International Journal Advances in Social Science and Humanities
Available online at: www.ijassh.com
RESEARCH ARTICLE
Perception of Medical Staff VIS-A-VIS the Stigma Patients with
Mental Disorders
Petronela Nechita*, Carolina Crăciun, Georgiana Crăciun
University of Medicine and Pharmacy, IASI, România.
*Corresponding Author: Email:[email protected]
Abstract
The aim is to show the perception of healthcare professionals on stigma and discrimination against patients with mental disorders in Moldova - Romania. Methods: The study is prospective, quantitative, descriptive type questionnaire applied to medical personnel during the period July 2012-July 2013 in medical centers in Iasi, Suceava, Botosani, Vaslui. It had population of 217 research staff members involved in patient with mental disorders: psychiatrists, psychologists, family physicians, clinicians from other specialties. The questionnaire covered all stages from pre-test, review, validation and application in their final form. The results were statistically processed for each item, showing the correlations later responses to questions based on different characteristics of study groups. Discussion: Stigma is a modifiable risk factor by removing avoidant coping strategies. Between stigma and mental health professionals there is a complex relationship in which they can be stigmatized, stigmatized and important partners in the fight against stigma. Stigma can be reduced through education, protest, legislative reform. Conclusions: Medical staff believes that psychiatric patient is discriminated and stigmatized. The subject of non-discrimination is an ambitious challenge in Romania, an EU member country.
Keywords: Health care, Social stigma, Mental disorder
The Concept of Stigma
According to sociological theories, stigma refers to a type of behavior, a feature, and the subject was classified as undesirable, his reputation was discredited [1]. Marginalized and excluded groups are attested in ancient written documents of mankind. Stigma is a
phenomenon with multiple negative
consequences in social functioning and in the personal. Stigma has four components as: labeling an individual with a particular disease, generalization individuals with the same disease, creating a division and discrimination of individuals. The diagnosis is a label, but it is not mandatory that diagnosis to determine stigmatization. Thus, breast cancer diagnosis is an example of that although in the past women were ashamed, they now talk openly about the illness without fear of stigmatization [2].
Public stigmatization of the patient
frequently generates marginalization on the subject, with social difficulties, difficulties in employment, healthcare unfair [2, 3]. A great individual contribution to social stigmatization has media, which associate
mental disorder with notions of
incompetence, violence, guilt. Often the stigma, discrimination and the patient is harmed [4]. Media play an important role in the stigmatization of patients with mental disorders, especially by issuing information,
which mistakenly focus on crime,
unpredictability, danger [5]. In society, the most vulnerable and stigmatized category is that of patients with mental disorders [4].
mental disorders towards the stigma. Identity involves affiliation to a group, and the reaction is the result of stigma [6]. Also features stigma (visibility, controllability, impact) is important in the process of stigmatization [7].
There are two main types of stigma: internal stigma and external stigma. In the case of internal stigma (self-stigma), the patient feels different and expects to be discriminated against by the society. Self-stigma refers to internalize inferiority feelings like guilt, shame [8]. External stigma refers to discrimination against others, employing an unfair attitude towards the patient [9]. Both internal and external stigma leads to social isolation [10] and to diminishing the social support [8]. Stigma is seen as a form of social oppression [11].
Self-Stigma, Social Stigma and
Stigma by Association in Psychiatry
Stigma, a complex process in the society, has multiple ethical implications [2]. The stigmatized patient may have difficulty in getting hired [12], is marginalized, and access to health care services is made difficult. The social stigma of individuals can lead by default to self-stigmatization, and the patient's family may be stigmatized through the so-called phenomenon of stigma by association [2].
Although multiple studies show that patients with mental disorders have a higher number of antisocial behaviors compared to individuals without mental disorders, they are unjustly socially rejected and stigmatized [13]. The perception of society towards the individuals with mental disorders is fear, anger, disgust, hostility, negative emotional experiences that translate into social discrimination [2]. Also, in contrast, the feelings of stigma are: depression, anxiety, guilt, shame, avoidance, anger, with negative consequences on the quality of life of the patients with mental disorders [14, 15]. Stigma in conjunction with the mental disorder represents a significant barrier to a qualitative mental health care act [5].
