LIMITED SUPERVISION STATUTE IN NORTH CAROLINA: KNOWLEDGE, OPINIONS, AND
UTILIZATION
Jehan Mohammed Alalkami
A thesis submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science (Dental Hygiene Education)
Department of periodontology in the Adams School of Dentistry.
Chapel Hill 2019
Approved by:
Jennifer Brame
Lewis N. Lampiris
Lattice D. Sams
© 2019
ABSTRACT
Jehan Mohammed Alalkami: Limited Supervision Statute in North Carolina: Knowledge, Opinions, and Utilization
(Under the direction of Jennifer Brame)
The North Carolina Dental Hygiene Limited Supervision Statute (DHLS) was created to allow
dental hygienists (DH) to provide care without direct supervision. No data shows effectiveness,
utilization or awareness of DHLS. Study aims included evaluation of utilization, knowledge, and opinions
of DHLS.
Mixed-methods study design included a report showing number, type, and location of services.
Surveys distributed to DH attending a continuing education course. Responses were analyzed using
descriptive statistics and chi-square.
Data showed average of 11 dentists annually utilizing DHLS for various services between 2008-
2016. Surveys completed by 115 DH. Data revealed 80% (N=88) wanted to utilize DHLS, 96% (N=109)
wanted to learn more. Most respondents lacked knowledge of allowable procedures and requirements.
Qualitative feedback indicated lack of knowledge, underutilization, and need.DHLS is underutilized in
NC; however, DH indicate a willingness to learn and utilize. Increasing knowledge and awareness may
To my mother, Laila AL Nasser, my greatest role model in life. I’m forever grateful for all her love and support she had given me throughout the years.
ACKNOWLEDGEMENTS
The completion of a graduation thesis could not be accomplished without the contributions and
efforts of my thesis committee. To Professor. Jennifer Brame, thank you for the support and guidance
you provided for the past two years. To Ms. Jennifer Harmon and Professor. Lattice Sams for their help
developing my survey questions and working with me on my tables and results. Dr. Lew Lampiris for the
timely feedback and edits. Dr. Philips for advice and statistical support.
I also like to thank NCSBDE’s Chief of Examiners Mr. Bobby White for providing the statistical
report on the Limited Supervision Statute. This project would not have been realized without each and
TABLE OF CONTENTS
LIST OF TABLES……….………..……… viii
LIST OF FIGURES……….……….………... vii
LIST OF ABBRAVIATIONS………..……….……... x
CHAPTER I. INTRODUCTION……….…..……….……… 1
CHAPTER II. REVIEW OF THE LITERATURE……….…..……….…... 4
ACCESS TO CARE IN THE UNITED STATES………..….…………..……….… 4
DENTAL HYGIENE AND SOLVING ACCESS TO CARE FOR THE UNDERSERVED………...………….……… 6
CHAPTER III. INTRODUCTION AND LITREATURE REVIEW……….……….….. 9
CHAPTER IV. METHODS ………..………..………..……….. 12
CHAPTER V. RESULTS …….……….……….……….……. 14
UTILIZATION DATA ……….……….………... 14
SURVEY DATA ……….…... 18
CHAPTER VI. DISCUSSION ……….………..………... 23
STUDY IMPLICATIONS ……….. 28
VHAPTER VII. CONCLUSION……….……….….………..…….…. 29
APPENDIX 1: STATE BOARD LETTER ………..……..……….……….………. 30
APPENDIX 2: STATE BOARD SURVEY……….………..……….………... 32
APPENDIX 3: SURVEY QUESTIONS ……….……….……….. 33
LIST OF FIGURES
Figure 1- North Carolina counties that benefitted from the
Services provided by dental hygienists under DHLS ………..……..………..17
Figure 2- Number of patients in facilities that received oral hygiene care under DHLS
Between 2008-2016 ……….……….………. 16
Figure 3- Demographics of survey respondents………..……….………..……… 20
LIST OF TABLES
Table 1 Dent al Hygiene Limited Supervision (DHLS) ……….…. 3
Table 2 Number of dentists who utilized DHLS in North Carolina between 2008 to 2016 compared to the total number
Of actively licensed dentists in North Carolina………. 15
Table 3 Types of services that were reported to have been performed by the limited supervision hygienists in North Carolina from
The year 2008 to 2016………..……… 15
Table 4 Respondents knowledge of DHLS allowable procedures and
Requirements ……….……….………. 20
Table 5 Major themes and corresponding quotes from qualitative survey
LIST OF ABBREVIATIONS
ADA American Dental association
ADHA American Dental Hygiene Association
CE Continuing Education
DDS Dentist
DH Dental Hygienist
DHLS Dental Hygiene Limited Supervision
IRB Institutional Review Board
NC North Carolina
NCSBDE North Carolina State Board of Dental Examiners
CHAPTER I: INTRODUCTION
For underserved populations in the United States, access to oral health care has been an
ongoing issue. 1 In an effort to combat this, several states established policies that expand the role of
dental hygienists, in order to improve access to oral health care and to eliminate health disparities. 2
In 2007 the Limited Supervision Statute was introduced into NC’s State Practice Act.2 This
provision allowed dental hygienists the ability to deliver preventive services for various facilities
including senior homes and state clinics, under indirect supervision, with specific conditions (Table 1).3
For example, the hygienist chosen would have to be identified, the licensed dentist would have to
evaluate the patient and create a specific treatment plan which would have to be followed and
conducted by the hygienist within 120 days.2 The Limited Supervision Statute was passed as a solution
for the lack of access to oral care for the underserved population.2 However, according to the North
Carolina Oral Health Collaborative, the Limited Supervision Statute is “underutilized “in terms of access
to care.4 Limited supervision has been enacted for almost a decade now; however, there is no reported
data demonstrating utilization, outcomes, knowledge, or attitudes by NC dentists and dental hygienists.
There are also no studies assessing how this statute is helping solve access to dental care for the
underserved population of NC. But an example of a similar law was found in the State of Oregon.
