J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5575
CAN MOTHERS CARE FOR ACUTE DIARRHOEAL DISEASE OF THEIR
UNDER FIVE CHILDREN EFFECTIVELY AT HOME? A CROSS
SECTIONAL STUDY IN SLUM COMMUNITY IN BANKURA
Eashin Gazi1, Aniket Chowdhury2, Rakesh Kumar3, Aditya Prasad Sarkar4, Subhra Samujjwal
Basu5, Sanjay Saha6
HOW TO CITE THIS ARTICLE:
Eashin Gazi, Aniket Chowdhury, Rakesh Kumar, Aditya Prasad Sarkar, Subhra Samujjwal Basu, Sanjay Saha. “Can Mothers Care for Acute Diarrhoeal Disease of their Under Five Children Effectively at Home? A Cross Sectional Study in Slum Community in Ankura”. Journal of Evidence based Medicine and Healthcare; Volume 2, Issue 36, September 07, 2015; Page: 5575-5584, DOI: 10.18410/jebmh/2015/772
ABSTRACT: BACKGROUND: Diarrhea is one of the major causes of morbidity and mortality in under- five children in developing world like India. WHO & Integrated Management of Neonatal and Childhood Illness (IMNCI) diarrheal management guidelines encourage mothers and caretakers to treat diarrhoea at home by giving ORS and oral rehydration therapy (ORT) to reduce the duration, severity, hospitalization, overall medical costs and death. OBJECTIVES: i) to assess the Knowledge, Attitude and Practice (KAP) of mothers on home care of acute diarrhoeal diseases and ii) To find out the factors affecting it, if any. MATERIALS AND METHODS: Community based cross-sectional study was conducted for three months duration among 76 mothers of slum-dwelling under five children (2-59 months) in Bankura. Information about KAP on management of acute diarrhoeal diseases was obtained by interview of mother using schedule based on WHO & IMNCI diarrheal management guidelines. RESULTS: In this study, majority mothers (64.7%) of children were of BPL category and mean schooling years of mothers was 7.97±4.12. Majority of mothers’ knowledge was average (66.2%) and favourable attitude was (76.5%). While 72.2% mothers performed average practice; only 9.3% of mothers performed good practice. Education, occupation and socio-economic status (SES) were the influencing factors of KAP on home care of diarrhea. Conclusions: A lot of gap was still present in knowledge, attitude and practice of home management of acute diarrheal diseases in an urban slum of Bankura. Health providers are needed to be skilled, motivated to percolate the information to mothers regarding home care of diarrhea.
KEYWORDS: Acute diarrheal diseases (DDs), KAP, BCC, Home management.
INTRODUCTION: Diarrhea is one of the major cause of morbidity as well as mortality in under- five children.(1) It now causes about 11 per cent of child deaths worldwide. 90 per cent of these
deaths occur in sub-saharan Africa and South Asia. In India acute diarrhoeal disease accounts for about 8 per cent of deaths in under 5 year age group. During the year 2011, about 10.6 million cases were reported in India.(2) Contaminated food and water, inadequate sanitation,
overcrowded shelters, poor hygiene practices as well as malnutrition affect the spread and severity of diarrhea.(2) Young age, dehydration, lack of breast feeding, and poor nutritional status
are the major risk factors for death from diarrhea.(3) Most of the diarrheal episodes are self-
limited, dehydration being the primary reason of mortality.(1) The single most strategy as
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5576 therapy(ORT) with ORS solution.(4) It is inexpensive and easily admissible at home by the
mothers or caretakers. In 2004, The WHO & UNICEF jointly recommended the use of newly formulated low osmolarity ORS and Zinc supplementation in the treatment of childhood diarrhea. But the range of coverage of ORT varies between 2-16% in India.(5) The coverage of ORS of
under three years children is 26.2% according to NFHS-3. According to the IMNCI guidelines, children with no dehydration should be managed at home with ORS, home available fluids (HAF) & continue feeding including breast feeding. The early detection of diarrhea at home, early and optimal use of ORT, maintenance of proper, hygienic and safe feeding practices reduce the duration, severity, hospitalization, overall medical costs and death of under five children in diarrhea. In this context the present study was planned in the following objectives;
1. To assess the Knowledge, Attitude and Practice (KAP) of mothers on home care of acute diarrhoeal diseases in slum-dwelling under five children in Bankura.