Adaptive and social skills of patients with mental disorders are diminished or absent,
resulting in difficulties in having an independent life [16]. Existing prejudices towards patients with mental disorders contribute to their social isolation, generating discrimination and labeling [3]. Also, the existence of a diagnosis of a mental disorder makes it difficult to the individual to be employed [10]. Psychiatric disorders are still topics that are open to be ridiculed. The perception of the media regarding
patients with mental disorders is
exaggerated, and they show the mentally ill individuals to be dangerous, unpredictable [5]. Individuals with certain psychiatric disorders, such as schizophrenia or bipolar disorder, are more stigmatized than the subjects with other psychiatric disorders, such as depression and anxiety [17].
Stigma is frequently associated with
psychiatric disorders, especially
schizophrenia. Thus, an increasing number of patients with schizophrenia face stigma [18, 19], both before and after the mental disorder is formally diagnosed. Thus, before the individual is to be diagnosed with schizophrenia, there is a prodromal phase of a few days, weeks, or months, with symptoms and behaviors such as: weird speech, bizarre preoccupations [20], loss of interest in hygiene, work, appearance and social activities, symptoms that can generate negative interactions between the individual and the society. Thus, the chronic negative interaction generates various types of stigma: social stigmatization, labeling [21], both at onset and during the course of the disease, whether the disorder was formally diagnosed or not [22]. These stereotypes of negative attitudes generate discrimination, ignorance [23, 24] and incorrect beliefs about the diagnosis of schizophrenia [25].
The general public associates dangerousness with schizophrenia, unlike individuals with addictions [8]. Depressive symptoms [26] are commonly associated with low self-esteem and diminished performance in socially stigmatized patients [27].The stigmatization
of the patient with mental disorders can generate negative discrimination with
multiple consequences both in the
and impact for the individual with mental disorders [30, 31].However, some psychiatric disorders such as depression are less stigmatized than schizophrenia; so the risk of external stigma is higher in the latter compared with affective disorders [10].
In Greece, according to some studies, the public has discriminatory attitudes [32], disapproving even of having their legal residence in the vicinity of patients with mental disorders [33].In general, individuals do not want to hire, to live with or to marry people who have a formal diagnosis of a mental disorder or who were hospitalized in a hospital with a psychiatric profile. For a person who has been admitted to a psychiatric hospital, fear of possible stigmatization or discrimination from others in society makes him or her hide, withdraw from society, as a form of protection. Thus, this attitude of avoidance disrupts the possibility of initiating and maintaining relations, with various future consequences such as not getting hired. Researchers show that labeling is often associated with unemployment, discrimination, depression, low self-esteem, loss of revenue [26, 34].
In 2007, in Romania, 9.8% of the individuals with mental disorders are employed, while 84.5% are unemployed or retired. Also in the US, 60-70% of the people with mental disorders would like to work [35], but only 15% of the people suffering from mental disorders are employed [36]. Unemployment creates poverty, erodes self-esteem and leads to discrimination and social isolation, creating fertile ground for the emergence of mental disorders.
In self-stigmatization, the subject is both the accuser and the target. This means that the subjects have an altered perception of themselves, with various consequences, such as diminished self-esteem, and a poor evolutionary prognosis of the psychiatric condition [2]. Thus, in the perception of the patient with mental disorders, a process of
transforming its identity into an
incompetent individual may take place [37]. The individual who was hospitalized in a psychiatric hospital anticipates social rejection, becoming defensive, socially withdrawn, living a complex inner conflict
[38]. The subject with psychiatric disorders who is aware of the disease has a better prognosis in terms of social functioning. But in situations where disease awareness [39] is associated with stigmatization, the social dysfunction is important [40]. Psychiatric medical research has shown the negative consequences of the internalized stigma, especially in patients with severe mental disorders. The internalized stigma of the patient with severe mental disorders, their quality of life, and their self-respect are in a directly proportional relationship [41]. According to some authors, the degree of social interactions, the quality of life, and the decrease of psychiatric symptoms are indicators that are commonly associated with the reduction of self-stigmatization of the mentally disordered patient [42].
Besides social stigma and
self-stigmatization, the phenomenon of stigma by association is common in the families of patients with mental disorders [2]. Stigma by association [9] generally covers all the family members of mentally ill patients, members who are constantly subjected to
psychological tensions. Thus, the
stigmatization process affects not only the person suffering from mental disorders, but those who come in contact with this person are also affected. The patient becomes a burden to family members, and if the patient with the psychiatric disorder is self-stigmatizing himself or herself, the burden increases in intensity [2]. This type of stigma involves the low esteem of the family, fear, anger, distrust, hopelessness and shame. In most cases, this damage brought to the families of the mentally ill patients leads to a lack of support.
