Vincristine for Successful Treatment of
Steroid-Dependent Infantile
Hemangiomas
Jonathan D. Wasserman, MD, PhDa,b, Sanjay Mahant, MD, MScb,c, Manuel Carcao, MDb,d, Kusiel Perlman, MDa,b, Elena Pope, MD, MScb,c,e
abstract
Infantile hemangiomas (IHs) are common, although systemic therapy has been generally limited to circumstances of potential compromise of vital functions (airway, vision, feeding, or cardiac), risk of disfigurement, or bleeding. IHs have previously been shown to express high levels of type III deiodinase, which catabolizes active thyroid hormone, resulting in a state of severe hypothyroidism, termed“consumptive hypothyroidism.”We describe an infant with diffuse hepatic hemangiomas who developed consumptive
hypothyroidism who was initially treated successfully with systemic
glucocorticoids andb-blockers. Several efforts to wean her medications were unsuccessful. She subsequently developed severe growth restriction and treatment alternatives were sought. Although previously limited to treatment of life-threatening hemangiomas, a trial of vincristine was initiated. She was ultimately weaned from all systemic therapies, with recovery of a normal growth trajectory. This case highlights broader indications for vincristine as a safe and effective systemic therapy for treatment of IHs. It also stresses the importance of close anthropometric monitoring of infants and toddlers receiving glucocorticoid therapy and intervention when growth compromise becomes evident.
Infantile hemangiomas (IHs) are the most common benign vascular tumors in infancy and childhood. They occur in ∼10% of births.1They
characteristically follow a triphasic growth pattern including proliferation, plateau, and involution. Spontaneous resolution is common, and thus treatment is generally limited to those circumstances in which airway, vision, cardiac function, or feeding are compromised or where there is risk of disfigurement or persistent bleeding.
Consumptive hypothyroidism is a rare, albeit potentially morbid complication of IHs. It was initially described by Huang et al2in association with
a critically ill infant with hepatic hemangiomas. The infant required high doses of thyroid hormone replacement
and ultimately succumbed to his illness. Overexpression of type III deiodinase within the hemangioma can result in a profound hypothyroid state. Type III deiodinase catalyzes the inactivation of thyroid hormones by converting biologically active T4 (thyroxine) and T3 (triiodothyronine) to inactive reverse T3 and T2 (diiodothyronine), respectively, via inner-ring deiodination. Subsequent reports of consumptive
hypothyroidism have since been described in the setting of other hepatic and nonhepatic vascular tumors3–6and, more recently, in
gastrointestinal stromal tumors.7
We describe an infant with steroid-dependent, diffuse hepatic
hemangiomas and consumptive
Divisions ofaEndocrinology,cPediatric Medicine, and
dHematology/Oncology, andeSection of Dermatology,
Department of Pediatrics, The Hospital for Sick Children, Toronto, Ontario, Canada; andbDepartment of Pediatrics,
University of Toronto, Toronto, Ontario, Canada
Dr Wasserman participated in clinical data collection and analysis, guided treatment decisions, and drafted the initial manuscript; Drs Mahant, Carcao, Perlman, and Pope participated in clinical data collection and analysis, guided treatment decisions, and critically reviewed and revised the manuscript; and all authors approved thefinal manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-2542
DOI:10.1542/peds.2014-2542 Accepted for publication Feb 19, 2015 Address correspondence to Jonathan D.
Wasserman, MD, PhD, Division of Endocrinology, The Hospital For Sick Children, 555 University Ave, Toronto, ON, M5G 1X8, Canada. E-mail: jonathan. wasserman@sickkids.ca
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
hypothyroidism who, in the course of systemic treatment, developed significant impairment of linear growth. The infant was treated with intravenous vincristine and was successfully weaned from all
medications, achieving a clinically and biochemically euthyroid state, which highlights this therapeutic option as a viable ancillary option for systemic therapy of IHs.
PATIENT PRESENTATION
A 7-week-old girl presented for evaluation of progressive abdominal distension and jaundice. She was the healthy full-term product of an uncomplicated pregnancy.
The family history was negative for endocrinopathies, early or atypical malignancies, hepatic disease, or infectious exposures. Prenatal
serologies were were normal, including negative hepatitis B and HIV titers.
Initial examination was notable for a well-appearing, nondysmorphic white infant with diffuse jaundice. There were no petechiae or ecchymoses. A single 1.5-mm hemangioma on the right palm was noted. She had a normal head and neck examination, no plethora, and a normal size tongue. There was no goiter. Her chest was clear to auscultation, and heart sounds were normal without gallop or murmur. The patient’s abdomen was markedly distended, with the hepatic edge palpable 14 cm below the right costal margin. The spleen was normal. There was no abdominal tenderness, and there were no caput medusae or spider angiomata.
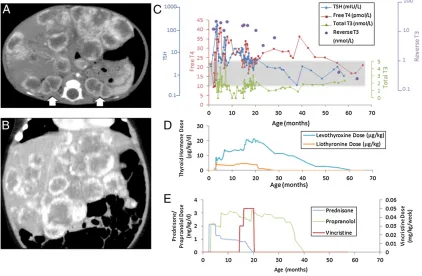
Initial biochemical evaluation revealed cholestasis with normal transaminases. Thyrotropin was 123 mIU/L (0.5–5 mIU/L), free T4 was 9.3 pmol/L (10–23 pmol/L), total
T3 was 0.8 nmol/L (1.6–4.4 nmol/L), and reverse T3 was 15.4 nmol/L (0.12–0.54 nmol/L).a-Fetoprotein was 1473mg/L (40–1000mg/L) and complete blood count was normal. Abdominal ultrasonography and computed tomography revealed diffuse hepatic hemangiomas and a solitary splenic lesion (Fig 1 A and B). There was normalflow through the hepatic vasculature and no obstruction of the biliary system. The provincial newborn screen was reviewed and confirmed to be normal, demonstrating a thyrotropin level of 3.5 mIU/L at 64 hours of life.
On the basis of her significant hypothyroidism and sonographic evidence consistent with multiple hepatic hemangiomas, a presumptive diagnosis of consumptive
hypothyroidism secondary to overproduction of type III deiodinase was established.
FIGURE 1
CLINICAL COURSE
Thyroid replacement was initiated with liothyronine (T3) 1.3mg/kg per day divided twice daily and
prednisone 2 mg/kg per day
(hydrocortisone equivalent: 200 mg/m2 per day). An initial increase in
thyrotropin to 244 mIU/L 3 weeks after initiation of therapy prompted the addition of levothyroxine (T4) at 8.9mg/kg per day and propranolol at 2 mg/kg per day. Within 3 weeks, thyrotropin declined to near-normal levels (thyrotropin = 6.14) and a steroid taper was commenced. Repeat
ultrasound revealed a slight decrease in the size of the hemangiomas. One month after discontinuation of steroid therapy, thyrotropin had rebounded to 71.2 mIU/L, prednisone was resumed, and propanolol increased (Fig 1E). Thyroid replacement was adjusted biweekly to target thyrotropin levels within the reference interval. Levothyroxine replacement reached a maximum dose of 21mg/kg per day and liothyronine reached a maximum of 4mg/kg per day. The initial liver function abnormalities and elevated
a-fetoprotein resolved within 3 months of treatment and remained normal thereafter. Two subsequent attempts to wean glucocorticoids were unsuccessful and the child remained steroid-dependent for the subsequent 12 months.
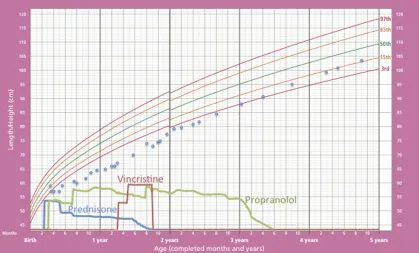
At 14 months, significant growth restriction was noted, with length and weight well below thefirst percentile for age, despite adequate nutrition (Fig 2). Persistent steroid
requirement, high doses of thyroid replacement, and concerns for iatrogenic growth retardation prompted consideration of alternate therapies. The multiple lesions were not amenable to embolization. Although liver transplantation was reported to reverse consumptive hypothyroidism in 2 patients with hepatic hemangiomas,4,8given the
patient’s otherwise excellent functional status and available medical options we elected to pursue nonoperative therapy.
Weekly vincristine infusion was initiated at 14 months at a dose of 0.03 mg/kg per dose. After 7 doses
without biochemical or radiographic response, the dose was escalated to 0.05 mg/kg per dose and continued weekly at this dose for an additional 20 weeks. The child was monitored routinely for adverse effects of vincristine and experienced none. Specifically, there was no peripheral neuropathy, constipation, or cytopenia.
During the course of vincristine therapy, prednisone was successfully weaned completely, whereas
a normal thyrotropin was maintained. The child was gradually weaned from all medications by 5.2 years and remains clinically and biochemically euthyroid after an additional year of follow-up. There was minimal sonographic decrease in the tumor burden at 5 years of age; however, by age 6 the radiographic appearance was consistent with generalized involution as the lesions became more sonographically indistinct from hepatic parenchyma. Growth
retardation resolved after the withdrawal of glucocorticoids and the child has assumed her genetically predicted growth trajectory.
FIGURE 2
Throughout the course of treatment, the patient remained clinically euthyroid. Developmental milestones were met age-appropriately. The patient remains in active follow-up with serial biochemical evaluation and imaging.
DISCUSSION
Therapy for IHs is indicated only in cases in which there is potential compromise of vital functions, disfigurement, or bleeding. Glucocorticoids have traditionally been the mainstay of systemic therapy, but are not without consequences, including secondary adrenal insufficiency, impairment of bone accretion, and growth
compromise.9Approximately 16% of
hemangiomas do not respond to steroid therapy.10b-Blockers were
serendipitously identified to promote regression of IHs and have assumed an increasingly prominent role in their treatment.11b-Blockers are now
considered standard-of-carefirst-line systemic therapy.12Vincristine has
been described for treatment of life-threatening and/or corticosteroid-resistant hemangiomas13–15;
however, its use in treating IHs for other indications is limited. In this report, we expand the indications for vincristine use to include
hemangiomas in patients with treatment-related morbidity.
The evolution of disease in this child is consistent with the natural history of IHs, which typically proliferate after birth and subsequently undergo spontaneous involution by 8 to 9 years of age. The tumor burden in this child and the associated hormonal abnormalities prompted early aggressive treatment to attempt to promote more rapid tumor involution.
This case identifies the challenging management of a child with hepatic hemangiomas resulting in
consumptive hypothyroidism. Although responsive to
glucocorticoids as a component of
multiagent therapy, growth-suppressive consequences
necessitated exploration of alternate treatments.
Several therapeutic challenges characterized this child’s care. Initial attempts to reestablish biochemical euthyroidism required multidrug therapy targeted at both thyroid hormone supplementation and at stabilization of the tumor, with eventual efforts to accelerate involution. Medical stabilization was ultimately achieved with a 4-drug regimen; however, iatrogenic complications limited the
continuation of this approach and prompted consideration of alternate strategies.
Vincristine is an antiangiogenic agent that acts via inhibition of cell mitosis and microtubule formation. It has been reported to be effective in life-threatening IHs and other vascular anomalies including tufted angiomas and kaposiform
hemangioendotheliomas.16The
introduction of vincristine in this circumstance allowed withdrawal of glucocorticoids within a period of weeks and was followed by tapering of all medications. Although it is possible that this response
represented, in part, the physiologic involution of the tumors, there had been little radiographic interval change, despite biochemical resolution. This observation
highlights that biochemical activity is separable from radiographic
appearance with respect to treatment response.
Other systemic therapies for second-line therapy of IHs have been proposed, including interferona17,18
and sirolimus.19,20Interferon therapy
is complicated by treatment-related toxicities including fever, irritability, malaise, liver function abnormalities, and neutropenia, although the potential for irreversible neurotoxicity (including several reports of spastic diplegia21,22)
substantially limits its consideration
as second-line therapy. It remains to be demonstrated which of these therapies is most appropriate; however, this report suggests vincristine to be a viable option that carries a tolerable side-effect profile.
We suggest vincristine to be an effective and safe adjunct therapy for systemic treatment of complicated IHs and that indications for use may expand beyond life-threatening situations to include those circumstances withfirst-line treatment failure and/or treatment-associated morbidity, provided appropriate clinical and biochemical monitoring is instituted.
