i Abstract
Background: Methamphetamine use disorder is a persistent and prevalent illness associated with serious physical, emotional, cognitive and social harms. No proven pharmacological treatments
have yet been identified and psychological therapies are currently the only evidence based
treatments. A recent systematic review and meta-analysis found no quantitative evidence of
benefit for psychostimulants in achieving abstinence or retention in treatment, but that review
was limited to specific pharmacological agents (Bhatt et al, 2016). An older systematic review
examined all treatments and found no single agent that demonstrated consistent efficacy
(Brackins et al, 2011). Many additional studies have since been published. The aim of this
systematic review is to critically evaluate the literature not previously covered by these and
examine the evidence for efficacy of all possible pharmacological treatments.
Methods: The literature search strategy consisted of an electronic search of PubMed. I included randomized controlled trials not previously reviewed of any pharmacological treatment for
methamphetamine use disorder that reported methamphetamine use by urine drug screen as an
outcome. I abstracted data from all identified studies using a standardized data collection
instrument and critically analyzed the risk of bias, internal validity and external validity of all
studies using a standardized form. I synthesized the review data.
Results: I identified and analyzed 11 studies not previously reviewed. Pharmacological treatments used in these studies included buprenorphine, N-acetyl-cysteine, aripiprazole,
citocoline, topiramate, naltrexone, mirtazapine, and a combined regimen of
flumazenil/gabapentin/hydroxyzine. No study was found to have both good internal and good
ii small study size and high numbers of drop outs. Comparison between studies was often not
possible due to inconsistently measured, defined and reported outcome measures.
Conclusions: Several studies reported positive results, but were limited by poor internal or external validity and no evidence was found to support treatment of methamphetamine use
disorder with a specific medication in the general outpatient population. There is a pressing need
for more research in this field. Future trials should use consistent outcome measures and address
possible challenges to statistical power caused by high attrition.
Bhatt M, Zielinski L, Baker-Beal L, et al. Efficacy and safety of psychostimulants for amphetamine and methamphetamine use disorders: a systematic review and meta-analysis.
Syst Rev. 2016;5(1):189. doi:10.1186/s13643-016-0370-x.
Brackins T, Brahm NC, Kissack JC. Treatments for methamphetamine abuse: a literature review for the clinician. J Pharm Pract. 2011;24(6):541-550.
Introduction
Methamphetamine use is a persistent and prevalent illness worldwide associated with serious
physical, emotional, cognitive and social harms. Taken together, methamphetamine and
amphetamine type stimulants have become the most popular psychostimulants in the world, with
24 million users worldwide.1Although the use of amphetamines other than methamphetamine is
on the rise, methamphetamine still accounted for 71% of all seizures of amphetamine type
stimulants in 2011.1 In the US in 2014, 1.6 million people used a stimulant drug for non-medical
purposes, 569,000 of whom were current methamphetamine users, representing 0.2% of the total
population. These numbers were similar to those from 2002-2013.2
Amphetamine was first synthesized from the Chinese herb Ma Huang in the early 19th century.1
Illegal methamphetamine recreational use first appeared in the United States in the 1930’s. 3
Methamphetamine and other related amphetamines were actually prescribed by physicians in the
US up until the 1960’s for weight loss and depression.4 An illegal powder form known variously
as “crank” or “meth” or “crystal” became available in the 1980’s when there was surge in
methamphetamine use in the US. Then, in 1988, a form of methamphetamine that could be
smoked known as “ice” or “glass” was identified first in Hawaii and then spread to the rest of the
US.5
Methamphetamine use is associated with many medical problems such as infectious disease
including HIV, cardiovascular and pulmonary disease, anxiety, depression, psychosis and
impaired cognition. It is also associated with an increased risk of mortality, primarily from HIV,
cardiovascular disease, or overdose.6 Amphetamine dependence has been calculated to account
2 The mainstay of treatment for methamphetamine abuse remains psychological treatments, which
have been supported by numerous trials and systematic reviews.8 All psychosocial treatments
have shown efficacy, with contingency management having the strongest evidence.9
An effective pharmacological treatment for methamphetamine abuse to complement physical
treatments could potentially play a major role in reducing the harms associated with the abuse.
The possibility of an effective pharmacological treatment has been suggested by advances in the
understanding of the neurochemical pathways associated with its use, as well as the experience
of effective pharmacological treatments for opioid and alcohol abuse.
While pharmacological treatment options are widely available for both opioid and alcohol abuse,
the general consensus among primary care physicians and those who specialize in addiction
treatment is that no pharmacological treatments have been shown to be effective treatments of
methamphetamine abuse in research of good quality.
Three basic approaches for a pharmacological treatment of methamphetamine use can be
postulated: (1) Agonist therapy, in which a medication replaces the effects of methamphetamine
as methadone does for opioid dependence; (2) Antagonist therapy, in which the medication
blocks the effects of methamphetamine in the same way naltrexone does for opioid dependence;
and (3) Symptomatic treatments that attempt to ameliorate the negative effects of use or
withdrawal.10
To my knowledge, 4 systematic reviews of treatments for methamphetamine abuse have been
published in addition to several non-systematic narrative reviews. The most recent and
well-conducted was a Cochrane review and meta-analysis published in November 2016 that updated a
3 psychostimulant, or agonist, treatments.11,12 Another systematic review published in 2004
similarly reviewed only agonist treatments for methamphetamine abuse.10 A systematic review
published by Shoptaw et all in 2009 examined only treatments for methamphetamine
withdrawal.13 Only one other systematic review published in 2011 reviewed all possible
pharmacological treatments for methamphetamine abuse.14 While agonist treatment is a
promising avenue for treatment of methamphetamine abuse, antagonist treatments and
symptomatic treatments may also be a useful addition to the pharmacological armamentarium.
The most recent systematic review and meta-analysis by Bhatt et al found no quantitative
evidence of benefit for psychostimulants in achieving abstinence or retention in treatment, but
this review was limited to specific pharmacological agents.11 An older systematic review by
Brackins et al examined all treatments and found no single agent that demonstrated consistent
efficacy.15 Many additional studies have been published since that comprehensive review in
2012, as evidenced by the updated findings in the meta-analysis of psychostimulant treatments.11
The aim of this systematic review is to critically evaluate the literature not previously covered by
these and examine the evidence for efficacy of all possible pharmacological treatments. The key
question for this review was:
What is the evidence in randomized placebo controlled trials for a pharmacological treatment of
methamphetamine use disorder in the general outpatient US population to reduce
4 Methods
Where applicable, I have reported the methods and results of this systematic review in
accordance with the PRISMA guidelines.16 I do not report on elements pertaining to a
meta-analysis. I did not register a study protocol. I formulated the search strategy and analysis
methods prior to beginning the process of study inclusion/exclusion and data extraction. In the
original design of the study a secondary objective and analysis method was to review preclinical
studies in addition to RCT’s and to correlate between the findings of preclinical studies and
clinical studies in order to guide future selection of candidate therapies. However, after initial
title and abstract review, due to the number of identified preclinical studies and time constraints,
I narrowed the scope of the study to clinical RCTs only.
Data Sources and Searches
To identify articles for review, I searched PubMed from inception to November 29, 2016. The
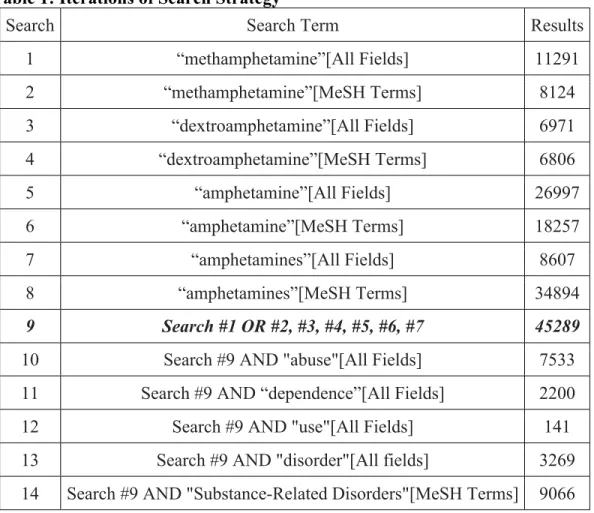
search was limited to studies of human subjects and English language articles. The various
iterations of the search strategy are outlined in Table 1.