Stigma is a risk factor [43] that can be modified by removing avoidant coping strategies [44, 45]. The recovery and social integration method is another approach to
reduce stigma. Thus, reducing the
stigmatization of the mentally disordered patient can be achieved by increasing
employment [46]. The process of
and public debates [3], using television and radio programs [10]. The anti-stigma campaign of 1981-1986 in the UK made using informative materials given to both health professionals and patients had a significant result in reducing the stigma associated with depression in that period [47]. Also, similar anti-stigma campaigns took place in the last few years in Germany and Estonia [49, 50].
Material and Methods
This study is prospective, questionnaire type, applied to the medical personnel involved in the psychiatric care of patients with mental disorders, and it was conducted during July 2012 - July 2013. It had a research population of 217 medical staff members involved in the therapy of patients with psychiatric disorders: psychiatrists, psychologists, general practitioners, clinicians from other specialties, from medical centers in Iasi, Suceava, Botosani, Vaslui (four towns from Romania). The questionnaires include questions related to Mental Health Law, stigma, discrimination, confidentiality and informed consent.
The questionnaires covered all stages from pre-test, review, validation, and to application in their final form. The results were statistically processed for each item, and then the correlations of the answers according to the different characteristics of
the study groups were made. The Cronbach alpha value was 0.730, a value that gives an acceptable result against the threshold of 0.70, which validates the usage of the questionnaire to other categories of doctors and psychologists involved in the monitoring of people with mental disorders.
In the groups of doctors, the analysis of the
frequency distribution based on
specialization highlights the predominance of resident doctors (54%); in the group Other specialties and specialist doctors (66%) from the group general practitioners, while in the
group of psychiatrist homogeneous
distribution stands out regarding the specialization. Applying the Kruskall-Wallis nonparametric inter-group test highlights statistically significant differences between the medical specialties that responded to the questionnaire (Chi-square = 15.22, df = 2, p = 0.001).
Results
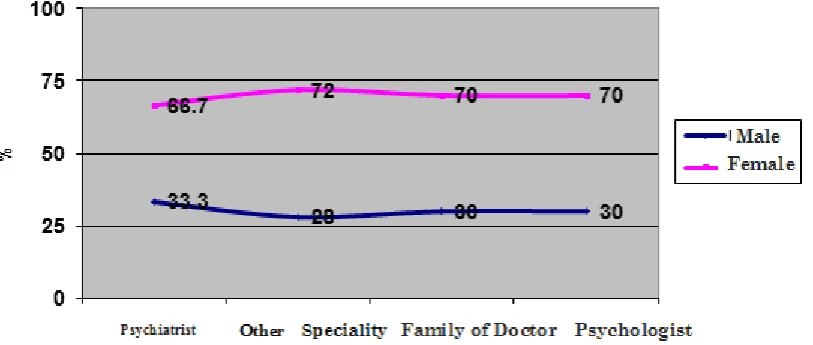
The distribution of the groups according to gender reveals the preponderance of females, sex ratio F / M = 2.3 / 1. The lowest share of women is found in the group of psychiatrists (66.7%), and the peak frequency occurs in the group of physicians
of another specialty but general
practitioners (72%), but the distribution of the frequency does not show significantly differences when compared to the other groups (χ2 = 0.38, df = 3, p = 0.944).
