G
uide
T
o
T
he
F
uTure
:
A Strategic Roadmap to Achieving Meaningful Use Objectives and Selecting an Integrated Electronic Dental Record (EDR)/Electronic Health Record (EHR) System to Improve Oral Health Access and Outcomes
table
of
contents
Introduction ... 1
Meaningful Use for Oral Health ... 2
Current Meaningful Use Objectives and Exclusions for Consideration ... 6
Core Set Objectives ... 7
Menu Set Objectives ... 8
Current Clinical Quality Measures for Oral Health ... 10
Clinical Quality Measures for Oral Health ... 12
EHR Selection ... 17
EDR/EHR Selection Tool ... 18
Step 1: Eligible Professional Assessment ... 19
Step 2: Vendor Background Information – Request for Information (RFI) ... 20
Step 3: Review of Meaningful Use Core & Menu Set Objectives ... 21
Step 4: Review of Meaningful Use Clinical Quality Measures (CQMs) ... 21
Step 5: Vendor Response to Meaningful Use Certification and Reporting Measures... 22
Step 6: Vendor Response to NNOHA’s Proposed CQMs for Oral Health ... 22
Step 7: Vendor Response to EDR/EHR Practice-Specific Requirements ... 23
Step 8: Vendor Response to Qualitative Requirements... 25
Step 9: Vendor Response to Vendor Solution Cost. ... 26
Step 10: Vendor Selection Criteria and Summary Ratings ... 26
Discussion on Use of EDR/EHR Selection Tool, Vendor’s Self Scoring and General Disclaimer ... 28
Challenges Selecting and Implementing an EDR/EHR Solution ... 29
EDR/EHR Implementation Strategies ... 30
Conclusion: A Strategic Pathway to the Future ... 33
Appendix A1: Meaningful Use Vendor Survey Responses ... 36
Appendix A2: Rating Chart: Vendor Response to EDR/EHR Practice-Specific Requirements... 38
Appendix A3: Rating Chart: Vendor Response to Qualitative Requirements ... 52
Appendix A4: Rating Chart: Vendor Response to Vendor Solution Cost ... 53
Appendix A5: Rating Chart: Vendor Selection Criteria and Summary Ratings... 55
Appendix A6: Vendor Background Information and Evaluations ... 55
Product Name: QSI Dental – Electronic Dental Record (EDR) ... 57
Product Name: Dentrix Enterprise/Sage Intergy ... 62
Product Name: Mediadent ... 72
Product Name: Open Dental and eClinicalWorks ... 80
Appendix B: Sources of Information/Additional Resources ... 87
Appendix C: Glossary ... 88
Appendix D: References ... 89
Appendix E: Credits ... 91
i
nTroducTion
The future of health care can be found in combining skillful providers with the technological tools that allow them to provide the best possible care for their patients. At the forefront of this combination is the concept of Meaningful Use: terminology used by the Centers for Medicare and Medicaid Services (CMS) that means providers must show they are using certified Electronic Health Record (EHR) technologies in ways that can be measured. The National Network for Oral Health Access (NNOHA) developed this white paper to present a strategic roadmap for achieving Meaningful Use for oral health and to provide critical steps that need to be taken to implement an EHR system that fully integrates Electronic Dental Records (EDR). This white paper will help oral health providers, staff, and patients understand the benefits of Meaningful Use incentives and serve as a guide to selecting an Electronic Dental and Health Record system.
NNOHA’s Health Information Technology (HIT) Workgroup (formerly HIT Committee) was established to help guide safety-net oral health programs through HIT decisions and challenges as they emerge. EDR issues have remained a priority for the Workgroup, which is continuing to assess the EHR needs of Health Center oral health programs and make recommendations to guide Health Centers in selecting technology solutions that are compatible with the systems used by both medical and dental staff. Through a Health Resources and Services Administration (HRSA) Cooperative Agreement, NNOHA strives to provide technical assistance to Health Centers seeking to provide, expand, or improve oral health services.
NNOHA’s HIT Workgroup goals are to:
■ Provide key stakeholders, Dental Directors, Executive Directors, and Information Technology (IT) decision makers with objective comparisons among the current leading EDR/EHR products.
■ Provide input to dental software developers on areas for improvement within existing applications to
better meet the challenges of Meaningful Use compliance, Health Center patient care, and practice management of oral health programs.
■ Advocate for integration of a dental module within Electronic Health Records as a vital part of the
product functionality offered to Health Centers.
■ Identify potential Meaningful Use measures for oral health.
■ Provide Dental Directors and Health Center oral health programs with practical resources for selecting, implementing, and optimizing HIT.
When a Health Center finds a system that best meets the needs of their organization, as well as Meaningful Use criteria, it allows for maximized resources, increased reimbursements, and improved patient care. This paper can serve as a guide in the process, and facilitate the Health Centers’ decision making process toward improved use of HIT.
Terminology
1 “Health Center” is the term commonly used to refer to Community Health Centers, migrant health centers, health centers that treat the homeless, and centers that
treat residents of public housing.
2 “Federally Qualified Health Center” or FQHC is a Medicare/Medicaid/CHIP term related to reimbursement, which includes Section 330 of the Public Health Service
Act funded centers, sub-recipients (e.g. sub-grantees) and look-alikes.
3 Authorizing Section 330 legislation has officially changed the term “Community Health Center” to the accepted term “Health Center” and that is the term used
throughout this paper to refer to the above listed types of grant-supported entities. © National Network for Oral Health Access, August 2012
The information in this document was accurate at the time of this printing. As regulations and information regarding Health Centers are not static, NNOHA recommends readers verify any critical information with different state regulations and changes that may have occurred since printing.
M
eaninGFul
u
se
F
or
o
ral
h
ealTh
Background
One only has to listen to the news or pick up a journal to know that the United States health care delivery system is highly fragmented. Dentists, physicians, and other health care specialists utilize separate records with patient’s health information residing in a broad mix of paper charts, ancient legacy systems, new web-based tools, and everything in between. This variation has resulted in a lack of coordination and effective data sharing among dental and other medical professionals, negatively affecting patient care. As a result, the federal government has invested billions of dollars to create a health information technology infrastructure. One important component of this support is the creation of financial incentives (stimulus funds) to encourage eligible professionals (EPs) and health care organizations to implement and use electronic health records (EHRs) effectively using a concept referred to as “Meaningful Use.”
Meaningful Use has become an important consideration for Health Centers not only because it could improve patient care, but because there are financial incentives available through the
American Recovery and Reinvestment Act of 2009 (ARRA). There are two important considerations when trying to interpret Meaningful Use: the requirements the health
professional or care delivery organization must meet, and the technology in use by the provider. In the simplest terms, “Meaningful Use” means providers need to show
they are using certified EHR technology in ways that can be measured significantly in quality and in quantity (Health Resources and Services Administration, 2011). Participating in the Meaningful Use incentive program has been a challenge for many EPs, especially dentists, who must meet the same eligibility requirements as other EPs in order to qualify for payments under the Medicaid Electronic Health Record Incentive Program. This also means that they must demonstrate all of the Meaningful Use objectives plus some optional measures detailed later in this report.
Current Meaningful Use objectives and measures are based on medical practice, and require observation, assessment and recording of areas of health that may not be pertinent for dental practice. As a result, several Meaningful Use objectives contain exclusion criteria. Dental practices will have to evaluate whether their practice meets the exclusion criteria for each applicable objective.
