Low-Intensity Exercise and Reduction of the Risk for
Falls Among At-Risk Elders
Robert O. Morgan,
1,2Beth A. Virnig,
3Maurice Duque,
4,5Elsayed Abdel-Moty,
6and
Carolee A. DeVito
4,71
Houston Center for Quality of Care and Utilization Studies, Houston VA Medical Center, Texas.
2
Baylor College of Medicine, Houston, Texas.
3
Division of Health Services Research and Policy, School of Public Health, University of Minnesota, Minneapolis.
4
The Miami VA Medical Center Health Services Research and Development Center, Florida.
5
Department of Exercise and Sport Sciences, School of Education, University of Miami, Coral Gables, Florida.
6
Departments of Industrial Engineering, College of Engineering, University of Miami, Coral Gables; Department of Neurological Surgery, School of Medicine, University of Miami; and Comprehensive Pain and Rehabilitation Center, University of Miami,
at South Shore Hospital and Medical Center, Miami Beach, Florida.
7
The Department of Psychiatry and the Behavioral Sciences, School of Medicine, University of Miami, Florida.
Background. Among elderly persons, falls account for 87% of all fractures and are contributing factors in many nursing home admissions. This study evaluated the effect of an easily implemented, low-intensity exercise program on the incidence of falls and the time to first fall among a clinically defined population of elderly men and women.
Methods. This community-based, randomized trial compared the exercise intervention with a no-intervention control. The participants were 294 men and women, aged 60 years or older, who had either a hospital admission or bed rest for 2 days or more within the previous month. Exercise participants were scheduled to attend exercise sessions lasting 45 minutes, including warm-up and cool-down, 3 times a week for 8 weeks (24 sessions). Assessments included gait and balance measures, self-reported physical function, the number of medications being taking at baseline, participant age, sex, and history of falling. Falls were tracked for 1 year after each participant’s baseline assessment.
Results. 29% of the study participants reported a fall during the study period. The effect of exercise in preventing falls varied significantly by baseline physical function level (p.002). The risk for falls decreased for exercise participants with low baseline physical functioning (hazard ratio, .51) but increased for exercise participants with high baseline physical functioning (hazard ratio, 3.51).
Conclusions. This easily implemented, low-intensity exercise program appears to reduce the risk for falls among elderly men and women recovering from recent hospitalizations, bed rest, or both who have low levels of physical functioning.
F
ALLS are the leading cause of nonfatal injuries in the United States and the second leading cause of all unintentional injury deaths, with 5.1 deaths per 100,000 persons annually (1–5). Among elderly men and women, falls account for 87% of all fractures and are contributing factors in 40% of nursing home admissions (6).The decline of muscle strength in elderly persons appears to be an important factor underlying poor balance as well as potential and actual falling (7,8). Similarly, an association has been found between tripping and the decline in gait velocity and step size (9), both of which may be related to muscle strength deficit in the lower extremities.
Although exercise programs can improve muscle strength, gait, and balance among elderly persons (9–11), the evidence that exercise decreases the number of falls is mixed (12). Exercise-related programs to reduce falls for general samples of community-residing elderly men and women have had the least success. In contrast, programs focusing on specific groups of at-risk elderly persons, such as older women (age 80þyears) (13,14) or elderly persons with gait or balance deficits (15), have been more effective, perhaps because these persons may benefit more from gains in strength than do persons who have higher levels of physical functioning (PF) (16).