In 1997, the state of Oregon enacted a law to allow dental hygienists to obtain a “Limited access
Permit” which allows dental hygienists to provide clinical and educational hygiene services to
public schools.2,5,6 Battrell et al. (2007) published a qualitative study that was done in Oregon to assess
the effectiveness of the limited access permit legislation on public access to oral health care. Although
the study concluded that it was too early to measure any effect of the law on access to oral care in the
state, Battrell et al. reported that limited access permit hygienists are providing their services through
promoting prevention through community-based programs, providing clinical and preventive
procedures, and collaborative health care delivery.5 Research needs to be done to investigate the
number of dental hygienists who are utilizing the limited supervision law and the type of services that
are provided. We undertook this mixed-methods study with the following aims: 1) to investigate the
exact number of dentists who are utilizing “Limited Supervision Statute” in North Carolina, 2) the types
of services provided by the dental hygienists, 3) whether the Limited Supervision Statute has helped
with the issue of access to oral care in North Carolina, and 3) the level of knowledge and opinions of
CHAPTER II: REVIEW OF THE LITERATURE
Access to care in the United States
Access to dental care in the United States (U.S.) is multifactorial and impacted by variants
including, age, ethnicity, socioeconomic status, and geography.8 One supporting study indicated that
African Americans and Hispanics have less access and utilization of dental care compared with white
Americans.9 Wu et.al reported that for senior adults, white Americans have 7.3 filled teeth, African
Americans had 2.7 and Hispanics 4.7 filled teeth.9 Wu et al. also added that number of caries and
missing teeth were found to be higher in Hispanics and African Americans than white Americans.9 In
addition, studies that had investigated the relationship between income and access to care reported
that low income families lack access to dental preventive services and therefore, have higher
percentages of dental diseases that could be preventable.8,10 In addition, dental care cost is one of
access to care barrier for the senior adults.8 People who live in rural areas face more challenges
accessing to oral care more than those living in urban areas.11
Access to receiving dental care is also influenced by the number of oral health care providers.
While conflicting reports exist, one shows an insufficient number of dentists available to serve the
constantly growing population.12 Mertz et.al have predicted that in the year 2020 there will be 52.7
dentists per 100.000 people in US.12 Contrary to this prediction, the American Dental Association (ADA)
reported that the number of dentists has in fact increased in 2018 to 60.97 dentists per 100.000 people.
This could indicate an increasing trend for the coming years.13 However, the distribution of oral health
care providers does have a major impact on access to care. In rural parts of US, the insufficient number
of dentists practicing in these areas is one of the major barrier to access to care.14, 15, 16
and Services Administration (HRSA), the dentist to population ratio in urban areas is 5.9 for every
10.000, while in rural areas the ratio is 3.6 for every 10.000 rural resident.17 The National Rural Health
Association recommended to the upcoming Surgeon General Report on Oral Health 2020, for an action
to solve access to care for the underserved population living in rural parts of US, by putting a focus on
efforts to increase recruitment for dental professionals to practice in underserved rural areas.11 This
recommendation is timely with a recent study indicating that in rural North Carolina (NC), senior adults
who had natural teeth reported not having routine dental care while irregular dental visits and no dental
visits at all was reported by edentulous senior adults.12 Moreover, more than one third of teenagers
living in rural areas did not receive regular dental services. And approximately 25% of rural teenagers
reported having unmet dental needs. A call for more preventive measures to address these factors are
many throughout the literature.14,20
Dental access to care for assisted living facilities and nursing homes residents is another
prevalent issue.21 Of one study aimed to assess the effectiveness of inter-professional collaboration
between nursing and dental hygiene students to perform screening and assessing nursing-homes
residents’ oral status.22 Results from this study demonstrated that the rural nursing home had a higher
number of lost teeth and poor oral health in general, than the residents of the urban facility.22 A
statewide survey of assisted living facilities in NC showed that 80% of these facilities across the state
Dental Hygienists and Solving Access to Care for the Underserved
Studies have investigated multiple approaches to address access to care disparities in the
US.25,26,27 With the ratio of dental hygienists to population (in 2010, 4.5 per 10.000 in rural areas)
exceeding the dentist to population ratio (in 2010, 3.6 per 10.000 in rural areas),17 it was crucial to utilize
preventive services that are provided by dental hygienists to improve the underserved population’s
dental care status. Dental hygienists have been utilized to minimize the gap of access to care especially
in states supportive dental hygiene Practice Acts.25 Stull et.al discussed the benefits of increasing access
to dental hygiene services for the underserved especially in rural and remote areas in the US. One of the
benefits discussed is the increase in accessibility to preventive services and therefore, reducing
preventable dental diseases like tooth decay and periodontal infections. Adding that, the restrictive
dental hygiene scope of practice is a barrier that needs to be addressed. Stull et al. concluded that a
change in dental hygiene practice laws will help increase access to dental care for the underserved.28
Dental hygiene scope of practice is different in each state,29 these differences allows for more
comparisons to be made between them.
