Relation of Serum Testosterone Levels to
High Density Lipoprotein Cholesterol and
Other Characteristics in Men
David S. Freedman, Thomas R. O'Brien, W. Dana Flanders,Frank DeStefano, and Joseph J. Barboriak
Although levels of high density lipoprotein (HDL) cholesterol in males decrease during adolescence and after treatment with testosterone derivatives, several studies have reported that levels of HDL cholesterol are positively associated with endogenous levels of testosterone in men. This association was further examined using data collected during 1985 and 1986 from 3,562 white and 500 black men who ranged in age from 31 to 45 years. Black men had higher mean levels of both HDL cholesterol (8 mg/dl) and total testosterone (33 ng/dl) than white men, and positive associations were observed between testosterone and HDL cholesterol levels (r=0.22, whites; r=0.26, blacks). In addition, levels of testosterone were related positively to alcohol consumption and cigarette smoking and negatively to age, Quetelet index, and use of 0-blockers. We used stratification and regression analyses to determine if any of these characteristics could account for the positive association between levels of HDL cholesterol and total testosterone. Although controlling for most factors had little influence, adjusting for Quetelet index reduced the strength of the association between levels of testosterone and HDL cholesterol by approximately 30%. These findings suggest that the positive association between levels of testosterone and HDL cholesterol may not be causal. Multivariable analyses that control for obesity and other potentially confounding characteristics should be used in studies that assess the relation of testosterone levels to coronary heart disease. (Arteriosclerosis and Thrombosis 1991;ll:307-315)
M
iddle-aged men in industrialized countries are at a threefold to 10-fold higher risk for coronary heart disease (CHD) than are women.1 Several investigators1"3 have assessed possible determinants of this sex differential, and it has been suggested that sex hormones play an impor-tant role, possibly through their regulation of lipo-protein metabolism. During adulthood, premeno-pausal women have higher levels of high density lipoprotein (HDL) cholesterol but lower levels of triglycerides and low density lipoprotein (LDL) cho-lesterol than do men.4From the Agent Orange Projects (D.S.F., W.D.F.), Center for Environmental Health and Injury Control, and the Center for Infectious Diseases (T.R.O.'B., F.D.), Centers for Disease Con-trol, Public Health Service, US Department of Health and Human Services, Atlanta, Ga., and the Department of Pharmacology and Toxicology (JJ.B.), Medical College of Wisconsin, Milwaukee Veterans Affairs Medical Center, Milwaukee, Wis.
Data for this study were gathered under an interagency agree-ment with the Veterans Administration.
Address for reprints: David S. Freedman, PhD, Centers for Disease Control, A-41, 1600 Clifton Road, Atlanta, GA 30333.
Received August 27, 1990; revision accepted October 23, 1990.
Some evidence suggests that estrogen and testos-terone are important determinants of levels of HDL cholesterol. During adolescence, levels of HDL cho-lesterol decline by more than 10 mg/dl in boys but not in girls,5'6 and large decreases are seen after treat-ment with testosterone derivatives.67 Although levels of HDL cholesterol increase after administration of estrogenic hormones,8 levels are low among women using oral contraceptives containing norgestrel, a progestin with androgenic activity.9 Because of these associations, it has been thought that the sex differ-ential in CHD may be due to the influence of sex hormones on levels of lipids and lipoproteins.
In contrast to these findings, however, several unexpected associations with endogenous levels of estrogen and testosterone have been reported. For example, in contrast to what might be anticipated on the basis of the lower incidence of CHD among women, Phillips10 reported that 15 men who survived a myocardial infarction had higher levels of estrogen than men in a control group. In addition, although there are exceptions,11 most cross-sectional studies of men have reported a positive association between endogenous levels of testosterone and HDL
choles-terol,12"17 with correlation coefficients ranging as high as 0.65.1<s These studies, however, have included only whites, and most were relatively small.
Some investigators11114 have suggested that the positive association between levels of testosterone and HDL cholesterol may be due to the confounding effects of obesity, alcohol intake, or sex hormone-binding globulin (SHBG).1-11-14 Although age-related decreases in testosterone levels are well established, relatively few investigators have examined other cor-relates of testosterone. Limited evidence, however, suggests that testosterone levels are associated in-versely with relative weight and positively with ciga-rette smoking.1417"19 The objective of this study of 4,062 men, 500 of whom are black, is to examine further the association between levels of total tes-tosterone and HDL cholesterol. In addition^ the influence of several characteristics (e.g., race, relative weight, alcohol consumption, cigarette smoking, and various medications) on the association between lev-els of testosterone and HDL cholesterol in these 31-to 45 -year-old men will be assessed.
Methods
Population
Subjects were participants in a historical cohort study comparing the health of Vietnam veterans with veterans who served elsewhere. Although the study was designed to examine the general experience of military service in Vietnam, much of the initial concern focused on exposure to Agent Orange and its contaminant, 2,3,7,8-tetrachlorodibenzo-p-dioxin. Data were obtained during 1) a telephone interview and 2) a medical examination of a random sample of telephone interviewees. Sample selection, interviews, and examinations were performed in 1985 and 1986 and have been described in detail elsewhere.20
Briefly, a random sample of 48,500 men who entered the US Army between 1965 and 1971 was generated. To increase the baseline comparability of men who were stationed in Vietnam with other veterans, participation was limited to men who 1) served only one term, 2) had 16 weeks or more of active service, 3) earned a military occupational specialty other than "trainee" or "duty soldier," and 4) had a pay grade at discharge no higher than that of sergeant. A total of 17,867 veterans were considered eligible for the study, with 9,078 (51%) having served in Vietnam.
