ABSTRACT
Purpose: Up to 80% of cancer patients are estimated to use Complementary and Alternative medicines (CAM) but most do not report their usage to oncologists. Here we assess self-reported knowledge and attitudes of oncologists towards CAM use.
Materials and Methods: Oncologists completed a web-based survey to determine their knowledge and attitudes towards different types of CAM (e.g. pharmacological/ ingestible or non-pharmacological) in different treatment settings (curative versus palliative), their CAM education needs and personal CAM use.
Complementary and Alternative Therapies
Used by Cancer Patients
1Linda M. Burnett MBBS (Hons), BApSc (MRT) (Hons), 2Haryana Dhillon, 1,2,3Janette Vardy. 1Sydney Medical School, University of Sydney, Australia. 2Centre for Medical Psychology and Evidence-based Decision Making, University of Sydney, Australia. 3Concord Cancer Centre, Australia.
Keywords: complementary and alternative medicines; oncologists; cancer treatments
Results: Eighty-five oncologists participated (response rate 36%). Many oncologists acknowledged they knew little about numerous CAM treatments and most over-estimated patient usage of CAM. Oncologists reported knowing most about therapies commonly used by patients: yoga, massage, acupuncture, meditation/relaxation/visualization and antioxidants/nutritional supplements. Forty-five percent never used a CAM personally and 29% used CAM at least monthly. Oncologists were more likely to ask patients about pharmacological/ingestible CAM use than non-pharmacological CAM, especially where treatment intent was curative, but most believed CAMs were more helpful in the palliative setting. Fifty-five percent of oncologists recommended non-pharmacological CAM at least monthly: most commonly for improvement of patients’ psychosocial well-being (66%). Sixty-two percent believed more CAM educational resources should be available, particularly information about CAM efficacy and specific herb-drug interactions.
INTRODUCTION
An Australian study published in 1996 reported that 22% of oncology patients were using at least one form of Complementary and Alternative medicine(CAM).1 A more recent North American study reports CAM use in cancer patients to be as high as 80%.2 The term CAM has come to encompass a wide variety of treatments ranging from biological agents such as herbs, to the use of meditation, acupuncture, aromatherapy and hypnotherapy.
While less invasive forms of CAM such as meditation are thought not to interfere with conventional cancer treatments, there is evidence of potential interaction between some herbal medications and cytotoxic drugs.3 Milk thistle, grape seed, ginseng and gingko biloba have all been shown to inhibit certain P450 liver enzymes4 which has the potential to alter the hepatic metabolism of conventional drugs; however there is very little research to indicate if these potential interactions are of clinical significance.
One study found that almost half of all oncology patients (47%) use nutritional supplements including anti-oxidants,5 yet there are data to suggest that taking antioxidants (including high dose vitamin C) concurrently with radiotherapy or chemotherapy might be harmful.6 This poses a concern that patients may be taking CAM which may make their conventional anti-cancer treatments less effective and/or increase the side effects of the chemotherapy or radiotherapy.
A 1997 study surveyed Australian oncologists and concluded that there were significant gaps in the knowledge of oncologists about CAM; with only 23% self-reporting knowing “lots” about antioxidants/high dose vitamin C and 13% indicating they had the same level of knowledge about herbal therapies/naturopathy.7 Another study has shown that 61% of physicians have reported they do not feel sufficiently knowledgeable about CAM safety and efficacy and 81% would like to receive more education on CAM treatments.8
Up to 46% of patients do not report CAM usage to their oncologist if not directly asked,5 and only 20% tell their doctor about CAM pharmacological therapies they are using for fear of disapproval.5 With little scientific evidence available to support the use of CAM, only 4% of physicians described their reactions to CAM as positive.9 Physicians were more likely to be supportive of CAM use in patients treated with palliative intent,7 and more
likely to ask a patient about their CAM use if they were sufficiently knowledgeable and comfortable with the topic themself.10
The aim of this study was to determine oncologists’ level of self-reported knowledge about CAM and evaluate their attitudes to CAM use by cancer patients at different stages in the disease trajectory.
METHODS
Ethics approval for this study was granted by the Human Research Ethics Committee of the University of Sydney. All participants gave informed consent.
A web-based survey containing 31 questions was designed using LimeSurvey, an open source online survey application. An email invitation to participate in the on-line survey was sent to oncologists who were members of the Medical Oncology, Radiation Therapy or Surgical Oncology Groups of the Clinical Oncological Society of Australia (COSA). Each responder was assigned a “once-only” token and all results were collected anonymously. After 2 weeks a reminder email was sent to non-responders.
For the purposes of the study CAMs were grouped into two categories:
1) Pharmacological/Ingestible CAMs including herbal medicines (eg St John’s Wort, ginkgo biloba, black cohosh), vitamin and mineral supplements, antioxidants, high dose vitamin C, megavitamins, homeopathy; and 2) Non-pharmacological CAMs including physical CAM (eg massage, acupuncture, Tai Chi, Reiki, osteopathic and chiropractic manipulation).
The questions estimating CAM use, self reported levels of knowledge about CAM and opinions of the efficacy of different CAMs were based on the study by Newell et al7. Additional questions were generated by the authors to assess oncologists’ demographics, circumstances in which oncologists ask patients about CAM use or are likely to recommend them, personal CAM use by oncologists and CAM education resources available to them. Where relevant, questions were divided depending on the intent of the treatment the patient was receiving: curative, anti-cancer treatment with palliative intent or best supportive care only.
demographic characteristics. Analysis involved simple statistics performed on Excel. Where responders did not answer any of the questions relating to CAM they were excluded from the data set.