Clinical events, such as hospitalizations and bed rest, lead to deconditioning and a higher risk for falls and injuries (17,18). The Study to Assess Falls Among Elderly–Geriatric Rehabilitation Intensive Program (SAFE-GRIP) was a ran-domized trial comparing community-based, short-term, low-intensity exercise intervention with ‘‘usual care.’’ The study’s goal was to determine whether the SAFE-GRIP exercise program improved functionality among elderly persons who were deconditioned as a result of bed rest associated with a hospitalization or illness and reduced the likelihood of falls. We previously reported data showing that, among persons who completed the preintervention and postintervention assessments, the SAFE-GRIP program significantly increased participants’ strength, gait, balance, and mobility, with the improvements maintained through the 6-month follow-up assessment. In contrast, participants in the control condition showed little or no improvement during the 2 months between the preintervention and postintervention assessments, followed by gradual improve-ment between the post-assessimprove-ment and 6-month follow-up examinations (10). These analyses evaluate the effect of the SAFE-GRIP program on the time to first fall among our clinically defined population of elderly men and women. 1062
METHODS
Participant Recruitment
Study participants were men and women aged 60 years or older. They had either a hospital admission lasting 2 days or longer or had been on bed rest for 2 days or more within the past month. Participants were classified as having been on bed rest for 2 or more days if they reported having more bed rest than normal for 2 or more consecutive days as a result of any illness.
Potential participants were identified by study staff from inpatient records at the Miami VA Medical Center or were identified by the registered nurse or physical therapist at their assisted living facility or outpatient physical therapy clinic. Potential participants were excluded if they had medical conditions that made it unsafe for them to participate in the exercise program (e.g., resting angina, severe osteoporosis) or interfered with their ability to follow instructions (e.g., dementia), required use of oxygen therapy at home, had planned future inpatient evaluations or treatments within the next 2 months, or required human assistance, a wheelchair, or artificial limbs to ambulate (use of a cane or walker was acceptable) (10).
Study participants were recruited from the Miami Department of Veterans Affairs Medical Center (VAMC), 9 assisted-living facilities in Broward and Dade Counties, Florida, and a private physical therapy clinic in Broward County. Each potential participant was screened initially by a registered nurse. This screening included a history of
falls during the past 12 months, the Folstein Mini-Mental State Examination (19), and a list of current medications. Potential participants who scored less than 23 on the Mini-Mental State Examination were excluded. After passing the initial screening and completing informed consent proce-dures (which were approved by the Miami VAMC Human Subjects Subcommittee), potential participants were screened by physicians to confirm that they could safely participate in the exercise program.
A total of 433 persons were identified and screened (97 from Miami VAMC and 336 from the other sites). Of the 433 persons screened, 101 were posthospitalization, 316 were post-bed rest, 4 were neither, and 12 were unsure. Two hundred ninety-four passed both the initial and the physician screenings and were randomized into the study. Virtually all participants who were posthospitalization were excluded because of one of the criteria in Table 1 (all but 1 of the randomized participants were post-bed rest). Table 1 lists the reasons for exclusion.
Randomization to the study arm (intervention versus control) was stratified by sex, age (,75 years versus75 years), and falls history during the past 12 months (fell or did not fall). This strategy was used to ensure that assignment to the treatment group was balanced with respect to factors that might correlate with study outcomes.
Assessments
The assessment protocol for this study has been reported previously (10). All participants completed their baseline assessment within 1 month of their index episode of hospitalization or bed rest. Assessments of gait and balance were obtained using Tinetti’s gait and balance assessment measures (20) and were performed by registered physical therapists at the participants’ assisted living facility or at a physical therapy rehabilitation clinic. Participants com-pleted the SF-36, a widely used measure of self-reported functional status (21), and reported the number of medications they were taking at their baseline assessment. Participant age, sex, and history of falls were obtained at recruitment.
Falls were tracked for 1 year after the baseline assessment. Participants were given predated postcard diaries to be completed and returned by mail every 2 weeks. These diaries were used to collect information about all falls occurring during each 2-week period.
Physical Restoration Intervention
Participants were organized into groups of approximately 5 persons. Each group was scheduled to attend exercise sessions 3 times a week for 8 weeks (24 total sessions). Each session lasted 45 minutes and consisted of 30 minutes of exercises, with sufficient rest periods within the session and a cool-down period. Exercises were performed in the sitting and standing postures (10). All sessions were supervised by a physical therapist assisted by a physical therapy assistant. No special equipment was required.