Many states have created new approaches to utilizing dental hygienists to better serve
populations with low access to dental care. In California, Health Manpower Pilot Project (HMPP) was
initiated in 1987, this project aimed to increase access to care by expanding the scope of practice for
health professionals.30 In 1991, and after three years of testing this practice model, this project
concluded that under indirect supervision of a dentist, dental hygienists are capable of providing
preventive and therapeutic services for the underserved. Consequently, Registered Dental Hygienists in
Alternative Practice “RDHAP” was passed in California in 1998. RDHAP enabled underserved and special
need patients to have a direct access to dental hygiene services and created a collaborative
environment between the hygienist and dentist through referrals, to connect the underserved with the
license that authorized dental hygienists under certain requirements, and a limited supervision, to serve
patients with limited or no access to care. The act was then replaced in 2001 with Expanded Practice
Dental Hygienists (EPDH) that allowed dental hygienists to gain more freedom to practice without
supervision.25 Fourteen years after its enactment, Bell et.al investigated the effect of EPDH on dental
care disparities in Oregon and concluded that EPDH had significantly decreased dental care disparity in
the state.31
One study aimed to review practices in four states’ “California, Florida, North Carolina, and
Minnesota” regarding delivery of care to long-term care facilities. Results from this study concluded that
when with practice laws, the elderly and special needs patients are the ones that most affected by the
restrictions, especially the ones that are limiting dental hygienists’ scope of practice.32
To address access of care limitations in NC, the Limited Supervision Dental Hygiene (LSDH)
statute was passed in 2007, to allow dental hygienists to provide care in remote settings. In the NC
Practice Act, dental hygienists must work under the direct control and supervision of a dentist, with no
more than two dental hygienists for each dentist actively engaged in the practice of dentistry. Under this
statute, a dentist can send their dental hygienist complete prescribed care for patients in long-term care
facilities, nursing homes, state/federal clinics, correctional institutions, and hospitals. There is no special
certificate nor a license to be obtained in order for the dental hygienist to see patients under this
statute. However, certain requirements have to be met by both the dentist and the dental hygienist. The
dental hygienist has to complete at least three years, or 2000 hours, of clinical experience working
under direct supervision of a dentist, complete 5 hours of CE courses, complete CPR training. The dentist
is required to submit an annual report to the NC Board of Dental Examiners with information about the
number of patients who received hygiene services, type/number of locations and the types and number
Dental access to care disparity is an acknowledged issue in NC. The literature supports
longstanding and consistent barriers that negatively impact patients receiving dental care.10,16,19
Utilization of dental hygienists to reach for the unreserved and provide preventive services for the
special needs and older patients has been shown efficacious in decreasing this lack of care disparity
among the underserved.28,29,31 Restricted dental hygiene practice acts in NC inhibits utilization for
providing care to those in underserved and rural areas. The DHLS was established to address this need;
however, there is no published data found in the literature regarding the effectiveness of the DHLS
statute in regards to access to care for NC.
Aims of Study
To investigate the number of dentists utilizing the DHLS and the type of services that have been
provided, learn of locations that benefited from the statute in terms of access to care, and to assess
CHAPTER III: INTRODUCTION AND LITERATURE REVIEW
Studies have investigated multiple approaches to address access to care disparities in the
U.S.25,26,27 With the ratio of dental hygienists to population (in 2010, 4.5 per 10.000 in rural areas)
exceeding the dentist to population ratio (in 2010, 3.6 per 10.000 in rural areas),17 it was crucial to utilize
preventive services that are provided by dental hygienists to improve the underserved population’s dental
care status. Dental hygienists have been utilized to minimize the gap of access to care especially in states
supportive dental hygiene Practice Acts.25 Stull et.al discussed the benefits of increasing access to dental
hygiene services for the underserved especially in rural and remote areas in the US. One of the benefits
discussed is the increase in accessibility to preventive services and therefore, reducing preventable dental
diseases like tooth decay and periodontal infections. Adding that, the restrictive dental hygiene scope of
practice is a barrier that needs to be addressed. Stull et al. concluded that a change in dental hygiene
practice laws will help increase access to dental care for the underserved.28
Dental hygiene scope of practice is different in each state,29 these differences allows for more
comparisons to be made between them.
Many states have created new approaches to utilizing dental hygienists to better serve
populations with low access to dental care. In California, Health Manpower Pilot Project (HMPP) was
initiated in 1987, this project aimed to increase access to care by expanding the scope of practice for
health professionals.30 In 1991, and after three years of testing this practice model, this project
concluded that under indirect supervision of a dentist, dental hygienists are capable of providing
Consequently, Registered Dental Hygienists in Alternative Practice “RDHAP” was passed in
California in 1998. RDHAP enabled underserved and special need patients to have a direct access to
dental hygiene services and created a collaborative environment between the hygienist and dentist
through referrals, to connect the underserved with the best dental care for their needs.22 The state of
Oregon enacted the Limited Access Permit in 1997, a license that authorized dental hygienists under
certain requirements, and a limited supervision, to serve patients with limited or no access to care. The
act was then replaced in 2001 with Expanded Practice Dental Hygienists (EPDH) that allowed dental
hygienists to gain more freedom to practice without supervision.25 Fourteen years after its enactment,
Bell et.al investigated the effect of EPDH on dental care disparities in Oregon and concluded that EPDH
had significantly decreased dental care disparity in the state.23
One study aimed to review practices in four states’ “California, Florida, North Carolina, and
Minnesota” regarding delivery of care to long-term care facilities. Results from this study concluded that
when with practice laws, the elderly and special needs patients are the ones that most affected by the
restrictions, especially the ones that are limiting dental hygienists’ scope of practice.32
To address access of care limitations in NC, the Limited Supervision Dental Hygiene (LSDH)
statute was passed in 2007, to allow dental hygienists to provide care in remote settings. In the NC
Practice Act, dental hygienists must work under the direct control and supervision of a dentist, with no
more than two dental hygienists for each dentist actively engaged in the practice of dentistry. Under this
statute, a dentist can send their dental hygienist complete prescribed care for patients in long-term care
facilities, nursing homes, state/federal clinics, correctional institutions, and hospitals. There is no special
certificate nor a license to be obtained in order for the dental hygienist to see patients under this
statute. However, certain requirements have to be met by both the dentist and the dental hygienist. The
dental hygienist has to complete at least three years, or 2000 hours, of clinical experience working
is required to submit an annual report to the NC Board of Dental Examiners with information about the
number of patients who received hygiene services, type/number of locations and the types and number
of services that were provided at each location.
Dental access to care disparity is an acknowledged issue in NC. The literature supports
longstanding and consistent barriers that negatively impact patients receiving dental care.10,16,19,17
Utilization of dental hygienists to reach for the unreserved and provide preventive services for the
special needs and older patients has been shown efficacious in decreasing this lack of care disparity
among the underserved.28,29,31 Restricted dental hygiene practice acts in NC inhibits utilization for
providing care to those in underserved and rural areas. The DHLS was established to address this need;
however, there is no published data found in the literature regarding the effectiveness of the DHLS
statute in regards to access to care for NC. We undertook this mixed-methods study with the following
aims: 1) to investigate the exact number of dentists who are utilizing “Limited Supervision Statute” in
North Carolina, 2) the types of services provided by the dental hygienists and locations that benefited
from the statute in terms of access to care 4) whether the DHLS has helped with the issue of access to
oral care in North Carolina, and 3) the level of knowledge and opinions of dental hygienists in North
CHAPTER IV: METHODS
This study was reviewed by the University of North Carolina Institutional Review Board and was
determined to be exempt. A mixed-methods study design was used, involving quantitative evaluation of
the utilization of limited supervision provision and qualitative analysis to gain perspectives on
knowledge and opinions of dental hygienists regarding the statute. To address the aims of the study, a
publicly available statistical report on the utilization of limited supervision dental hygienists from 2008
to 2016 was obtained from the North Carolina State Board of Dental Examiners [NCSBDE]. The
information was collected by the State Board using an annual survey questionnaire completed by
dentists during the required license renewal process.