Of these men, 15,288 (87% of Vietnam veterans and 84% of non-Vietnam veterans) were located and given a structured interview by telephone. Of those interviewed, 6,443 men were randomly selected to participate in medical and psychological examina-tions conducted at the Lovelace Medical Foundation in Albuquerque, N.M. Of those invited to the exam-ination, 4,462 men (75% of Vietnam veterans and 63% of other veterans) actually participated.
Our analyses are restricted to the 3,562 white men and 500 black men who were between the ages of 31
and 45 years at the time of the medical examination. Men were excluded for one or more of the following reasons: Hispanics (n=200), Asians (rc=34), Native Americans (n=49), and men older than 45 years of age (n=5). Also excluded were men who reported that they had not fasted before the examination (n=47), whose weight was not recorded at the medical examination (n=l), or who had been told by a physician that they were diabetic (n=46) or had suffered a heart attack (n=18). In addition, men who did not answer questions concerning frequency of alcohol consumption (n=10) or cigarette smoking (n=2) were deleted from analyses involving these variables.
Risk Factor Information
Telephone interview and medical examination.
Infor-mation on race was obtained during the telephone interview for more than 99% of the veterans, and Army records were used to find this information for the remaining men. Data on household income and educational achievement were also obtained during the telephone interview. Data on cigarette smoking (current smoking status and mean number of daily cigarettes) and alcohol consumption (average num-ber of days per month during which alcohol was consumed and mean number of daily drinks) were obtained in a standardized interview during the medical examination. Information on the current use of medications, including specific names, was also collected. Use of £-blockers, hydantoins, and ana-bolic steroids is included in several analyses because of reported associations with levels of HDL choles-terol.21 Quetelet index, a measure of relative weight, was calculated as weight in kilograms divided by height in meters squared.
Data collected during the telephone interviews were used to assess the similarity between the 4,462 men who participated in the medical examination and the 10,826 men who did not, and only minor differences were found. For example, 11% of the 10,826 men inter-viewed by telephone only were black, whereas 12% of the 4,462 men who participated in the medical exami-nation were black. Furthermore, participation in the medical examination was not associated with marital status, household income, cigarette smoking status, Quetelet index (calculated from self-reported weight and height), or alcohol consumption. Men who partic-ipated in the medical examination, however, tended to be slightly more educated than those interviewed only by telephone.22
Laboratory determinations. Because animal studies
have suggested that exposure to 2,3,7,8-tetrachloro-dibenzo-p-dioxin may lead to hyperlipidemia23 and decreased levels of testosterone,24 these characteris-tics were measured as part of the medical examina-tion. Venipuncture was performed after an overnight fast. Although levels of testosterone exhibit a strong diurnal cycle, the effects of this variation on the study results should be minimal because all blood samples were obtained between 8 and 10 AM, near the time of peak testosterone levels.25
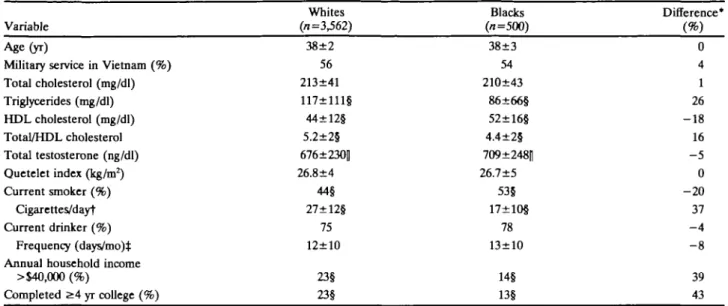
TABLE 1. Comparison of Selected Characteristics in Men: Vietnam Experience Stndy, 1985-1986 Variable Whites (0=3,562) Blacks (n=500) Difference* Age (yr)
Military service in Vietnam (%) Total cholesterol (mg/dl) Trigfycerides (mg/dl) HDL cholesterol (mg/dl) Total/HDL cholesterol Total testosterone (ng/dl) Quetelet index (kg/m2) Current smoker (%) Cigarettes/dayt Current drinker (%) Frequency (days/mo)$ Annual household income
>$40,000 (%) Completed 2:4 yr college (%) 38±2 56 213±41 117±111§ 44±12§ 5.2±2§ 676±230| 26.8±4 44§ 27±12§ 75 12±10 23§ 23§ 38±3 54 210+43 86±66§ 52±16§ 4.4±2§ 709±248|] 26.7±5 53§ 17±10§ 78 13±10 14§ 13§ 0 4 1 26 - 1 8 16 - 5 0 - 2 0 37 - 4 39 43 HDL, high density lipoprotein.
Except for percentages, all values are mean±SD.
'Percentage difference between blacks and whites: [(mean level among whites—mean level among blacks)] + (mean level among whites). tRestricted to current smokers (1,572 whites, 264 blacks).
^Restricted to current drinkers (2,672 whites, 387 blacks). p values were assessed using t tests or \2 tests: §p<0.001, |[p<0.01.
Levels of total cholesterol were assayed by an en2ymatic method, and HDL cholesterol was mea-sured after precipitating the LDL and very low density lipoprotein cholesterol fractions with dextran sulfate. The laboratory used an Ektachem 700 (Eastman Ko-dak, Rochester, N.Y.), and in addition to internal controls, the Centers for Disease Control standard-ized and monitored the laboratory.26 Levels of trigryc-erides were determined by an enzymatic method, and levels of total testosterone were measured with a standard, double-antibody radioimmunoassay system (Leeco Diagnostics, Inc., Southfield, Mich.).27
All laboratory determinations were monitored by using bench and "blind" repeat quality control pro-cedures. The coefficient of variation for the various laboratory measurements ranged from 2.6% to 3.7% for HDL cholesterol and from 4.5% to 9.7% for testosterone.26
Statistical Methods
Using t tests, we assessed differences in mean levels of HDL cholesterol, testosterone, and other characteristics between black and white men; differ-ences in categorical variables were assessed using x2 tests. In addition to regression analyses, we examined graphically the association between levels of tes-tosterone and age using smoothed medians28 because of 1) the small numbers of black men at various ages and 2) uncertainty concerning the shape of the association between age and testosterone. We exam-ined race-specific associations between levels of tes-tosterone and other characteristics using stratifica-tion and age-adjusted correlastratifica-tion coefficients; both Pearson and Spearman correlations yielded similar results. F tests were used to examine linear trends in
levels of testosterone across categorical variables having more than two levels.
We then examined whether the observed associa-tion between levels of testosterone and HDL choles-terol was due to confounding by extraneous variables. The association between levels of testosterone and HDL cholesterol was examined within strata of sev-eral covariates (e.g., age and cigarette smoking). With HDL cholesterol as the dependent variable in regression analyses, we also examined changes in the magnitude of the coefficient for testosterone after adjusting for additional covariates.29 In all analyses, the use of logarithmically transformed values for testosterone and HDL cholesterol yielded results similar to those obtained by using the original values.
Results Descriptive Characteristics and Black/White Comparisons
Levels of selected characteristics are compared be-tween white and black men in Table 1. The mean age among both groups was 38 years, and similar propor-tions of black men and white men were Vietnam veterans. Levels of total cholesterol, Quetelet index, and alcohol consumption were also similar for both groups. Among blacks, however, mean levels of triglyc-erides were 26% (31 mg/dl) lower, while mean HDL cholesterol levels were 18% (8 mg/dl) higher than among whites. We also found smaller but statistically significant differences in testosterone levels, with mean levels 5% (33 ng/dl) higher among black men than among whites. A larger proportion of black men smoked cigarettes than did whites, but among the smokers, white men reported smoking more cigarettes
100 if ?5
I
£ 501
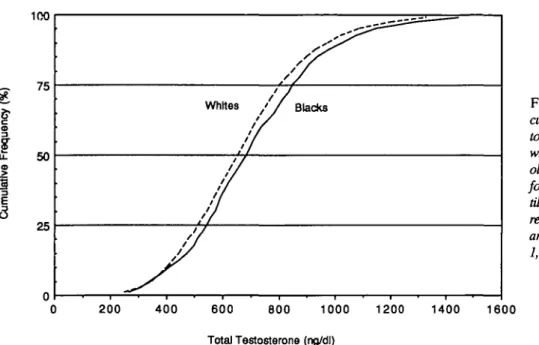
25Whites / / Blacks FIGURE 1. Cumulative frequency
curve showing distribution of tes-tosterone levels (mg/dl) in 3,562 white and 500 black 31- to 45-year-old men. Among whites, the levels for the 10th, 50th, and 90th
percen-tiles are 405, 656, and 974 ngldl, respectively. Corresponding levels among blacks are 415, 684, and 1,027 ngldl, respectively.
0 200 400 600 800 1000 Total Testosterone (ng/dl)
1200 1400 1600
per day. Fewer than 1% of the examined men reported using J3-blockers, hydantoins, or anabolic steroids.
B S 5 300 55 50 45 40 35 30 40 45 / -Whites V Blacks -• 30 35 40 45 Age(yeara)
FIGURE 2. Line graphs showing median levels o)'testosterone (ng/dl) (panel A) and high density lipoprotein (HDL) choles-terol (mgldl) (panel B) by age in blacks (-) and whites ( — ) . Median values have been smoothed in groups of three because of the small sample sizes at various ages.
Although levels of total testosterone were posi-tively skewed (Figure 1), the difference in median levels between the two groups (684 ng/dl in blacks versus 656 ng/dl in whites) was comparable to the 33 ng/dl difference in mean levels. Despite these differ-ences in average levels, similar proportions of black and white men had low levels of testosterone: the fifth percentiles were 341 and 349 ng/dl, and the 10th percentiles were 405 and 415 ng/dl, respectively.
Despite the relatively young ages of the subjects, levels of testosterone were inversely associated with age: correlation coefficients were -0.17 among whites and —0.29 among blacks. An examination of median testosterone levels by age (Figure 2) sug-gested that the difference between black and white men decreased with age. As estimated by regression analyses that included race x age terms, the higher mean testosterone levels among blacks decreased from 97 ng/dl (among 31- to 35-year-olds) to 7 ng/dl (among 41- to 45-year-olds), a significant (p<0.01) interaction. In contrast to these associations, HDL cholesterol levels were not linearly associated with age (r=-0.01 [whites] and -0.04 [blacks]), and age did not modify the black/white difference, p=Q37.