The physical restoration intervention was designed to directly affect neuromuscular functioning (i.e., muscle strength, joint flexibility), balance, and gait. Standard physical therapy exercises were selected to target these
Table 1. Reasons for Exclusion
Information Source Number Excluded
From initial screen:
Cannot ambulate without human assistance 25 Future inpatient evaluations or treatment
within next 2 months
19
Resting angina 14
Does not live at home or in an ALF 13
Unable to follow directions 10
Blind 6
Requires O2therapy at home 5
Not in the hospital or on bed rest for 2 or more days within the past month
4
Change in usual anginal pattern 3
Fractures due to osteoporosis 1
Seizure in the last 2 months 1
From physician screen:
Dementia 3
Severe osteoporosis 3
Plegia 2
Severe COPD 1
Chronic steroid usage 1
Severe obesity 1
Other:
Passed screening process but did not consent 26
Did not pass Folstein MMSE 1
Total 139
Note: ALF¼assisted living facility; O2¼oxygen; COPD¼chronic
areas (22) (Figure 1). The programs were individualized by allowing each participant to adjust the intensity of exercises according to his or her perception and progression. No cardiac monitoring was required during exercise. No participant reported cardiovascular distress during the ex-ercises that required cardiac or pulse monitoring. All parti-cipants tolerated the activity levels and workloads. Control participants were instructed to continue their usual activities during the study.
Statistical Methods
Contingency table analyses and analyses of variance were used to assess differences between our intervention and control groups on demographic measures and measures of baseline functioning. We used Cox proportional hazards models to assess the effect of the intervention on time to first fall. Persons who had not fallen were censored at the end of the 1-year follow-up period or at the time of last follow-up postcard for those who did not complete the entire follow-up period. Self-rated PF, using the SF-36 physical function subscale, was included in the models to determine specifically whether the effects of exercise in preventing falls varied between persons who had high rather than low PF. Analyses controlled for age, sex, falling history during the previous 12 months, baseline measures of gait and balance, and the number of medications reported at baseline. All analyses were conducted as ‘‘intention-to-treat’’ analyses.
RESULTS
Participant Characteristics
Of the 294 randomized participants, 245 were assessed at baseline. The 49 participants lost to attrition between consent and enrollment and the baseline assessment changed their minds regarding participation for a variety of reasons, including family members who reported having concerns about potential ‘‘hidden’’ costs to participation and participants being unwilling to begin once they contem-plated the time commitment, leaving the South Florida area to be cared for by relatives, and feeling ‘‘too sick’’ to start or, alternatively, ‘‘feeling better’’ and deciding not to begin the program. An additional 16 participants (8 exercise and 8 control) were omitted from these analyses because they were missing one or more of the measures.
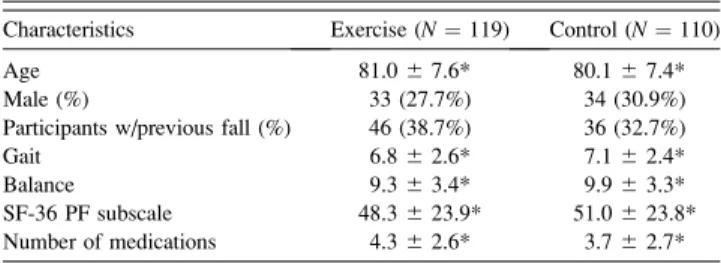
Two hundred twenty-nine participants had complete data (77.9% of the randomized sample and 93.5% of the participants having a baseline assessment). Among these persons, there were no differences between the exercise and control groups in terms of their average age, the percentage of men and women, the percentage of participants with falls in the previous year, their average gait, balance, PF subscale scores, or the average number of medications they were taking (Table 2).
Before analysis, participants were classified as having ‘‘high’’ baseline PF (PF subscale score55) versus ‘‘low’’ PF (PF,55) (23). The mean (6 standard deviation [SD])
Figure 1. Component exercises of the Study to Assess Falls Among Elderly– Geriatric Rehabilitation Intensive Program (SAFE-GRIP) study.