2. To find out the factors, if any affecting the KAP of study population.
MATERIAL AND METHODS:
Study design, area, subject and duration: This community based cross-sectional study was carried out in an urban slum of Bankura municipality. The study was carried on the mothers of having at least one child aged 2-59 months and permanent resident of the area. Seriously ill mothers and mothers of child suffering from chronic diarrhea were excluded from the study. Total study duration was three months from Nov 2013 to January 2014.
Sampling: Multistage sampling was done. In First stage one urban slum (Patpur slum) was selected through simple random sampling (SRS) from the total slums of Bankura municipality. In second stage one ICDS centre was taken by SRS out of four ICDS centers of the selected slum (Ward no. 17). All mothers (76) of children (2-59months) of that ICDS centre were approached for participation in the study. However 68 mothers gave informed consent to participate in study.
Ethics: The approval for the study was taken from the Chairman of institution ethics committee of B.S. Medical College. The purpose of the study was explained adequately to mothers and their written informed consent was obtained.
Data collection methods: Data were collected on a pre-designed and pre-tested schedule by interview of eligible mothers through house to house visit. The schedule had two parts. In the first part, the socio- demographic characteristics were recorded. In the second part, the KAP about diarrhea and its home care were assessed using 21 questions based on WHO(6) and IMNCI
diarrhea management guidelines.
Data analysis: Eight questions were used for knowledge and practice assessment each. Every right answer was awarded one mark, and wrong answer zero. Based on quartile values of obtained score, mother scoring above 3rd quartile value (score=6 for knowledge & score=7 for
practice) was considered to have good knowledge and practice in their respective scale. Similarly mothers scored between 1st quartile (score=4 for both knowledge & practice) and third quartile
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5577 (score) was considered to have average & those having score below 1st quartile (score=4 for both
knowledge& practice) was considered poor knowledge/ practices. Five questions were used for assessment of attitude adopting a 4 point Likert scale with most favorable answer was given four marks and most unfavorable was given one. The outcome measure for attitude was dichotomized based on median value as favorable (with score >median=13) and unfavorable (with score ≤median=13). Data were codified and entered in MS excel spread sheet. Percentage, mean and SD were used present descriptive data. Association between socio-demographic factors and KAP of mothers was determined by chi-square/ Fisher’s exact test with 95% Confident level.
RESULTS: The study revealed that 63.2% mothers were Hindu. The mean age of mothers was 23.68 (±4.89) years, range from 18yrs to 42yrs. General, SC, and OBC category were of 57.4%, 39.7% & 2.9% mothers respectively. Mean schooling years of mothers and their husbands were respectively 7.97±4.12 and 6.54±3.775. Majority mothers (64.7%) were of BPL category and 54.4% mothers lived in joint family. Mean family size of the study population was 5.68±2.778, range from 3 to 13. Majority of mothers (57.4%) had single child. 94.1% mothers were housewife. Majority of husbands’ occupation belonged to either daily wage labourer (DWL) (30.8%) or driver (33.9%) in this study.
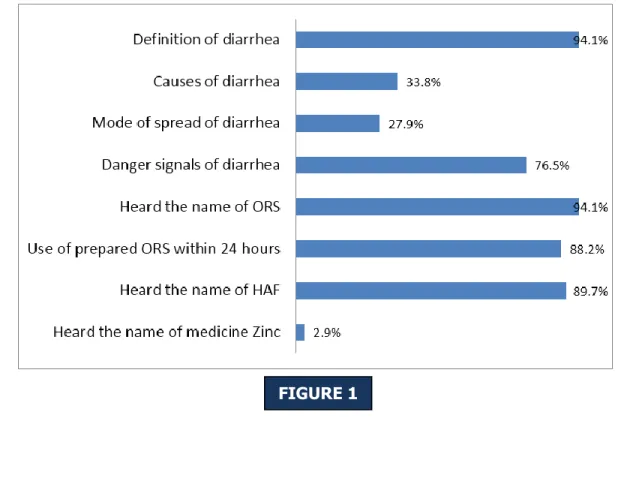
Figure 1: Distribution of study population according to their correct knowledge.
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5578
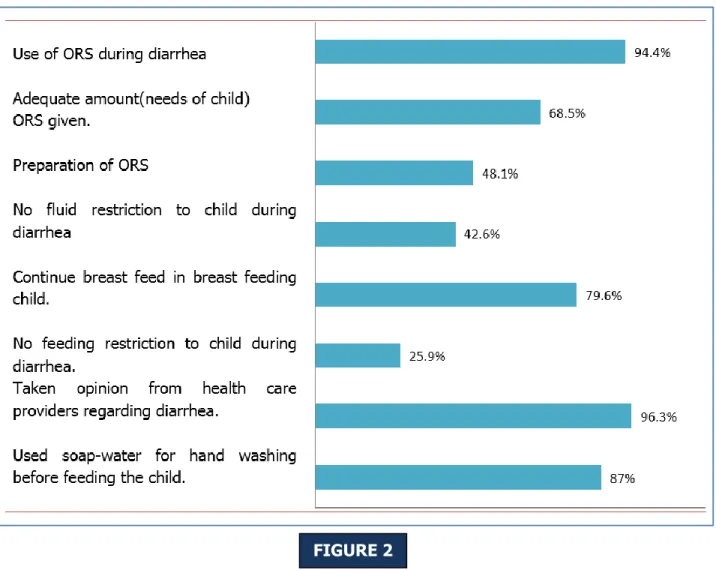
Figure 2: Distribution of study population according to their correct Practices.
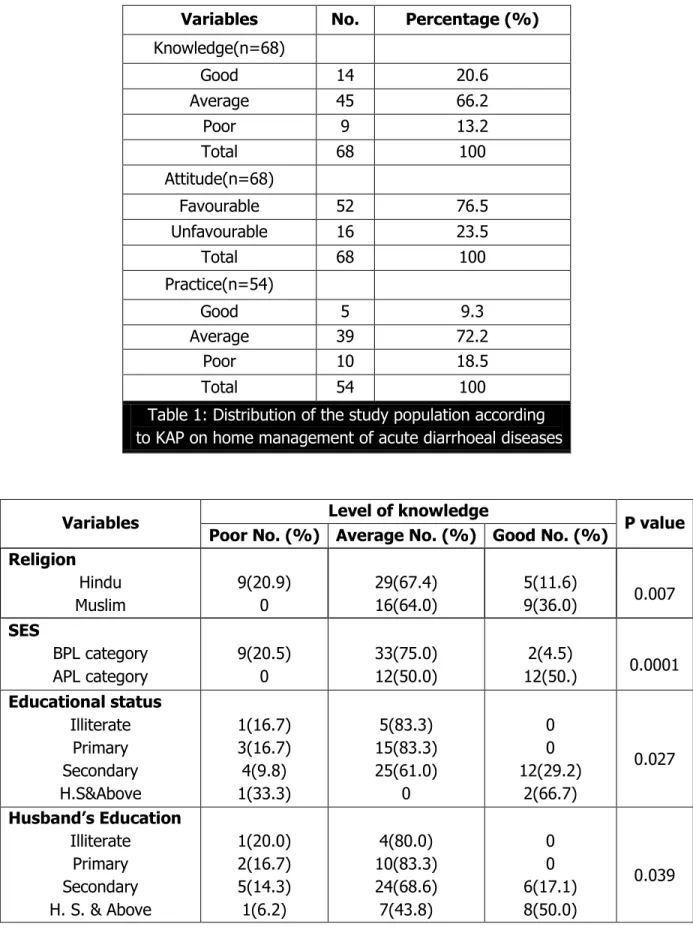
Mothers’ knowledge on home based management of diarrhoea was good in 20.6%average in 66.2% and poor in 13.2% of mothers [Table 1]. Knowledge was significant related with the religion, Socio-economic status (SES), educational status of mothers and their husbands, and husband’s occupation [Table 2]. The mothers’ knowledge was significantly (p <.05) higher in Islam religion, APL category, secondary or higher educational status of mothers and their husbands, and also the occupation of husband who were in services. Mothers’ attitude on home based management of diarrhoea was favourable in 76.5% [Table 1]. The attitude was significantly related with SES, educational status of mothers and also husband’s education & occupation [Table 3].
But 72.2% mothers performed average practice of diarrhoeal management at home; while 9.3% mother’s had good practice in this study [Table 1] 20.58% mothers had no experience to manage the diarrheal disease of their child at home. The practice had a relation with SES, educational status of mothers and their husbands, occupation of mothers [Table 4].
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5579
Variables No. Percentage (%)
Knowledge(n=68) Good 14 20.6 Average 45 66.2 Poor 9 13.2 Total 68 100 Attitude(n=68) Favourable 52 76.5 Unfavourable 16 23.5 Total 68 100 Practice(n=54) Good 5 9.3 Average 39 72.2 Poor 10 18.5 Total 54 100
Table 1: Distribution of the study population according to KAP on home management of acute diarrhoeal diseases
Variables Level of knowledge P value Poor No. (%) Average No. (%) Good No. (%)
Religion Hindu Muslim 9(20.9) 0 29(67.4) 16(64.0) 5(11.6) 9(36.0) 0.007 SES BPL category APL category 9(20.5) 0 33(75.0) 12(50.0) 2(4.5) 12(50.) 0.0001 Educational status Illiterate Primary Secondary H.S&Above 1(16.7) 3(16.7) 4(9.8) 1(33.3) 5(83.3) 15(83.3) 25(61.0) 0 0 0 12(29.2) 2(66.7) 0.027 Husband’s Education Illiterate Primary Secondary H. S. & Above 1(20.0) 2(16.7) 5(14.3) 1(6.2) 4(80.0) 10(83.3) 24(68.6) 7(43.8) 0 0 6(17.1) 8(50.0) 0.039
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5580 Husband’s Occupation Service Business Driver DWL 0 2(18.2) 1(4.3) 6(28.6) 3(23.1) 7(63.6) 20(87.0) 15(71.4) 10(76.9) 2(18.2) 2(8.7) 0 0.000
Table 2: Distribution of the mothers according to socio-demographic factors and the knowledge on diarrhoeal management (n=68)
Variables Level of Attitude
Unfavorable No. (%) Favorable
No. (%) P value SES BPL category APL category 15(34.1) 1(4.2) 29(65.9) 23(95.8) 0.006 Educational status Illiterate Primary Secondary H.S&Above 2(33.3) 9(50.0) 5(12.2) 0 4(66.7) 9(50.0) 36(87.8) 3(100.0) 0.011 Husband’s Education Illiterate Primary Secondary H.S&Above 1(20.0) 9(75.0) 4(11.4) 2(12.5) 4(80.0) 3(25.0) 31(88.6) 14(87.5) 0.000 Husband’s Occupation Service Business Driver DWL 0 1(9.1) 5(21.7) 10(47.6) 13(100.0) 10(90.9) 18(78.3) 11(52.4) 0.007
Table 3: Distribution of the mothers according to socio-demographic factors and the attitude on diarrhoeal management (n=68)
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5581
Variables Level of Practice P value Poor No. (%) Average No. (%) Good No. (%)
SES BPL category APL category 10(29.4) 0 23(67.6) 16(80.0) 1(2.9) 4(20.0) 0.006 Educational status Illiterate Primary Secondary H. S & Above 2(33.3) 7(43.8) 1(3.4) 0 4(66.7) 9(56.2) 24(82.8) 2(66.7) 0 0 4(13.8) 1(33.3) 0.014 Husband Education Illiterate Primary Secondary H. S & Above 1(20.0) 6(54.5) 3(10.7) 0 4(80.0) 5(45.5) 22(78.6) 8(80.0) 0 0 3(10.7) 2(20.0) 0.023 Occupation Housewife Service Others 9(18.0) 0 1(33.3) 37(74.0) 0 2(66.7) 4(8.0) 1(100.0) 0 0.032 Table 4: Distribution of the mothers according to socio-demographic
factors and the practices on diarrhoeal management (n= 54)
DISCUSSION: Knowledge of mother about meaning of diarrhea was almost 90% in this study. Around one third mothers in present study as well as in a Nigerian study were aware of contaminated food and water causes of diarrhea.(7) While 30% mothers knew the mode of spread
of diarrhea in current study while negligible proportion of them were aware about role of Zinc in treatment of diarrhea. ORS was known to almost all respondents in this study. In the study by Meenakshi M Dhadave et al. 65.7% of mothers were aware of ORS solution. Also another study conducted in West Bengal showed that 75% of mothers of under five children was aware of ORS.(8) Around 90% of mothers knew about others home available fluids (HAF) which was better
than that in a study in Nepal.(9) Around half of the mother could prepare ORS correctly, gave
others HAF and continued feeding to the underfives during diarrheal attack. In a study of West Bengal, 66.7% of mothers could prepare the ORS solution correctly.(8) The studies of Mirzapur
and Varanasi were found that 66.25% and 38.2% of mothers were continued feed their children during diarrheal episode as usual.(10,11) Another study in India reported that 88% of mothers
restricted their children’s diet during diarrhea.(12) Kolahi et.al found that during diarrhea only 10%
of mothers had increased amount of breast milk or food in their children’s diet.(13) About 80%
mothers had continued breast fed their during acute diarrheal diseases in present study. A study conducted in Chandigarh, was found that near about 90% of mothers preferred to continue breastfeeding.(14)
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5582 In this study, mothers’ knowledge on home management of diarrhea was good in 20.6% and poor in 13.2% [Table 1]. In a study of Iran was revealed that 28.8% and 24.7% of the mothers had good and low knowledge in diarrhea respectively.(15) Studies in Kenya and in Aligarh
were reported the same findings.(16, 17) Attitude was favourable in 75% mothers but only 9.3% of
mothers had performed good practice in present study.
The mothers’ knowledge was significantly (p<.05) higher in Islam religion, APL category, secondary or higher educational status of mothers and their husbands, and also the occupation of husband who were in services. No such significant relation was found with age of mothers, family type and no. of children. In a study in Iran, it was found that the knowledge of mothers had significant relation with mother’s age, education of husband, no. of children, occupation of mother and source of knowledge.(15) Mothers’ attitude were significantly related to SES of
mothers, educational status mothers and their husbands, and husband’s occupation also. Similarly practice of mothers on home care in diarrhea was significantly associated with SES of mothers, educational status mothers and their husbands, and mother’s occupation in this study. No relation was found with maternal age, family type and no. of children with regard to attitude and practice of mothers on home care of diarrhea.
CONCLUSION: There are gaps in knowledge, attitude and practice of mothers on home care of diarrhea among underfives. It is needed to be addressed through intervention of motivated and skilled peripheral health personnel. SES of mother, educational status and occupation are the associated factors of KAP of the mothers on home care of diarrhea
ACKNOWLEDGEMENT: The authors would like to thank the HOD, and faculty members of the Department of Community Medicine, B. S. Medical College, Bankura and all the participants of this study.
Author’s Contribution: Study concept and design: Eashin Gazi, Aditya Prasad Sarkar, Subhra Samujjwal Basu, Data Analysis and Interpretation: Aniket Chowdhury, Rakesh Kumar, Sanjay Saha. Drafting the Manuscript: Eashin Gazi, Rakesh Kumar, Aniket Chowdhury. Critical version of the manuscript important intellectual content: Aditya Prasad Sarkar, Subhra Samujjwal Basu.
REFERENCES:
1. Patel AB, Ovung R, Badhoniya NB, Dibley MJ. Risk factors for predicting diarrheal duration and morbidity in children with acute diarrhea. Indian J Pediatr. 2012; 79(4): 472-7.
2. Park K, Park’s Text Book of Preventive and Social Medicine, 22nd Edition, Jabalpur(India),
Banarsidas Bhanot 2013; 200-07.
3. O'Reilly CE, Jaron P, Ochieng B, Nyaguara A, Tate JE, Parsons MB, et al. Risk factors for death among children less than 5 years old hospitalized with diarrhea in rural western Kenya, 2005-2007: a cohort study. PLoS Med. 2012; 9(7): 1-13.
4. Mengistie B, Berhane Y, Worku A. Predictors of Oral Rehydration Therapy use among under-five children with diarrhea in Eastern Ethiopia: a community based case control study. BMC Public Health. 2012; 12(1): 1029.
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5583 5. Jones G, Schultink W, Babille M. Child survival in Indian. Indian journal of pediatricts. 2006;
73(6): 479-87.
6. The treatment of diarrhoea, A manual for physicians and other senior health workers, 4th
Revision, World Health Organization, Geneva, 2005.
7. Adimora GN, Ikefuna AN, Ilechukwu G. Home management of childhood diarrhoea: need to intensify campaign. Niger J Clin Pract. 2011; 14(2): 237-41.
8. Kaushik Chattopadhyay, Awareness of Oral Rehydration Salt (ORS) among Mothers of Under-Five Children in Kamala Village, West Bengal, India: A Cross-Sectional Study, Florida, USA, 2008.
9. Harmeet S R. et al. Mothers need to know more regarding management of childhood acute diarrhea. IJPSM 2003; 34(1&2): 40-45.
10.Mishra CP, Satish Kumar, Tiwari IC. A study on some diarrhea related practices in urban Mirzapur, Indian J Pub Hlth. 1990; 34: 6-10.
11.Kaur P, Singh G. Food practices during diarrhea. IJPH 1994; 38: 58-61.
12.Sood AK, Kapil U. Knowledge and practices among rural mothers in Haryana about childhood diarrhea. Indian J Pediatr. 1990; 57(4): 563-6.
13.Kolahi AA, Shekarriz R. Maternal knowlege and practice in toward oral rehydration therapy in acute diarrheal in less than five years old children in southern of Tehran. J Trop Infect Dis. 2008; 44 (14): 45-50.
14.Bhatia V, Swami HM, Bhatia M, Bhatia S.Attitudes and practices regarding diarrhea in rural community in Chandigarh. Indian J Pediatr 1999; 66: 499-503.
15.Ghasemi A. A, Talebian A, Alavi N M, Mousavi G A. Knowledge of Mothers in Management of Diarrhea in Under- Five Children, in Kashan, Iran. Nurs Midwifery Study.2013; 1(3): 158- 62.
16.Othero DM, Orago AS, Groenewegen T, Kaseje DO, Otengah PA. Home management of diarrhea among underfives in a rural community in Kenya: household perceptions and practices. East Afr J Public Health. 2008; 5(3): 142-6.
17.Shah MS, Ahmad A, Khalique N, Afzal S, Ansari MA, Khan Z. Homebased management of acute diarrhoeal disease in an urban slum of Aligarh, India. J Infect Dev Ctries. 2012; 6(2): 137-42.
J of Evidence Based Med &Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 36/Sept. 07, 2015 Page 5584
5. Assistant Professor, Department of Community Medicine, BSMC, Bankura. 6. Assistant Professor, Department of
Community Medicine, BSMC, Bankura.
NAME ADDRESS EMAIL ID OF THE CORRESPONDING AUTHOR:
Dr. Eashin Gazi,
NH-214, Chaitanya Health City,
Konaseema Institute of Medical Sciences & Research Foundation.
Amalapuram – 533201, A. P. E-mail: [email protected]
Date of Submission: 17/08/2015. Date of Peer Review: 18/08/2015. Date of Acceptance: 20/08/2015. Date of Publishing: 03/09/2015. AUTHORS: 1. Eashin Gazi 2. Aniket Chowdhury 3. Rakesh Kumar 4. Aditya Prasad Sarkar 5. Subhra Samujjwal Basu 6. Sanjay Saha
PARTICULARS OF CONTRIBUTORS:
1. Assistant Professor, Department of Community Medicine, KIMS & RF, Amalapuram.
2. Post Graduate Trainee, Department of Community Medicine, BSMC, Bankura. 3. Post Graduate Trainee, Department of
Community Medicine, BSMC, Bankura. 4. Associate Professor, Department of