ORIGINAL CONTRIBUTION
Effects of Interferon Beta-1b on Black Holes
in Multiple Sclerosis Over a 6-Year Period
With Monthly Evaluations
Francesca Bagnato, MD; Shiva Gupta, BA; Nancy D. Richert, MD, PhD; Roger D. Stone, BS; Joan M. Ohayon, CRNP; Joseph A. Frank, MD; Henry F. McFarland, MD
Background:Chronic, hypointense black holes (BHs) are recognized as a sign of permanent damage in pa-tients with multiple sclerosis. Although the effects of in-terferon beta-1b in reducing the formation of new BHs are established, it is not clear whether the drug may re-duce BH duration after these lesions are formed. Objective:To analyze the effects of interferon beta-1b in reducing the duration of T1 BHs in patients with mul-tiple sclerosis.
Design:Patients were clinically assessed and imaged monthly over a 36-month natural history phase and 36-month therapy phase. Numbers of contrast-enhanced lesions and newly formed BHs were counted on each scan. Each BH was counted until it was no longer seen.
Setting: Outpatient service of the Neuroimmunology Branch at the National Institutes of Health, Bethesda, Md.
Patients: Six patients with relapsing-remitting mul-tiple sclerosis were included. One patient did not form any BHs during the therapy phase. Analyses were per-formed on the remaining 5 individuals.
Interventions:Interferon beta-1b at the dosage of 8 mil-lion international units every other day.
Main Outcome Measures:Number and duration (in
months) of newly formed BHs.
Results:Rate of BH accumulation decreased with treat-ment (P=.01), but Kaplan-Meier models revealed that the duration of BHs did not shorten (2
1= 2.47,P= .12). Conclusions:Interferon beta-1b reduces the frequency of new BH formation but does not appear to decrease their duration in time. Analyses with larger patient cohorts are needed to confirm these preliminary findings.
Arch Neurol . 2005;62:1684-1688
I
NTERFERON BETA (IFN)RE-duces formation of contrast-enhanced lesions (CELs)1,2and T1 hypointense black holes (BHs) on magnetic resonance imaging (MRI)3,4in patients with multiple sclero-sis (MS).
Questions remain regarding the abil-ity of the drug to shorten the duration of
BHs after they have formed. This is clini-cally relevant because BHs of shorter du-ration are believed to be associated with the presence of transient edema, and chronic, persisting BHs reflect areas of ir-reversible axonal loss and permanent dam-age.5Hence, by shortening the duration of
BHs, the formation of permanent detri-ment lesions may be prevented, ulti-mately exerting a neuroprotective effect.
In a previous study, we observed that the life span of BHs did not change in a cohort of 12 patients imaged monthly for 18 months before therapy and 18 months during IFN-1b treatment.6Because (1) the findings were not significant (ie, P= .26), although a trend toward a posi-tive effect in shortening BH duration was seen to be operating by IFN-1b; (2) a small number of lesions was detected dur-ing the therapy phase; and (3) a rela-tively large proportion of censored ob-
ser-CME course available at
www.archneurol.com
For editorial comment
see page 1666
Author Affiliations:Neuroimmunology Branch, National Institute of Neurological Disorders and Stroke, (Dr Bagnato, Mr Gupta, Dr Richert, Mr Stone,
Ms Ohayon, and Dr McFarland) and Laboratory of Diagnostic Radiology and Research (Dr Frank), National Institutes of Health, Bethesda, Md; and New York Medical College, Valhalla (Mr Gupta).
vations was present during the short-term follow-up, further investigations were warranted.6
This study is an attempt to extend these preliminary findings in a cohort of patients with MS followed for a longer period. For 6 patients with relapsing-remitting (RR) MS, we analyzed MRIs obtained during the 36-month pe-riods immediately before and after the start of IFN-1b therapy. We describe the accumulation of newly formed BHs in individual patients during a longer natural his-tory phase (NHP) and therapy phase (TP). We also com-pare the duration of new BHs arising during the TP with those originating during the NHP.
METHODS
PATIENTS AND STUDY DESIGN
This retrospective study was approved by the intramural re-search board of the National Institute of Neurological Disor-ders and Stroke (Bethesda, Md) and performed at the National Institutes of Health (Bethesda). Each patient signed an in-formed consent. Six female patients with RRMS7were sequen-tially enrolled. We excluded patients who had previously re-ceived immunomodulatory or immunosuppressive drugs, except intravenous methylprednisolone at 1 g per day for 3 to 5 days or oral prednisone taper for a clinical relapse. Patients were clini-cally examined by rating disability using the Expanded Dis-ability Status Scale (EDSS)8and imaged monthly for 71 months (ie, 72 evaluations) without missing any clinical examination or MRI. Sustained change in the EDSS score was defined as any change of 1 or more for an EDSS score of 5.0 or lower or a change of 0.5 or more for an EDSS score of 5.5 or more confirmed on at least 2 examinations 3 months apart.9,10
MRI ACQUISITION AND EVALUATION
A total of 432 MRI scans were obtained. Standard precontrast and postcontrast MRIs (gadopentate dimeglumine, 0.1 mmoL per kilogram of body weight) were performed at 1.5 T (Gen-eral Electric Medical Systems, Milwaukee, Wis).11One of us (F.B.) recorded the numbers of CELs and BHs. This proce-dure was repeated 3 times for each patient until a coefficient of variation of less than 2% was reached. Black holes were de-fined as hypointense regions visible on nonenhanced T1-weighted images with corresponding hyperintensities on T2-weighted images, but without enhancements on postcontrast MRIs. Black holes already present at the first scan gave the num-ber of BHs at baseline, but only BHs originating from previ-ously identified CELs over the study course (ie, new BHs) were used for the subsequent statistical analyses performed in this article. Each new BH was tracked until it was no longer vis-ible. No BHs occurred without any evidence of visible CELs or separated by a gap after the cessation of the enhancement dur-ing the 36 months of observation.
New BH counts during the NHP and TP were performed separately. That is, lesions visible at the end of the NHP were no longer followed and therefore not tracked into the TP.
NEUTRALIZING ANTIBODIES
Neutralizing antibodies (NABs) were measured every 2 months for the first 24 months of therapy and yearly afterwards by the means of the Mixovirus-A protein inhibition assay from Ber-lex Laboratories (Montville, NJ).12Patients were considered to be NAB⫹when NAB titers of 1:20 or more were detected in at least 2 consecutive samples.
STATISTICAL ANALYSIS
For the first 2 types of statistical analyses described here, each patient’s data were considered separately because of heteroge-neity among patients. Accumulation of new BHs and compari-sons in the accumulations of new BHs over the NHP and TP were performed by a linear regression analysis. The correspond-ing slopes of these linear relations were evaluated to deter-mine whether the monthly numbers of new BHs increased over time within the NHP and TP. Further analysis of these slopes described whether the rate of accumulation of new BHs dur-ing the NHP was significantly higher than durdur-ing the TP. For these 2 analyses, natural logarithmic transformation of the month of the NHP or TP was applied to linearize the nonlinear re-gression relation between the month of the NHP or TP and the accumulation of BHs. The third analysis consisted of a Kaplan-Meier survival model and log rank test to detect a potential dif-ference between the duration (measured in months) of new BHs during the NHP vs the TP. For this analysis, data from all in-dividuals were combined. ReportedPvalues were based on 2-tailed statistical tests, with a significance level of .05. The sta-tistical analyses were performed using DataDesk (Data Descrip-tion Inc, Ithaca, NY) version 6.0 (for Windows) for the slope analyses and StatView (SAS, Cary, NC) version 5.0 for sur-vival analyses and log rank tests.
RESULTS CLINICAL OUTCOME
At baseline, the age range was 32 to 42 years; the EDSS score range, 1.5 to 3.5; and the disease duration range, 1 to 9 years. The number of CELs ranged from 1 to 5, and the number of preexisting BHs ranged from 3 to 18.
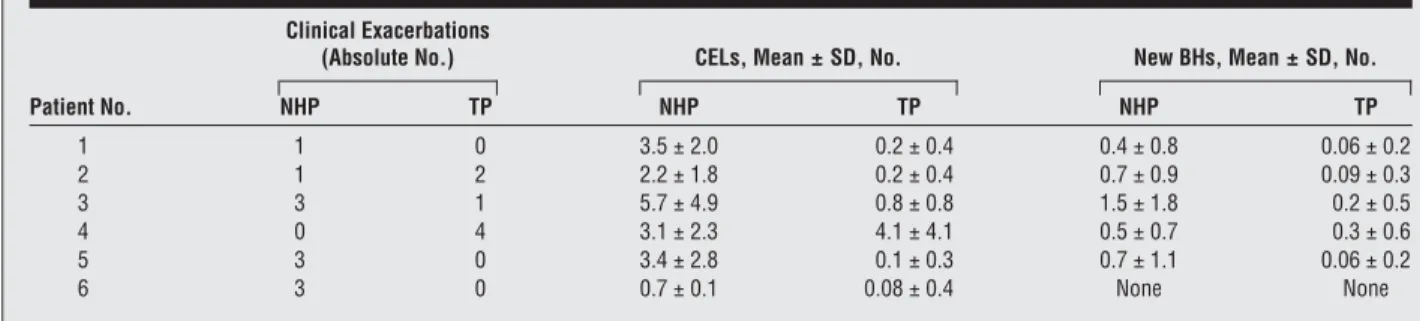
Over the study course, 1 patient (patient 3) had a sus-tained change in EDSS score during both the NHP (ie, from 3.0 to 6.0) and the TP (from 6.0 to 6.5). Two pa-tients showed increased EDSS scores exclusively over the TP. The EDSS score of patient 2 increased from 1.5 to 3.0, and patient 4 showed an increased EDSS score from 2.0 to 4.5. The EDSS scores of the remaining 3 patients (patients 1, 5, and 6) did not change. The number of clini-cal exacerbations and MRI outcomes of individual pa-tients during the NHP and TP of the study are reported inTable 1. One patient (patient 6) did not have any CELs or new BHs over the TP and was excluded from the sta-tistical analyses reported here.
IFN-1b EFFECT IN FORMATION
AND PERSISTENCE OF NEW BHS
The number of accumulating new BHs and natural loga-rithm of the month were linearly related (Pⱕ.001) for each individual within the NHP (R2range, 58.4%-85.3%) and TP (R2range, 35.7%-86.1%). Specifically, the number of new BHs increased (Pⱕ.001) for each indi-vidual within the NHP and TP. However, for each pa-tient, the rate of accumulation of new BHs during the TP was significantly lower than during the NHP (Table 2, Figure 1).
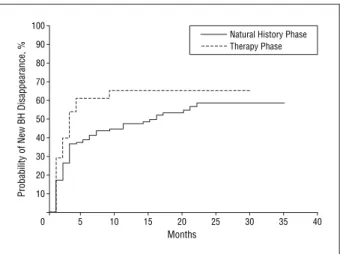
A total of 156 new BHs were identified during the NHP and 31 during the TP; 49.7% of the NHP observations and 38.9% of the TP observations were censored. That
is, a large percentage of the BHs during the NHP and TP persisted to the end of the observation periods, and thus, these BHs were assumed to last to the end of the obser-vation phases. Kaplan-Meier analysis revealed that the duration of new BHs arising during the TP was not shorter than the duration of BHs arising during the NHP (2
1=2.47, P= .12;Figure 2).
NAB OCCURRENCE
Two patients developed NABs during therapy. Patient 3 had transient low titers (eg,⬍1:100) at month 20 of therapy. Patient 4 had a sustained NAB seroconversion, beginning during the third month of therapy. Specifi-cally, titers increased up to 1:200 at month 9 of therapy, Table 1. Clinical Exacerbations and MRI Outcomes of Individual Patients During the NHP and TP
Patient No.
Clinical Exacerbations
(Absolute No.) CELs, Mean ± SD, No. New BHs, Mean ± SD, No.
NHP TP NHP TP NHP TP 1 1 0 3.5 ± 2.0 0.2 ± 0.4 0.4 ± 0.8 0.06 ± 0.2 2 1 2 2.2 ± 1.8 0.2 ± 0.4 0.7 ± 0.9 0.09 ± 0.3 3 3 1 5.7 ± 4.9 0.8 ± 0.8 1.5 ± 1.8 0.2 ± 0.5 4 0 4 3.1 ± 2.3 4.1 ± 4.1 0.5 ± 0.7 0.3 ± 0.6 5 3 0 3.4 ± 2.8 0.1 ± 0.3 0.7 ± 1.1 0.06 ± 0.2 6 3 0 0.7 ± 0.1 0.08 ± 0.4 None None
Abbreviations: BHs, black holes; CELs, contrast-enhanced lesions; MRI, magnetic resonance imaging; NHP, natural history phase; TP, therapy phase.
Table 2. Accumulation of New BHs During the NHP and TP: Individual Comparisons Between Linearized Slopes of the NHP and TP
Patient No. NHP Slope, 1/[ln (mo)] TP Slope, 1/[ln (mo)] F1,66 PValue
1 3.12 0.39 63.9 ⱕ.001
2 5.42 0.33 171.3 ⱕ.001
3 11.61 0.90 10.4 ⱕ.005
4 2.36 0.82 7.4 ⱕ.01
5 7.71 0.92 107.1 ⱕ.001
Abbreviations: BHs, black holes; ln, natural logarithm; NHP, natural history phase; TP, therapy phase.
40 30 35 25 20 15 5 10 1 5 9 13 17 21 25 29 33 4 8 12 16 20 24 28 32 36 NHP, mo TP, mo
Lesions, No. (New BHs)
Case 1 Case 2 Case 3 Case 4 Case 5 0
peaked at 1:695 during month 16 of treatment, and gradu-ally returned below 1:100 at the beginning of the third year of therapy. The NABs did not completely disappear at the end of therapy for this patient.
COMMENT
The results of the present article are based on the evalu-ation of serial MRIs of 6 patients. The sample size is small, but the length of the longitudinal follow-up (ie, 72 months) represents a robust and valid data set for de-scribing the course of MS during both NHPs and TPs.
We demonstrate that new BHs may significantly accumulate over time even when IFN-1b is adminis-tered. However, repeated administration of the drug did significantly decrease the rate of BH formation, thus protecting the brain tissue from accumulating degenera-tive lesions. Except for patient 4, a dramatic decrease in the number of CELs was observed in each individual patient, and this might have accounted for the corre-sponding decrease in the formation of new BHs. In this regard, our findings are similar to those reported in previous studies, which were based on analyses of larger cohorts of patients but with shorter monthly time windows.3,4,13
Given the exceptional behavior seen here in patient 4, additional analyses were performed. The NABs occurred from the early months of therapy in this patient and persisted throughout the study period. Neu-tralizing antibody formation could account for the lack of decrease in CEL occurrence. However, of the total new CELs, a significant decrease in the proportion of CELs forming BHs was found when comparing NHP vs TP lesions (data not shown). One may hypothesize that NABs did not block the whole amount of IFN-1b administered to this patient. Residual drug, if any is pre-sent, although unable to reduce the amount of inflam-matory activity, might have promoted the formation of less severe inflammatory lesions (as given by the ability of CELs to evolve into BHs) during the TP. The effect of IFNin promoting the formation of less aggressive CELs has been previously reported. Repeated adminis-tration of IFN reduced the proportion of CELs con-verting into BHs in patients with RRMS14(as for patient 4) but not in those with secondary progressive MS or mixed populations of patients with RRMS and secondary progressive MS.13,15 A possible explanation for these observations is that the immune factors that allow CELs to arise during the RR phase of MS are less aggressive and allow more prompt repair during the administration of IFNthan the CELs of patients with progressive dis-ease. However, care needs to be taken in the interpreta-tion of our results (reported on an individual case) with particular respect to the NAB findings. Additional appropriate investigations are warranted.
Amelioration of the disease course was further stud-ied to see if IFNcould shorten the life span of new BHs. This constituted the primary aim and novel aspect of our study. For this analysis, lesions (ie, BHs) were pooled across patients. Kaplan-Meier analysis showed that the duration of new BHs that arose during the NHP was not
shorter than those that arose during the TP. One can pos-tulate that although IFNmay reduce the frequency of BHs, after the lesion occurs, the drug is not changing the pathological process. However, the significance levels at which differences were detected are not straightforward. Heterogeneity in the number of new BHs for each patient as well as large proportions of censored observations during the study phases may potentially bias these re-sults. Consequently, we cannot distinguish between the possible ability of IFN-1b to promote either the forma-tion of less aggressive new BHs or faster recovery from them. Knowing this would be of great importance and would suggest the utility of introducing Kaplan-Meier approaches for lesion survival as additional tools for monitoring drug efficacy. This would allow one to prop-erly establish the role of IFN-1b (or any other neuro-protective drug of the central nervous system) for pa-tients with MS. Larger cohorts of papa-tients over longer periods are required to minimize potential bias because of the high heterogeneity of disease expression in indi-vidual cases.
Accepted for Publication:March 15, 2005.
Correspondence:Francesca Bagnato, MD,
Neuroimmu-nology Branch, National Institute of Neurological Dis-orders and Stroke, National Institutes of Health, Bldg 10, Room 5B16, 10 Center Dr, Bethesda, MD 20892-1400 ([email protected]).
Author Contributions:Study concept and design: Bag-nato, Gupta, Richert, Frank, and McFarland. Acquisi-tion of data:Richert, Stone, Ohayon, and Frank. Analy-sis and interpretation of data:Bagnato, Gupta, and Richert. Drafting of the manuscript:Bagnato, Gupta, and Frank. Critical revision of the manuscript for important intellec-tual content: Bagnato, Gupta, Richert, Stone, Ohayon, Frank, and McFarland.Statistical analysis:Bagnato and Gupta.Obtained funding:McFarland.Administrative, tech-nical, and material support:Stone and McFarland.Study
supervision:Frank and McFarland.
Acknowledgment:It is a pleasure to record our indebt-edness to all the patients.
100 80 90 70 60 50 40 30 20 10 0 5 10 15 20 25 30 35 40 Months
Probability of New BH Disappearance, %
Natural History Phase Therapy Phase
Figure 2.Kaplan-Meier analysis for probability of the disappearance of black holes (BHs) (ie, recovery to isointense lesions on T1-weighted images) during the natural history phase and therapy phase.
REFERENCES
1. Stone LA, Frank JA, Albert PS, et al. The effect of interferon-beta on blood-brain barrier disruptions demonstrated by contrast-enhanced magnetic resonance imaging in relapsing-remitting multiple sclerosis.Ann Neurol. 1995;37:611-619.
2. Miller DH, Molyneux PD, Barker GJ, et al. Effect of interferon-beta1b on mag-netic resonance imaging outcomes in secondary progressive multiple sclerosis: results of a European multicenter, randomized, double-blind, placebo-controlled trial. European Study Group on Interferon-beta1b in secondary pro-gressive multiple sclerosis.Ann Neurol. 1999;46:850-859.
3. Gasperini C, Pozzilli C, Bastianello S, et al. Interferon-beta-1a in relapsing-remitting multiple sclerosis: effect on hypointense lesion volume on T1 weighted images.J Neurol Neurosurg Psychiatry. 1999;67:579-584.
4. Barkhof F, van Waesberghe JH, Filippi M, et al. T1hypointense lesions in
sec-ondary progressive multiple sclerosis: effect of interferon beta-1b treatment.Brain. 2001;124:1396-1402.
5. Bitsch A, Kuhlmann T, Stadelmann C, Lassmann H, Lucchinetti C, Bruck W. A longitudinal MRI study of histopathologically defined hypointense multiple scle-rosis lesions.Ann Neurol. 2001;49:793-796.
6. Bagnato F, Jeffries N, Ohayon J, et al. A 36-month longitudinal study on the evalu-ation of the effect of interferon beta in the durevalu-ation of black holes in multiple sclerosis.Mult Scler. 2002;8(suppl 1):S3.
7. Poser CM, Paty DW, Scheinberg L, et al. New diagnostic criteria for multiple scle-rosis: guidelines for research protocols.Ann Neurol. 1983;13:227-231.
8. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded dis-ability status scale (EDSS).Neurology. 1983;33:1444-1452.
9. Li DK, Paty DW. Magnetic resonance imaging results of the PRISMS trial: a randomized, double blind, placebo-controlled study of interferon-beta1a in relapsing-remitting multiple sclerosis. Prevention of Relapses and Disability by Interferon-beta1a Subcutaneously in Multiple Sclerosis.Ann Neurol. 1999; 46:197-206.
10. Leary SM, Miller DH, Stevenson VL, Brex PA, Chard DT, Thompson AJ. Inter-feron beta-1a in primary progressive MS: an exploratory, randomized, con-trolled trial.Neurology. 2003;60:44-51.
11. Bagnato F, Jeffries N, Richert ND, et al. Evolution of T1 black holes in patients with multiple sclerosis imaged monthly for 4 years.Brain. 2003;126:1782-1789.
12. Pungor E Jr, Files JG, Gabe JD, et al. A novel bioassay for the determination of neutralizing antibodies to IFN-beta1b.J Interferon Cytokine Res. 1998;18:1025-1020.
13. Brex PA, Molyneux PD, Smiddy P, et al. The effect of IFNbeta-1b on the evolu-tion of enhancing lesions in secondary progressive MS.Neurology. 2001;57: 2185-2190.
14. Paolillo A, Bastianello S, Frontoni M, et al. Magnetic resonance imaging out-come of new enhancing lesions in relapsing-remitting multiple sclerosis pa-tients treated with interferon beta1a.J Neurol. 1999;246:443-448.
15. Bagnato F, Jeffries N, Richert ND, et al. Interferon beta therapy does not affect duration in time of Gd-enhancing lesions and black holes in relapsing remitting multiple sclerosis.Neurology. 2003;60(suppl 1):4-92.
Visit www.archneurol.com.
As an individual subscriber, you may elect to be con-tacted when a specific article is cited. Receive an e-mail alert when the article you are viewing is cited by any of the journals hosted by HighWire. You will be asked to enter the volume, issue, and page number of the article you wish to track. Your e-mail address will be shared with other journals in this feature; other journals’ privacy poli-cies may differ fromJAMA & Archives Journals. Sign up to receive an e-mail alert when articles on particular top-ics are published.