The final formal algorithm for searching MEDLINE was (("methamphetamine"[MeSH Terms]
OR "methamphetamine"[All Fields]) OR ("dextroamphetamine"[MeSH Terms] OR
"dextroamphetamine"[All Fields] OR "amphetamines"[MeSH Terms] OR "amphetamines"[All
Fields] OR "amphetamine"[All Fields] OR "amphetamine"[MeSH Terms])) AND ("abuse"[All
Fields] OR "dependence"[All Fields] OR "use"[All Fields] OR "disorder"[All fields] OR
"Substance-Related Disorders"[MeSH Terms]) AND (("therapy"[Subheading] OR "therapy"[All
Fields] OR "treatment"[All Fields] OR "therapeutics"[MeSH Terms] OR "therapeutics"[All
Fields] OR "medication"[All Fields]) OR "amphetamine-related disorders/drug therapy"[MAJR])
5 Eligibility Criteria and Study Selection
I screened all titles and abstracts identified by the search and selected articles for further
eligibility review. In order to capture all relevant studies including preclinical studies, I selected
at screening all articles with titles or abstracts that reported results of a study examining the
effect of a pharmacological treatment in the setting of methamphetamine use. In cases where
there was doubt, I selected the article for review. I imported the citations of all selected articles
into Papers for Mac Version 3.3.1 and downloaded the full PDF of each article.
In the eligibility review I examined articles in their entirety and excluded articles from the main
analysis according to the algorithm presented in Figure 1. Exclusion criteria included previously
reviewed studies (specifically, studies included in the review by Brackins et al or the systematic
review of agonist treatment by Bhatt et al11,15), studies that included populations without
methamphetamine use (i.e. studies that included populations with cocaine use but not
methamphetamine use), studies that included participants younger than 18 years old, studies that
only examined the effects of behavioral therapies, non-randomized studies, un-controlled studies,
articles that were reports, commentaries, or re-analyses of other identified articles, or studies that
did not include reduction in methamphetamine use as an outcome measure. I also excluded
pre-clinical studies that examined cognitive, behavioral, or symptom effects after laboratory based
administration of medications. Because of the change in DSM criteria during the years of articles
reviewed, I included studies using any diagnostic criteria for methamphetamine abuse, use or
dependence. Because methamphetamine use disorder is often a comorbid disorder with other
drug and psychological conditions, I included studies irrespective of additional diagnoses. I
included studies of any duration. By design of the search strategy, I excluded non-English
6 Figure 1: Eligibility Criteria
Data Collection Process and Assessment of Risk of Bias
I abstracted data from each study using a data extraction chart in Microsoft Excel I adapted from
the reported methods of Castell et al in their systematic review of treatments for cocaine
dependence.17 I did not contact authors of articles to obtain missing data or confirm published
data. Data extracted from each study include:
• Study description and funding: study author, year, conflicts of interest, funding source Duplicate
Is the study intervention an agonist treatment?
Has this study been previously reviewed?
Is this a preclinical study?
Does this study report only on behavioral treatments?
Are there participants who don’t use amphetamines?
Does this study include participants younger than 18?
Does this study measure amphetamine use?
Is this a randomized controlled trial?
Is this original research?
Agonist treatment
Previously reviewed
Preclinical study
Wrong intervention
Wrong population
Wrong age
Wrong outcome
Non-RCT
Yes
Yes
Yes
Yes
Yes
Yes
No
No
7
• Methods: sequence generation, allocation concealment, blinding of
patients/clinicians/therapists/assessors, single or multiple site, study duration, number of
participants handling of dropouts, instruments used
• Participants: source population, inclusion criteria, exclusion criteria, sex, age, ethnicity,
employment status, frequency of methamphetamine use, years of methamphetamine use,
route, comorbid drug disorders, comorbid psychiatric disorders
• Intervention and control: drug, dose, control type, adherence, adjunct interventions
• Outcomes: methamphetamine use by urine drug screen (UDS), retention in treatment,
methamphetamine craving, self-reported use, number who finished study, reason for drop
outs, CGI score, psychotic symptoms, anxiety severity, depression severity, cocaine use
by UDS, opiate use by UDS, number dropped out due to adverse events, number who had
serious adverse events
For this review, the primary outcome measure of interest was reduction in methamphetamine use
as measured by urine drug screens. Secondary outcome measures of interest included retention in
treatment and methamphetamine craving.
I assessed the internal and external validity of each included study using a standard chart in
Microsoft Excel that included 9 items for internal validity, a single summary judgement of
internal validity and an overall judgement for external validity. I adapted the criteria for items
1-9 from a recent Cochrane review of treatment for cocaine which was itself based on the
recommendations in the Cochrane Handbook.17,18 I chose this method of analysis because of its
standardized form, previous use, and for ease of comparability with the systematic reviews of
8 criteria for the assessment of the risk of bias for items 1-9 are presented in Appendix A and are
taken from the Cochrane Handbook.18
I added to the assessment of risk of bias a summary item (number 10) on the overall internal
validity of each study rated as good, fair or poor. This was my own judgement based on the
likely magnitude and direction of the risks of bias identified in items 1-9. A judgement of poor
internal validity is meant to indicate that there is a high likelihood that the results have been
significantly affected by some form of bias to the point of altering the conclusion of the study. A
judgement of fair internal validity is meant to indicate that two or more significant sources of
bias were identified but that the likelihood of changing the conclusion of the study was small. A
judgement of good internal validity is meant to indicate that only one or no significant source of
bias was identified, and any bias was unlikely to change the conclusion of the study.
Finally, I included a single judgement of good, fair or poor on the external validity of the results
as applied to the general outpatient population in the USA who suffer from methamphetamine
use disorder. A judgement of poor external validity is meant to indicate that the results cannot be
applied. A judgement of fair external validity is meant to indicate that the results may be
applicable, but that there were significant differences in the source population compared to the
general population. A judgment of good external validity was given when the results were felt to
be directly applicable.
Data Synthesis and Analysis
Because of the expected heterogeneity of pharmacological treatments, I did not plan on
conducting any meta-analyses or computational combination of results identified. Instead, I
9 external validity of each study. I also looked for trends in the risks of bias in the identified
studies to help guide future research.
Results
Table 1: Iterations of Search Strategy
Search Search Term Results
1 “methamphetamine”[All Fields] 11291
2 “methamphetamine”[MeSH Terms] 8124
3 “dextroamphetamine”[All Fields] 6971
4 “dextroamphetamine”[MeSH Terms] 6806
5 “amphetamine”[All Fields] 26997
6 “amphetamine”[MeSH Terms] 18257
7 “amphetamines”[All Fields] 8607
8 “amphetamines”[MeSH Terms] 34894
9 Search #1 OR #2, #3, #4, #5, #6, #7 45289
10 Search #9 AND "abuse"[All Fields] 7533
11 Search #9 AND “dependence”[All Fields] 2200
12 Search #9 AND "use"[All Fields] 141
13 Search #9 AND "disorder"[All fields] 3269
14 Search #9 AND "Substance-Related Disorders"[MeSH Terms] 9066
10
Table 1, continued
15 Search #10 OR #11, #12, #13, #14 15014
16 Search #15 AND "therapy"[All Fields] 2879
17 Search #15 AND "therapy"[Subheading] 3377
18 Search #15 AND "treatment"[All Fields] 4503
19 Search #15 AND "therapeutics"[MeSH Terms] 2697
20 Search #15 AND “therapeutics”[All Fields] 145
21 Search #15 AND "medication"[All Fields] 820
22 Search #15 AND "amphetamine-related disorders/drug therapy"[MAJR] 127
23 Search #16 OR #17, #18, #19, #20, #21, #22 7915
24 Search #23 AND "humans"[MeSH Terms] 5749
25 Search #23 AND English[lang] 7430
26 Search #23 AND "adult"[MeSH Terms] 2963
27 Search #24 AND #25, #26 2765
Study Selection
Results of the various iterations of the PubMed search strategy are presented in Table 1. The
search included records from date of inception of PubMed to November 29, 2016. The last
search was performed on December 2, 2016. The process of record screening and eligibility
review is outlined in Figure 2. I identified a total of 2,765 records with the final search. I
screened the title and abstracts of each record and excluded 2,666. I downloaded the full text of
the remaining 99 articles and reviewed the eligibility of each for final inclusion in analysis. I
excluded 88 articles from the final analysis. Finally, 11 articles were included in the analysis.