Association Between Levels of Testosterone and High Density Lipoprotein Cholesterol
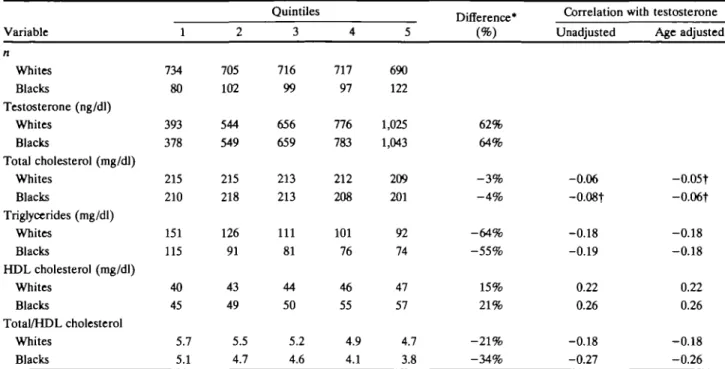
Mean levels of the lipids and lipoproteins accord-ing to testosterone quintile and correlation coeffi-cients are shown in Table 2. Levels of total testoster-one showed little association with total cholesterol but were associated inversely with levels of triglycer-ides (r=-0.18 to -0.19) and positively with levels of HDL cholesterol (r=0.22 to 0.26). Men in the highest testosterone quintile had mean levels of HDL cho-lesterol that were 7 mg/dl (whites) to 12 mg/dl (blacks) higher than those observed among men in
TABLE 2. Mean Levels of LJpids and Lipoproteins According to Qnintiles of Testosterone: Vietnam Experience Study, 1985-1986 Variable n Whites Blacks Testosterone (ng/dl) Whites Blacks TotaJ cholesterol (mg/dl) Whites Blacks Triglycerides (mg/dl) Whites Blacks HDL cholesterol (mg/dl) Whites Blacks Total/HDL cholesterol Whites Blacks 1 734 80 393 378 215 210 151 115 40 45 5.7 5.1 2 705 102 544 549 215 218 126 91 43 49 5.5 4.7 Quin tiles 3 716 99 656 659 213 213 111 81 44 50 5.2 4.6 4 717 97 776 783 212 208 101 76 46 55 4.9 4.1 5 690 122 1,025 1,043 209 201 92 74 47 57 4.7 3.8 Difference* (%) 62% 64% - 3 % - 4 % - 6 4 % - 5 5 % 15% 2 1 % - 2 1 % - 3 4 % Correlation with Unadjusted -0.06 -0.08t -0.18 -0.19 0.22 0.26 -0.18 -0.27 testosterone Age adjusted -0.05t -0.06t -0.18 -0.18 0.22 0.26 -0.18 -0.26 HDL, high density lipoprotein.
'Calculated as [(mean level among men in quintile 5-mean level among men in quintile l)]+(mean level among men in quintile 5). Allp values are <0.001 unless noted; t/>>0.001.
the lowest quintile. Adjustment for age did not affect the magnitudes of the examined associations.
Adjustment for Other Characteristics
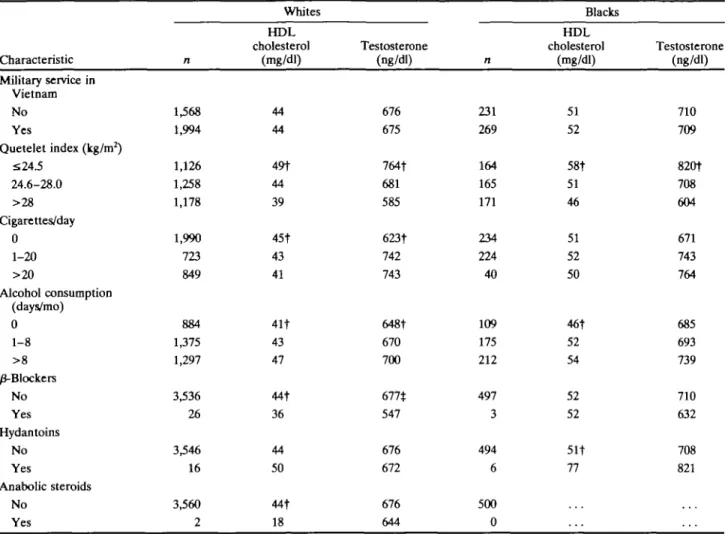
Table 3 shows mean age-adjusted levels of HDL cholesterol and testosterone within categories of several characteristics. Although there were small differences between blacks and whites in the magni-tudes of the observed associations, levels of HDL cholesterol were, as expected, related inversely to both Quetelet index and cigarette smoking and pos-itively to alcohol consumption. (As compared with white men, the association between smoking and levels of HDL cholesterol in blacks was more strongly confounded by alcohol consumption.) Levels of tes-tosterone were most strongly associated with Quete-let index, with the heaviest men (>28 kg/m2) having mean levels that were about 200 ng/dl lower than men who were relatively thin (^24.5 kg/m2). Al-though alcohol consumption was positively associ-ated with levels of testosterone, the relations of smoking to levels of HDL cholesterol and testoster-one differed. Cigarette smoking was related inversely to levels of HDL cholesterol but positively to tes-tosterone, with mean testosterone levels 120 ng/dl (743-623 ng/dl) higher among white men who smoked more than 20 cigarettes per day than among nonsmokers. The comparable difference among black smokers and nonsmokers was 93 ng/dl.
Despite the small number of men reporting use of various drugs, several medications were also associ-ated with levels of testosterone or HDL cholesterol (Table 3). Among whites, men who reported using
/3-blockers had lower mean levels of HDL cholesterol (-8 mg/dl) and testosterone (-130 ng/dl) than other men. The two men who reported using anabolic ste-roids had HDL cholesterol levels of 16 mg/dl and 20 mg/dl. In contrast, hydantoin users had higher levels of HDL cholesterol: whites, 6 mg/dl; blacks, 16 mg/dl.
We then examined the magnitude of the associa-tion between levels of HDL cholesterol and testoster-one after controlling for several characteristics by stratification and partial correlations (Table 4). Ad-justment for most characteristics, however, had little influence on the strength of the association. Among white men, for example, correlations within each age group were identical to the unadjusted association (r=0.22) between testosterone and HDL cholesterol levels. The association between levels of HDL cho-lesterol and testosterone, however, increased slightly after controlling for cigarette smoking, with correla-tion coefficients of 0.27 among both white and black men. The largest effect, however, was seen after controlling for Quetelet index: partial correlation coefficients were reduced to 0.13 (whites) and 0.15 (blacks). Similar results were seen in the stratum-specific analyses, with a correlation coefficient of only 0.09 among white men who had a Quetelet index below 24.5 kg/m2.