Fig. 1: Structure places sex
According to age groups, a higher share of
Table 1: Batches according to age group
Age group (years)
Psychiatrist another specialty Family of doctor Psychologist
n % n % n % n %
< 30 ani 12 21.1% 16 32.0% 1 2.0% 6 10.0%
30-39 ani 32 56.1% 23 46.0% 23 46.0% 30 50.0%
40-49 ani 4 7.0% 10 20.0% 18 36.0% 23 38.3%
50-59 ani 2 3.5% 7 14.0%
60-69 ani 5 8.8% 1 2.0% 1 2.0% 1 1.7%
70-79 ani 2 3.5%
In the study groups, the distribution by age group reveals statistically significant differences in frequency among the groups surveyed according to the age group (χ2 = 227.14, df = 5, p = 0.001):
In the group of psychiatrists most of the interviewed subjects are found in the 30-39 years range (56.1%) and 12.3% of them are older than 60 years;
In the group of doctors of another specialty the subjects in the age group 30-39 years (46%) are predominant, followed by the age group under 30 (32%);
46% of the general practitioners were aged 30-39 years, while 36% of them are situated in the 40-49 years range; 50% of the psychologists were aged between 30-39 years, and 38.3% in the 40-49 range
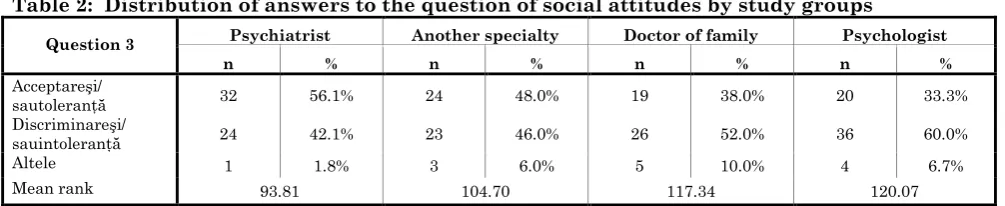
Question: "Do you think that the social attitude in relation to the patient with mental disorders one of:"
Responses to this question revealed statistically significant percentage differences between the study groups (Chi-square = 8.01; df = 3, p = 0.046):
Acceptance and / or tolerance: 56.1% of the
psychiatrists and 48% of the doctors of other specialties, compared to 38% of the general practitioners;
Discrimination and / or intolerance: 60% of the psychologists and 52% of the general practitioners, compared to 42.1% of the psychiatrists and 46% of the doctors of other specialties.
Table 2: Distribution of answers to the question of social attitudes by study groups
Question 3 Psychiatrist Another specialty Doctor of family Psychologist
n % n % n % n %
Acceptareşi/
sautoleranţă 32 56.1% 24 48.0% 19 38.0% 20 33.3%
Discriminareşi/
sauintoleranţă 24 42.1% 23 46.0% 26 52.0% 36 60.0%
Altele 1 1.8% 3 6.0% 5 10.0% 4 6.7%
Mean rank 93.81 104.70 117.34 120.07
Question: "Do you think that the patient with
psychiatric disorders is being discriminated
against, when compared to other patients?"
Responses
to
this
question
revealed
statistically significant percentage differences
between the groups analyzed (Chi-square =
25.63, df = 3, p = 0.001):
The view that the patient with mental
disorders is discriminated in relation to other
patients is found in 93% of the psychiatrists
and 81.7% of the psychologists, while only
52% of the doctors of another specialty and
72% of the general practitioners responded
affirmatively this question;
30% of the doctors of other specialty cannot
appreciate and 18% of them consider that
patients with mental disorders are not
discriminated against in relation to other
patients;
Tabel 3:Distribution of answers to the question of discrimination patient Question 7
Psychiatrist Another specialty Doctor of family Psychologist
n % n % n % n %
Yes 53 93.0% 26 52.0% 36 72.0% 49 81.7%
Not 1 1.8% 9 18.0% 7 14.0% 5 8.3%
I can appreciate 3 5.3% 15 30.0% 7 14.0% 6 10.0%
Mean rank 90.42 135.09 112.25 102.20
Conclusion
In the treatment of the patients with mental disorders, stigma is a major obstacle that
must be overcome. Between the
professionals working in the mental health area and stigma there is a complex relationship in which they can be stigmatized, the ones stigmatizing, and important partners in the fight against stigma. Stigma can be reduced through education, protest, legislative reform; either through the self-management of stigma or
through support. The topic of non-discrimination is an ambitious challenge in Romania, an EU member country, and in the social services, stigma is a major problem in modern psychiatric healthcare.
Acknowledgements
The authors thank AMPOSDRU for supporting their research in this study, conducted within the “Inter-university partnership to improve healthcare quality and interdisciplinary of medical doctoral research by granting doctoral scholar- ships -DocMed.net”, POSDRU/107/1.5/S/78702).
References
1. Surdu L (2010) Mecanismele de
construcţie şi deconstrucţie a
stigmatizării, în cazul romilor din România. Calitatea vieţii, XXI(1-2): 51-70.
2. Pădurariu M, Ciobîrcă A, Persson C, Ştefănescu C (2011) Self-stigma in psychiatry: ethical and bio-psycho-social perspectives. Romanian Journal of Bioethics, 9(1): 76-82.
3. Smith M (2002) Stigma. APT , 8: 317-323.
4. Johnstone MJ (2009) Bioethics: A Nursing Perspective. Elsevier, 5th edition, 184
5. Zalar B, Strbad M, Svab V (2007) Psychiatric education: does it affect stigma? Acad Psychiatry, 31(3): 245-246. 6. Crocker J. Major B, Steele C (1998)
Social stigma. In: Gilbert D, Fiske ST, Lindzey G, editors. The handbook of social psychology. New York: McGraw-Hill, 2: 504–553.
7. Arboleda-Flórez J (2003) Considerations on the stigma of mental illness. Can J Psychiatry, 48(10): 645-650.
8. Gray AJ (2002) Stigma in psychiatry. J R Soc Med, 95(2): 72-76.
9. Stuart, H. (2005) Fighting stigma and discrimination is fighting for mental health. Canadian Public Policy - Analyse de Politiques, 31(Suppl.): 21-28.
10.Suciu R, Ardelean M (2007) O
perspectivă psihiatrică asupra stigmei. Psihiatru.ro, 11: 30-33.
11.Arboleda-Flórez J, Stuart H (2012) From sin to science: fighting the stigmatization of mental illnesses. Can J Psychiatry, 57(8): 457-463.
12.Henderson C, Williams P, Little K, Thornicroft, G (2013) Mental health problems in the workplace: changes in employers’ knowledge, attitudes and practices in England 2006-2010. Br J Psychiatry Suppl, 55: 70-76.
13.Damir D, Toader E (2007) Importanţa expertizei medico-legale în apărarea drepturilor fundamentale ale persoanei. Revista romană de Bioetică, 5(2):78-82. 14.Dinos S, Stevens S, Serfaty M et al
Psychiatry, 184:176-181.
15. Verhaeghe M, Bracke P, Bruynooghe K
(2008) Stigmatization and self-esteem of
persons in recovery from mental illness: the
role of peer support. Int J Soc Psychiatry,
54:206-218.
16.Corrigan PW (2007) How clinical diagnosis might exacerbate the stigma of mental illness. Social Work, 52(1): 31-39. 17.Popa CO, Nirestean A, Ile L, Ardelean
M, Moica T, Buicu G (2013) Community Mental Health Services - The Treatment of Anxiety and Its Effects from the Point of View of the Association of Personality Dimensions. Revista de Cercetare si Interventie Sociala,43:49-60.
18. Lee, S, Chiu, MY, Tsang, A et al. (2006).
Stigmatizing experience and structural
discrimination associated with the treatment of schizophrenia in Hong Kong. Soc Sci Med, 62(7): 1685-1696. 19.Dickerson FB, Sommerville J, Origoni
AE et al. (2002) Experiences of stigma among outpatients with schizophrenia. Schizophr Bull, 28(1):143-155.
20.Janssen I, Hanssen M, Bak M et al. (2003) Discrimination and delusional ideation. Br J. Psychiatry, 182:71-76.
21.Corrigan PW, Wassel A (2008)
Understanding and influencing the stigma of mental illness. J. Psychosoc Nurs Ment Health Serv, 46(1):42-48. 22.Van Zelst C (2009) Stigmatization as an
environmentalrisk in schizophrenia: a userperspective. Schizophr Bull, 35(2): 293-296.
23.Lincoln TM, Arens E, Berger C, Rief W (2008) Can antistigma campaigns be improved? A test of the impact of biogenetic vs psychosocial causal explanations on implicit and explicit attitudes to schizophrenia. Schizophr Bull, 34(5):984-994.
24.Thornicroft G, Rose D, Kassam A, Sartorius N (2007) Stigma: ignorance, prejudice, or discrimination? Br J Psychiatry, 190:192-193.
25.Schulze B (2007) Stigma and mental health professionals: a review of the
Rev Psychiatry, 19(2):137-155.
26.Sirey JA, Bruce ML, Alexopoulos GS (2001) Perceived stigma as a predictor of treatment discontinuation in young and older outpatients with depresion. Am. J. Psychiatry, 158(3):479-481.
27.Yang LH (2007) Application of mental illness stigma theory to Chinese societies: synthesis and new directions. Singapore Med J, 48(11): 977-985.
28.Perlick DA, Rosenheck RA, Clarkin JF (2001) Stigma as a barier to recovery: Adverse effects of perceived stigma on social adaptation of persons diagnosed with bipolar affective disorder. Psychiatr Serv, 52(12):1627-1632.
29.Sartorius N (2006) Lessons from a 10-year global programme against stigma and discrimination because of an illness. Psychol Health Med, 11(3):383-388. 30.Buizza C, Schulze B, Bertocchi E et al.
(2007) The stigma of schizophrenia from patient’s and relative’s view: a pilot study in an Italian rehabilitation residenţial care unit. Clin Pract Epidemol Ment Health, 3:23.
31.González-Torres MA, Oraa R, Arístegui
M et al. (2007) Stigma and
discrimination towards people with schizophrenia and their family members. A qualitative study with focus groups. Soc Psychiatry Psychiatr Epidemiol, 42(1):14-23.
32.Evans-Lacko S, Henderson C,
Thornicroft G (2013) Public knowledge, attitudes and behaviour regarding people with mental illness in England. Br. J. Psychiatry, 55: s51-57.
33.Economou M, Richardson C,
Gramandani C et al. (2009) Knowledge about schizophrenia and attitudes towards people with schizophrenia in Greece. Int. J. Soc. Psychiatry, 55(4): 361-371.
35.Bond GR, Becker DR, Drake, RE et al
(2001) “Implementing supported
employment as an evidence-based practice.” Psychiatric Services, 52(3): 313-322.
36.Crowther RE, Marshall M, Bond GR, Huxley P (2001) “Helping people with serios mental illness obtain work: a systematic review” British Medical Journal, 322(7280):204-208.
37.Yanos PT, Roe D, Markus K, Lzsaker PH (2008) Pathwazs between internalized stigma and outcomes related to recoverz in schizophrenia spectrum disorders. Psychiatr Serv, 59(12):1437-1442.
38.Watson AC, Corringan P, Larson J, Selis EM. (2007) Self-stigma in People with
Mental Illness. Schizoph Bull,
33(6):1312-1318.
39.Cooke M, Peters E, Fannon D et al. (2007) Insight, distress and coping styles in schizophrenia. Schizophr Res, 94(1-3):12-22.
40.Lysaker PH, Roe D, Yanos PT (2007) Toward understanding the insight paradox: internalized stigma moderates the association between insight and social functioning, hope, and self-esteem
among people with schizophrenia
spectrum disorders. Schizophr Bull, 33:192-199.
41.Mashiach-Eizenberg M, Hasson-Ohayon I, Yanos PT et al. (2013)Internalized stigma and quality of life among persons with severe mental illness: The mediating roles of self-esteem and hope. Psychiatry Res, 208(1): 15-20.
42.Resnick SG, Fontana A, Lehman AF, Rosenheck RA (2005) An empirical conceptualization of the recovery orientation. Schizophr Res, 75(1):119-128.
43.Smith ME. (2012). Where has all the stigma gone? Afr J Psychiatry, 15(2): 75-77.
44. Vauth R, Kleim B, Wirtz M, Corrigan PW (2007) Self-efficacy and empowerment as outcomes of self-stigmatizing and coping in schizophrenia. Psychiatry Res, 150:71-80.
45.Ertugrul A, Uluğ B (2004) Perception of
stigma among patients with
schizophrenia. Soc Psychiatry Psychiatr Epidemiol, 39(1):73-77.
46.Perkins DV, Raines JA, Tschopp MK, Warner TC (2009) Gainful employment reduces stigma toward people recovering from schizophrenia. Community Ment Health J, 45(3):158-162.
47.Kovac C (2001) Education campaigns can reduce stigma of depression and cut suicides. BMJ, 323(7315):714.
48.Smith M (2013) Anti-stigma campaigns: time to change. Br. J. Psychiatry Supl, 55:49-50.
49.Friedrich B, Evans-Lacko S, London J et al. (2013). Anti-stigma training for medical students: the Education Not Discrimination project. Br J Psychiatry, 202 (suppl 55): s89–94.
50.Evans-Lacko S, Henderson C,
Thornicroft G, McCrone P.