REFERENCES
1. Sadler TW, Langman J.Langman’s Medical Embryology. 11th ed. Baltimore, MD: Lippincott William & Wilkins; 2009
2. Huang SA, Tu HM, Harney JW, et al. Severe hypothyroidism caused by type 3 iodothyronine deiodinase in infantile hemangiomas.N Engl J Med. 2000;343(3): 185–189
3. Konrad D, Ellis G, Perlman K. Spontaneous regression of severe acquired infantile hypothyroidism associated with multiple liver
hemangiomas.Pediatrics. 2003;112(6 pt 1):1424–1426
4. Balazs AE, Athanassaki I, Gunn SK, et al. Rapid resolution of consumptive hypothyroidism in a child with hepatic hemangioendothelioma following liver transplantation.Ann Clin Lab Sci. 2007; 37(3):280–284
5. Howard D, La Rosa FG, Huang S, et al. Consumptive hypothyroidism resulting from hepatic vascular tumors in an athyreotic adult.J Clin Endocrinol Metab. 2011;96(7):1966–1970
6. Huang SA, Fish SA, Dorfman DM, et al. A 21-year-old woman with consumptive hypothyroidism due to a vascular tumor expressing type 3 iodothyronine deiodinase.J Clin Endocrinol Metab. 2002;87(10):4457–4461
8. Lee TC, Barshes NR, Agee EE, et al. Resolution of medically resistant hypothyroidism after liver transplantation for hepatic
hemangioendothelioma.J Pediatr Surg. 2006;41(10):1783–1785
9. Boon LM, MacDonald DM, Mulliken JB. Complications of systemic corticosteroid therapy for problematic hemangioma. Plast Reconstr Surg. 1999;104(6): 1616–1623
10. Bennett ML, Fleischer AB Jr, Chamlin SL, Frieden IJ. Oral corticosteroid use is effective for cutaneous hemangiomas: an evidence-based evaluation.Arch Dermatol. 2001;137(9):1208–1213
11. Frieden IJ, Drolet BA. Propranolol for infantile hemangiomas: promise, peril, pathogenesis.Pediatr Dermatol. 2009; 26(5):642–644
12. Püttgen KB. Diagnosis and management of infantile hemangiomas.Pediatr Clin North Am. 2014;61(2):383–402
13. Perez J, Pardo J, Gomez C. Vincristine— an effective treatment of corticoid-resistant life-threatening infantile
hemangiomas.Acta Oncol. 2002;41(2): 197–199
14. Hoyoux C. Vincristine treatment for management of alarming hemangiomas in infancy [in French].Rev Med Liege. 2008;63(1):14–17
15. Perez Payarols J, Pardo Masferrer J, Gomez Bellvert C. Treatment of life-threatening infantile hemangiomas with vincristine.N Engl J Med. 1995; 333(1):69
16. Fahrtash F, McCahon E, Arbuckle S. Successful treatment of kaposiform hemangioendothelioma and tufted angioma with vincristine.J Pediatr Hematol Oncol. 2010;32(6):506–510
17. Chang E, Boyd A, Nelson CC, et al. Successful treatment of infantile hemangiomas with interferon-alpha-2b.J Pediatr Hematol Oncol. 1997;19(3): 237–244
18. Wilson MW, Hoehn ME, Haik BG, Rieman M, Reiss U. Low-dose cyclophosphamide and interferon alfa 2a for the treatment of capillary hemangioma of the orbit. Ophthalmology. 2007;114(5):1007–1011
19. Hammill AM, Wentzel M, Gupta A, et al. Sirolimus for the treatment of complicated vascular anomalies in children.Pediatr Blood Cancer. 2011; 57(6):1018–1024
20. Greenberger S, Yuan S, Walsh LA, et al. Rapamycin suppresses self-renewal and vasculogenic potential of stem cells isolated from infantile hemangioma.J Invest Dermatol. 2011;131(12):2467–2476
21. Barlow CF, Priebe CJ, Mulliken JB, et al. Spastic diplegia as a complication of interferon Alfa-2a treatment of hemangiomas of infancy.J Pediatr. 1998; 132(3 pt 1):527–530
22. Wörle H, Maass E, Köhler B, Treuner J. Interferon alpha-2a therapy in haemangiomas of infancy: spastic diplegia as a severe complication.Eur J Pediatr. 1999;158(4):344
DOI: 10.1542/peds.2014-2542 originally published online May 18, 2015;
2015;135;e1501
Pediatrics
Pope
Jonathan D. Wasserman, Sanjay Mahant, Manuel Carcao, Kusiel Perlman and Elena
Hemangiomas
Vincristine for Successful Treatment of Steroid-Dependent Infantile
Services
Updated Information &
http://pediatrics.aappublications.org/content/135/6/e1501
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/135/6/e1501#BIBL
This article cites 21 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/therapeutics_sub
Therapeutics
http://www.aappublications.org/cgi/collection/pharmacology_sub
Pharmacology
milestones_sub
http://www.aappublications.org/cgi/collection/growth:development_
Growth/Development Milestones
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior
Developmental/Behavioral Pediatrics following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2014-2542 originally published online May 18, 2015;
2015;135;e1501
Pediatrics
Pope
Jonathan D. Wasserman, Sanjay Mahant, Manuel Carcao, Kusiel Perlman and Elena
Hemangiomas
Vincristine for Successful Treatment of Steroid-Dependent Infantile
http://pediatrics.aappublications.org/content/135/6/e1501
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.