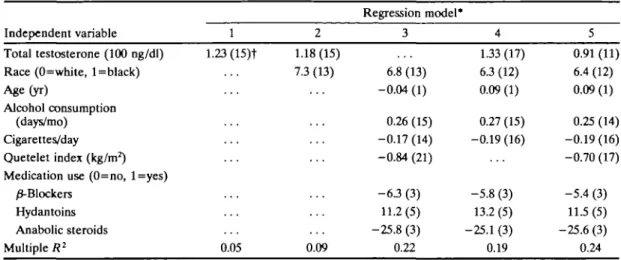
Coefficients from several regression models exam-ining the cross-sectional association between levels of HDL cholesterol and several characteristics are shown in Table 5. Before adjustment for any covariate (mod-el 1), a 100 ng/dl increase in testosterone was associ-ated with a 1.2 mg/dl increase in levels of HDL
TABLE 3. Mean Levels of High Density Lipoprotein Cholesterol and Testosterone by Categories of Selected Characteristics: Vietnam Experience Study, 1985-1986 Characteristic Military service in Vietnam No Yes Quetelet index (kg/m2) S24-5 24.6-28.0 >28 Cigarettes/day 0 1-20 >20 Alcohol consumption (days/mo) 0 1-8 > 8 0-Blockers No Yes Hydantoins No Yes Anabolic steroids No Yes n 1,568 1,994 1,126 1,258 1,178 1,990 723 849 884 1375 1,297 3,536 26 3,546 16 3,560 2 Whites H D L cholesterol (mg/dl) 44 44 49t 44 39 45t 43 41 41t 43 47 44t 36 44 50 44t 18 Testosterone (ng/dl) 676 675 764t 681 585 623t 742 743 648f 670 700 677* 547 676 672 676 644 n 231 269 164 165 171 234 224 40 109 175 212 497 3 494 6 500 0 Blacks HDL cholesterol (mg/dl) 51 52 58t 51 46 51 52 50 46t 52 54 52 52 51t 77 Testosterone (ng/dl) 710 709 820t 708 604 671 743 764 685 693 739 710 632 708 821
•All values have been age adjusted.
p values were assessed by a test for a linear trend (polychotomous variables) or a test for difference in means or medians: tp< 0.001, lp<0.01.
cholesterol, and adjustment for race (model 2) did not alter this association. (Results of model 2 also indicate that the higher mean HDL cholesterol level among blacks exists independently of differences in levels of testosterone.) The association between several cova-riates and levels of HDL cholesterol is shown in model 3: HDL cholesterol was associated positively with use of alcohol and hydantoins and inversely with cigarette smoking, Quetelet index, and use of ^-blockers or anabolic steroids. Controlling for most covariates slightly increased the magnitude of the association between levels of testosterone and HDL cholesterol (model 4). Further adjustment for Quetelet index (model 5), however, indicated that an increase of 100 ng/dl in levels of testosterone was associated with an increase of 0.91 mg/dl in levels of HDL cholesterol, about 30% less than that predicted in model 4.
Discussion
Results of prospective studies30-32 have shown that baseline levels of testosterone and estrogen are not strongly predictive of subsequent CHD, and it has been suggested that the associations between levels
of sex hormones and risk factors be studied further. In agreement with the results of previous studies,12"17 our cross-sectional findings indicate that levels of total testosterone and HDL cholesterol are positively associated (r=0.22 to 0.26). Furthermore, we ob-served that mean levels of HDL cholesterol and testosterone were higher among black men than among whites and that both were related similarly to obesity (inversely) and alcohol consumption (posi-tively). We found different relations, however, with age and cigarette smoking. Age was inversely associ-ated with testosterone levels (estimassoci-ated yearly dec-rements of 15 ng/dl for whites and 25 ng/dl for blacks) but not with levels of HDL cholesterol. Cigarette smokers had lower mean levels of HDL cholesterol but higher levels of testosterone than did nonsmokers. Analyses indicated that the positive association between levels of HDL cholesterol and testosterone was, at least in part, due to their inverse associations with obesity.
Levels of total testosterone were measured in the current study, and only a small proportion of total testosterone exists unbound to protein, with most
TABLE 4. Association Between Levels of Testosterone and High Density Upoproteln Cholesterol, Controlling for Various Charac-teristics: Vietnam Experience Study, 1985-1986
Pearson correlation coefficients Whites (n=3,562) Blacks (n= 500) Characteristic adjusted for Within strata Adjusted* Within strata Adjusted* Unadjusted Age (yr) 31-35 36-40 41-45 Cigarettes/day 0 1-20 >20 Alcohol consumption (days/mo) 0 1-8 >8 Quetelet index 0.22 0.26 0.22 0.27 0.26 0.27 0.17 0.20 0.23 • 0.20 0.21 0.28 0.27 0.25 <24.5 24.6-28.0 >28 0.13 0.16 0.16 0.16 0.15 'Value is partial correlation coefficient for the association between levels of testosterone and high density lipoprotein cho-lesterol, adjusted for individual characteristic.
fLevels of Quetelet index were divided into tertiles: sample sizes among whites range from 1,126 to 1,178; among blacks, from 164 to 171.
bound to SHBG. Although it is uncertain whether our findings would also apply to levels of free tes-tosterone, some evidence suggests that they would. Gutai et al13 reported 1) a strong correlation (r=0.76) between levels of free and total testosterone and 2) that levels of free and total testosterone followed the same pattern of association with levels of HDL cholesterol and other characteristics. Other investigators have also reported positive associations between levels of free testosterone and HDL choles-terol.1416 Lindstedt et al33 have suggested that some of the protein-bound testosterone may be biologically active.