Table 2. Baseline Characteristics
Characteristics Exercise (N¼119) Control (N¼110)
Age 81.067.6* 80.167.4*
Male (%) 33 (27.7%) 34 (30.9%)
Participants w/previous fall (%) 46 (38.7%) 36 (32.7%)
Gait 6.862.6* 7.162.4*
Balance 9.363.4* 9.963.3*
SF-36 PF subscale 48.3623.9* 51.0623.8* Number of medications 4.362.6* 3.762.7*
Notes: *Mean6SD(standard deviation). PF¼physical function.
PF scores for our high and low PF groups were 70.9 (6 10.6) and 29.7 (6 13.3), respectively.
Study Attrition
Seventy-two of 229 (31.4%) participants dropped out of the study before reaching 1 of the study end points (i.e., their first fall or the end of the follow-up). These persons were included in the analyses, with their length of follow-up censored an average of 86.5 (685.7) days after randomi-zation. Neither frequency of censoring nor time to censoring varied by intervention group assignment. Men were more likely to drop out than were women (41.8% versus 27.2%, respectively; p , .03); however, this difference was con-sistent across intervention groups. Our baseline measures of age, history of falling, gait, balance, PF, and number of reported medications were all unrelated to study attrition.
Exercise Sessions
Overall, participants in the exercise group completed an average of 70% of the 24 scheduled exercise sessions (mean6SD, 16.8 68.4). Participants who dropped out of the study completed an average of 31.7% (7.667.4) of the exercise sessions compared with 82.9% (19.9 6 6.2) completed sessions by those who did not drop out.
Time to First Fall
Sixty-eight of the 229 (29.7%) study participants reported a fall during the study period. Table 3 shows the univariate associations of our study predictors with time to first fall. Participants were more likely to fall if they had a history of previous falls, were older, were taking more medications at baseline, or if they had low baseline PF or poor gait or balance.
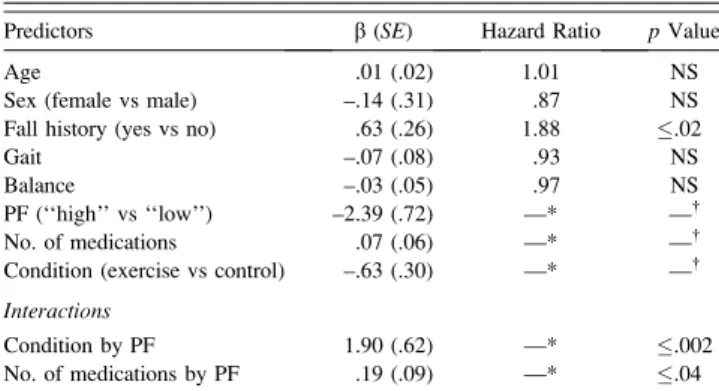
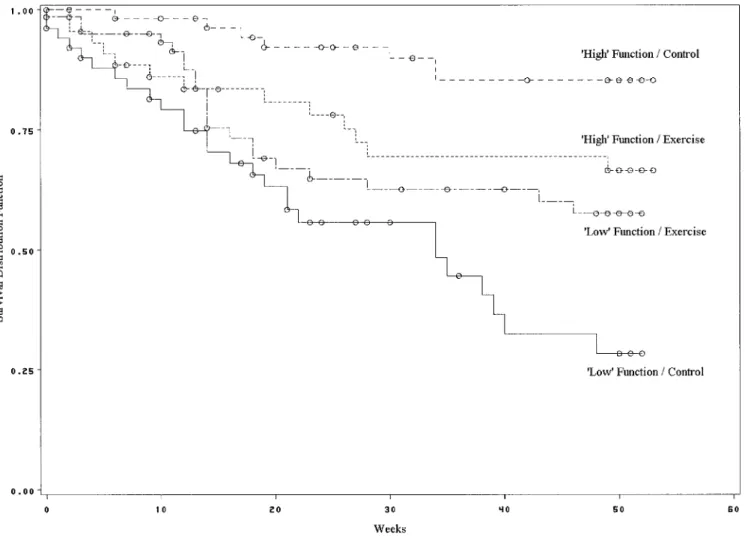
The proportion of participants who fell was comparable between the exercise and control groups (28.6% versus 30.9%, respectively). However, the effect of exercise in preventing falls varied significantly by PF level (p .002; Table 4). The risk for falling decreased for exercise participants with low baseline PF (p .03; hazard ratio [HR], .51) but increased for exercise participants with high baseline PF (p.02; HR, 3.51). This pattern is supported by the Kaplan-Meier curves for the exercise and control participants at high and low baseline PF levels (Figure 2). There was also a significant interaction between PF level and number of medications taken (p.04; Table 3). Both high and low PF participants reported using moderate numbers of medications at baseline (3.6 6 2.6 versus
4.46 2.7 [mean6 SD], respectively; p.02). However, increasing numbers of medications were only associated with a shorter time to first fall for participants with high PF (p.001; HR, 1.30) not for participants with low PF (p¼