Additional information related to the North Carolina Dental Hygiene Limited Supervision Statute
[DHLS] was collected utilizing a survey design with a convenience sample of dental hygienists attending
a continuing education course in April 2018. A survey was developed to assess knowledge, attitudes,
and opinions from dental hygienists. The survey was piloted with three dental hygienists and one dentist
to ensure content validity. The survey consisted of 19 items in three primary domains: 1) close-ended
items to gather demographic information such as gender, age, current profession, years of practice, and
place/ type of practice; 2) Likert scale questions to assess participants’ knowledge and willingness to
utilize the Limited Supervision; and 3) open-ended items to gather participant’s comments and opinion
Hygiene Limited Supervision [DHLS] Act. Surveys were transferred to a Teleform TM (HP Autonomy)
paper design and transfer of answers was completed by electronic scanning to ensure continuity and
accuracy.
The survey was distributed to a convenience sample of dental hygienists who attended the
Annual Dental Hygiene Continuing Education Lecture at the Friday Center in Chapel Hill, NC. An
invitation to participate was given by the event speaker who explained the importance and purpose of
the study using an informed consent script. Participants were informed that survey responses would be
anonymous and confidential. Surveys were distributed following the announcement and returned
voluntarily. Inclusion criteria included dental hygienists who were currently licensed in North Carolina.
The primary outcome variable was the utilization of the limited supervision statute, types of
services performed, and locations between 2008-2016.Discriptive statistics on the utilization was done
by the State’s Board of Dental Examiners. Secondary outcomes included dental hygienists’ level of
knowledge and willingness Descriptive statistics such as frequency distributions and percentages were
used to analyze data. Chi-square analysis was used to assess whether the proportion of dental
hygienists, based on their age, time in practice, and organization affiliation, differed in their level of
knowledge and/or willingness regarding limited supervision. The level of significance was set at p<0.05
CHAPTER V: RESULTS
Utilization Data
Utilization data was obtained from the North Carolina State Board of Dental Examiners
(NCSBDE). As part of DHLS requirements, dentists who employ dental hygienists to practice under
limited supervision are required to annually report to the state board, number and type of location
those hygienists provided services in under this statute, as well as the number of patients and the type
of services these patients received. The state board mails a letter and a survey instrument to the
dentists who reported using DHLS in the previous year. This letter briefly explains what dental hygiene
limited supervision statute is and asks to report the information needed in the survey and mail it back.
In an analysis of utilization data from 2008-2016, there was an average of 11 practicing dentists
in North Carolina (NC) per year utilizing DHLS (Table 2). Although the report did not reveal the number
of DH performing preventive services, this study found that DH provided a variety of services through
the DHLS (Table 3). During this nine-year period, oral prophylaxis was identified as the highest service
According to the utilization data report, four unique settings were identified as sites where
specific services were provided between 2008 and 2016 (Figure 2). In the first year (2008) of DHLS, 47%
of the services were provided at a hospital facility, 32% at a nursing home/ long-term care facility, and
20.8% at a non-profit community clinic (Figure 2). During 2016, 46% of services were delivered at a
correctional institution. Surprisingly, there was a significant decline in the services performed in nursing
homes (29%) and hospitals (35%) in 2016 (Figure 2).
0 500 1000 1500 2000 2500 3000 3500 4000 4500 5000
2008 2009 2010 2011 2012 2013 2014 2015 2016
2008 2009 2010 2011 2012 2013 2014 2015 2016
Nursing homes/assisted living/long
term care facilities 123 897 495 1,165 671 763 515 2,940 28
Hospitals 181 25 137 159 33 36 0 0 74
State/federal/county clinics 0 55 0 63 171 63 552 117 185
non-profit community clinics 80 10 134 87 0 0 92 37 82
Correctional institutions 0 0 0 1800 1550 1500 0 1500 320
Figure 2. Number of patients in facilities that recieved
oral hygiene care under DHLS between 2008-2016
Nursing homes/assisted living/long term care facilities Hospitals
State/federal/county clinics non-profit community clinics
Findings showed that services between 2008 to 2016 were provided in many regions across NC.
DHLS was utilized in most regions across the state. Figure two illustrates services rendered by various
regions. The analysis also revealed that a small number of practitioners utilized DHLS in the coastal
region, with only four counties participating in DHLS care. In this region between 2008 and 2015. From
Survey Data
Of the 175 surveys distributed only 115 were completed for a response rate of 65%. Data
revealed that a majority of the sample (34 %) had been practicing for 26-35 years, followed by 27% that
had practiced for 6-15 years (Figure 3). Over two thirds of the respondents (70%) were employed in
private practice, and 17% practiced in an educational setting. Approximately one third of the
respondents (31%) indicated that they were only affiliated with the American Dental Hygiene
Association (ADHA). In addition, 4% reported that they were affiliated with other professional
organization in addition to their affiliation with ADHA (Figure 3).
The majority of participant responses indicated a lack of understanding for the services
allowable by a DH under the DHLS. When participants were asked if DHs could provide sealants and
apply fluoride to school children under the limited supervision statute requirements, 90% (n=103)
answered incorrectly (Table 4). Seventy-five percent (n=85) of participants believed that in order for a
DH to practice using the DHLS a certification of expanded functions training and an active license were
required.