Although we observed, as have others,12"17 a pos-itive association between levels of testosterone and HDL cholesterol, this relation is somewhat surprising since 1) men have a higher incidence of CHD than women and 2) HDL cholesterol levels decrease in boys during puberty and after administration of testosterone derivatives.6 Furthermore, there is a plausible biologic mechanism that may explain the inverse association, with decreased levels of HDL cholesterol resulting from a testosterone-stimulated increase in hepatic lipase activity.34 To reconcile these differences, it has been suggested1.11-14 that the positive association between levels of endogenous testosterone and HDL cholesterol is not direct but is
due to their joint association with another factor. Investigators have found that several indexes of obesity are inversely related to levels of both HDL cholesterol35 and testosterone,11141517 and we found that controlling for Quetelet index reduced the strength of the association between levels of tes-tosterone and HDL cholesterol by about 30%.
In agreement with these results, Dai et al15 ob-served that controlling for relative weight reduced the longitudinal association between changes in tes-tosterone and HDL cholesterol. SHBG may be in-volved in these joint associations with obesity, and an inverse association between levels of testosterone and HDL cholesterol has been reported after con-trolling for SHBG.36 An increased peripheral conver-sion of testosterone to estradiol in obese men may also be important.
Although we found a positive association between levels of testosterone and HDL cholesterol even after controlling for Quetelet index, this index is a very indirect measure of obesity.37 If adiposity was more accurately assessed (e.g., by measurement of skinfold thicknesses), the association between testosterone and HDL cholesterol may have been further re-duced. In addition, body fat distribution is correlated with levels of both HDL cholesterol and SHBG,38 and it may also play a role in the association between levels of testosterone and HDL cholesterol. Other mechanisms, however, may also be involved. For example, testosterone may lead to a generalized increase in microsomal enzyme activity, resulting in increased HDL production by the liver.15
Previous reports have shown that testosterone levels in middle-aged men are associated negatively with age and positively with cigarette smoking.17"19 Although we found similar associations, testosterone levels appear to decrease with age beginning with men in their early 30s, a younger age than is generally realized. The positive correlation that we observed between alcohol consumption and levels of testoster-one does not agree, however, with findings of a previous study18 and needs confirmation. To our knowledge, differences in testosterone levels be-tween black and white men have not been previously described: we found that mean levels were approxi-mately 5% higher among black men. This black/white difference, however, is 1) smaller than the correspond-ing 18% difference in mean levels of HDL cholesterol and 2) not constant across age groups. As observed by other investigators, only a small proportion of the variability in levels of testosterone can be accounted for by the examined characteristics, and other factors, such as physical activity and diet,39 may be important. The importance of testosterone levels in the etiol-ogy of CHD is uncertain. Although some case-control studies indicate that testosterone levels among myo-cardial infarction survivors do not differ significantly from levels among controls,10-40-41 there are several reports of lower testosterone levels among men with CHD17-42-43 and with arteriographically confirmed stenotic disease.44-46 Breier et al45 have suggested that
TABLE 5. Prediction of High Density Lipoprotein Cholesterol Levels in Various Linear Regression Models: Vietnam Experience Study, 1985-1986
Independent variable Total testosterone (100 ng/dl) Race (0=white, l=black) Age (yr)
Alcohol consumption (days/mo) Cigarettes/day Quetelet index (kg/m2) Medication use (0=no, l=yes)
^-Blockers Hydantoins Anabolic steroids Multiple R2 1 1.23 (15)t 0.05 2 1.18(15) 7.3 (13) 0.09 Regression model* 3 6.8 (13) -0.04 (1) 0.26 (15) -0.17 (14) -0.84 (21) -63 (3) 11.2(5) -25.8 (3) 0.22 4 133 (17) 63 (12) 0.09 (1) 0.27 (15) -0.19 (16) -5.8 (3) 13.2(5) -25.1 (3) 0.19 5 0.91 (11) 6.4 (12) 0.09 (1) 0.25 (14) -0.19(16) -0.70 (17) -5.4 (3) 11.5 (5) -25.6 (3) 0.24 •All analyses are restricted to the 4,051 men for whom values for all variables were available.
fValues are regression coefficient and, in parentheses, the absolute value of the t statistic; a t value of 2.6 is statistically significant at the 0.01 level; a value of 3.3 is statistically significant at the 0.001 level.
the decreased levels of HDL cholesterol among men with CHD may be secondary to the association be-tween testosterone and lipoprotein lipase activity. Interestingly, some results suggest that levels of total testosterone are as strongly associated with CHD as are levels of free testosterone.42-46
Because levels of sex hormones may be altered by a myocardial infarction, the results of prospective stud-ies may be more valid. Results of a nested case-control study, in which sex hormone levels were mea-sured in plasma samples obtained as many as 12 years before the clinical event, suggest that high levels of testosterone may be somewhat protective against CHD mortality.32 The results, however, were not statistically significant. Two other similarly designed studies30-31 provide no evidence that testosterone lev-els are related to CHD risk, but relatively few cases were studied. Deterioration of sex hormones during long-term storage of blood samples31 may reduce the magnitude of the association between levels of tes-tosterone and CHD in nested case-control studies.