References for all excluded articles and reason for exclusion can be found in the references
11 The majority of excluded articles were pre-clinical studies of the effects of various
pharmacological treatments on different aspects of methamphetamine use. Most of these studies
were conducted in controlled human laboratory settings. Broadly, these studies fell into one or
more of the following categories of investigation: attenuation of various effects of acute
amphetamine exposure, enhancement of neurocognitive processes in participants with chronic
methamphetamine exposure, changes in the choice of amphetamine dose under controlled
conditions, or safety and/or tolerability of proposed treatments. The different pharmacological
treatments found in these preclinical studies include naltrexone, modafinil, bupropion, diltiazem,
clonidine, isradipine, topiramate, rivastigmine, gamma-vinyl-gamma-amminobutyric acid,
aripiprazole, selegiline, perindopril, progesterone, risperidone, lithium, atomoxetine, varenicline,
valproate, and cytidine-5’-diphosphate choline.
Fourteen articles were studies included in the systematic review of agonist treatments by Bhatt et
al.11 Five articles were previously reviewed by Brackins et al.15 Four articles were either
republications of previously published studies or secondary analyses of previously published
studies. Three articles did not include reduction in methamphetamine use as an outcome
measure. Another three articles were conducted on inpatient populations. These articles were
focused on symptom reduction and also did not include reduction in methamphetamine use as an
outcome. One study reported on the decline in methamphetamine use in a population with
12 Figure 2: Flow diagram
Study characteristics
The eleven studies included in the analysis examined 8 different pharmacological treatments
among 802 participants. The characteristics of studies included in the final analysis are presented
in Table 2. Eight studies were published after 2011 when the previous systematic review by
Brackins et al was done.15 Interestingly, three studies were published before 2012 but were not
identified in that review. Most studies were conducted in the USA, although the most recent
studies were conducted in Iran and Malaysia. One study each was conducted in Russia and
Sweden. Study size was small in all trials, ranging from 31 to 140 participants.
Interventions included buprenorphine, citocoline, topiramate, mirtazapine, N-acetyl-cysteine
(NAC), naltrexone, aripiprazole, and a combination of flumazenil/gabapentin/hydroxyzine. One
study each used buprenorphine, citocoline, topiramate, and mirtazapine as interventions. One
study used N-acetyl-cysteine (NAC) by itself, while another used a combination of NAC and
Full Text Articles Excluded N = 88
Preclinical Study = 41 Not a RCT = 17 Agonist Treatment = 14 Previously Reviewed = 5
Duplicate = 4 Wrong outcome = 3
Wrong setting = 3 Wrong population = 1 Duplicates Removed
N = 0
Title and Abstracts Screened N = 2765
Full Text Articles Assessed for Eligibility
N = 99
Studies Included for Qualitative Synthesis
N = 11
Records Excluded After Initial Review
N = 2666 Records Identified Through
PubMed Search N = 2765
Records Identified Through Other Sources
N = 0
In
cl
ud
ed
Elig
ib
ili
ty
Sc
re
en
in
g
Id
en
tifi
ca
tio
13 naltrexone. Two studies used aripiprazole. Three studies used naltrexone: one in combination
with NAC, one as an oral pill, and another as an implant. All studies used inactive placebos for
controls, including one study with a placebo implant.
All 11 studies reported that methamphetamine use was measured using urine drug screens
(UDS), but two of the studies did not report the results of these measurements. Three studies did
not report study retention as an outcome measure, and did not provide enough data to calculate a
statistical comparison of numbers remaining in each arm at the end of the study. Two studies
reported that they measured scores for methamphetamine craving, but did not present the results.
14 Table 2: Characteristics and results of included studies
Author Yr Design N Dura-tion
Participants Intervention UDS Retention Craving Int Val Ext Val
Salehi et al 2015 RCT 40 16 weeks
All men referred to treatment center in Iran
Buprenorphine 6mg
NR Reported results by each visit.
Significant differences favoring intervention in visits 3-6 but no summary analysis done
NR Significant improvement Decreased score in intervention group p<0.001 ANCOVA
Poor Poor
Mousavi et al
2015 Placebo controlled crossover
32 8 weeks (two 4 week periods)
Treatment seeking patients referred to tertiary care in Iran
NAC 1200mg NR Stated as measured but not reported
NR Significant improvement Significant. improvement in intervention group p<0.001 ANOVA
Poor Poor
Sulaiman et al
2013 RCT 49 8 weeks All participants had been included in a 2-week open label trial of aripiprazole immediately prior to this study in Malaysia Aripiprazole 5-10mg No significant difference p=0.173 GEE Significant difference Better retention in intervention 48.7 vs 37.1 days p<0.05 Kaplan-Meier survival analysis Significant decrease BSCS score favoring intervention p=0.015 MMRM
Poor Poor
Coffin et al 2013 RCT 90 12 weeks Treatment seeking patients recruited Aripiprazole 20mg No significant difference No significant difference No significant difference
15 from community in
the USA RR 0.88 intervention vs control for positive UDS (0.66-1.19 p=0.41) number of completed counseling sessions 76% intervention vs 80% placebo p=0.11 visual analog scale scores p=0.38 Brown and Gabrielson
2012 RCT 60 12 weeks
Patients with bipolar depression or MDD in the USA Citocoline 2000mg No significant difference RR 1.09 intervention vs control for positive UDS (p=0.23) Significant improvement Improved survival in intervention group. 41% completed in intervention group vs 14% in control, p=0.02 Kaplan-Meier
NR Poor Poor
Elkashef et al
2012 RCT 140 13 weeks
Patients at multiple substance abuse treatment centers in the USA Topiramate 200mg No significant difference P=0.13 GEE No significant difference 39 in interven retained to end of study vs 38 control, p=0.72 No significant difference Change in BSCS score p=0.09
Fair Good
Tiihonen et al
2012 RCT 100 10 weeks
Treatment seeking patients in Russia
Naltrexone implant 1000mg No significant difference 40% negative UDS in intervention vs 24% control, p=0.09 Significant Improved retention in intervention group, 52% present at end of study vs 28% control p=0.01 No significant difference Statistics not reported
16 Ling et al 2012 RCT 120 108
days
Treatment seeking patients in USA
Flumazenil IV 2mg, gabapentin 1200mg and hydroxyzine 50mg No significant difference P=0.28 No significant difference
57 days for intervention vs 74 days p=0.30 No significant difference Visual analog scale
Good Fair
Colfax et al
2011 RCT 60 12 weeks
Treatment seeking MSM with high risk sexual behavior recruited from community in the USA Mirtazapine 30mg Significant improvement in intervention RR0.57 for positive UDS p=0.02
NR NR Good Poor
Grant et al 2010 RCT 31 8 weeks Treatment seeking patients recruited from the
community in the USA NAC 2400mg and naltrexone 200mg No significant difference 46.2% intervention vs 35.3% p=0.547 No significant difference Penn Craving Scale p=0.106 No significant difference Study completion 64.3% intervention vs 47.1% control p=0.337
Poor Poor
Jayaram-Lindström et al
2008 RCT 80 12 weeks
Treatment seeking patients from community in Sweden. Majority (84%) using D/L-amphetamine, not methamphetamine. Naltrexone 50mg Significant improvement 65.2% negative UDS in intervention vs 47.7% control p<0.05 No significant difference Significant reduction Visual analog scale, P<0.05
Fair Poor
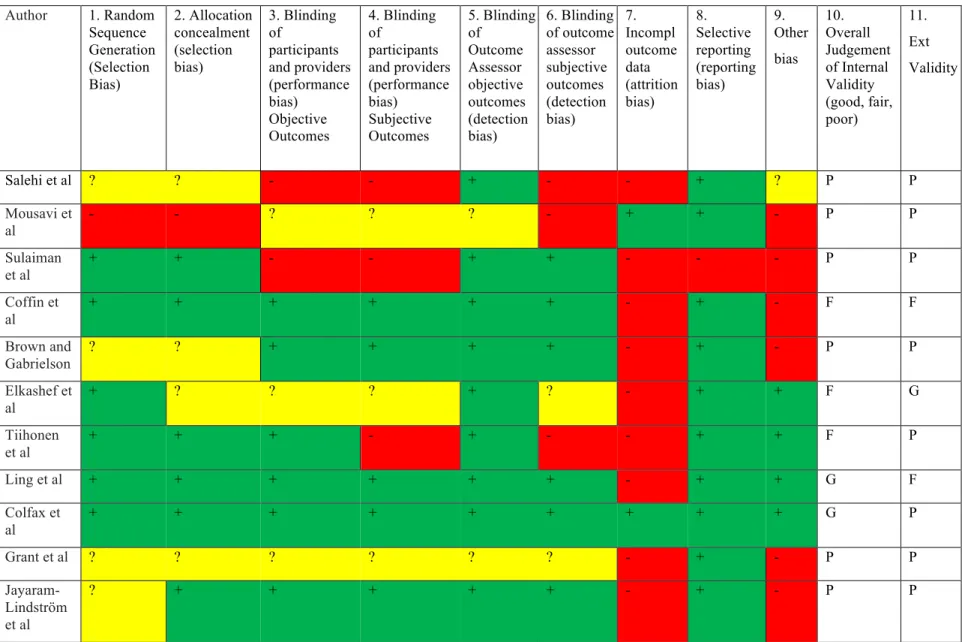
17 Author 1. Random
Sequence Generation (Selection Bias) 2. Allocation concealment (selection bias) 3. Blinding of participants and providers (performance bias) Objective Outcomes 4. Blinding of participants and providers (performance bias) Subjective Outcomes 5. Blinding of Outcome Assessor objective outcomes (detection bias) 6. Blinding of outcome assessor subjective outcomes (detection bias) 7. Incompl outcome data (attrition bias) 8. Selective reporting (reporting bias) 9. Other bias 10. Overall Judgement of Internal Validity (good, fair, poor) 11. Ext Validity
Salehi et al ? ? - - + - - + ? P P
Mousavi et al
- - ? ? ? - + + - P P
Sulaiman et al
+ + - - + + - - - P P
Coffin et al
+ + + + + + - + - F F
Brown and Gabrielson
? ? + + + + - + - P P
Elkashef et al
+ ? ? ? + ? - + + F G
Tiihonen et al
+ + + - + - - + + F P
Ling et al + + + + + + - + + G F
Colfax et al
+ + + + + + + + + G P
Grant et al ? ? ? ? ? ? - + - P P
Jayaram-Lindström et al
? + + + + + - + - P P
18 The results of the analysis of the risk of bias and overall internal validity are presented in Figure 3 above. Only 2 studies (Ling et al and Colfax et al) were judged to have good internal validity. Four studies were judged to have fair internal validity, and the remaining 5 studies had poor internal validity. The most common domain for a high risk of bias was attrition bias due to differential loss of participants between the arms, overall high numbers of drop outs, and/or no presented analysis of the drop outs. The second most common domain with a high risk of bias was the “other” category, in all but one case because of imbalance at baseline between arms of the study or lack of reporting on baseline characteristics. Full information including supporting comments on the risks of bias for each study can be found in Appendix B.
Results of individual studies
The results from each study for the main outcome measures of interest to this review can be found in Table 2. Two studies (Colfax et al20 and Jarayam-Lindstrom et al21) reported significant improvements in UDS results for mirtazapine and naltrexone, respectively. Three studies
(Sulaiman et al22, Brown and Gabrielson23, and Tiihonen et al24) reported significant
improvements in retention for aripiprazole, citocoline, and naltrexone implant respectively. Four studies (Salehi et al, Moussavi et al, Sulaiman et al, and Jarayam-Lindstrom et al) reported significant improvements in craving scores for buprenorphine, NAC, aripiprazole, and naltrexone respectively.
19 through 6, but did not report an overall measure of UDS positivity. They did not report on the prevalence of opioid use in the sample population, which significantly limits the interpretability of the results. Most importantly, the study reported 20 participants in each arm and 100% completion rate, but the numbers given for the first week craving score indicated that there were actually 31 participants in the control group and 23 in the intervention group at the beginning of the study. No reasons or explanation for the discrepancy were given and I judged it to have poor internal validity as a result.
Mousavi et al conducted a randomized cross-over study in 32 men and women in Iran with methamphetamine dependence referred to a tertiary care center using N-acetyl-cysteine (NAC) 1200mg and reported a significant decrease in methamphetamine craving as determined by CCQ-brief scores (p<0.001 ANOVA). However, the results were analyzed only among participants who finished the study, and 28% of the participants were lost to follow-up. Moreover, I judged it to have high risk of reporting bias as the study methods stated that UDS were done at each visit, but no results from the UDS were reported.
Sulaiman et al reported on an RCT of aripiprazole 10mg in 49 participants in Malaysia with methamphetamine dependence and a history of psychotic symptoms and reported no significant difference in UDS results (p = 0.173 GEE). They did report a significant reduction in craving as measured by the Brief Substance Craving Scale (p = 0.015 MMRM) and a significant
20 Coffin et al performed an RCT of aripiprazole 20mg in 90 men and women with
methamphetamine dependence recruited from the general community in San Francisco. They reported no significant difference in positive UDS (RR 0.88 p = 0.41), craving, as measured by a visual analog scale (p = 0.38) or retention, defined as number of completed weekly counseling sessions (76% in intervention versus 80% in control, p = 0.11). There were twice as many participants in the intervention group (10) that dropped out of the study, and the reasons for drop out was not reported.
Brown and Gabrielson reported on an RCT of citicoline 2000mg in 60 men and women in the USA with methamphetamine use and either bipolar depression or major depressive disorder. They reported no significant difference in UDS results (RR 1.09 favoring control p = 0.23), although they did report significantly improved retention in the intervention arm (p = 0.02 Kaplan-Meier). The results, however, were analyzed only among the 48 of 60 participants who returned for follow-up after randomization.
Elkashef et al conducted an RCT of topiramate 200mg in 140 men and women with
methamphetamine dependence in the USA. They found no significant difference in UDS (p = 0.13 GEE), craving by BSCS (p = 0.09), or retention defined as completion of study (p = 0.72). The study was limited by a high loss of participants; only 55% completed the study.
21 detected by experienced opioid users in a dual opioid and methamphetamine population makes it unclear if the results are due to changes in opioid use, un-blinding, or a true effect on
methamphetamine use.
Ling et al conducted an RCT of the PROMETA™ protocol (a proprietary protocol involving flumazenil 2mg IV, gabapentin 1200mg, and hydroxyzine 50mg) in 120 treatment seeking men and women with methamphetamine dependence. They found no significant differences in UDS (p = 0.28), craving (statistics not reported), or retention in treatment when adjusted for a baseline imbalance in age between groups (p = 0.30). As in other studies, there was a high rate of attrition in both groups (41.1% in intervention arm, and 30.9% in control arm).
Colfax et al conducted an RCT of mirtazapine 30mg in 60 MSM with methamphetamine dependence and high risk sexual practices. They reported a significant difference in UDS favoring the intervention (RR 0.57 CI 0.35-0.93). They did not report on retention or craving. I found no significant sources of bias affecting internal validity. However, because
methamphetamine use was associated with sex in this population it is possible that the results were due not to a direct effect of mirtazapine on methamphetamine use, but rather to a reduction in high risk sex that was accompanied by methamphetamine use among the study participants. Grant et al performed an RCT of NAC 2400mg plus naltrexone 200mg in 31 men and women with methamphetamine dependence. They reported no significant difference in UDS (p = 0.547), craving as measured by the Penn Craving Scale (p = 0.106), or retention defined as study
completion (p = 0.337). The study had a high rate of attrition, with only 17 of 31 (54%)
22 Jayaram-Lindstrom et al conducted an RCT of naltrexone 50mg in 80 men and women in
Sweden with amphetamine dependence. They reported a significant difference in UDS favoring the intervention arm with 65.2% negative UDS versus 47.7% in control arm (p < 0.05). They also reported a significant difference in craving scores (p < 0.05), although the actual numbers were not reported. They did not analyze retention in treatment, but from the data they did present, 72.5% in the intervention arm finished the study as did 65% in the control arm. There was a high attrition rate, with only 55 patients finishing the study, and there was a significant baseline difference between groups in the severity of amphetamine use (31 days used in the previous 12 weeks in the intervention group versus 27 in the control). An important caveat to this study is that the main form of amphetamine used by participants in the study was a mixture of dextro- and levo-amphetamine, not methamphetamine, and that 47.5% of participants carried a diagnosis of ADHD.
Synthesis of results
I found no study with both good internal and good external validity. The overall level of internal validity within studies was limited by small study size and high numbers of drop outs.
Comparison between studies was often not possible because outcome measures were inconsistently measured, defined and reported. Because of this, it is difficult to comment on potential reasons for differences between the studies.
When considered by level of internal validity, only studies with good or fair internal validity reported significant improvements on the objective measure of UDS, whereas a higher
23 Table 3
Internal Validity N
Benefit on UDS (n) %
Benefit for Retention (n) %
Benefit for Craving (n) %
Any
Benefit (n) %
Poor 5 0 0% 2 40% 3 60% 4 80%
Fair 4 1 25% 1 25% 1 25% 2 50%
Good 2 1 50% 0 0% 0 0% 1 50%
The 2 studies that reported significant improvement in UDS used different medications, mirtazapine and naltrexone. Both had higher percentages of participants retained to the end of the study than the average among analyzed studies. Colfax et al had an impressive retention rate of 93%, while Jayaram-Lindstrom et al had a completion rate of 69%. They also both examined the treatment in populations distinct from the general population of methamphetamine use disorder. Colfax et al included only MSM with high risk sexual practices, while Jayaram-Lindstrom et al included participants with amphetamine dependence who used mostly non-methamphetamine.