Survey questions also sought to obtain participant levels of knowledge regarding policy and
requirements to practice using DHLS. Only 25% knew that a special certification was not needed to
practice under the DHLS. Although 59% (n=67) of participants had knowledge regarding the
performance of clinical procedures without the direct supervision of a dentist under DHLS, 41% of
respondents lacked knowledge of this component of the statute. Additionally, only 76% indicated
knowledge that the employing dentist must provide an annual report of utilization to the NC Board of
Eighty-one percent of the respondents answered correctly that a dentist must complete an
initial exam prior to sending their employing hygienist to provide preventive care under the DHLS. A
majority of respondents (87%) agreed that DHLS can help solve access to care in North Carolina. In fact,
one participant stated, “I feel as though more patients will have access to care with limited supervision
statute in place”. Another commented, “I think this is great for the hygienists to be able to provide care
to more people especially in rural areas or in places with limited chances to access to care”. (Table 5).
Findings also show that a small percentage (12.5%) disagreed with the statement. In addition, the vast
majority of respondents (99%, n=113) agreed that it is important for DH and dentists to learn about
DHLS (Figure 3). While, 96% (n=109) of participants felt that they wanted to learn more about the
statute, only 80% (n=88) wanted to utilize the DHLS to practice in NC (Figure 3). Thirty-seven percent
(n=42) of respondents indicated that they wanted to obtain more knowledge regarding DHLS through
journal articles, continuing education courses, educational curriculum, and professional organizations.
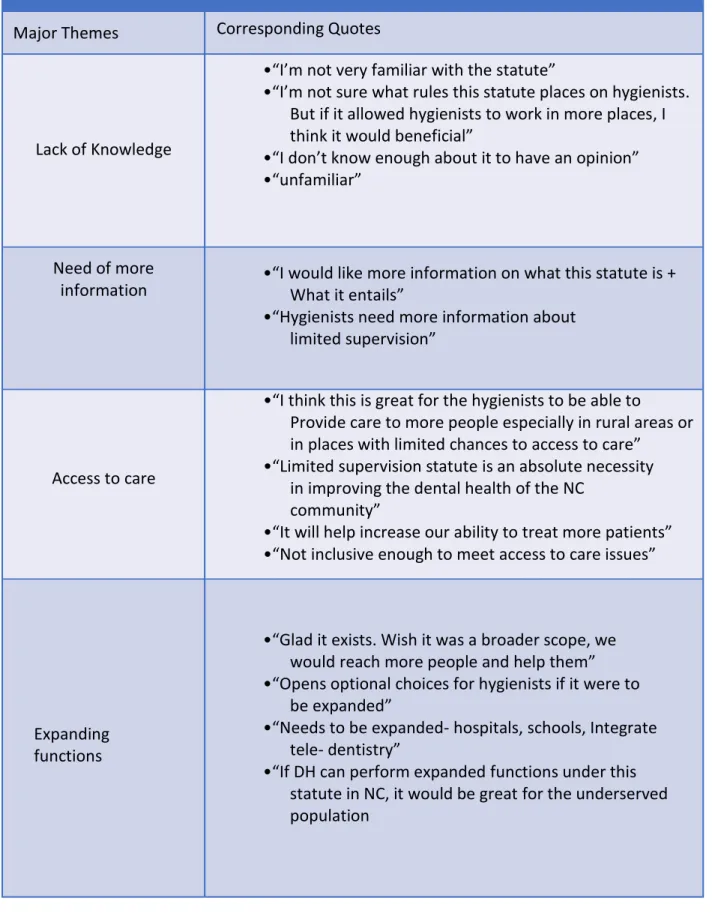
The qualitative feedback received showed four common themes (Table 5). Some of those
comments included:
“I’m not familiar with the statute of limited supervision. If DH can perform expanded functions under this statute in NC, it would be great for the underserved population”
“I’m not sure what rules this statute places on hygienists but if it allowed hygienists to work in more places I think it would beneficial”
Table 5. Major themes and corresponding quotes from qualitative survey items
Major Themes Corresponding Quotes
Lack of Knowledge
•“I’m not very familiar with the statute”
•“I’m not sure what rules this statute places on hygienists.
But if it allowed hygienists to work in more places, I
think it would beneficial”
•“I don’t know enough about it to have an opinion”
•“unfamiliar”
Need of more
information
•“I would like more information on what this statute is +
What it entails”
•“Hygienists need more information about
limited supervision”
Access to care
•“I think this is great for the hygienists to be able to
Provide care to more people especially in rural areas or
in places with limited chances to access to care”
•“Limited supervision statute is an absolute necessity
in improving the dental health of the NC
community”
•“It will help increase our ability to treat more patients”
•“Not inclusive enough to meet access to care issues”
Expanding
functions
•“Glad it exists. Wish it was a broader scope, we
would reach more people and help them”
•“Opens optional choices for hygienists if it were to
be expanded”
•“Needs to be expanded- hospitals, schools, Integrate
tele- dentistry”
CHAPTER VI: DISCUSSION
The 2000 Surgeon General’s Report on Oral Health in America referred to dental diseases as “a
silent epidemic” that affects the underserved populations especially the elderly and children. The report
also stated that action needs to be made in order to fix inequality in access to dental care. 1 People in
rural areas and elderly residents in assisted living facilities are the most affected by oral health
disparities in the US. Nursing homes residents have a higher need for preventive services in order to
ensure a high quality of life. This need stems from the fact that they are more likely to develop
numerous oral health problems that can lead to a decline in their health and quality of life.21 It was
reported that in 2008, the US had 15,728 long-term care facilities. With increasing number of older
populations along the years, dental needs will grow as will their need for access to dental care.21
To increase access to care for underserved populations, different states have made an effort to
increase access to dental hygienists, especially for rural areas where shortage of dentists, travel
distances, and transportation are a barrier to seek dental care.29 According to the National Center for
Health Workforce analysis report titled “National and State-Level Projections of Dentists and Dental
Hygienists in the U.S between 2012-2025”, it is estimated that the increase in practicing dentists will not
be sufficient to the rise in dental needs. On the other hand, dental hygienists increases are expected to
In Oregon, dental hygienists provided preventive care for the unreserved without the direct
supervision of an attending dentist since 1997 when the “Limited access permit” was placed. Then in
2008, an Expanded Practice Dental Hygienists practice model was introduced where hygienists can treat
limited access patients and is positively impacting access to dental care for the underserved.