There is a significant gap between the current situation and achieving Meaningful Use objectives, making it difficult for oral health providers and electronic dental record (EDR) vendors to participate in the national initiative to increase the use of technology as a means to improve health care. NNOHA will continue to assist Health Centers in Meaningful Use involvement by monitoring the capabilities of dental software vendors in meeting Meaningful Use criteria and providing guidance in selection of EDR/EHR systems. NNOHA and other key stakeholders have identified oral health measures for Stage 2 and the proposed rule includes the following two oral health measures beginning with Calendar Year (CY) 2014:
■ NQF 1335: Title – Children who have dental decay or cavities.
■ NQF 1419: Title – Primary Caries Prevention Intervention as Part of Well/Ill Child Care as Offered by Primary Care Medical Providers.
NNOHA will continue to develop or identify clinical quality measures for dental/oral health care with partners and stakeholders that could be ready for future years.
Stimulating EHR Implementation
Health Information Technology (HIT) has tremendous potential to transform the delivery of health care by integrating clinical, administrative and financial systems and other administrative tasks, and providing the infrastructure to support them. One of the essential clinical systems is the EHR. An EHR generally includes a longitudinal collection of information on the health of an individual or the care provided. An EHR also provides immediate electronic access to patient and population-level information by authorized users, decision support to enhance the quality, safety, and efficiency of patient care, and support of efficient processes for health care delivery (Melvin, 2008).
In April 2004, President George W. Bush called for widespread adoption of interoperable EHRs within ten years and issued an executive order that established the position of the National Coordinator for Health Information Technology within the Department of Health and Human Services (Melvin, 2008). A framework document released two months later described four main goals for achieving nationwide interoperability of HIT. These goals included: (1) informed clinical practice, (2) interconnection of clinicians, (3) personalized care, and (4) improvements in population health (Thompson & Brailer, 2004). Collectively, these initiatives laid the groundwork for an organized effort to drive adoption of interoperable HIT. However, other barriers still exist, including the initial high costs of investing in HIT, the ongoing maintenance required in all information systems, and short-term loss of productivity as staff adapt to new technology and systems.
To stimulate the investment and use of EHRs, the federal government has established a combination of voluntary financial incentives and eventual penalties to encourage the Meaningful Use of EHR for Medicare and Medicaid providers. Stimulus funds, designed to increase the use of EHRs, is only one of many information technology initiatives encouraged by the federal government. However, lack of Meaningful Use measures relating to oral health may lead to a reduction in dental provider participation in the stimulus fund program for
EDR/EHR implementation and integration.
HIT is becoming increasingly prevalent in medical offices and facilities. Like President George W. Bush before him, President Barack Obama announced a plan
to computerize the medical records of all Americans by 2014 (Jones, 2009). The functionality of comprehensive EHR systems goes far beyond the traditional
role of paper dental/medical records. In addition to providing ready access to clinical documentation, these systems quickly transmit diagnostic test images and results to physicians so that the data can be reviewed and shared with patients. EDR/EHRs feature computerized provider order entry (CPOE), which allows health care providers to send patient orders, such as those for laboratory tests and medications, electronically to appropriate parties. EDR/EHR systems also provide decision support tools, including clinical reminders, drug allergy/ interaction alerts, drug-dose recommendations, and suggestions for diagnostic and treatment options (Hoffman & Podgurski, 2011). EDR/EHRs are revolutionizing business in the health care industry, allowing medical professionals to work faster, smarter, and more efficiently than ever before.
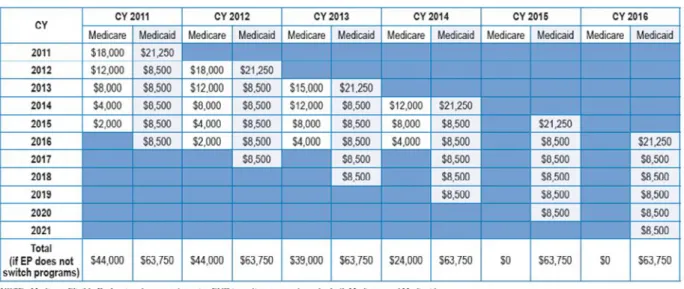
The American Recovery and Reinvestment Act of 2009 (ARRA) dedicated $27 billion to the promotion of HIT. It provides payments of up to $44,000 per clinician under the Medicare incentive program and $63,750 per clinician under the Medicaid program (Hoffman & Podgurski, 2011). Meaningful Use regulations were issued in July 2010, delineating what hospitals and clinicians must do to be deemed meaningful users of EHR systems in 2011 and beyond. Those in compliance will be eligible for EHR incentive payments, registration for which began in January 2011. Two additional phases of Meaningful Use requirements will be staged in three steps over the course of the next five years.
■ Stage 1 (2011 and 2012) sets the baseline for electronic data capture and information sharing.
■ Stage 2 expected to be implemented in 2014 under the proposed rule: “Meaningful Use” includes standards such as online access for patients to their health information and electronic health information exchange between providers.
■ Stage 3 expected to be implemented in 2016: “Meaningful Use” includes demonstrating that the
quality of health care has been improved (Centers for Medicare & Medicaid Services, 2012).
During Stage 1, EPs (e.g., dentists and other health center providers) are required to meet fifteen “core” objectives. Later in this report is a diagram that highlights the steps for determining eligibility for dentists (refer to Figure 1, “Eligible Professional Assessment Map for Dentists”). Several of these measures focus on basic data entry, including
vital signs, patient demographics, drug and allergy lists, updated problem lists, and smoking status. In addition, EPs must comply with five out of a “menu” of ten additional objectives. Some of the menu items include: performing drug-formulary checks, incorporating laboratory results into patient records, providing patients with reminders for needed care, supplying relevant educational resources, and supporting transitions between care facilities or personnel (Centers for Medicare & Medicaid Services, 2012).
Up until now, the adoption of HIT has generally been slow in the United States. Recent research highlights accelerated adoption of EMR/EHR systems. EMR/EHR system use among office-based physicians increased from 18% in 2001 to 57% in preliminary 2011 estimates (CDC, 2011). The federal Meaningful Use EHR incentive program intends to boost those numbers through millions of dollars in federal incentive payments. While much of the discussion to date has focused on physician practices and hospitals, it is notable that the incentive program was made available to doctors of dental surgery and dental medicine as well.
The United States spends more on health care than any other country, yet performs far below many others in quality measures that include life expectancy, equities in the access to care, and the inconsistency of care in demographic locations (Gaylin, et al., 2011). The use of information technology is recognized as having a major role in the transformation of health care in order to meet the Six Aims for Improvement as identified in the Institute of Medicine’s Committee on the Quality of Health Care in America, Crossing the Quality Chasm (2001). The use of technology in health care will increase treatment and business efficiency, promote patient safety, increase continuity of care, increase access to quality care, and reduce disparities in health care. Increasing evidence shows that the future of health care will involve an integration of two historically separate modalities of health care, medicine and dentistry (Rudman, 2010). The level of communication necessary to increase the quality of care that will be generated by the integration of medical and dental services will have a much greater success rate with the utilization of technology accessible by all providers.