Risk of bias across studies
I did not conduct an assessment of the risk of bias across studies. Discussion
Summary of evidence
24 The results of this review do not alter the conclusions of the other 2 published systematic reviews on this topic, which also found no evidence for a particular pharmacological treatment. Bhatt et al systematically reviewed and meta-analyzed RCTs on modafinil, bupropion,
dextroamphetamine, and methylphenidate. Brackins et al systematically reviewed RCTs on sertraline, bupropion, mirtazapine, modafinil, dexamphetamine, ondansetron, risperidone, baclofen, gabapentin, and aripiprazole.
I compared the list of pharmacological treatments studied in clinical RCTs to treatments
examined in the pre-clinical studies and identified 12 pharmacological agents that have not been evaluated in a clinical trial for the treatment of methamphetamine use disorder. These include diltiazem, clonidine, isradipine, rivastigmine, gamma-vinyl-gamma-amminobutyric acid (vigabatrin), selegiline, perindopril, progesterone, lithium, atomoxetine, varenicline, and valproate.
Limitations of the data
A major limitation of the reviewed literature is that the sizes of reported studies are likely to be inadequate for detecting significant treatment effects. This is compounded by the fact that almost all studies, with the exception of the mirtazapine study among MSM by Colfax et al, suffered large numbers of drop outs.20 The high percentage of drop outs in these studies is likely an inevitable complication of trials for substance use disorders. High proportions of drop outs in these studies means that the studies are more likely to underestimate the true effect size. Larger sample sizes in anticipation of high attrition rates may help to minimize this bias by providing greater power to detect significant differences.
25 injectable or implant formulations where possible. Long acting formulations of naltrexone, buprenorphine and several antipsychotics are now or will soon be available. Use of these formulations would significantly improve the reliability of the results. Barring this, use of biomarker measures of adherence such as blood level monitoring or measurement of urine riboflavin incorporated into study drugs could help to pinpoint whether adherence is, in fact, a major reason for non-significant findings.
Several reviews and studies used “abstinence” from MA use as a main outcome. However, the definition of abstinence varied between studies, not all studies reported it as an outcome, and the clinical significance of subjectively defined “abstinence” vs overall reduction in MA use is not clear. A more useful and comparable approach for future studies would be either to adopt a standard definition of “abstinence” in the context of short term trials (the creation of which is limited by the lack of evidence on what constitutes a significant measure), or report all trials using the same measure of percentage of positive UDS. This would also limit the risk of selective reporting bias, as it is not always clear if the definitions of “positive week” or “abstinence” could have been manipulated to yield more significant results.
Measurement bias is a significant concern. Some studies in this review measured UDS only once every 2 weeks, while others performed UDS 3 times a week. The risk of not detecting significant differences is already higher because of attrition bias, which is very difficult to change, and increasing and standardizing the frequency of UDS in studies is an obvious and achievable way of improving the internal validity of future trials. A related issue is, in effect, the uncertainty about what might otherwise be thought of as the interventions’ Minimal Clinically Significant Difference: there appears to be no agreed upon standard by which to judge the clinical
26 positive across all weeks, while others performed analyses on varying periods of time with negative UDS.
Limitations of this review
A significant limitation of this review is that it was conducted by a single investigator. Analyses of the internal and external validity of studies will usually contain some element of subjectivity. It is possible that some of the findings of this review, particularly judgements about the various risks of bias within studies and generalizability of findings, would be slightly different if done independently by multiple researchers. If possible, having multiple researchers conduct a future review would strengthen the internal validity of the review itself.
I did not conduct an assessment of possible publication bias. However, I believe it is unlikely that any un-published studies would change the conclusion of this review that no
pharmacological treatments for methamphetamine use disorder have been proven to be effective. Publication bias tends toward publishing of positive, rather than negative results. It is more likely that there are un-published negative studies of treatments. Nevertheless, the knowledge of
negative results would help to move the field forward, and a future review would be strengthened by attempting to identify which treatments have been studied but not published. Potential
strategies for addressing this in a future review include searching trial registries, searching for relevant conference proceedings and meeting abstracts, and consulting with experts and study authors to identify other relevant studies that may not have been published.
27 identified by the use of a looping search strategy that repeated the iterations of the search process with slight variations to keep all previously identified studies while potentially including new relevant studies.
Finally, while the goal of this systematic review was to fill in the gap between the two previously published systematic reviews, the usefulness of this review in guiding future research is limited by the fact that the many pertinent studies of agonist treatments were left out of the analysis. It is possible that a synthesis of all pertinent studies including agonist treatments would have yielded different conclusions about the various risks of bias, the potential reasons for non-significant results, and the potential approach to minimizing these issues in future research.
Conclusion
Several studies reported positive results, but were limited by poor internal or external validity and no evidence was found to support treatment of methamphetamine use disorder with a specific medication in the general outpatient population, which had also been found in 2 other systematic reviews of a distinct set of studies. There is a pressing need for more research in this field. Future trials should use consistent outcome measures and address possible power issues caused by high attrition.
Funding
28 Acknowledgements
Dr. Evans had primary responsibility for the conception and design of the review, development of a search strategy, choice of data collection instruments, analysis of included studies,
29 References
Cited Sources
1. Chomchai C, Chomchai S. Global patterns of methamphetamine use. Curr Opin Psychiatry. 2015;28(4):269-274. doi:10.1097/YCO.0000000000000168.
2. Behavioral Health Trends in the United States: Results From the 2014 National Survey on Drug Use and Health. Center for Behavioral Health Statistics and Quality; 2015.
http://www.samhsa.gov/data.
3. Miller MA, Kozel NJ, US Department of Health and Human Services; National Institute on Drug Abuse. Methamphetamine Abuse: Epidemiologic Issues and Implications. 1991. doi:10.1037/e496202006-001.
4. Anderson AL, Li S-H, Biswas K, et al. Modafinil for the treatment of methamphetamine dependence. Drug Alcohol Depend. 2012;120(1-3):135-141.
doi:10.1016/j.drugalcdep.2011.07.007.
5. Cretzmeyer M, Sarrazin MV, Huber DL, Block RI, Hall JA. Treatment of
methamphetamine abuse: research findings and clinical directions. J Subst Abuse Treat. 2003;24(3):267-277.
6. Herbeck DM, Brecht M-L, Lovinger K. Mortality, causes of death, and health status among methamphetamine users. J Addict Dis. 2015;34(1):88-100.
doi:10.1080/10550887.2014.975610.
7. Nguyen D, Smith LM, Lagasse LL, et al. Intrauterine growth of infants exposed to prenatal methamphetamine: results from the infant development, environment, and lifestyle study. J Pediatr. 2010;157(2):337-339. doi:10.1016/j.jpeds.2010.04.024. 8. Lee NK, Rawson RA. A systematic review of cognitive and behavioural therapies for
methamphetamine dependence. Drug Alcohol Rev. 2008;27(3):309-317. doi:10.1080/09595230801919494.
9. Minozzi S, Saulle R, De Crescenzo F, Amato L. Psychosocial interventions for
psychostimulant misuse. Minozzi S, ed. Cochrane Database Syst Rev. 2016;9:CD011866. doi:10.1002/14651858.CD011866.pub2.
10. Grabowski J, Shearer J, Merrill J, Negus SS. Agonist-like, replacement pharmacotherapy for stimulant abuse and dependence. Addict Behav. 2004;29(7):1439-1464.
doi:10.1016/j.addbeh.2004.06.018.
30 amphetamine and methamphetamine use disorders: a systematic review and meta-analysis. Syst Rev. 2016;5(1):189. doi:10.1186/s13643-016-0370-x.
12. Pérez-Mañá C, Castells X, Torrens M, Capellà D, Farre M. Efficacy of psychostimulant drugs for amphetamine abuse or dependence. Pérez-Mañá C, ed. Cochrane Database Syst Rev. 2013;(9):CD009695. doi:10.1002/14651858.CD009695.pub2.
13. Shoptaw SJ, Kao U, Heinzerling K, Ling W. Treatment for amphetamine withdrawal. Shoptaw SJ, ed. Cochrane Database Syst Rev. 2009;(2):CD003021.
doi:10.1002/14651858.CD003021.pub2.