not significant; HR, 1.06). Age, gait score, and balance score were not significantly related to time to first fall after controlling for PF level, history of falling, and number of medications.
DISCUSSION
Our results support recommendations that low-intensity exercise for the purpose of reducing the risk for falling is best targeted at specific subgroups of elderly men and women. In our study group, mild exercise was beneficial in preventing falls among participants with low PF, whereas exercise actually increased the risk for falling for those persons with better PF. These results are consistent with conclusions drawn by Gardner and colleagues (16) from their review of exercise interventions for preventing falls. They conclude that interventions targeted at higher functioning persons may be less effective because those persons may not have reached ‘‘threshold’’ levels of weakness at which functioning begins to be affected. In contrast, lower functioning persons may benefit significantly from relatively small increases in strength. Our results showing increased risk for high-functioning participants are also consistent with research indicating an association between increasing activity and increasing risks for falls (24,25). Our study also suggests that medication use has its greatest effect among elderly persons with relatively high PF levels, possibly because they are the most likely to be physically active and therefore to have more opportunities for falling. Thus, our results suggest that the mixed findings observed in earlier studies among community dwelling elderly persons may have, at least in part, been due to failure to examine or control for differences in outcomes among persons with high and low PF levels. Further research to confirm these differential effects would help clarify how best to target exercise interventions.
Our study had several limitations. First, participants were assigned to the PF subgroups after randomization. Thus, we
Table 3. Univariate Associations With Fall Risk
Characteristics b(SE) Hazard Ratio pValue
Age .04 (.02) 1.04 .01
Sex (female vs male) .12 (.29) 1.13 ns
Fall history (yes vs no) 1.02 (.25) 2.77 .0001
Gait –.22 (.05) .80 .0001
Balance –.13 (.04) .88 .001
PF (‘‘high’’ vs ‘‘low’’) –1.07 (.27) .34 .0001
No. of medications .13 (.04) 1.14 .001
Condition (exercise vs control) .05 (.24) 1.05 NS
Note: PF¼physical function;SE¼standard error; NS¼not significant.
Table 4. Model Results
Predictors b(SE) Hazard Ratio pValue
Age .01 (.02) 1.01 NS
Sex (female vs male) –.14 (.31) .87 NS
Fall history (yes vs no) .63 (.26) 1.88 .02
Gait –.07 (.08) .93 NS
Balance –.03 (.05) .97 NS
PF (‘‘high’’ vs ‘‘low’’) –2.39 (.72) —* —
No. of medications .07 (.06) —* —
Condition (exercise vs control) –.63 (.30) —* —
Interactions
Condition by PF 1.90 (.62) —* .002
No. of medications by PF .19 (.09) —* .04
Notes: *Hazard ratios (HRs) are not shown in the table for terms included in the interaction effects. See text for respective HRs.