Our results are based on men who entered the US Army between 1965 and 1971, and extrapolations to the general population should be made with caution. Furthermore, as a result of the multistep procedure leading to inclusion of men in the current analyses, which included tracing the veterans and obtaining their agreement to take part in both the telephone interview and medical examination, final participa-tion rates ranged from 53% (non-Vietnam veterans) to 66% (Vietnam veterans). Several of the findings, however, suggest that the observed associations may be generalizable. Mean levels of testosterone among men in our study were comparable with those previ-ously reported among similarly aged men18-32 and slightly higher than those reported among 45- to 59-year-old men.17 Other findings in this study, such as differences between black and white men in levels of HDL cholesterol and the relation of HDL
choles-terol levels to relative weight, cigarette smoking, and alcohol consumption, also agree with the results of other investigations.35
Although a previously reported cross-sectional as-sociation between levels of testosterone and CHD was reduced after controlling for levels of triglycer-ides,17 others have found that the association is independent of HDL cholesterol levels.46 Our find-ings concerning the interrelations among levels of testosterone, HDL cholesterol, cigarette smoking, and obesity emphasize the importance of multivari-able analyses in studies that examine the relation of testosterone levels to CHD.
Acknowledgments
We thank the leaders of veterans service organiza-tions who provided important input and support for the study and the veterans whose cooperation made this study possible.
References
1. Godsland IF, Wynn V, Crook D, Miller NE: Sex, plasma lipoproteins, and atherosclerosis: Prevailing assumptions and outstanding questions. Am Heart J 1987;114:1467-1503 2. Nikkila EA, Tikkanen MJ, Kuusi T: Gonadal hormones,
lipoprotein metabolism, and coronary heart disease, in Oliver MF, Vedin A, Wilhelmsson C (eds): Myocardial Infarction in Women. Edinburgh, Churchill Livingstone, 1986, pp 34-43 3. Hazzard WR: Atherogenesis: Why women live longer than
men. Geriatrics 1985;40:42-52
4. The Lipid Research Clinics Population Study Data Booh Volume 1. The Prevalence Study. Bethesda, Md, National Institutes of Health, 1980, DHHS publication No. (NIH) 80-1527 5. Berenson GS, Srinivasan SR, Cresanta JL, Foster TA, Webber
LS: Dynamic changes of serum lipoproteins in children during adolescence and sexual maturation. Am J Epidemiol 1981;113: 157-170
6. Kirkland RT, Keenan BS, Probstfleld JL, Patsch W, Lin TL, Clayton GW, Insull W: Decrease in plasma high-density lipoprotein cholesterol levels at puberty in boys with delayed adolescence: Correlation with plasma testosterone levels. JAMA 1987;257:502-507
7. Taggart HM, Applebaum-Bowden D, Haffner SM, Warnick GR, Cheung MC, Albers JJ, Chestnut CH, Hazzard WR: Reduction in high-density lipoproteins by anabolic steroid (stanozolol) therapy for postmenopausal osteoporosis. Metab-olism 1982;31:1147-1152
8. Albers JJ, Wahl PW, Cabana VG, Hazzard WR, Hoover JJ: Quantitation of apolipoprotein A-I of human plasma high density lipoprotein. Metabolism 1976;25:633-644
9. Wahl P, Walden C, Knopp R, Hoover J, Wallace R, Heiss G, Rifkind B: Effect of estrogen/progestin potency on lipid/ lipoprotein cholesterol. N Engl J Med 1983;308:862-867 10. Phillips GB: Evidence for hyperoestrogensemia as a risk factor
for myocardial infarction in men. Lancet 1976;2:14-18 11. Stefanick ML, Williams PT, Kiauss RM, Terry RB, Vranizan
KM, Wood PD: Relationships of plasma estradiol, testoster-one, and sex hormone-binding globulin with lipoproteins, apolipoproteins, and high density lipoprotein subtractions in men. / Clin Endocrinol Metab 1987;64:723-729
12. Nord0y A, Aakvaag, Thelle D: Sex hormones and high density lipoproteins in healthy males. Atherosclerosis 1979;34:431-436 13. Gutai J, LaPorte R, Kuller L, Dai W, Falvo-Gerard L, Caggiula
A: Plasma testosterone, high density lipoprotein cholesterol and other lipoprotein fractions. Am J Cardiol 1981;48:897-902 14. Heller RF, Wheeler MJ, Micallef J, Miller NE, Lewis B:
Relationship of high density lipoprotein cholesterol with total and free testosterone and sex hormone binding globulin. Ada Endocrinol 1983;104:253-258
15. Dai WS, Gutai JP, Kuller LH, LaPorte RE, Falvo-Gerard L, Caggiula A: Relation between plasma high-density lipoprotein cholesterol and sex-hormone concentrations in men. Am J Cardiol 1984^3:1259-1263
16. Hamalainen E, Adlercreutz H, Ehnholm C, Puska P: Rela-tionships of serum lipoproteins and apoproteins to sex hor-mones and to the binding capacity of sex hormone binding globulin in healthy Finnish men. Metabolism 1986;35:535-541 17. Iichtenstein M, Yarnell JWG, Ehvood PC, Beswick AD,
Sweetnam PM, Marks V, Teale D, Riad-Fahmy D: Sex hormones, insulin, lipids, and prevalent ischemic heart dis-ease. Am J Epidemiol 1987;126:647-657
18. Dai WS, Kuller LH, LaPorte RE, Gutai JP, Falvo-Gerard L, Caggiula A: The epidemiology of plasma testosterone levels in middle-aged men. Am J Epidemiol 1981;114:804-816 19. Desrypere JP, Vermeulen A: Leydig cell function in normal
men: Effect of age, lifestyle, residence, diet, and activity. / Clin Endocrinol Metab 1984;59:955-962
20. Centers for Disease Control Vietnam Experience Study: Health status of Vietnam veterans: I. Psychosocial character-istics. JAMA 1988;259:2701-2707
21. Wallace RB, Hunninghake DB, Reiland S, Barrett-Connor E, Mackenthun A, Hoover J, Wahl P: Alterations of plasma high-density lipoprotein cholesterol levels associated with consump-tion of selected medicaconsump-tions: The Lipid Research Clinics Pro-gram Prevalence Study. Circulation 1980;62(suppl IV): IV-77-IV-82
22. Freedman DS, Strogatz DS, Eaker E, Joesoeph MR, DeSte-fano F: Differences between black and white men in correlates of HDL cholesterol. Am J Epidemiol 1990;132:656-669 23. Martin JV: Lipid abnormalities in workers exposed to dioxin.