To promote the use of technology, the Health Information Technology for Clinical Use Act (HITECH) allows for access to federal stimulus funds for Medicaid and Medicare providers who show Meaningful Use of electronic information technology. Stage 1 of the Meaningful Use guidelines does not provide specific oral health measures that can be utilized by dental providers, thus delaying dentists from achieving Meaningful Use. Support for EDR/ EHR implementation by public dental organizations is evidenced in a 2010 collaborative letter from vested dental organizations sent to the Centers for Medicare and Medicaid Services (CMS) (Tankersley, et al., 2010). The letter states that these organizations realize the value and potential for health care providers, including dentists, to participate in EHR implementation. The organizations echoed a recurring theme addressing concerns that face dental providers in their attempt to meet Meaningful Use requirements. The system requirements associated with EHR implementation place a potentially significant burden on solo and small group practices. Large dental groups are better equipped to implement these systems; however, practices with five or more providers, account for less than 1.2% of all dental practices (Tankersley, et al., 2010).
c
linical
Q
ualiTy
M
easure
B
arriers
The primary areas of contention for dental providers in meeting Meaningful Use are the clinical quality measures (CQMs). The CQMs are defined by the CMS as the processes, experiences, and/or outcomes of patient care that are measured through observations and treatment addressing one or more of the Six Aims for Improvement in Health Care (Heubusch, 2010). The use of quality metrics is recognized as the driver of improvements in health care. Unless measures that address oral health are utilized, oral health care may be overlooked in the health care reform initiative. The Department of Health and Human Services (HHS) recognizes oral health as one of the target areas in achieving optimal national health through its Healthy People 2020 publication (Healthy People, 2011). This recognition supports the inclusion of oral health quality metrics for Meaningful Use. NNOHA’s Health Information Technology and Meaningful Use Workgroup has identified six clinical quality core measures and other alternative measures for consideration by HHS as potential Meaningful Use measures that can be met by oral health providers. A consideration for oral health-focused CQMs is important in development of a data format that can be captured and stored in an EHR. It will then be necessary for such data to be electronically transmitted to CMS in a structured, standardized format.
CMS prefers to select CQMs endorsed by the National Quality Forum (NQF) for the Meaningful Use
requirements. The NQF is a nonprofit organization established in 1999 whose membership is made up of public and private sector entities with an interest in quality health care. The NQF’s mission is to improve the quality of American health care by setting national priorities and goals for performance endorsements through national consensus standards for measuring and public reporting of performance. The NQF promotes the attainment of national goals through education and public outreach programs (NQF, 2011). Currently, all the clinical quality measures recognized by CMS for Meaningful Use are endorsed by the NQF. NNOHA has recognized the need for NQF endorsement and will support future endorsement efforts for oral health CQMs.
The average length of the endorsement process is three years; however, a consideration to expedite the process can occur if measures are shown to be well-established, widely used, or meet an urgent national need (NQF, 2011). The expedited consideration decreases the number of days for several of the steps in the process, but does not decrease the criteria for evaluation. NNOHA is currently exploring an expedited process to include relevant CQM for oral health.
Current Meaningful Use Objectives and Exclusions for Consideration
One of the requirements for receiving Meaningful Use reimbursements is to track several quality improvement objectives. The question asked most often by dentists regarding Meaningful Use is: “Do dentists have to meet all of the required Core Set Meaningful Use objectives?” The answer is currently yes, with some explanation. CMS has a list of 15 required “Core Set” objectives and 10 additional “Menu Set” objectives. CMS states that, “To qualify for an incentive payment, 20 of these 25 objectives must be met. There are 15 required core objectives. The remaining 5 objectives may be chosen from the list of 10 Menu Set objectives” (Centers for Medicare & Medicaid Services, 2011). However, there are exclusions available that can be claimed during attestation (the online process where EPs prove they are
meeting the Meaningful Use requirements). The exclusion requirements for each objective are available at CMS’s website link: https://www.cms.gov/ehrincentiveprograms and also shown in the tables and figures below.
The following table lists all fifteen of the required Core Set objectives and also identifies if they are part of a dentist’s normal routine and if there are any known exclusions.
Objective Measure exclusiOn Dentist rOutine
Record patient demographics (sex, race, ethnicity, date of birth, preferred language)
More than 50% of patients’ demographic data recorded as structured data
None Yes
Record vital signs and chart changes (height, weight, blood pressure, body-mass index, growth charts for children)
More than 50% of patients 2 years of age or older have height, weight, and blood pressure recorded as structured data
An EP who either sees no patients 2 years or older, or who believes that all three vital signs of height, weight, and blood pressure of their patients have no relevance to their scope of practice
Yes: Blood pressure No: Other vitals
Maintain up-to-date problem list of current and active diagnoses
More than 80% of patients have at least one entry recorded as structured data
None Yes
Maintain active medication list More than 80% of patients have at least one entry recorded as structured data
None Yes
Maintain active medication
allergy list More than 80% of patients have at least one entry recorded as structured data
None Yes
Record smoking status for patients
13 years of age or older More than 50% of patients 13 years of age or older have smoking status recorded as structured data
An EP who sees no patients
13 years or older Potential
Provide patients with clinical
summaries for each office visit Clinical summaries provided to patients for more than 50% of all office visits within 3 business days
An EP who has no office visits during the EHR reporting period
Potential
On request, provide patients with an electronic copy of their health information (including diagnostic test results, problem list, medication lists, medication allergies)
More than 50% of requesting patients receive electronic copy within 3 business days
An EP that has no requests from patients or their agents for an electronic copy of patient health information during the EHR reporting period
Potential
Generate and transmit permissible
prescriptions electronically More than 40% are transmitted electronically using certified EHR technology
An EP who writes fewer than 100 prescriptions during the EHR reporting period
Potential
Computer provider order entry
(CPOE) for medication orders More than 30% of patients with at least one medication in their medication list have at least one medication ordered through CPOE
An EP who writes fewer than 100 prescriptions during the EHR reporting period
Objective (cOnt.) Measure exclusiOn Dentist rOutine
Implement drug and
drug-allergy interaction checks Functionality is enabled for these checks for the entire reporting period
None Yes
Implement capability to
electronically exchange key clinical information among providers and patient-authorized entities
Perform at least one test of EHR’s capacity to electronically exchange information
None Yes
Implement one clinical decision support rule and ability to track compliance with this rule
One clinical decision
support rule implemented None Yes
Implement systems to protect privacy and security of patient data in the EHR
Conduct or review a security risk analysis, implement security updates as necessary, and correct identified security deficiencies
None Yes
Report clinical quality measures
(CQMs) to CMS or states For 2011, provide aggregate numerator and denominator through attestation; for 2012, electronically submit measures. Note: NNOHA has proposed additional CQMs for consideration that are relevant to oral health.