Main effectpvalues are not shown in the table for terms included in the interaction effects. See text for thepvalues associated with the HRs.
could not fully capitalize on our randomized design to evaluate the relationship between baseline PF and the effects of our exercise intervention. Factors other than intervention group assignment may have played a role in the subgroup outcomes.
Second, we did not collect specific information on the participants’ exercise habits or activity levels. Thus, we do not know how many participants, if any, were regular exercisers, nor how their exercise habits may have affected our findings. Furthermore, because we did not include a measure of physical activity, we could not explicitly study the relationship between exercise and changes in activity level. We could not determine, therefore, whether our findings that exercise participants who were initially at high initial PF levels have an increased risk for falling is a result of an increase in their activity level.
Finally, we did not categorize medications by class. Previous research has shown that use of specific types of medications (e.g., psychotropic medications, medications that suppress abnormal heart rhythms such as digoxin) are related to higher risks for falling (26), and that reducing the use of psychotropic medications can reduce this risk (14). Although our findings indicate that use of increased
numbers of medications in general are related to increased risks for falls, at least among persons with high levels of PF, greater specificity of medication class would have allowed us to conduct more sensitive analyses of medication use and falls risk.
Conclusions
The HMO Workgroup on Care Management, which meets regularly to discuss delivery of care to Medicare beneficiaries, recognizes deconditioning as a primary area in which to provide interventions to reduce the risk for falls among elderly men and women, and further recognizes that transportation to physical therapy or exercise programs represents a significant barrier to program adherence (27). The SAFE-GRIP program is based on standard physical therapy exercises and is designed to be tailored to the functional abilities of individual participants. Specific attention was given to replicability by usual care site practitioners to increase the portability of the program to a variety of settings, as well as its inclusion in a multi-factorial falls reduction program, thereby reducing the need for additional transportation by program participants. Furthermore, because no special equipment was required,
the cost of the intervention is limited to the cost for the physical therapist and physical therapist assistant time.
This easily implemented, low-cost, low-intensity, in-dividualized exercise program appears to reduce the risk for falling among elderly men and women recovering from recent hospitalizations, bed rest, or both. However, the reduction in risk appears to depend on the PF level of the participants at baseline. Our results support the conclusion that low-intensity exercise for the purpose of reducing falls is most effective for elderly persons with low levels of PF. The program may actually increase the risk for falling for those participants at initially high levels of PF. Further research to confirm these differential effects would help clarify how best to target exercise interventions.
ACKNOWLEDGMENTS
The authors thank the Research Service of the Miami Department of Veterans Affairs Medical Center and South Shore Hospital and Medical Center, Miami Beach, Florida, for their support and assistance. We are also grateful to Nelda Wray, MD, MPH, Nancy Wilson, MSW, MPH, and George Taffet, MD, for their comments on earlier versions of this manuscript.
Supported by the Office of Research and Development Health Services R & D Service, Department of Veterans Affairs (HSR&D IIR 94-003).
Address correspondence to Robert O. Morgan, PhD, Houston Center for Quality of Care and Utilization Studies, VA Medical Center (152), 2002 Holcombe Boulevard, Houston, TX 77030. E-mail: rmorgan@bcm.tmc.edu
REFERENCES
1. Baker SP, O’Neil B, Karpf RS.The Injury Fact Book.Lexington, MA: Lexington Books, 1984.
2. National Safety Council.Accident Facts.Chicago, IL: National Safety Council; 1985.
3. Committee on Trauma Research, Commission on Life Sciences, National Research Council, Institute of Medicine.Injury in America.
Washington, DC: National Academy Press; 1985.
4. Rice DP, Mackenzie EJ, Associates.Cost of Injury in the United States: A Report to Congress. San Francisco, CA Institute for Health and Aging, University of California and Injury Prevention Center, The John Hopkins University; 1985.
5. Sattin RW. Falls among older persons: a public health perspective.
Annu Rev Publ Hlth.1992;13:489–508.