14. Brackins T, Brahm NC, Kissack JC. Treatments for methamphetamine abuse: a literature review for the clinician. J Pharm Pract. 2011;24(6):541-550.
doi:10.1177/0897190011426557.
15. Brackins T, Brahm NC, Kissack JC. Treatments for methamphetamine abuse: a literature review for the clinician. J Pharm Pract. 2011;24(6):541-550.
doi:10.1177/0897190011426557.
16. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9–W64.
17. Castells X, Cunill R, Pérez-Mañá C, Vidal X, Capellà D. Psychostimulant drugs for cocaine dependence. Castells X, ed. Cochrane Database Syst Rev. 2016;9:CD007380. doi:10.1002/14651858.CD007380.pub4.
18. Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]. The Cochrane Collaboration; 2011.
www.handbook.cochrane.org.
19. Pérez-Mañá C, Castells X, Torrens M, Capellà D, Farre M. Efficacy of psychostimulant drugs for amphetamine abuse or dependence. Pérez-Mañá C, ed. Cochrane Database Syst Rev. 2013;(9):CD009695. doi:10.1002/14651858.CD009695.pub2.
20. Colfax GN, Santos G-M, Das M, et al. Mirtazapine to reduce methamphetamine use: a randomized controlled trial. Arch Gen Psychiatry. 2011;68(11):1168-1175.
doi:10.1001/archgenpsychiatry.2011.124.
21. Jayaram-Lindström N, Hammarberg A, Beck O, Franck J. Naltrexone for the treatment of amphetamine dependence: a randomized, placebo-controlled trial. Am J Psychiatry. 2008;165(11):1442-1448. doi:10.1176/appi.ajp.2008.08020304.
22. Sulaiman AH, Gill JS, Said MA, Zainal NZ, Hussein HM, Guan NC. A randomized, placebo-controlled trial of aripiprazole for the treatment of methamphetamine dependence and associated psychosis. Int J Psychiatry Clin Pract. 2013;17(2):131-138.
31 23. Brown ES, Gabrielson B. A randomized, double-blind, placebo-controlled trial of
citicoline for bipolar and unipolar depression and methamphetamine dependence. J Affect Disord. 2012;143(1-3):257-260. doi:10.1016/j.jad.2012.05.006.
24. Tiihonen J, Krupitsky E, Verbitskaya E, et al. Naltrexone implant for the treatment of polydrug dependence: a randomized controlled trial. Am J Psychiatry. 2012;169(5):531-536. doi:10.1176/appi.ajp.2011.11071121.
Studies included in analysis
Brown ES, Gabrielson B. A randomized, double-blind, placebo-controlled trial of
citicoline for bipolar and unipolar depression and methamphetamine dependence. J Affect Disord. 2012;143(1-3):257-260. doi:10.1016/j.jad.2012.05.006.
Coffin PO, Santos G-M, Das M, et al. Aripiprazole for the treatment of methamphetamine dependence: a randomized, double-blind, placebo-controlled trial. Addiction.
2013;108(4):751-761. doi:10.1111/add.12073.
Colfax GN, Santos G-M, Das M, et al. Mirtazapine to reduce methamphetamine use: a randomized controlled trial. Arch Gen Psychiatry. 2011;68(11):1168-1175.
doi:10.1001/archgenpsychiatry.2011.124.
Elkashef A, Kahn R, Yu E, et al. Topiramate for the treatment of methamphetamine addiction: a multi-center placebo-controlled trial. Addiction. 2012;107(7):1297-1306. doi:10.1111/j.1360-0443.2011.03771.x.
Grant JE, Odlaug BL, Kim SW. A double-blind, placebo-controlled study of N-acetyl cysteine plus naltrexone for methamphetamine dependence. European
Neuropsychopharmacology. 2010;20(11):823-828. doi:10.1016/j.euroneuro.2010.06.018.
Jayaram-Lindström N, Hammarberg A, Beck O, Franck J. Naltrexone for the treatment of amphetamine dependence: a randomized, placebo-controlled trial. Am J Psychiatry. 2008;165(11):1442-1448. doi:10.1176/appi.ajp.2008.08020304.
32 Mousavi SG, Sharbafchi MR, Salehi M, Peykanpour M, Karimian Sichani N, Maracy M. The efficacy of N-acetylcysteine in the treatment of methamphetamine dependence: a double-blind controlled, crossover study. Arch Iran Med. 2015;18(1):28-33.
Salehi M, Emadossadat A, Kheirabadi GR, Maracy MR, Sharbafchi MR. The Effect of Buprenorphine on Methamphetamine Cravings. J Clin Psychopharmacol. 2015;35(6):724-727. doi:10.1097/JCP.0000000000000408.
Sulaiman AH, Gill JS, Said MA, Zainal NZ, Hussein HM, Guan NC. A randomized, placebo-controlled trial of aripiprazole for the treatment of methamphetamine dependence and associated psychosis. Int J Psychiatry Clin Pract. 2013;17(2):131-138.
doi:10.3109/13651501.2012.667116.
Tiihonen J, Krupitsky E, Verbitskaya E, et al. Naltrexone implant for the treatment of polydrug dependence: a randomized controlled trial. Am J Psychiatry. 2012;169(5):531-536. doi:10.1176/appi.ajp.2011.11071121.
Studies excluded from analysis
Agonist treatments
Anderson AL, Li S-H, Markova D, et al. Bupropion for the treatment of
methamphetamine dependence in non-daily users: a randomized, double-blind, placebo-controlled trial. Drug Alcohol Depend. 2015;150:170-174.
doi:10.1016/j.drugalcdep.2015.01.036.
Anderson AL, Li S-H, Biswas K, et al. Modafinil for the treatment of methamphetamine dependence. Drug Alcohol Depend. 2012;120(1-3):135-141.
doi:10.1016/j.drugalcdep.2011.07.007.
Galloway GP, Buscemi R, Coyle JR, et al. A randomized, placebo-controlled trial of sustained-release dextroamphetamine for treatment of methamphetamine addiction. Clin Pharmacol Ther. 2011;89(2):276-282. doi:10.1038/clpt.2010.307.
Heinzerling KG, Gadzhyan J, van Oudheusden H, Rodriguez F, McCracken J, Shoptaw S. Pilot randomized trial of bupropion for adolescent methamphetamine abuse/dependence. J Adolesc Health. 2013;52(4):502-505. doi:10.1016/j.jadohealth.2012.10.275.
33 Alcohol Depend. 2010;109(1-3):20-29. doi:10.1016/j.drugalcdep.2009.11.023.
Konstenius M, Jayaram-Lindström N, Beck O, Franck J. Sustained release
methylphenidate for the treatment of ADHD in amphetamine abusers: a pilot study. Drug Alcohol Depend. 2010;108(1-2):130-133. doi:10.1016/j.drugalcdep.2009.11.006.
Ling W, Chang L, Hillhouse M, et al. Sustained-release methylphenidate in a randomized trial of treatment of methamphetamine use disorder. Addiction. 2014;109(9):1489-1500. doi:10.1111/add.12608.
Longo M, Wickes W, Smout M, Harrison S, Cahill S, White JM. Randomized controlled trial of dexamphetamine maintenance for the treatment of methamphetamine dependence. Addiction. 2010;105(1):146-154. doi:10.1111/j.1360-0443.2009.02717.x.
Miles SW, Sheridan J, Russell B, et al. Extended-release methylphenidate for treatment of amphetamine/methamphetamine dependence: a randomized, double-blind,
placebo-controlled trial. Addiction. 2013;108(7):1279-1286. doi:10.1111/add.12109.
Rezaei F, Emami M, Zahed S, Morabbi M-J, Farahzadi M, Akhondzadeh S. Sustained-release methylphenidate in methamphetamine dependence treatment: a double-blind and placebo-controlled trial. Daru. 2015;23(1):2. doi:10.1186/s40199-015-0092-y.
Shearer J, Wodak A, Mattick RP, et al. Pilot randomized controlled study of
dexamphetamine substitution for amphetamine dependence. Addiction. 2001;96(9):1289-1296. doi:10.1080/09652140120070346.
Shearer J, Darke S, Rodgers C, et al. A double-blind, placebo-controlled trial of modafinil (200 mg/day) for methamphetamine dependence. Addiction. 2009;104(2):224-233.
doi:10.1111/j.1360-0443.2008.02437.x.
Shoptaw S, Heinzerling KG, Rotheram-Fuller E, et al. Randomized, placebo-controlled trial of bupropion for the treatment of methamphetamine dependence. Drug Alcohol Depend. 2008;96(3):222-232. doi:10.1016/j.drugalcdep.2008.03.010.
