Clinical decision support systems
Full text
Figure
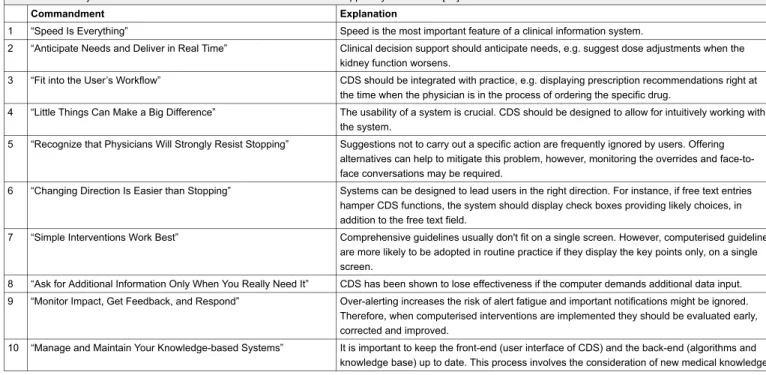
![Table 1: Overview of CDS types and functions, adapted from Wright et al. [15].](https://thumb-us.123doks.com/thumbv2/123dok_us/9212927.2805353/3.892.80.829.1019.1190/table-overview-cds-types-functions-adapted-wright-et.webp)
Related documents
Instructional designers work with multimedia, educational games, virtual realities, online learning & other cutting-edge projects... Jobs /
This implies a greater increase in the expected value of entering the industry following the opening of costly trade (equation (28)), and so a larger increase in the zero-pro fi
These trends surround increasing regulatory scrutiny on debit-interchange fee, design of sales force, Payment Cards Industry Data Security Standards (PCI-DSS) compliance, rising
He however notes that this is likely to give rise to two problems: Firstly, the Statute refers to ‘trial by another court’ and the term court is not inclusive of a truth
Berkay Celik ( Purdue University ); Abbas Acar, Hidayet Aksu ( Florida International University ); Patrick McDaniel ( Penn State University ); Engin Kirda ( Northeastern University
A raster-based stop detection algorithm (Section 3.2) is the core function that processes the GPS records into a stop/move structure while the raster cells are preserved
whether state anti-bootlegging laws protect the same rights as federal copyright laws and may not be preempted by Title 17 or Congress’s Copyright Clause authority. However,
Here, we consider the following issue. Consider a patient who decides to visit a health professional in an oce setting. We wish to identify factors that explain patient's choice