6. The prevention of falls in later life. A report of the Kellogg International Work Group on the Prevention of Falls by the Elderly.
Dan Med Bull.1987;34(Suppl 4):1–24.
7. Murray MP, Gardner GM, Mollinger LA, Sepic SB. Strength of isometric and isokinetic contractions: knee muscles of men aged 20 to 86.Phys Ther.1980;60:412–419.
8. Whipple RH, Wolfson LI, Amerman PM. The relationship of knee and ankle weakness to falls in nursing home residents: an isokinetic study.
J Am Geriatr Soc.1987;35:13–20.
9. Imms FJ, Edholm OG. The assessment of gait and mobility in the elderly.Age Ageing.1979;8:261–267.
10. DeVito CA, Morgan RO, Duque M, Moty EA, Virnig BA. Physical performance effects of low intensity exercise among clinically defined high-risk elders.Gerontology.2003;49:146–154.
11. Signoile JF, Carmel MP, Czaja SJ, et al. Differential increases in average isokinetic power by specific muscle groups of older women due to variations in training and testing.J Gerontol Med Sci.2002;57A: M683–M690.
12. Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH. Interventions for preventing falls in elderly people (Cochrane Review). In:The Cochrane Library,Issue 2, 2002. Oxford: Update Software; 2002.
13. Campbell AJ, Robertson MC, Gardner GM, O’Neil B, Tinetti ME. Randomised controlled trial of a general practice programme of home-based exercise to prevent falls in elderly women. BMJ. 1997;315: 1065–1069.
14. Campbell AJ, Robertson MC, Gardner MM, Norton RN. Falls prevention over 2 years: a randomized controlled trial in women 80 years and older.Age Ageing.1999;28:513–518.
15. Buchner DM, Cress ME, de Lateur BJ, et al. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults.J Gerontol A Med Sci Biol Sci.1997; 52A:M218–M224.
16. Gardner MM, Robertson MC, Campbell AJ. Exercise in preventing falls and fall related injuries in older people: a review of randomised controlled trials.Br J Sports Med.2000;34:7–17.
17. Final Report to the Study to Assess Falls Among Elderly (SAFE). Submitted to the Centers for Disease Control by the Department of Health and Rehabilitative Services, Dade County Public Health Unit, Miami, Florida, June 1990.
18. DeVito CA, Sattin RW. SAFE Study Group.Developing a Model of Outcome Measures for Intervention Studies: Fall Related Injuries Among the Elderly.Springfield, IL: Charles C Thomas; 1991. 19. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: a practical
method for grading the cognitive state of patients for the clinician.
J Psychiatr Res.1975;12:189–198.
20. Tinetti ME. Performance-oriented assessment of mobility problems in elderly patients.J Am Geriatr Soc.1986;34:119–126.
21. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection.Med Care.1992; 30:473–483.
22. O’Sullivan S, Cullen K, Schmitz T.Physical Rehabilitaton: Evaluation and Treatment Procedures. Philadelphia, PA: FA Davis Company; 1981.
23. Morgan RO, Duque M, DeVito CA. Using the SF-36 Physical Function Subscale to screen for falls-risk in a clinically defined sample of at-risk elders. Presented at the annual meeting of the Gerontological Society of America, Boston, Massachusetts; 2002.
24. King MB, Tinetti ME. Falls in community-dwelling older persons.
J Am Geriatr Soc.1995;43:1146–1154.
25. Rubenstein LZ, Josephson KR, Trueblood PR, et al. Effects of a group exercise program on strength, mobility, and falls among fall-prone elderly men.J Gerontol Med Sci.2000;55A:M317–M321.
26. Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: II. Cardiac and analgesic drugs.J Am Geriatr Soc.1999;47:40–50.
27. HMO Workgroup on Care Management.Improving the Care of Older Adults With Common Geriatric Conditions.Washington DC: AAHP Foundation; 2002.
Received December 13, 2002 Accepted March 13, 2003