None Potential
Objective Measure exclusiOn Dentist rOutine
Implement drug formulary checks Drug formulary check system is implemented and has access to at least one internal or external drug formulary for the entire reporting period
None Yes
Incorporate clinical laboratory test results into EHRs as structured data
More than 40% of clinical laboratory test results whose results are in positive/ negative or numerical format are incorporated into EHRs as structured data
An EP who orders no lab tests whose results are either in a positive/negative or numeric format during the EHR reporting period
Yes – available via integration with an EHR (Intergy)
Generate lists of patients by specific conditions to use for quality improvement, reduction of disparities, research, or outreach
Generate at least one listing of patients with a specific condition
None Yes
Use EHR technology to identify patient-specific education resources and provide those to the patient as appropriate
More than 10% of patients are provided patient-specific education resources
None Yes
An EP must report on 5 out of 10 Menu Set objectives; 1 of the 5 must be a Public Health Objective (designated as *PH*)
Objective (cOnt.) Measure exclusiOn Dentist rOutine
Perform medication reconciliation
between care settings Medication reconciliation is performed for more than 50% of transitions of care
An EP who was not the recipient of any transitions of care during the EHR reporting period
Potential
Provide summary of care record for patients referred or transitioned to another provider or setting
Summary of care record is provided for more than 50% of patient transitions or referrals
An EP who neither transfers a patient to another setting nor refers a patient to another provider during the EHR reporting period
Potential
Send reminders to patients (per patient preference) for preventive and follow-up care
More than 20% of patients 65 years of age or older or 5 years of age or younger are sent appropriate reminders
An EP who has no patients 65 years old or older or 5 years old or younger with records maintained using certified EHR technology
Potential
Provide patients with timely electronic access to their health information (including laboratory results, problem list, medication lists, medication allergies)
More than 10% of patients are provided electronic access to information within 4 days of its being updated in the EHR
An EP that neither orders nor creates any of the information listed at 45 CFR 170.304(g) during the EHR reporting period
Potential
*PH* Submit electronic
immunization data to immunization registries or immunization
information systems
Perform at least one test of data submission and follow-up submission (where registries can accept electronic submissions)
An EP who administers no immunizations during the EHR reporting period or where no immunization registry has the capacity to receive the information electronically
No
*PH* Submit electronic syndromic surveillance data to public health agencies
Perform at least one test of data submission and follow-up submission (where public health agencies can accept electronic data)
An EP who does not collect any reportable syndromic information on their patients during the EHR reporting period or does not submit such information to any public health agency that has the capacity to receive the information electronically
Potential
To be able to report on these objectives, it is essential that practices utilize an EHR. The CMS Medicare and Medicaid incentive programs provide a financial reward for the Meaningful Use of certified EHRs to achieve health and efficiency goals. The Office of the National Coordinator for Health Information Technology (ONC) regulations specify the technical capabilities that EHR technology must have to be certified and to support providers in achieving the Meaningful Use objectives. In 2010, the ONC released this definition of “certified EHR technology,” “a Complete EHR or a combination of EHR Modules, each of which (1) meets the requirements included in the definition of a Qualified EHR; and (2) has been tested and certified in accordance with the certification program established by the National Coordinator as having met all applicable certification criteria adopted by the ONC” (Federal Register, 2010).
For more information about the Medicare and Medicaid EHR Incentive Program, please visit http://www.cms.gov/ EHRIncentivePrograms.
c
urrenT
c
linical
Q
ualiTy
M
easures
F
or
o
ral
h
ealTh
Dentists must report six CQMs that include three Core Set measures. The remaining three measures must be selected from a Menu Set of alternative measures. Clinical quality measure reporting is a requirement; however no thresholds must be met. There are 38 additional CQMs, listed later in this section, from
which a dentist must select three. A maximum of nine CQM measures would be reported if the dentist needed to attest to the three required core, the three alternate core, and the three additional measures.
The following table lists the current CQMs:
cOre set Menu set
Clinical Quality Metrics 3 are required (select alternative core set measures if the core measure does not apply)
3 out of other clinical quality measures alternative measures are required
Current CQMs: Core Set Measures (must select 3 measures)
ePs Must rePOrt On three cOre set Measures Dentist rOutineHypertension: Blood Pressure Measurement Potential Tobacco Use Assessment & Counseling Potential
Adult Weight Screening and Follow-up No
alternate cOre set Measures fOr ePs
(substitute when any Of the abOve 3 DO nOt aPPly)
Weight Assessment & Counseling for Children
and Adolescents No
Influenza Vaccination for Patients > 50 years No
Childhood Immunization Status No
*An alternate core set of 3 measures is substituted for any of the 3 core metrics where the measure does not apply to the dental program. Clinical quality measure reporting is a requirement; however no thresholds must be met.
Current Menu Measures for All EPs (must select 3 measures):
In addition to the three CQM selections described earlier, providers will need to select 3 more measures from the current Menu Set of 38 CQMs on the next page.
Menu Measures nQf PQri
Pneumonia Vaccination for Patients 65 Years and Older 0043 111
Screening Mammography 0031 112
Colorectal Cancer Screening 0034 113
Cervical Cancer Screening 0032 —
Chlamydia Screening in Women 0033 —
Controlling High Blood Pressure 0018 —
Asthma: Pharmacologic Therapy 0047 53
Asthma Assessment 0001 64
Use of Appropriate Medications for People with Asthma 0036 —
Childhood Immunization Status 0038 —
Diabetes Mellitus: Dilated Eye Exam in Diabetic Patient 0055 117
Diabetes Mellitus: Urine Screening for Microalbumin 0062 119
Diabetes Mellitus: Hemoglobin A1c Poor Control 0059 1
Comprehensive Diabetes Care: HbA1c Control (<8.0%) 0575 —
Diabetes Mellitus: Foot Exam 0056 163
Diabetic Retinopathy: Documentation of Retinopathy 0088 18
Diabetes Mellitus: High Blood Pressure Control 0061 3
Communication with the Physician Managing On-going Care 0089 19
Diabetes Mellitus: Low Density Lipoprotein (LDL-C) Control 0064 2
Diabetes Mellitus: Dilated Eye Exam in Diabetic Patient 0055 117
Oral Antiplatelet Therapy Prescribed for Patients with CAD 0067 6
Beta-Blocker Therapy for CAD Patients with Prior MI 0070 7
Beta-Blocker Therapy for Left Ventricular Dysfunction (LVSD) 0083 8
Drug Therapy for Lowering LDL-Cholesterol 0073 197
Use of Aspirin or Another Antithrombotic 0068 204
Warfarin Therapy for Patients with Atrial Fibrillation 0084 200
Blood Pressure Management Control 0073 201
Use of Aspirin or Another Antithrombotic 0068 204
ACE Inhibitor or ARB for Left Ventricular Dysfunction (LVSD) 0081 5
Breast Cancer: Hormonal Therapy for Stage IC-IIIC Estrogen Receptor/
Progesterone Receptor (ER/PR) Positive Breast Cancer 0387 71
Colon Cancer: Chemotherapy for Stage II Colon Cancer Patients 0385 72 Prostate Cancer: Avoidance of Overuse of Bone Scan for Staging Low-Risk
Prostate Cancer Patients 0389 102
Major Depression: (a) Effective Acute Phase Rx Treatment and (b) Continuation 0105 9 Initiation and Engagement of Alcohol and Other Drug Dependence Treatment:
(a) Initiation, (b) Engagement 0004 —
Prenatal Screening for Human Immunodeficiency Virus (HIV) 0012 —
Prenatal Anti-D Immune Globulin 0014 —
Appropriate Testing for Children with Pharyngitis 0002 66
c
linical
Q
ualiTy
M
easures
F
or
o
ral
h
ealTh
In Stage 1, the Core Set Clinical Quality Measures (CQMs) are not as pertinent to oral health as they could be. NNOHA identified six measures that are particularly applicable to Health Center oral health programs (listed below). These measures were selected based on: (1) ease of data gathering; (2) ability to report through the current coding system; and (3) impact on improving the oral health status of the patients. The following Core Set Measures for Oral Health would be substituted when any of the current CQMs do not apply (please note: these measures are under review and have not been approved by CMS).
These CQMs for oral health would provide a significant step toward measurable, valuable, uniform clinical quality oral health measures across all Health Centers.