In California, the tele-dentistry practice model provided limited access patients with the
appropriate level. It utilizes dental hygienists and other dental professionals to perform screening and
take the necessary radiographs, then sending those findings to the dentist through online software, to
diagnose and develop treatment plans.34 This innovative health delivery model is relatively new but it
encourages and emphasizes the dental hygienist’s role as a part of the oral health care team to improve
dental access to care. Other states like Washington DC, Alaska, and Arkansas had a more progressive
laws and allowed for a direct access to dental hygiene services.
In North Carolina, 75% rural senior citizens, reported in 2011 that they don’t visit the dentist
regularly.19 In an effort to combat access to care issues in NC, the DHLS act was created and
implemented in 2007 (Table 1). While the statute’s purpose was to create new pathways of providing
preventive care to patients with limited availability of care, its impact on access to care in NC since its
inception is still unclear. Our first objective in this study is to evaluate the utilization of DHLS in NC. All
data collected by the state dental board was obtained and reviewed to evaluate the number of dentists
using this practice model, type and location of facilities and to investigate the type and number of
services provided.
Results show that for the time period 2008-2016, utilization of the statute was less than 1% of
the total number of licensed dentists in NC (Table 2). This finding confirms the North Carolina Oral
health collaborative statement about DHLS being underutilized9. For the first year “2008”, out of 4,080
That year were provided at hospitals and nursing homes (Table1) (Figure2). Prophylaxis was the only
provided service reported that year (Table 3). Given that it was the first year this statute has taken into
effect; the number was not very surprising.
Study authors noted an increase in the number of dentists’ utilization in the years 2010, 2011,
2012, 2013 (number of dentists was 17, 16, 13, and 15 respectively) (Table 2) This increase could be
linked to the report published by the Special Care Dentistry Advisory Group in 2010. This group was a
collaboration between the Division of Medical Assistance, Division of Public Health, and Division of Aging
and Adult Services in the Department of Health and Human and the University of North Carolina at
Chapel Hill, the East Carolina University Schools of Dentistry, and the North Carolina Dental Society to
assess the oral health status for special care populations. The report was presented to the North
Carolina Study Commission on Aging and the Public Health Study Commission.35 Their report had sixteen
recommendations to help better the access to dental care for the underserved. Defining the special care
population as “those with intellectual and/or developmental disabilities, the frail elderly, those with
multiple complex medical diagnoses, and the many other individuals with disabilities who do not fit into
these categories but also encounter barriers when trying to access dental care in their community”.35
Although this report has acknowledged the issue with access to dental care for this population and the
need for immediate action, recommendations did not mention the limited supervision statute and the
importance of utilizing dental hygienists to provide periodic preventive treatments for the special care
patients. However, the increase in number of dentists who utilized DHLS in the same year of publishing
the report and the following years may have been caused by the report findings.
As for the number of services provided in 2015, eleven dentists reported utilization out of 4,893
(0.22%) (Table 2). That year, assisted home livings and correctional institutions were the most frequent
locations where services were reported (Figure 2). Yet, there were counties like Hartford, Berte, Halifax,
Many counties were found to not benefit from DHLS (Figure 1). There were minimum/no reports of
DHLS utilization along the coastal plain and parts of the Piedmont region (Figure 1). A 2017 statewide
survey showed that, nursing homes and long-term care facilities in these areas had a higher need for
access to dental care. 17
Total number of services reported to have been performed showed that SRPs and periodontal
maintenance were the least to have been provided (Table 3). This may be due to the fact dental
hygienists in North Carolina are not permitted to administer local anesthesia. This restriction and the
absence of an attending dentist to administer the injection at the time of the hygiene appointment,
could be factors that influenced the low number of these procedures. It is interestingly to note the
significant decline in number of services provided in nursing homes (29%) and hospitals (35%) in 2016
(Figure 2). This decline could be attributed to retired dentist(s) or hygienist(s), which led to the
significant decline in number of patients treated during that year.
The qualitative part of the survey provided a clearer indication on what NC dental hygienists felt
about DHLS. Answers generated three main themes, lack of knowledge, call for expanded function, and
A call for more CE courses and educational material regarding the statute (table 4). One of the
respondents wrote: “I’m not aware of the limited supervision statute. I think this is great for the
hygienists to be able to provide care to more people especially in rural areas or in places with limited
chances to access to care”
Lack of knowledge among NC dentists about DHLS was evident from the number of dentists –
with an average of 37 per year- who incorrectly responded with ”yes”, when asked if they have utilized
DHLS, during their annual license renewal, then corrected their response with “no” in the follow-up
Efforts to provide more information about the statute and to encourage the use of the DHLS in order to
serve its original purpose.
The second objective of the study was to survey dental hygienists regarding their knowledge,
attitude and willingness to implement DHLS. Survey results showed that the majority of participants had
no knowledge about DHLS. Since professional organizations like ADHA and ADA should have a role in
advocating and providing information about state boards legislations and rules; it was very important to
ask the participants about their professional affiliation (Table 5). When we analyzed participant’s
characteristics and their knowledge, although more than one-third of the participants were affiliated
with ADHA (32%), a high number of the respondents (75%) did not know that a special permit is not
needed for a DH in order to work under limited supervision in NC.
It was interesting to note that comments yielded from respondents showed positive attitude
and willingness to utilize DHLS despite the lack of knowledge. One respondent mentioned the positive
potentials DHLS would have on access to care, if it gave dental hygienists more expanded function: “I’m
not familiar with the statute of limited supervision. If DH can perform expanded functions under this
statute in NC, it would be great for the underserved population “another respondent pointed out that 2
dental hygienists to 1 dentist ratio can be a barrier for implementation: “Too restrictive. If DDS has one
RDH in nursing home, they must count the RDH as one of his 1:2 DDS: RDH ratio. Needs to be expanded-
Hospitals, schools, Integrate tele-dentistry”.
Limitations from the current study included the NC State Board’s source of DHLS utilization
information begin dependent on the dentists’ self-reporting through the licensure renewal survey
instrument mailed to NC dentists. Therefore, incorrect reporting of services or locations could occur.
Another limitation is that the qualitative portion of our study was done with a convenience sample of
dental hygienists who were attending a CE course. Therefore, it is not possible to make broad
Study Implications:
DHLS need to be included into the dental and dental hygiene curricula to encourage future
utilization of the statute, professional organizations must take a leading role to publish articles and offer
continuing educations courses on DHLS requirements and other updates on access to care status in the
state. By increasing knowledge, statute’s use will positively impact access to care among the
CHAPTER VII: CONCLUSION
Approximately 99% of the dentists in NC reported that they did not utilize or have never utilized
dental hygienists under the limited supervision. However, if utilized properly, DHLS may improve access
to dental care for the underserved population in rural areas across NC. It would enable dental hygienists
to provide prophylactic treatment to patients in places like nursing homes and long-term care facilities,
where transportation costs and travel distance are barriers to accessing care. In addition, efforts to
reduce barriers like DDS and DH lack of knowledge about DHLS by providing information and
encouraging more utilization of the statute across NC using CE courses, journal articles, and through
REFERENCES
1. Oral Health in America: A Report of the Surgeon General (Executive Summary). Available at: https://www.nidcr.nih.gov/DataStatistics/SurgeonGeneral/Report/ExecutiveSummary.htm. Accessed December 3, 2017.
2. US Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General—Executive Summary. Rockville, MD: National Institute of Dental and Craniofacial Research; 2000.
3. American Dental Hygienists Association. Direct Access | ADHA. Available at: http://www.adha.org/direct-access. Accessed December 2, 2017.
4. Limited Supervision Rules | North Carolina Dental Hygienists’ Association. Available at: https://www.ncdha.org/limited-supervision-rules/. Accessed December 2, 2017.
5. North Carolina Oral Health Collaborative. Available at: https://www.oralhealthnc.org/. Accessed December 4, 2017.
6. Battrell AM, Gadbury-Amyot CC, Overman PR. A qualitative study of limited access permit dental hygienists in Oregon. J Dent Educ 2008; 72(3):329-343.
7. Board of Dentistry Hygienist Licensing. Available at:
http://www.oregon.gov/Dentistry/Pages/licenses_hygienist.aspx. Accessed December 4, 2017
8. Edelstein, B.L. and Chinn, C.H. 2009. Update on disparities in oral health and access to dental care for America’s children. Academic pediatrics 9(6), pp. 415–419.
9. Wu, B., Liang, J., Plassman, B.L., Remle, R.C. and Bai, L. 2011. Oral health among white, black, and Mexican-American elders: an examination of edentulism and dental caries. Journal of public health
dentistry 71(4), pp. 308–317.
10. Kenney, G.M., McFeeters, J.R. and Yee, J.Y. 2005. Preventive dental care and unmet dental needs among low-income children. American Journal of Public Health 95(8), pp. 1360–1366.
11. Caldwell, J.T., Ford, C.L., Wallace, S.P., Wang, M.C. and Takahashi, L.M. 2016. Intersection of living in a rural versus urban area and race/ethnicity in explaining access to health care in the United States. American Journal of Public Health 106(8), pp. 1463–1469.
12. Mertz, E. and O’Neil, E. 2002. The Growing Challenge of Providing Oral Health Care Services to All Americans. Health affairs 21(5), pp. 65–77. Available at:
13. Munson, B. and Vujicic, M. 2018. HPI Research Brief - Supply of Full-Time Equivalent Dentists in the US Expected to Increase SteadilySupply of Full-Time Equivalent Dentists in the U.S. Expected to IncreaseSteadily[Online].Available at:
https://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_0718_1.pdf?la= en [Accessed: 22 March 2019].
14. Skillman, S.M., Doescher, M.P., Mouradian, W.E. and Brunson, D.K. 2010. The challenge to delivering oral health services in rural America. Journal of public health dentistry 70 Suppl 1, pp. S49-57.
15. Allison, R.A. and Manski, R.J. 2007. The supply of dentists and access to care in rural Kansas.
The Journal of rural health : official journal of the American Rural Health Association and the National Rural Health Care Association 23(3), pp. 198–206.
16. Douthit, N., Kiv, S., Dwolatzky, T. and Biswas, S. 2015. Exposing some important barriers to health care access in the rural USA. Public Health 129(6), pp. 611–620.
17. National Center for Health Workforce Analysis 2014. NCHWA Fact Sheet: Distribution of U.S. Health Care Providers Residing in Rural and Urban Areas. . Available at:
https://bhw.hrsa.gov/sites/default/files/bhw/nchwa/nchwafactsheet.pdf [Accessed: 22 March 2019]
18. Seigel J. 2020 Surgeon General Oral Health Report: NRHA Submits Comments [Internet]. National Rural Health Association . 2019 [cited 2019Mar4]. Available from:
https://www.ruralhealthweb.org/blogs/ruralhealthvoices/january-2019/2020-surgeon-general-oral- health-report-nrha-subm
19. Arcury, T.A., Savoca, M.R., Anderson, A.M., et al. 2012. Dental care utilization among North Carolina rural older adults. Journal of public health dentistry 72(3), pp. 190–197.
20. Dodd, V.J., Logan, H., Brown, C.D., Calderon, A. and Catalanotto, F. 2014. Perceptions of oral health, preventive care, and care-seeking behaviors among rural adolescents. The Journal of school health 84(12), pp. 802–809.
21. Smith, B.J., Ghezzi, E.M., Manz, M.C. and Markova, C.P. 2010. Oral healthcare access and adequacy in alternative long-term care facilities. Special care in dentistry : official publication of the American
Association of Hospital Dentists, the Academy of Dentistry for the Handicapped, and the American Society for Geriatric Dentistry 30(3), pp. 85–94.
22. Jablonski, R.A., Swecker, T., Munro, C., Grap, M.J. and Ligon, M. 2009. Measuring the oral health of nursing home elders. Clinical Nursing Research 18(3), pp. 200–217.
23. Romaszewski, J.K. 2017. The journey to improving access to dental services for individuals in assisted living facilities across north carolina. North Carolina Medical Journal 78(6), pp. 398–401.
26. Innes, N.P.T. and Evans, D.J.P. 2013. Evidence of improved access to dental care with direct access arrangements. Evidence-based dentistry 14(2), pp. 36–37.
27. Fiscella, K., Franks, P., Gold, M.R. and Clancy, C.M. 2000. Inequality in quality: addressing socioeconomic, racial, and ethnic disparities in health care. The Journal of the American Medical
Association 283(19), pp. 2579–2584.
28. Sharon, S.C., Connolly, I.M. and Murphree, K.R. 2005. A review of the literature: the economic impact of preventive dental hygiene services. Journal of dental hygiene : JDH / American Dental
Hygienists’ Association 79(1), p. 11.
29. Catlett, A.V. and Greenlee, R. 2013. A retrospective comparison of dental hygiene supervision changes from 2001 to 2011. Journal of dental hygiene : JDH / American Dental Hygienists’
Association 87(3), pp. 110–117.
30. Coppola, S.L., Furgeson, D., Fontana, M., Kinney, J.S. and Gwozdek, A.E. 2017. Factors Associated with the Economic Sustainability of the Registered Dental Hygienist in Alternative Practice. Journal of
dental hygiene : JDH / American Dental Hygienists’ Association 91(5), pp. 15–25.
31. Bell, K.P. and Coplen, A.E. 2016. Evaluating the impact of expanded practice dental hygienists in oregon: an outcomes assessment. Journal of dental hygiene : JDH / American Dental Hygienists’
Association 90 Suppl 1, pp. 33–41.
32. Mertz, E. and Wildes, C. Evolving Delivery Models for Dental Care Services in Long-Term Care Settings. 4 States Case Studies . Oral Health workforce. Available at:
http://www.oralhealthworkforce.org/webcontent/uploads/2016/03/OHWRC_Long_Term_Care_201 6.pdf [Accessed: 21 March 2019].
33. U.S. Department of Health and Human Services 2015. National and State-Level Projections of Dentists and Dental Hygienists in the U.S., 2012-2025
34. Langelier M, Rodat C, Moore J. Case Studies of 6 Teledentistry Programs: Strategies to Increase Access to General and Specialty Dental Services. Rensselaer, NY: Oral Health Workforce Research Center, Center for Health Workforce Studies, School of Public Health, SUNY Albany; December 2016.
35. Special Care Dentistry Advisory Group Special Care. North Carolina Study Commission On Aging & North Carolina Public Health Study Commission 2010. Oral Health Services A North Carolina
Commitment. Available at: https://ncleg.net/Library/studies/2010/st11825.pdf. Accessed February 2019.
36. Seigel J. 2020 Surgeon General Oral Health Report: NRHA Submits Comments [Internet]. National Rural Health Association . 2019 [cited 2019Mar4]. Available from:
https://www.ruralhealthweb.org/blogs/ruralhealthvoices/january-2019/2020-surgeon-general-oral- health-report-nrha-subm
37. Arcury, T.A., Savoca, M.R., Anderson, A.M., et al. 2012. Dental care utilization among North Carolina rural older adults. Journal of public health dentistry 72(3), pp. 190–197.
84(12), pp. 802–809.
39. Smith, B.J., Ghezzi, E.M., Manz, M.C. and Markova, C.P. 2010. Oral healthcare access and adequacy in alternative long-term care facilities. Special care in dentistry : official publication of the American
Association of Hospital Dentists, the Academy of Dentistry for the Handicapped, and the American Society for Geriatric Dentistry 30(3), pp. 85–94.
40. Jablonski, R.A., Swecker, T., Munro, C., Grap, M.J. and Ligon, M. 2009. Measuring the oral health of nursing home elders. Clinical Nursing Research 18(3), pp. 200–217.
41. Romaszewski, J.K. 2017. The journey to improving access to dental services for individuals in assisted living facilities across north carolina. North Carolina Medical Journal 78(6), pp. 398–401.
42. Schrimshaw, E.W., Siegel, K., Wolfson, N.H., Mitchell, D.A. and Kunzel, C. 2011. Insurance-related barriers to accessing dental care among African American adults with oral health symptoms in Harlem, New York City. American Journal of Public Health 101(8), pp. 1420–1428.
43. Naughton, D.K. 2014. Expanding oral care opportunities: direct access care provided by dental hygienists in the United States. The Journal of Evidence-Based Dental Practice 14 Suppl, p. 171– 82.e1.
44. Innes, N.P.T. and Evans, D.J.P. 2013. Evidence of improved access to dental care with direct access arrangements. Evidence-based dentistry 14(2), pp. 36–37.
45. Fiscella, K., Franks, P., Gold, M.R. and Clancy, C.M. 2000. Inequality in quality: addressing socioeconomic, racial, and ethnic disparities in health care. The Journal of the American Medical
Association 283(19), pp. 2579–2584.
46. Sharon, S.C., Connolly, I.M. and Murphree, K.R. 2005. A review of the literature: the economic impact of preventive dental hygiene services. Journal of dental hygiene : JDH / American Dental
Hygienists’ Association 79(1), p. 11.
47. Catlett, A.V. and Greenlee, R. 2013. A retrospective comparison of dental hygiene supervision changes from 2001 to 2011. Journal of dental hygiene : JDH / American Dental Hygienists’ Association 87(3), pp. 110–117.
48. Coppola, S.L., Furgeson, D., Fontana, M., Kinney, J.S. and Gwozdek, A.E. 2017. Factors Associated with the Economic Sustainability of the Registered Dental Hygienist in Alternative Practice. Journal of
dental hygiene : JDH / American Dental Hygienists’ Association 91(5), pp. 15–25.
49. Bell, K.P. and Coplen, A.E. 2016. Evaluating the impact of expanded practice dental hygienists in oregon: an outcomes assessment. Journal of dental hygiene : JDH / American Dental Hygienists’
Association 90 Suppl 1, pp. 33–41.
50. Mertz, E. and Wildes, C. Evolving Delivery Models for Dental Care Services in Long-Term Care Settings. 4 States Case Studies . Oral Health workforce. Available at: