior among injection drug users in Tehran, Iran.Addiction2007,102:1472–1482. 25. Pourahmad M, Javady A, Karimi I, Ataei B, Kassaeian N:Seroprevalence of
and risk factors associated with hepatitis B, hepatitis C, and human immunodeficiency virus among prisoners in Iran.Infect Dis Clin Pract 2007,15:368–372.
26. Fallahzadeh H, Morowatisharifabad M, Ehrampoosh M:HIV/AIDS epidemic features and trends in Iran, 1986–2006.AIDS Behav2009,13:297–302. 27. Zamani S, Vazirian M, Nassirimanesh B,et al:Needle and syringe sharing
practices among injecting drug users in Tehran: a comparison of two neighborhoods, one with and one without a needle and syringe program.AIDS Behav2010,14(4):885–890.
28. Ghanbarzadeh N, Nadjafi Semnani M:A study of HIV and other sexually transmitted infections among female prisoners in Birjand.J Birjand Univ Med Sci2006,13:69–75.
29. Ghannad M, Arab S, Mirzaei M, Moinipur A:Epidemiologic study of human immunodeficiency virus (HIV) infection in the patients referred to health centers in Hamadan Province, Iran.AIDS Res Hum Retrov2009,25:277–283. 30. Rahimi-Movaghar A, Razaghi E, Sahimi-Izadian E, Amin-Esmaeili M:HIV,
hepatitis C virus, and hepatitis B virus co-infections among injecting drug users in Tehran, Iran.Int J Infec Dis2010,14(14):e28–e33.
31. Zamani S, Farnia M, Tavakoli S,et al:A qualitative inquiry into methadone maintenance treatmenmt for opiod-dependent prisoners in Tehran, Iran. Int J Drug Policy2010,21(3):167–172.
32. Rafiey H, Narenjiha H, Shirinbayan P,et al:Needle and syringe sharing among Iranian drug injectors.Harm Reduct J2009,6:21.
33. Taylor A, Goldberg D, Hutchinson S, Cameron S, Gore SM, McMenamin J, Green S, Pithie A, Fox R:Prevalence of hepatitis C virus infection among injecting drug users in Glasgow 1990–1996: are current harm reduction strategies working?J Infect2000,40:176–183.
35. Ruefli T, Rogers SJ:How do drug users define their progress in harm reduction programs? Qualitative research to develop user-generated outcomes.Harm Reduct J2004,1:8.
36. Mohammadpour A, Yekta ZP, Nikbakht Nasrabadi AR, Mohraz M:Coming to terms with a diagnosis of HIV in Iran: a phenomenological study.J Assoc Nurses AIDS Care2009,20:249–259.
37. Jahani MR, Alavian SM, Shirzad H, Kabir A, Hajarizadeh B:Distribution and risk factors of hepatitis B, hepatitis C, and HIV infection in a female population with“illegal social behavior”.Sex Transm Infect2005,81:185.
doi:10.1186/1477-7517-10-41
Cite this article as:Aslet al.:Outcome assessment of a triangular clinic as a harm reduction intervention in Rajaee-Shahr Prison, Iran.Harm Reduction Journal201310:41.
Submit your next manuscript to BioMed Central and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution