43
Int J Res Med. 2013; 2(4);43-47 e ISSN:2320-2742 p ISSN: 2320-2734Study of socio demographic factors influencing vaccination status of children in
dared industrial area of Jamnagar
Mithun M. Sanghvi
1*1
Assistant Professor, Department of Community Medicine, Shree M.P. Shah Medical College, Jamnagar (Gujarat).
INTRODUCTION
Immunization has been one of the most significant, cost-effective and stimulatory public health interventions. About one-quarter, or 25%, of under-5 mortality is due to vaccine-preventable diseases1. The World Health Organization (WHO) launched the Expanded Program on Immunization (EPI) in 1974 globally with focus on prevention of the six childhood vaccine-preventable diseases by the year 20002. Immunization Program in India was introduced in 1978 as Expanded Program of Immunization. This gained momentum in 1985 as Universal Immunization Program (UIP) and implemented in phased manner to cover all districts in the country by 1989-903. Further, a national socio-demographic goal was set up in National Population Policy (NPP) 2000 to achieve universal immunization of children against all vaccine-preventable diseases by 20104. decrease in the incidence of malaria in most parts of the In the last few years, urbanization is growing in India. Most of this growth is due to migration, industrialization and natural growth (through birth). With the rapid growth of big cities, an impending threat of outbreak of vaccine-preventable diseases always exists due to the high population density, continuous influx of a new pool of infective agents with the immigrating population and poor coverage with primary immunization in the urban slums. In
*Corresponding Author
Dr. Mithun M. Sanghavi (Assistant Professor) 201, Panchnath Apartment, Opp. Sardar Patel Boarding, Nr. Solarium, Nutan Nagar Society, Jamnagar-360001 (Gujarat-India)
Email: drmmsanghavi@rediffmail.com
order to control and eliminate the vaccine preventable diseases it is important to know the vaccination coverage and reasons for non-vaccination. Hence the present study was undertaken with aim of finding out vaccination coverage. Coverage data are traditionally considered as the best indicators of an immunization program's performance because they reflect the management of, access to, and utilization of services. This study is also done to find out various reasons responsible for the suboptimal coverage of vaccination. There are few population based studies on the factors associated with immunization coverage in industrial area from our country. The current study was undertaken with objective of seeking association of socio demographic factors and vaccination status of children. This study helps to understand the needs/problems to better manage the program at the local level.
MATERIALS AND METHODS
The community based cross sectional study was carried out in the Dared industrial area of Jamnagar district from May-2012 to July-2012. Total population of Dared area is around 10000 according to record available at PHC Aliabada for this year). All the children in the age group of 1 to 5 yrs were selected for this study. The proportion of under five children was about 9% of total population in Gujarat in 20115. The proportion of infants may be about 3% of total population2. So, the proportion of children between 01 to 05 yrs is about 6%. So there
ORIGINAL ARTICLE
ABSTRACT
BACKGROUND: Immunization has been one of the most significant, cost-effective and stimulatory public health interventions. The current study seeks to assess vaccination coverage and socio demographic factors affecting immunization status of children. This study helps to understand the needs/problems to better manage the program at
the local level. MATERIALS AND METHODS: A cross-sectional survey was conducted in Dared area of
Jamnagar district in May-2012 to July-2012. 20% of children between 01 yrs to 05 yrs were included in the study.
Data were collected by a predesigned, pre-tested, semi structured questionnaire by house to house visit.RESULTS:
The coverage level was 51.66% for complete vaccination. Migration (20.83%) and lack of knowledge regarding immunization (14.16%) were the most common reasons for incomplete vaccination. Low parental age, illiteracy of parents, lower socioeconomic class, home delivery, less antenatal visits etc. are significantly associated while gender and birth order of children was not significantly associated with vaccination coverage of children in the
study area. CONCLUSION: Observation from the present study points towards pressing the need to accelerate
efforts of more focused interventions towards the target group (i.e. illiterate parents, lower age of parents, lower socioeconomic class, home delivered mothers etc.) for improving the situation in the study area.
44
Int J Res Med. 2013; 2(4);43-47 e ISSN:2320-2742 p ISSN: 2320-2734 were around 600 children between 01 to 05 yrspresent in the study area. It was decided to take sample of 20% of children between 01 to 05 yrs. So the sample size was about 120. Data were collected by using a pretested semi structured questionnaire from guardians of children during house to house visit after their verbal consent. The selection of children had been done by simple random method. The method used for the determination of the vaccination status was ‘the vaccination card or the recall’. The primary respondent was the mother of the child; and in case of her absence, the father acted as the next respondent. In case of absence of both of them, an adult in the household who remained with the child for most of the time or had taken the child for immunization on at least one occasion was interviewed. The questionnaire seeks information regarding various socio-demographic factors about the vaccination status and reasons for incomplete vaccination of the children. Modified Prasad’s classification was used for socioeconomic class. The child was considered as ‘Completely vaccinated’ if he/ she had received one dose each of BCG and measles and three doses each of DPT and polio (excluding Polio 0 dose) by his/her first birthday. Those who had missed any one vaccine out of the six primary vaccines were described as ‘Incompletely vaccinated’. Statistical analysis was done by odds ratio and chi square test. A p-value of <0.05 was considered significant. Regression analysis was also performed with immunization status as the dependent variable and the risk factors as independent variables.
RESULTS
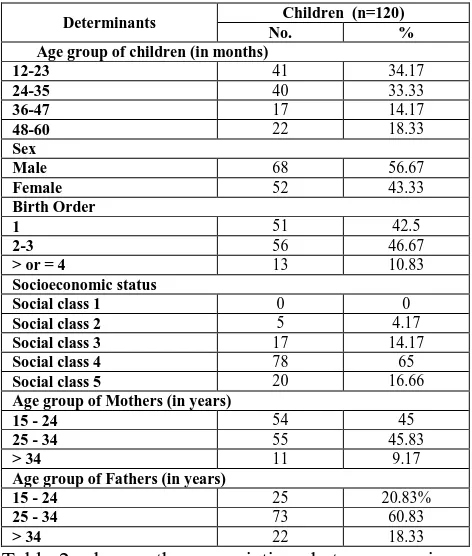
Total 120 children were included in the study. Some socio demographic characteristics of these children were depicted in Table-1. About 71.67% of mothers were illiterate, 21.67% educated up to primary level, 5% educated up to secondary level and 1.67% up to higher secondary level. Majority of mothers (68.33%) were house wife and rest of 31.66% engaged in labour work at industries. Majority of fathers (66.67%) were illiterate, 14.17% educated up to primary level, 16.67% educated up to secondary level and 2.5% up to higher secondary level. Most of fathers (94.16%) worked in industries while rest of engaged in agricultural work. Out of total surveyed children, vaccination card was seen among 41.66%. It is observed in the present study that 51.66% of children completed all the recommended vaccines and 48.33% received one or more vaccines, but did not complete all the recommended doses. 44.17% of mothers did not visit health facility for Antenatal care during pregnancy while 35.83% visited health facility one to three times during their pregnancy and 20% of mothers visited health facilities more than three
times during their pregnancy. Out of total studied children, 51.67% delivered in home and rest of delivered in hospitals (27.5% in Government hospitals and 20.83% in private hospitals). The common reasons for incomplete vaccination were: Migration (43.10%), lack of knowledge about immunization (29.31%); distance (13.79%), immunization has side-effects (5.17%) and other like OPV was thought to be the only vaccination, vaccination timing etc.
Table 1: Frequency of children between 01 to 05 yrs of age regarding Socio demographic characteristics
Determinants Children (n=120)
No. %
Age group of children (in months)
12-23 41 34.17
24-35 40 33.33
36-47 17 14.17
48-60 22 18.33
Sex
Male 68 56.67
Female 52 43.33
Birth Order
1 51 42.5
2-3 56 46.67
> or = 4 13 10.83
Socioeconomic status
Social class 1 0 0
Social class 2 5 4.17
Social class 3 17 14.17
Social class 4 78 65
Social class 5 20 16.66
Age group of Mothers (in years)
15 - 24 54 45
25 - 34 55 45.83
> 34 11 9.17
Age group of Fathers (in years)
15 - 24 25 20.83%
25 - 34 73 60.83
> 34 22 18.33
45
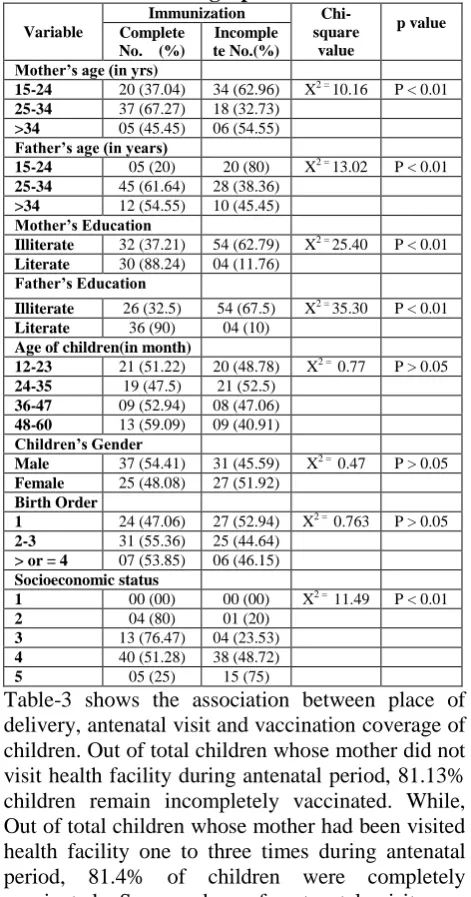
Int J Res Med. 2013; 2(4);43-47 e ISSN:2320-2742 p ISSN: 2320-2734 Table 2: Immunization status of children inrelation to socio demographic factors
Variable
Immunization
Chi-square value
p value Complete
No. (%)
Incomple te No.(%) Mother’s age (in yrs)
15-24 20 (37.04) 34 (62.96) X2 = 10.16 P < 0.01
25-34 37 (67.27) 18 (32.73)
>34 05 (45.45) 06 (54.55)
Father’s age (in years)
15-24 05 (20) 20 (80) X2 = 13.02 P < 0.01
25-34 45 (61.64) 28 (38.36)
>34 12 (54.55) 10 (45.45)
Mother’s Education
Illiterate 32 (37.21) 54 (62.79) X2 = 25.40 P < 0.01
Literate 30 (88.24) 04 (11.76)
Father’s Education
Illiterate 26 (32.5) 54 (67.5) X2 = 35.30 P < 0.01
Literate 36 (90) 04 (10)
Age of children(in month)
12-23 21 (51.22) 20 (48.78) X2 = 0.77 P > 0.05
24-35 19 (47.5) 21 (52.5)
36-47 09 (52.94) 08 (47.06)
48-60 13 (59.09) 09 (40.91)
Children’s Gender
Male 37 (54.41) 31 (45.59) X2 = 0.47 P > 0.05
Female 25 (48.08) 27 (51.92)
Birth Order
1 24 (47.06) 27 (52.94) X2 = 0.763 P > 0.05
2-3 31 (55.36) 25 (44.64)
> or = 4 07 (53.85) 06 (46.15)
Socioeconomic status
1 00 (00) 00 (00) X2 = 11.49 P < 0.01
2 04 (80) 01 (20)
3 13 (76.47) 04 (23.53)
4 40 (51.28) 38 (48.72)
5 05 (25) 15 (75)
Table-3 shows the association between place of delivery, antenatal visit and vaccination coverage of children. Out of total children whose mother did not visit health facility during antenatal period, 81.13% children remain incompletely vaccinated. While, Out of total children whose mother had been visited health facility one to three times during antenatal period, 81.4% of children were completely vaccinated. So, number of antenatal visit was significantly associated with vaccination coverage of children (p<0.01). Children born in a hospital were more likely to be completely vaccinated as compared to those born at home and this difference is statistically significant (X2=22.7, p<0.01).
Table 3: Association between place of delivery, antenatal visit and Immunization coverage of children.
Factors Immunization Odd
ratio Chi-square value
p value Complete
No. %
Incomplete No. %
Number of ANC Visit X2 = 1.58 P < 0.01
No 10(18.87) 43 (81.13) 1
1-3 35 (81.40) 08 (18.60) 18.81 P < 0.01 >3 17 (70.83) 07 (29.17) 10.44 P < 0.01
Place of Delivery X2 = 22.699 P < 0.01
Home 19 (30.65) 43 (69.35) 1 Govt.
Hospital
25 (75.76) 08 (24.24) 07.07 P < 0.01
Private Hospital
18 (72) 07 (28) 5.82 P < 0.01
DISCUSSION
46
Int J Res Med. 2013; 2(4);43-47 e ISSN:2320-2742 p ISSN: 2320-2734 incomplete vaccination of children in the presentstudy. Similar finding of the close association between parental educations has also been documented by other studies10,13,14,15. The present study revealed high odds ratio (OR=2.97) for complete vaccination for the children of mothers whose age is 25 yrs and more. This indicates the probability of children being vaccinated is high whose mother’s age is higher. Similar findings was observed by Harihar Sahoo15. Lower age of parents significantly associated with incomplete vaccination (p<0.01) suggesting that lower age of marriage and child bearing was associated with incomplete vaccination of children. In the present study lower socio economic status was significantly associated with incomplete vaccination of children. Similar findings were observed by Vilas R. Malkar et al in rural area of Beed district (Maharashtra) in 2010 and Madhuri Inamdar et al in school children of Indore district in 201116,17. They observed that higher proportion of children from the families belonging to upper socioeconomic class had significantly completed their immunization successfully and vice versa16,17. The difference is probably due to difference in attitude, education, awareness and affordability. Present study revealed that children born in a hospital were significantly more likely to be completely vaccinated as compared to those born at home. Similar finding was observed by other authors11,12,13,16. Present study also revealed that number of antenatal visit was significantly associated with vaccination coverage of children. 81.13% children remain incompletely vaccinated whose mother did not visit health facility during antenatal period. Similar observation seen in the study by H. Sahu who observed that the odds of immunizing the children are higher among those mothers who have gone through full antenatal care as compared to those mothers who have not gone for any antenatal care15. So, number of antenatal visit has a positive impact on child vaccination coverage.
CONCLUSION
The present study highlights that the vaccination status of children in industrial area is low and certain factors like low educational status of parents, lower age of parents, lower socioeconomic class, home delivery, less antenatal visit etc. are closely associated with it. Migration and lack of knowledge regarding vaccination were the most common reasons for incomplete vaccination. Recommendation: Observation from the present study points towards pressing the need to accelerate efforts of more focused information, education and communication activities towards the target group (like low age mother, illiterate mother, mother belong to lower SE class and mother who delivered
at home) in the study area for improving the situation. Various reasons for incompletely vaccinated children reflects the un-met needs of the community, which require organization of outreach services on fixed date and timing with prior information to the locality in the study area. Acknowledgement:
I
would like to acknowledge my sincere thanks to team of interns posted in the community medicine department during study period for their help in data collection.REFERENCES
1. Kalaivani K, Mathiyazhagan T, Patro BC. Editorial. News Lett Nat Inst Health and Family Welfare 2006;8:1-2.
2. Park K. Park’s Textbook of Preventive and Social Medicine. 22nd edition, Jabalpur, M/s Banarsidas Bhanot Publisher, 2013:114, 491. 3. Chapter V. Annual report. Ministry of Health
and Family Welfare: New Delhi; 2012-13. p. 66,68. Available from: http=1709&lid=1604. pdf. Accessed on Sep 03, 2013.
4. National Population policy 2000, Ministry of Health and Family Welfare. Government of India: New Delhi; 2000
5. Sample Registration system Statistical report 2011, Office of the Registrar General, India, Ministry of Home affairs, Government of India, New Delhi. Chapter 2: Population composition. 2013:14 Available from: http://www.Censusin dia.gov.in/vital_statistics/SRS_Report/9Chap% 202%20-%202011.pdf Accessed on Sep 04, 2013.
6. District Level Household and Facility Survey. Fact Sheet, Gujarat. Ministry of Health and Family Welfare, Govt. of India. International Institute for Population Science, Mumbai. 2007-08:88,89. Available on http://www.gujhealth .gov.in/ Portal/Tender/1/3_dlhs2.pdf Accessed on Sep 17, 2013.
7. The situation of children in India A profile. UNICEF, New Delhi; May 2011: 60.
8. S. Yadav, S. Mangal, N. Padhiyar et al. Evaluation of Immunization Coverage in Urban Slums of Jamnagar City. Indian J Community Med Oct-Dec 2006; 31(4): 300.
9. Nath B, Singh J V, Awasthi S, Bhushan V, Kumar V, Singh S K. A study on determinants of immunization coverage among 12-23 months old children in urban slums of Lucknow district, India. Indian J Med Sci 2007;61:598-606. 10. Dr. Varsha chaudhary, Dr. Rajeev Kumar, Dr.
47
Int J Res Med. 2013; 2(4);43-47 e ISSN:2320-2742 p ISSN: 2320-2734 11. Kulkarni SV, Chavan MK. A study to assess theimmunization coverage in an urban slum of Mumbai by lot quality technique. Int J Med Public Health 2013;3:21-5.
12. D Kumar, A Agrawal and S Gomber. Immunization Status of Children Admitted to a Tertiary-care Hospital of North India: Reasons for Partial Immunization or Non-immunization. J Health Popul Nutr. 2010 June; 28(3): 300– 304.
13. Chhabra P, Nair P, Gupta A, Sandhir M, Khnnan AT. Immunization in Urbanized villages of Delhi. Indian Journal of Paediatrics 2007; 74: 131-34.
14. Yadav R J, Singh P. Immunization status of children and mothers in the state of Madhya Pradesh. Indian Journal of Community Medicine 2004; 29(3):147-48.
15. Harihar Sahoo. Coverage of Child Immunization and Its Determinants in India. Social Change. Published by SAGE publication, Los Angeles, London, New Delhi, Singapore, Washington DC. 2012;42 (2):187-20.
16. Vilas R. Malkar, Hrishikesh Khadilakar, Rajesh N. Lakde, Umesh S. Joge, Sonali G. Chaudhari. Assessment of Socio demographic Factors Affecting Immunization Status of Children in Age Group of 12-23 Months in a Rural Area. Indian Medical Gazette May 2013; 164-69. 17. Madhuri Inamdar, Saurabh Piparsania, Savita