BrJ Ind Med 1984;41:254-256
24. Moore RW, Potter CL, Theobald HM, Robinson JA, Peterson RE: Androgenic deficiency in male rats treated with 2,3,7,8-tetrachlorodibenzo-p-dioxin. Toxicol Appl Pharmacol 1985;79: 99-111
25. Faiman C, Winter JSD: Diurnal cycles in plasma FSH, tes-tosterone and cortisol in men. / Clin Endocrinol Metab 1971; 33:186-192
26. Centers for Disease Control Vietnam Experience Study: Health Status of Vietnam Veterans: Supplement A: Laboratory Methods and Quality Control Atlanta, Ga, Centers for Disease Control, 1989
27. Leeco Diagnostics: Testosterone Diagnostic Kit Test Protocol Southfield, Mich, Leeco Diagnostics, 1983
28. Tukey JW: Exploratory Data Analysis. Reading, Mass, Addi-son-Wesley Publishing Co, 1977, pp 205-236
29. Neter J, Wasserman W, Kutner MH: Applied Linear Statistical Models, ed 2. Homewood, 111, Richard D. Irwin, Inc, 1985, pp 271-299
30. Cauley JA, Gutai JP, Kuller LH, Dai WS: Usefulness of sex steroid hormone levels in predicting coronary artery disease in men. Am J Cardiol 1987;60:771-777
31. Phillips GB, Yano K, Stemmermann GN: Serum sex hormones and myocardial infarction in the Honolulu Heart Program: Pitfalls in prospective studies on sex hormones. / Clin Epide-miol 1988;41:1151-1156
32. Barrett-Connor E, Khaw KT: Endogenous sex hormones and cardiovascular disease in men: A prospective population-based study. Circulation 1988;78:539-545
33. Lindstedt G, Lundberg PA, Hammond GL, Vihko R: Sex hormone-binding globulin: Still many questions. Scand J Clin Lab Invest 1985;45:l-6
34. Tikkanen MJ, Nikkila EA: Regulation of hepatic lipase and serum lipoproteins by sex steroids. Am Heart J 1987;13: 562-567
35. Heiss G, Johnson NJ, Reiland S, Davis CE, Tyroler HA: The epidemiology of plasma high-density lipoprotein cholesterol levels: The Lipid Research Clinics Program Prevalence Study: Summary. Circulation 1980;62<suppl IV):rV-116-IV-136 36. Semmens J, Rouse I, Beilin LJ, Masarei JRL: Relationship of
plasma HDL cholesterol to testosterone, estradiol, and sex-hormone-binding globulin levels in men and women. Metabo-lism 1983;32:428-432
37. Willet WD: Nutritional Epidemiology. New York, Oxford Uni-versity Press, 1990, pp 217-244
38. Kissebah AH, Evans DJ, Peiris A, Wilson CR: Endocrine characteristics in regional obesities: Role of sex steroids, in Vague J, Bjorntorp P, Guy-Grand B, RebufK-Scrive M, Vague P (eds): Metabolic Complications of Human Obesities. Amster-dam, Elsevier, 1985, pp 115-129
39. Gutin B, Alejandro D, Duni T, Segal K, Phillips GB: Levels of serum sex hormones and risk factors for coronary heart disease in exercise-trained men. Am J Med 1985;79:79-83 40. Heller RF, Jacobs HS, Vermeulen A, Deslypere JP:
Andro-gens, oestroAndro-gens, and coronary heart disease. Br Med J 1981; 282:438-439
41. Phillips GB, Castelli WP, Abbott RD, McNamara PM: Asso-ciation of hyperestrogenemia and coronary heart disease in the Framingham cohort. Am J Med 1983;74:863-869 42. Sewdarsen M, Jialal I, Vythilingum S, Desai R: Sex hormone
levels in young Indian patients with myocardial infarction. Arteriosclerosis 1986;6:418-421
43. Mendoza SG, Zerpa A, Carrasco H, Colmenares O, Rangel A, Gartside PS, Kashyap ML: Estradiol, testosterone, apolipo-proteins, lipoprotein cholesterol and lipolytic enzymes in men with premature infarction and angiographically assessed cor-onary occlusion. Artery 1983;12:l-23
44. Barth JD, Jansen H, Hugenholtz PG, Birkenhager JC: Post-heparin lipases, lipids and related hormones in men undergo-ing coronary arteriography to assess atherosclerosis. Athero-sclerosis 1983;48:235-241
45. Breier C, Muhlberger V, Drexel H, Herald M, Lisch HJ, Knapp E, Braunsteiner H: Essential role of post-heparin lipoprotein lipase activity and of plasma testosterone in coro-nary artery disease. Lancet 1985;1:1242-1244
46. Chute CG, Baron JA, Kiel DP, Plymate SR, Pavia AT, Lozner EC, O'Keefe T, MacDonald GJ: Sex hormones and coronary artery disease. Am J Med 1987;83:853-859
KEY WORDS • high density lipoprotein cholesterol • testosterone • blacks