Additional Menu Set Measures for Oral Health
The current Menu Set of 38 items is not applicable for oral health programs. Measures that have been recently added to Stage 2 proposed rule or could be added in the future to the Menu Set that would be more applicable to oral health are listed below. (Please note: two of the following oral health measures, NQF 1335 and NQF 1419, were included in the Stage 2 proposed rule).
*For the definition of “Phase 1” treatment, please refer to the “Fundamentals” Chapter of the Operations Manual for Health Center Oral Health Programs: http://www.nnoha.org/practicemanagement/manual.html.
cOre set Measures nuMeratOr DenOMinatOr
4. Oral Cancer Risk Assessment & Counseling – Percentage of all patients who receive soft tissue screening, oral cancer exam and counseling.
The number of patients who receive soft tissue screening, oral cancer exam and counseling.
The number of patients who receive a comprehensive oral health exam (ADA code 0110) or a periodic recall (ADA code 0120) oral health exam during the report period.
5. Periodontal Disease Assessment –
Percentage of patients age 18 years and older who have been screened for the presence of periodontal disease.
The number of patients age 18 years and older who have been screened for the presence of periodontal disease.
who have been screened for the presence of periodontal disease. The number of patients age 18 years and older who receive a comprehensive oral health exam (ADA code 0110) or a periodic recall (ADA code 0120) oral health exam during the report period.
6. Completed Comprehensive Treatment Plan – Percentage of all dental patients for whom the Phase 1* treatment plan is completed within a 12 month period.
The number of patients with a completed Phase 1 treatment within 12 months of initiation.
The number of patients that receive a comprehensive oral health exam (ADA code 0110) or a periodic recall (ADA code 0120) oral health exam during the report period.
Menu set Measures fOr Oral health nQf
Children who received preventive dental care 1334
Children who have dental decay or cavities (INCLUDED in STAGE 2) 1335 Primary caries prevention intervention as part of well/ill child care as offered by
primary care medical providers (INCLUDED in STAGE 2) 1419
Total eligible patients who received preventive dental services (EPSDT) N/A Total eligible patients who received dental treatment services (EPSDT) N/A Percentage of new dental emergency patient visits (scheduled and unscheduled,
walk-in) N/A
Percentage of pregnant patients that receive an oral exam or
preventive dental treatment N/A
PrOPOseD tOP three alternate cOre set Measures fOr Dentists (substitute when any Of the
current cQMs DO nOt aPPly) Dentist rOutine
Annual Oral Health Visit Yes
Topical Fluoride or Fluoride Varnish Treatment Yes
Periodontal Disease Assessment Yes
PrOPOseD Other alternate cOre set Measures fOr Dentists Dentist rOutine
Dental Sealant Yes
Oral Cancer Risk Assessment & Counseling Yes
Completed Comprehensive Treatment Plan Yes
cOre set Measures nuMeratOr DenOMinatOr
1. Annual Oral Health Visit—
Percentage of patients who had at least one dental visit during the measurement year (the last 12 months).
The number of patients with one
or more dental visits. The total number of registered patients at the Health Center.
2. Topical Fluoride or Fluoride Varnish Treatment – Percentage of patients age 14 years and younger with at least one topical fluoride treatment or fluoride varnish treatment documented (the last 12 months).
The number of patients age 14 years and younger with at least one topical fluoride or Fluoride Varnish treatment (ADA code 1203).
The number of patients age 14 years and younger who receive a comprehensive oral health exam (ADA code 0110) or a periodic recall (ADA code 0120) oral health exam during the report period.
3. Dental Sealant – Percentage of patients age 6 to 20 years that have sealants on 1st and 2nd permanent molars.
The number of patients age 6 to 20 years that received sealant treatment on 1st and 2nd permanent molars after examination.
The number of patients age 6 to 20 years who were treatment planned to receive sealants at the examination.
Please note the four oral health measures endorsed by NQF (Aug, 2011) are listed below. ■ Annual dental visit
■ Children who received preventive dental care
■ Primary caries prevention intervention as part of well/ill child care as offered by primary care medical providers (INCLUDED in STAGE 2)
■ Children who have dental decay or cavities (INCLUDED in STAGE 2)
All four measures need to be e-measure specified (Harris, 2011). An eMeasure is a health quality measure encoded in a health quality measure format (HQMF). eMeasure testing should be done on the major EDR/EHR vendor systems in use to ensure that reliability and validity. NQF endorsement implies that a measure has been tested and shown to have adequate rates of validity and reliability. NNOHA plans to move forward with plans to test these measures. Stage 2 of Meaningful Use will include new requirements, criteria associated with new objectives and measures, and changes to the scope and threshold of existing measures. EPs who attest to Stage 1 Meaningful Use in 2011 will have until 2014 to meet Stage 2 Meaningful Use standards and receive incentive payments. NNOHA and other key stakeholders endorse the new two following oral health measures for Stage 2 beginning with CY 2014:
■ NQF 1335: Title – Children who have dental decay or cavities.
■ Description: Assesses if children aged 1-17 years have had tooth decay or cavities in the past 6 months.
■ NQF 1419: Title – Primary Caries Prevention Intervention as Part of Well/Ill Child Care as Offered by Primary Care Medical Providers.
■ Description: The measure will a) track the extent to which the PCMP or clinic (determined by the
provider number used for billing) applies FV as part of the EPSDT examination and b) track the degree to which each billing entity’s use of the EPSDT with FV codes increases from year to year (more children varnished and more children receiving FV four times a year according to ADA recommendations for
high-risk children).
In the Medicare & Medicaid EHR Incentive Program Registration and Attestation System (the online registration system for receiving reimbursements), dentist must fill in the numerators
and denominators for the Meaningful Use objectives and CQMs, indicate if they qualify for exclusions to specific objectives, and attest their eligibility by entering that data into the Attestation System. An EDR/EHR system must provide a report of the numerators, denominators and other required information.
To attest for the Medicare EHR Incentive Program in the first year of participation, a dentist will need to have met Meaningful Use for a consecutive 90-day reporting period. Incentive payments for the Medicare EHR Incentive Program will be made approximately 4 to 8 weeks after a dentist meets the program requirements and successfully attests.
At the time of this publication, under the Medicaid EHR Incentive Program, dentists in many states can register and attest. If the state’s EHR Incentive Program has not yet launched at the time of the dentist’s registration, the file will be placed into a pending status until the state’s program launches. Once registered, dentists can attest that they have adopted, implemented or upgraded certified EHR technology in their first year of participation to receive an incentive payment. Medicaid incentives will be paid by the states and are required to issue incentive payments within 45 days of dentists successfully attesting. Adopt, implement or upgrade means:
■ Adopt – Acquire, purchase or install a certified EHR system. ■ Implement – Install or commence use of certified EHR technology
and have started one of the following:
• A training program for the certified EHR technology;
• Data entry of patient demographic and administrative data into the EHR; • Establishment of data exchange agreements and a relationship between
the provider’s certified EHR technology and other providers (such as laboratories, pharmacies, or health information exchanges).
■ Upgrade – Expand the available functionality of certified EHR technology capable of meeting Meaningful Use requirements at the practice site, including staffing, maintenance, and training, or upgrade from existing EHR technology to certified EHR technology per the Office of the National Coordinator (ONC) EHR certification criteria. Some examples of upgrading the existing EHR technology are the addition of clinical decision support, e-prescribing functionality, and computerized physician order entry.
Several states are currently capable of supporting all activities related to participation in the Medicaid EHR Incentive Program, including:
• Program eligibility
• Registration
• Attestation to adoption, implementation, and upgrade activities
• Incentive program payments
In the first year of participation in the Medicaid EHR Incentive Program, dentists that choose to demonstrate eligibility based on adopt/implement/upgrade (AIU) activities will need to attest to the following:
• Purchase and installation of ONC certified EHR technology that is commercially available
• Development or upgrade of custom EHR technology with subsequent certification by an ONC-ACTB
• Integration of certified EHR technology modules
• Testing and training in the use of the certified EHR technology
As part of initial registration with the CMS National Level Repository (NLR), providers have the opportunity to specify the CMS EHR Certification ID of their EHR system. Dentists will need to supply the CMS EHR
Certification ID during the Meaningful Use attestation process and attest that this Certification ID reflects a system that is actually being adopted, implemented, or upgraded. The accuracy of the attestation as to the specific certified EHR system is ultimately the responsibility of the provider. Providers will be instructed that it is their responsibility to maintain all applicable records to support their attestations for a period of no less than six years in the event of a post-payment audit.
To support attestations to AIU of certified EHR technology in the first year of participation in the Medicaid EHR Incentive Program, providers would supply documentation that demonstrates either a binding financial commitment or actual expenditures on adoption, implementation, or upgrade of the EHR technology. The documentation from an EDR/EHR vendor should include product name and version in such a way that it can be matched to a specific product or combination of products in the ONC’s web-based Certified HIT Product List (CHPL). The following documentation should be retained and produced upon request:
■ Signed contracts, purchase orders, or receipts for purchase or lease of commercial off-the-shelf certified EHR software or proof of subscription to hosted EHR software
■ Documentation of expenses incurred in development, testing, maintenance, and upgrade of custom certified EHR systems or modules
■ Proof of payment for professional services related to the selection, acquisition, installation,
and setup of certified EHR technology and the successful integration of the certified EHR technology into the clinical workflow
■ Purchase agreements or receipts for computer hardware or software required to operate the
certified EHR system
■ Documentation of expenses incurred in transitioning patient records to the certified EHR system ■ Contracts or proof of actual expenditures for testing and/or training for the certified EHR system Note that the software must be in use in clinical practice to count as adoption as a part of meeting the adopt/ implement/upgrade requirements. Centers should also be prepared, in the event of post-payment audit, to demonstrate that the certified EHR technology is actually in use in the clinical setting. For a detailed illustration of this process, view page C-5 of the New York State MEDICAID Health Information Technology Plan: http://www.health.ny.gov/regulations/arra/docs/medicaid_health_information_technology_plan.pdf.
ehr s
elecTion
People sometimes use the terms “Electronic Medical Record” (EMR) or “Electronic Dental Record” (EDR) when talking about Electronic Health Record (EHR) technology. Very often an EDR or EMR is just another way to describe an EHR, and both providers and vendors sometimes use the terms interchangeably. For the purposes of the Medicare and Medicaid Incentive Programs, EPs must use ONC certified EHR technology. The Certified HIT Product List (CHPL) provides the authoritative, comprehensive listing of Complete EHRs and EHR Modules that have been tested and certified under the Temporary Certification Program maintained by the Office of the National Coordinator for Health IT (ONC). Certified EHR technology gives assurance to purchasers and other users that an EHR system or module offers the necessary technological capability, functionality, and security to help them meet the meaningful use criteria. Certification also helps providers and patients be confident that the electronic health IT products and systems they use are secure, can maintain data confidentially, and can work with other systems to share information.
Currently there are no flawless EDR systems or EDR/EHR integrated solutions available on the market. Every system has imperfections in working with oral health programs. Some systems are more robust with different features than others; some are more user-friendly, but none meets every need for Health Center oral health programs. The task becomes finding the best fit for each Health Center depending on their needs, current systems, and resources.
In general, EHRs, although not evaluated by this workgroup, are not considered to be dental friendly, especially when it comes to flexible scheduling or graphics. However, EMR products are well ahead of dental products in terms of tracking disease outcomes and diagnosis. This is because dental practices, with the exception of oral surgery and hospital practices, do not usually use diagnostic codes for billing as do medical practices. In addition, scheduling for dental procedures is challenging in medical EHR products since dental scheduling is not as flexible. While medical appointments may be slotted for 15 to 30 minutes, the appointment time for dental services vary with procedures, type of providers (general or specialist), and level of experience of the providers, such as new or seasoned graduates, students and residents.
While using an integrated EHR sounds ideal, Health Centers have other issues to consider before this can be a reality. If a dental patient is not a medical patient at the Center, medical records or other relevant information are not readily available. In the process of deciding which EDR/EHR system to use for an oral health program, the Dental Director may not have a lot of flexibility, as oral health programs are generally on the same practice management system with the medical department so that all types of data tracking can be done by one department. Until a true health home is established, access to a patient’s medications or ailments will remain a challenge. With these thoughts in mind, NNOHA has developed an EHR Selection Tool described below. For more information about which EHR systems and modules are certified for the Medicare and Medicaid EHR Incentive Programs, please visit http://healthit.hhs.gov/.
edr/ehr s
elecTion
T
ool
Now that it has been established that electronic health records (EHR) are a key piece of Meaningful Use and the future of health programs in general, the next step for many entities will be determining the best technology for their organization. The NNOHA EDR/EHR selection tool is a multistep process that will guide members and other interested stakeholders in evaluating and selecting an EDR/EHR for oral health programs and assist dentists (an eligible professional (EP)), in determining eligibility for the Medicare and Medicaid EHR incentive programs. The selection tool is available to NNOHA members and other key stakeholders on the NNOHA website: http://www.nnoha.org/practicemanagement/hit.html
The NNOHA selection tool starts with guiding the dentist through a series of questions to determine eligibility for EDR/EHR incentive payments and financial impact. The guide also includes key criteria to identify which EDR/EHR systems can achieve interoperability between EDR and EHR systems, meet national Meaningful Use objectives and are capable of reporting NNOHA’s proposed clinical quality measures for oral health.
The four vendors that have been included in this process for consideration are:
■ QSI/NextGen – QSI EDR and NextGen EHR.
■ Open Dental/eClinicalWorks – Open Dental EDR and eClinicalWorks EHR. Please note eClinicalWorks is a separate corporation.
■ Henry Schein/Vitera (formerly Sage) – Dentrix Enterprise and Sage Intergy EHR.
Please note Vitera is a separate corporation and has a HL7 interface to Dentrix Enterprise.
■ Mediadent/SuccessEHS – Mediadent EDR and Success EHS EHR.
The selection tool also includes clinical, financial and administrative requirements that have been grouped into categories and a vendor solution cost assessment.
THE PROCESS
s
Tep1: e
liGiBlep
roFessionala
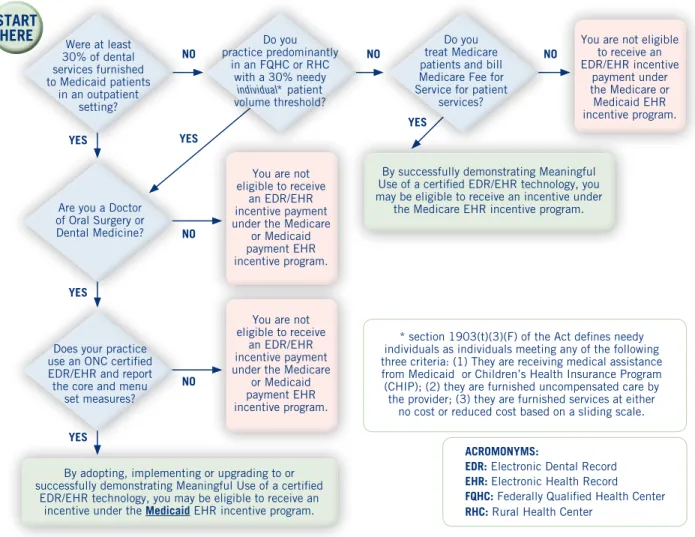
ssessMenTEach Health Center’s dentists should start by completing the eligible professional assessment and deciding to participate in Meaningful Use. The eligible professional assessment flow chart, below in Figure 1, will help determine if a dentist is eligible for the MU incentive and payment schedule shown in Figure 2.
Figure 1: Eligible Professional Assessment Map for Dentists
steP DescriPtiOn Of stePs
1 Eligible Professional Assessment
2 Vendor Background Information - Request For Information (RFI) 3 Review of Meaningful Use Core & Menu Set Objectives
4 Review of Meaningful Use Clinical Quality Measures (CQMs)
5 Vendor Response to Meaningful Use Certification and Reporting Measures
6 Vendor Response to NNOHA’s Proposed Clinical Quality Measures (CQMs) for Oral Health 7 Vendor Response to EDR-EHR Practice-Specific Requirements
8 Vendor Response to Qualitative Requirements 9 Vendor Response to Vendor Solution Cost 10 Vendor Selection Criteria and Summary Ratings
Verification of Provider Eligibility
After the dentist determines eligibility status, the process continues by applying for the Medicaid EHR Incentive Program by visiting the website of the CMS National Level Repository (NLR) and logging in with the required information, including National Provider Identifier (NPI) and CMS Certification Number (CCN). Visit the CMS site for more details: https://www.cms.gov/EHRIncentivePrograms/20_RegistrationandAttestation.asp#TopOfPage.
Were at least 30% of dental services furnished to Medicaid patients in an outpatient setting? START HERE NO YES NO NO NO YES YES YES YES NO
Are you a Doctor of Oral Surgery or Dental Medicine?
Does your practice use an ONC certified EDR/EHR and report the core and menu
set measures?
By adopting, implementing or upgrading to or successfully demonstrating Meaningful Use of a certified
EDR/EHR technology, you may be eligible to receive an incentive under the Medicaid EHR incentive program.
Do you practice predominantly in an FQHC or RHC with a 30% needy individual* patient volume threshold?
You are not eligible to receive
an EDR/EHR incentive payment under the Medicare
or Medicaid payment EHR incentive program.
You are not eligible to receive
an EDR/EHR incentive payment under the Medicare
or Medicaid payment EHR incentive program.
Do you treat Medicare patients and bill Medicare Fee for Service for patient
services?
You are not eligible to receive an EDR/EHR incentive payment under the Medicare or Medicaid EHR incentive program.
By successfully demonstrating Meaningful Use of a certified EDR/EHR technology, you may be eligible to receive an incentive under
the Medicare EHR incentive program.
* section 1903(t)(3)(F) of the Act defines needy individuals as individuals meeting any of the following three criteria: (1) They are receiving medical assistance from Medicaid or Children’s Health Insurance Program (CHIP); (2) they are furnished uncompensated care by the provider; (3) they are furnished services at either
no cost or reduced cost based on a sliding scale. ACROMONYMS:
EDR: Electronic Dental Record EHR: Electronic Health Record FQHC: Federally Qualified Health Center RHC: Rural Health Center
Meaningful Use Eligibility Flowchart
How to Use This Flow Chart:Doctors of Dental Medicine or Oral Surgery are eligible professionals (EPs) and may be eligible for EDR/EHR incentive payments. A dental EP that qualifies to receive EDR/EHR incentive payments under Medicare or Medicaid will maximize their payments by choosing the Medicaid EHR incentive program. Follow the path of answering the question to determine eligibility and start by assuming the dental EP did not perform 90% of the dental services in an inpatient hospital or emergency room hospital setting. A dental EP who qualifies for both Medicaid and Medicare can only participate in one program.
The NLR website will collect required information on the applicant, such as name, e-mail address, business address, telephone number, and the desired incentive program (Medicare or Medicaid, and state, if applicable). CMS will then transmit to the State a list of applicants who selected the Medicaid EHR Incentive Program, along with the CMS Certification Number (CCN).
s
Tep2: V
endorB
ackGroundi
nForMaTion– r
eQuesTF
ori
nForMaTion(rFi)
The process continues by identifying EDR/EHR vendors that the Health Center is considering and requesting both company background information and product information. The Health Center’s evaluation and selection team should learn what basic and advanced functions the EDR/EHR systems perform, how these systems will improve efficiency, understand the various deployment models (e.g. ASP – Application Service Provider, SaaS- Software-as-a-Service), and learn industry terminology. At least three EDR/EHR vendors should be considered for evaluation. Research the vendor’s financial status, technical capabilities, customer satisfaction, and gain a general sense of what these systems cost. The following information should be considered for the RFI request.
■ Company and Product Capabilities:
– History of delivering EDR/EHR solutions
– Client base (# of organizations)
– Number of safety net/Health Center clients
– Largest client (number of connected sites and number of users)
■ Implementation and Support Services: Ask vendors to respond to the approach to define and implement systems to meet all requirements and resources assigned to customer support. Tools/approaches are utilized to help diagnose and resolve customer issues, with remote diagnosis and on-site.
■ Compelling Reasons to Select Solutions: Ask vendors to provide reasons for selecting their EDR/EHR and imaging solution.
■ Meaningful Use (MU) Plans: Ask vendors to respond to plans to attain MU certification and provide tools, knowledge, and services available to assist in attaining MU incentives.
■ Integration Capabilities: Ask vendors to respond to capabilities to integrate EDR/EHR with radiographic
imaging and intraoral camera technologies, manage the images, access the images from within charting software, and optimize workflow.
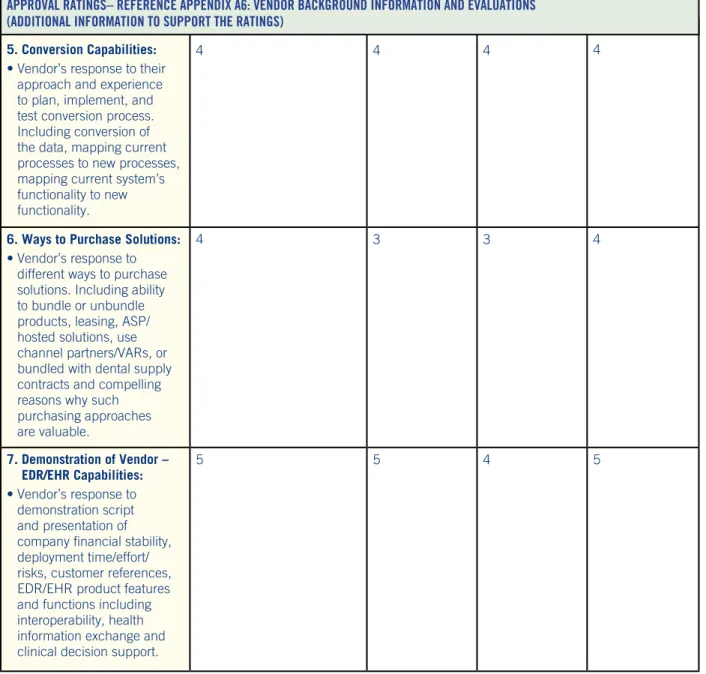
■ Conversion Capabilities: Ask vendors about their approach and experience in planning, implementing,
and testing conversion processes, including conversion of the data, mapping current processes to new processes, and mapping current systems functionality to new functionality.
■ Ways to Purchase Solutions: Ask vendors to respond to different ways to purchase solutions, including ability to bundle or unbundle products, leasing, ASP/hosted solutions, use of channel partners/VARs, or bundled with dental supply contracts. Ask, why are such purchasing approaches valuable?
■ Demonstration of Vendor EDR/EHR Capabilities: Ask vendors to respond to a demonstration script
and present the company financial performance, deployment time/effort/risks, customer references, EDR/EHR product features and functions including interoperability, health information exchange, and clinical decision support.
s
Tep3: r
eViewo
FM
eaninGFulu
sec
ore& M
enus
eTo
BjecTiVesStep three of the selection tool continues with an assessment of meeting specific Meaningful Use requirements. The Health Center should review the Core and Menu Set objectives and determine which objectives align with the dental routine. NNOHA has provided an initial assessment for review earlier in this paper.
s
Tep4: r
eViewo
FM
eaninGFulu
sec
linicalQ
ualiTyM
easures(cQM
s)
Step four continues with an assessment of meeting specific Meaningful Use clinical quality measure (CQM) requirements that were discussed earlier in this paper. Dentists must report from the table of 44 clinical quality measures which includes, 3 Core Set, 3 Alternate Core Set, and 38 additional CQMs.
The 3 Core Set CQMs are Hypertension, Smoking Cessation, and Adult Weight Screening. The 3 Alternate Core CQMs are Weight Assessment for Children, Flu Vaccinations for Patients over 50, and Childhood Immunizations. Dentists must report on the 3 Core Set CQMs. If a dentist reports “0”s for one or more of the 3 “Required Core” CQMs, he/she must then report on up to 3 Alternate Core CQMs. Therefore, dentists may have to report on as many as six Core CQMs.
Dentists must also select 3 additional CQMs from a set of 38 measures in addition to the core/alternate core measures. It is acceptable to have a ‘0’ denominator provided the dentist does not have an applicable population. Several dentists will find the measures not relevant to their patient populations. However, they must still report on 3 of these measures with numerators and denominators where possible and “0”s for the others.
s
Tep5: V
endorr
esponseT
oM
eaninGFulu
sec
erTiFicaTiona
ndr
eporTinGM
easuresStep five ascertains if the vendor response meets Meaningful Use certification and reporting requirements. To qualify for the program, a dentist must own or have access to certified EHR technology that has been certified by the Office of the National Coordinator for Health Information Technology (ONC). Dentists must also be able to demonstrate Meaningful Use of that technology. The NNOHA HIT Workgroup engaged in a product evaluation of four leading electronic dental record systems that are committed to Meaningful Use and have EDR/EHR solutions for Health Centers. As previously mentioned, the four vendors that participated in the NNOHA HIT survey are as follows:
■ QSI/NextGen – QSI EDR and NextGen EHR.
■ Open Dental/eClinicalWorks – Open Dental EDR and eClinicalWorks EHR. Please note eClinicalWorks is a separate corporation.
■ Henry Schein/Vitera (formerly Sage) – Dentrix Enterprise and Sage Intergy EHR. Please note Vitera
is a separate corporation and has a HL7 interface to Dentrix Enterprise.
■ Mediadent/SuccessEHS – Mediadent EDR and Success EHS EHR. Please note that other EDR/EHR vendors may meet Health Centers’ requirements and would be included in this step.
The responses to the survey are listed in Appendix A1. To verify if a vendor is ONC certified visit: http://onc-chpl.force.com/ehrcert.
s
Tep6: V
endorr
esponseT
onnoha’
sp
roposedcQM
sF
oro
ralh
ealThThe NNOHA HIT Workgroup identified six Core Set Proposed Clinical Quality Measures (CQMs) for oral health and additional alternative Menu Set measures for potential inclusion in dentists’ Meaningful Use reporting in the future. This step shows the vendor responses to NNOHA’s Request for Information (RFI) with commercially available products. All vendor responses stated they would be able to support the reporting of the proposed measures with current or future upgrades. NNOHA recommends that each Health Center’s evaluation team find out what is required to generate the reports with current versions of the product during vendor demonstrations.
Dentrix – ehr sOlutiOn
(sage intergy) nextgen ehrQsi eDr – MeDiaDent – successehs eclinical wOrksOPen Dental –
Considering NNOHA’s proposed Clinical Quality Measures for oral health providers, would you be able to support the reporting of these sets of measures:
Annual oral health visit Yes Yes Yes Yes
Topical fluoride or fluoride
varnish Treatment Yes Yes Yes Yes
Periodontal disease
assessment Yes Yes Yes Yes
(cOnt.) Dentrix – ehr sOlutiOn
(sage intergy) nextgen ehrQsi eDr – MeDiaDent – successehs eclinical wOrksOPen Dental –
Dental sealant Yes Yes Yes Yes
Oral cancer risk assessment
& counseling Yes Yes Yes Yes
Completed comprehensive
treatment plan Yes Yes Yes Yes
Children who received
preventive dental care Yes Yes Yes Yes
Children who have dental decay or cavities (INCLUDED IN STAGE 2)
Yes Yes Yes Yes
Primary caries prevention intervention as part of well/ ill child care as offered by primary care medical providers (INCLUDED IN STAGE 2)
Yes Yes Yes Yes
Total eligible patients who received dental treatment services (EPSDT)
Yes Yes Yes Yes
Percentage of new dental emergency patient visits (scheduled & unscheduled, walk-in)
No Yes Yes Yes
Percentage of pregnant patients that receive an oral exam or preventive dental treatment
Yes Yes Yes Yes
Periodontal disease
assessment Yes Yes Yes Yes
s
Tep7: V
endorr
esponseT
oedr/ehr p
racTice-s
peciFicr
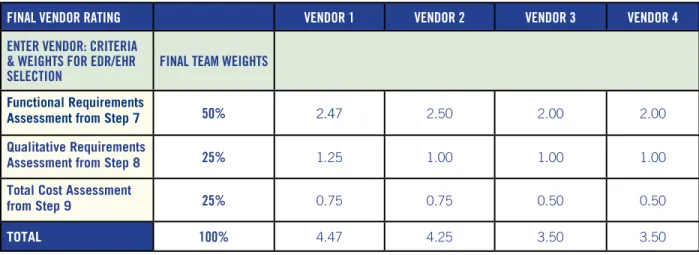
eQuireMenTsThis step compares the vendor responses to EDR/EHR functional requirements. The NNOHA HIT Workgroup members expanded the EDR/EHR functional requirements to more closely reflect the needs of Health Center providers and administrators. This is an initial set of EDR/EHR functional requirements.
Functional requirements define a function of an EDR/EHR system or its components. A function is described as a set of inputs, the behavior, and outputs. These requirements are presented as a starting point for oral health programs to use in their system evaluation and selection process but they are not intended to be complete or inclusive. Customizing and prioritizing the requirements to meet the organization’s needs are essential. Meaningful Use and other qualitative requirements have also been included and specify criteria that can be used to judge the operation of a system or vendor. Non-functional requirements are often called “qualities of a system” (e.g., quality goals, quality of service requirements).