Previously reviewed
34 Heinzerling KG, Shoptaw S, Peck JA, et al. Randomized, placebo-controlled trial of
baclofen and gabapentin for the treatment of methamphetamine dependence. Drug Alcohol Depend. 2006;85(3):177-184. doi:10.1016/j.drugalcdep.2006.03.019.
Piasecki MP, Steinagel GM, Thienhaus OJ, Kohlenberg BS. An exploratory study: the use of paroxetine for methamphetamine craving. J Psychoactive Drugs. 2002;34(3):301-304. doi:10.1080/02791072.2002.10399967.
Shoptaw S, Huber A, Peck J, et al. Randomized, placebo-controlled trial of sertraline and contingency management for the treatment of methamphetamine dependence. Drug Alcohol Depend. 2006;85(1):12-18. doi:10.1016/j.drugalcdep.2006.03.005.
Tiihonen J, Kuoppasalmi K, Föhr J, et al. A comparison of aripiprazole, methylphenidate, and placebo for amphetamine dependence. Am J Psychiatry. 2007;164(1):160-162. doi:10.1176/ajp.2007.164.1.160.
Preclinical studies
Comer SD, Mogali S, Saccone PA, et al. Effects of acute oral naltrexone on the subjective and physiological effects of oral D-amphetamine and smoked cocaine in cocaine abusers. Neuropsychopharmacology. 2013;38(12):2427-2438. doi:10.1038/npp.2013.143.
Dean AC, Sevak RJ, Monterosso JR, Hellemann G, Sugar CA, London ED. Acute modafinil effects on attention and inhibitory control in methamphetamine-dependent humans. J Stud Alcohol Drugs. 2011;72(6):943-953.
Elkashef AM, Rawson RA, Anderson AL, et al. Bupropion for the treatment of methamphetamine dependence. Neuropsychopharmacology. 2008;33(5):1162-1170. doi:10.1038/sj.npp.1301481.
Ersche KD, Roiser JP, Abbott S, et al. Response perseveration in stimulant dependence is associated with striatal dysfunction and can be ameliorated by a D(2/3) receptor agonist. Biol Psychiatry. 2011;70(8):754-762. doi:10.1016/j.biopsych.2011.06.033.
Fabian JE, Silverstone PH. Diltiazem, a calcium antagonist, partly attenuates the effects of dextroamphetamine in healthy volunteers. Int Clin Psychopharmacol. 1997;12(2):113-120.
Ghahremani DG, Tabibnia G, Monterosso J, Hellemann G, Poldrack RA, London ED. Effect of modafinil on learning and task-related brain activity in methamphetamine-dependent and healthy individuals. Neuropsychopharmacology. 2011;36(5):950-959. doi:10.1038/npp.2010.233.
35 from methamphetamine dependence. Exp Clin Psychopharmacol. 2010;18(6):489-497. doi:10.1037/a0021791.
Hysek CM, Brugger R, Simmler LD, et al. Effects of the α₂-adrenergic agonist clonidine on the pharmacodynamics and pharmacokinetics of 3,4-methylenedioxymethamphetamine in healthy volunteers. J Pharmacol Exp Ther. 2012;340(2):286-294.
doi:10.1124/jpet.111.188425.
Hysek CM, Simmler LD, Nicola VG, et al. Duloxetine inhibits effects of MDMA (“ecstasy”) in vitro and in humans in a randomized placebo-controlled laboratory study. Laks J, ed. PLoS ONE. 2012;7(5):e36476. doi:10.1371/journal.pone.0036476.
Jayaram-Lindström N, Konstenius M, Eksborg S, Beck O, Hammarberg A, Franck J. Naltrexone attenuates the subjective effects of amphetamine in patients with amphetamine dependence. Neuropsychopharmacology. 2008;33(8):1856-1863.
doi:10.1038/sj.npp.1301572.
Jayaram-Lindström N, Wennberg P, Hurd YL, Franck J. Effects of naltrexone on the subjective response to amphetamine in healthy volunteers. J Clin Psychopharmacol. 2004;24(6):665-669.
Johnson BA, Ait-Daoud N, Wells LT. Effects of isradipine, a dihydropyridine-class calcium channel antagonist, on D-methamphetamine-induced cognitive and physiological changes in humans. Neuropsychopharmacology. 2000;22(5):504-512. doi:10.1016/S0893-133X(99)00116-5.
Johnson BA, Roache JD, Ait-Daoud N, et al. Effects of acute topiramate dosing on methamphetamine-induced subjective mood. Int J Neuropsychopharmacol.
2007;10(1):85-98. doi:10.1017/S1461145705006401.
Johnson BA, Roache JD, Ait-Daoud N, et al. Effects of isradipine, a dihydropyridine-class calcium-channel antagonist, on d-methamphetamine's subjective and reinforcing effects. Int J Neuropsychopharmacol. 2005;8(2):203-213. doi:10.1017/S1461145704005036.
Johnson BA, Roache JD, Ait-Daoud N, et al. Effects of topiramate on methamphetamine-induced changes in attentional and perceptual-motor skills of cognition in recently abstinent methamphetamine-dependent individuals. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(1):123-130. doi:10.1016/j.pnpbp.2006.08.002.
Johnson BA, Roache JD, Ait-Daoud N, Wallace C, Wells LT, Wang Y. Effects of isradipine on methamphetamine-induced changes in attentional and perceptual-motor skills of cognition. Psychopharmacology (Berl). 2005;178(2-3):296-302.
doi:10.1007/s00213-004-1998-0.
Kalechstein AD, La Garza De R, Newton TF. Modafinil administration improves working memory in methamphetamine-dependent individuals who demonstrate baseline
36 La Garza De R, Mahoney JJ, Culbertson C, Shoptaw S, Newton TF. The
acetylcholinesterase inhibitor rivastigmine does not alter total choices for
methamphetamine, but may reduce positive subjective effects, in a laboratory model of intravenous self-administration in human volunteers. Pharmacol Biochem Behav. 2008;89(2):200-208. doi:10.1016/j.pbb.2007.12.010.
La Garza De R, Newton TF, Haile CN, et al. Rivastigmine reduces “Likely to use methamphetamine” in methamphetamine-dependent volunteers. Prog
Neuropsychopharmacol Biol Psychiatry. 2012;37(1):141-146. doi:10.1016/j.pnpbp.2011.12.014.
La Garza De R, Yoon JH. Evaluation of the effects of rivastigmine on cigarette smoking by methamphetamine-dependent volunteers. Prog Neuropsychopharmacol Biol
Psychiatry. 2011;35(8):1827-1830. doi:10.1016/j.pnpbp.2011.07.006.
La Garza De R, Zorick T, Heinzerling KG, et al. The cardiovascular and subjective effects of methamphetamine combined with gamma-vinyl-gamma-aminobutyric acid (GVG) in non-treatment seeking methamphetamine-dependent volunteers. Pharmacol Biochem Behav. 2009;94(1):186-193. doi:10.1016/j.pbb.2009.08.007.
Lile JA, Stoops WW, Vansickel AR, Glaser PEA, Hays LR, Rush CR. Aripiprazole attenuates the discriminative-stimulus and subject-rated effects of D-amphetamine in humans. Neuropsychopharmacology. 2005;30(11):2103-2114.
doi:10.1038/sj.npp.1300803.
Marks KR, Lile JA, Stoops WW, Rush CR. Separate and combined impact of acute naltrexone and alprazolam on subjective and physiological effects of oral d-amphetamine in stimulant users. Psychopharmacology (Berl). 2014;231(14):2741-2750.
doi:10.1007/s00213-014-3449-x.
Newton TF, La Garza De R, Fong T, et al. A comprehensive assessment of the safety of intravenous methamphetamine administration during treatment with selegiline. Pharmacol Biochem Behav. 2005;82(4):704-711. doi:10.1016/j.pbb.2005.11.012.
Newton TF, La Garza De R, Grasing K. The angiotensin-converting enzyme inhibitor perindopril treatment alters cardiovascular and subjective effects of methamphetamine in humans. Psychiatry Res. 2010;179(1):96-100. doi:10.1016/j.psychres.2009.11.011. Newton TF, Reid MS, La Garza De R, et al. Evaluation of subjective effects of aripiprazole and methamphetamine in methamphetamine-dependent volunteers. Int J Neuropsychopharmacol. 2008;11(8):1037-1045. doi:10.1017/S1461145708009097.
Newton TF, Roache JD, La Garza De R, et al. Bupropion reduces methamphetamine-induced subjective effects and cue-methamphetamine-induced craving. Neuropsychopharmacology. 2006;31(7):1537-1544. doi:10.1038/sj.npp.1300979.
37 2005;182(3):426-435. doi:10.1007/s00213-005-0102-8.
Ray LA, Bujarski S, Courtney KE, et al. The Effects of Naltrexone on Subjective
Response to Methamphetamine in a Clinical Sample: a Double-Blind, Placebo-Controlled Laboratory Study. Neuropsychopharmacology. 2015;40(10):2347-2356.
doi:10.1038/npp.2015.83.
Reed SC, Levin FR, Evans SM. The effects of progesterone pretreatment on the response to oral d-amphetamine in Women. Horm Behav. 2010;58(3):533-543.
doi:10.1016/j.yhbeh.2010.04.003.
Rush CR, Stoops WW, Hays LR, Glaser PEA, Hays LS. Risperidone attenuates the discriminative-stimulus effects of d-amphetamine in humans. J Pharmacol Exp Ther. 2003;306(1):195-204. doi:10.1124/jpet.102.048439.
Rush CR, Stoops WW, Lile JA, Glaser PEA, Hays LR. Subjective and physiological effects of acute intranasal methamphetamine during d-amphetamine maintenance. Psychopharmacology (Berl). 2011;214(3):665-674. doi:10.1007/s00213-010-2067-5.
Silverstone PH, Pukhovsky A, Rotzinger S. Lithium does not attenuate the effects of D-amphetamine in healthy volunteers. Psychiatry Res. 1998;79(3):219-226.
Sofuoglu M, Poling J, Hill K, Kosten T. Atomoxetine attenuates dextroamphetamine effects in humans. Am J Drug Alcohol Abuse. 2009;35(6):412-416.
doi:10.3109/00952990903383961.
Stoops WW, Bennett JA, Lile JA, Sevak RJ, Rush CR. Influence of aripiprazole pretreatment on the reinforcing effects of methamphetamine in humans. Prog Neuropsychopharmacol Biol Psychiatry. 2013;47:111-117.
doi:10.1016/j.pnpbp.2013.08.007.
Stoops WW, Lile JA, Glaser PEA, Rush CR. A low dose of aripiprazole attenuates the subject-rated effects of d-amphetamine. Drug Alcohol Depend. 2006;84(2):206-209. doi:10.1016/j.drugalcdep.2006.02.004.
Stoops WW, Pike E, Hays LR, Glaser PE, Rush CR. Naltrexone and bupropion, alone or combined, do not alter the reinforcing effects of intranasal methamphetamine. Pharmacol Biochem Behav. 2015;129:45-50. doi:10.1016/j.pbb.2014.11.018.
Verrico CD, Mahoney JJ, Thompson-Lake DGY, Bennett RS, Newton TF, La Garza De R. Safety and efficacy of varenicline to reduce positive subjective effects produced by methamphetamine in methamphetamine-dependent volunteers. Int J
Neuropsychopharmacol. 2014;17(2):223-233. doi:10.1017/S146114571300134X.
38 Yoon SJ, Lyoo IK, Kim HJ, et al. Neurochemical alterations in
methamphetamine-dependent patients treated with cytidine-5'-diphosphate choline: a longitudinal proton magnetic resonance spectroscopy study. Neuropsychopharmacology. 2010;35(5):1165-1173. doi:10.1038/npp.2009.221.
Non-randomized or uncontrolled studies
Camacho A, Ng B, Frye MA. Modafinil for bipolar depression with comorbid methamphetamine abuse. Am J Addict. 2010;19(2):190-191. doi:10.1111/j.1521-0391.2009.00024.x.
Carnwath T, Garvey T, Holland M. The prescription of dexamphetamine to patients with schizophrenia and amphetamine dependence. J Psychopharmacol (Oxford).
2002;16(4):373-377.
Fechtner RD, Khouri AS, Figueroa E, et al. Short-term treatment of cocaine and/or methamphetamine abuse with vigabatrin: ocular safety pilot results. Arch Ophthalmol. 2006;124(9):1257-1262. doi:10.1001/archopht.124.9.1257.
Fleming PM, Roberts D. Is the prescription of amphetamine justified as a harm reduction measure? J R Soc Health. 1994;114(3):127-131.
Hellem TL, Sung Y-H, Shi X-F, et al. Creatine as a Novel Treatment for Depression in Females Using Methamphetamine: A Pilot Study. J Dual Diagn. 2015;11(3-4):189-202. doi:10.1080/15504263.2015.1100471
Jayaram-Lindström N, Wennberg P, Beck O, Franck J. An open clinical trial of naltrexone for amphetamine dependence: compliance and tolerability. Nord J Psychiatry.
2005;59(3):167-171. doi:10.1080/08039480510023052.
Laqueille X, Dervaux A, Omari El F, Kanit M, Baylé FJ. Methylphenidate effective in treating amphetamine abusers with no other psychiatric disorder. Eur Psychiatry. 2005;20(5-6):456-457. doi:10.1016/j.eurpsy.2005.03.013.
Maletzky BM. Phenelzine as a stimulant drug antagonist: a preliminary report. Int J Addict. 1977;12(5):651-655.
Mann N, Bitsios P. Modafinil treatment of amphetamine abuse in adult ADHD. J Psychopharmacol (Oxford). 2009;23(4):468-471. doi:10.1177/0269881108091258.
McElhiney MC, Rabkin JG, Rabkin R, Nunes EV. Provigil (modafinil) plus cognitive behavioral therapy for methamphetamine use in HIV+ gay men: a pilot study. Am J Drug Alcohol Abuse. 2009;35(1):34-37. doi:10.1080/00952990802342907.
39 McRae-Clark AL, Brady KT, Hartwell KJ, White K, Carter RE. Methylphenidate
transdermal system in adults with past stimulant misuse: an open-label trial. J Atten Disord. 2011;15(7):539-544. doi:10.1177/1087054710371171.
Meredith CW, Jaffe C, Yanasak E, Cherrier M, Saxon AJ. An open-label pilot study of risperidone in the treatment of methamphetamine dependence. J Psychoactive Drugs. 2007;39(2):167-172. doi:10.1080/02791072.2007.10399875.
Nejtek VA, Avila M, Chen L-A, et al. Do atypical antipsychotics effectively treat co-occurring bipolar disorder and stimulant dependence? A randomized, double-blind trial. J Clin Psychiatry. 2008;69(8):1257-1266.
Pal R, Mendelson JE, Flower K, et al. Impact of prospectively determined A118G polymorphism on treatment response to injectable naltrexone among methamphetamine-dependent patients: an open-label, pilot study. J Addict Med. 2015;9(2):130-135.
doi:10.1097/ADM.0000000000000107.
Sattar SP, Bhatia SC, Petty F. Potential benefits of quetiapine in the treatment of substance dependence disorders. J Psychiatry Neurosci. 2004;29(6):452-457.
Tennant FS, Rawson RA. Cocaine and amphetamine dependence treated with desipramine. NIDA Res Monogr. 1983;43:351-355.
Republication or secondary analysis of previously published study
Brensilver M, Heinzerling KG, Swanson A-N, Telesca D, Furst BA, Shoptaw SJ. Cigarette smoking as a target for potentiating outcomes for methamphetamine abuse treatment. Drug Alcohol Rev. 2013;32(1):96-99. doi:10.1111/j.1465-3362.2012.00423.x. McCann DJ, Li S-H. A novel, nonbinary evaluation of success and failure reveals
bupropion efficacy versus methamphetamine dependence: reanalysis of a multisite trial. CNS Neurosci Ther. 2012;18(5):414-418. doi:10.1111/j.1755-5949.2011.00263.x.
Stoops WW, Lile JA, Glaser PEA, Rush CR. A low dose of aripiprazole attenuates the subject-rated effects of d-amphetamine. Drug Alcohol Depend. 2006;84(2):206-209. doi:10.1016/j.drugalcdep.2006.02.004.
Zorick T, Sugar CA, Hellemann G, Shoptaw S, London ED. Poor response to sertraline in methamphetamine dependence is associated with sustained craving for methamphetamine. Drug Alcohol Depend. 2011;118(2-3):500-503. doi:10.1016/j.drugalcdep.2011.04.015.
Wrong outcome
Cruickshank CC, Montebello ME, Dyer KR, et al. A placebo-controlled trial of mirtazapine for the management of methamphetamine withdrawal. Drug Alcohol Rev. 2008;27(3):326-333. doi:10.1080/09595230801935672.