RESULTS
Eight-five of the 234 oncologists invited to participate registered for the survey (response rate 36%), however two did not complete any questions and eleven completed the demographics section only and were not included in
the analysisof the CAM data. There were complete data for 65 oncologists and incomplete CAM data for a further seven respondents.
Most respondents (87%) were consultants with 61% working in Medical Oncology. Demographic details are outlined in Table 1. There was no difference in demographic characteristics between the oncologists who completed the survey and those who only completed the demographic section.
Oncologists were more likely to ask patients about
Table 1. Demographic details of oncologists - n (%)
Age Area of Specialty Training
20-29 years 1 (1.5%) 30-39 years 22 (26.5%)
40-49 years 31 (37%)
50-59 years 24 (29%)
>60 years 5 (6%)
Medical Oncology 45 (61%) Radiation Oncology 14 (19%) Surgical Oncology 11 (15%)
Other 4 (5%)
Gender Level of Training
Male 46 (55%)
Female 37 (45%) Consultant (staff) Resident/Fellow 5 (7%)64 (86.5%)
Other 5 (6.5%)
Country of Birth Primary Type of Cancer Treated*
Australia 56 (67.5%)
Other 27 (32.5%) Breast 51 (69%)Thoracic 33 (44.5%)
Colorectal 31 (42%)
Prostate/genitourinary 28 (38%) Melanoma 26 (35%) Upper GI 26 (35%) Central Nervous System 2 (30%) Gynecological 18 (24%) Head/Neck 14 (19%) Other 20 (27%)
Primary language spoken at home Primary type of hospital worked in
English 81 (97.5%)
Other 2 (2.5%) Public Hospital 58 (78%)Private Hospital 9 (12%) Other 7 (10%)
Years since graduating from medical degree Primary work location
<10years 8 (10.5%)
10-19years 23 (31%)
20-29years 27 (36%)
30-39years 14 (18.5%)
>40years 3 (4%)
Rural 6 (8%) Urban 68 (92%)
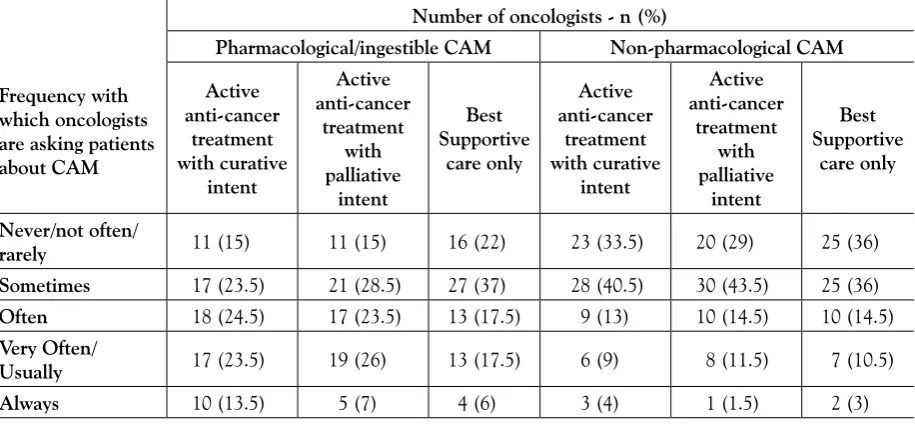
their use of pharmacological/ingestible CAM than non-pharmacological CAM (Table 2). Only 37% of oncologists usually or always asked patients receiving anti-cancer treatment with curative intent about their use of pharmacological/ingestible CAM, compared with 13% asking about non-pharmacological CAM.
Oncologists indicated their primary reason for asking a patient about their use of pharmacological/ingestible CAM was if the patient indicated they may be taking something non-conventional (46%), while 32% stated it was because certain pharmacological CAM may interact with some treatments. Many oncologists indicated that they specifically asked patients if they take high dose anti-oxidants (eg vitamin C) when being treated with radiotherapy or some types of chemotherapy (Fluorouracil, Methotrexate or CHOP - Cyclophosphamide, Adriamycin, Vincristine, Prednisone). Several indicated they asked patients about St John’s Wort if the patient was receiving a hepatically metabolised chemotherapy. Two participants indicated they inquired about Black Cohosh use in patients taking Tamoxifen. Oncologists were more likely to ask about any type of CAM use if the patient was being treated with curative intent (Table 2).
Thirty-one percent of oncologists reported they would never recommend a pharmacological/ingestible CAM to a patient, 27% said they would no more than twice a year
and 43% said they would recommend a pharmacological/ ingestible CAM daily, weekly or monthly. The same question was asked about non-pharmacological CAM and 12% said they would never recommend one, 33% said they would recommend use twice a year or less and 55% said they would recommend use daily, weekly or monthly.
The CAM oncologists reported most commonly recommending to patients were non-pharmacological treatments including relaxation, massage, meditation and/or acupuncture. The pharmacological/ingestible CAMs sometimes recommended included vitamin and mineral supplements, fish oil, black cohosh, and natural therapies for hot flushes (e.g. evening primrose oil). The main reasons for recommending a CAM included improving patient’s psychological well-being (66%), relaxation (57%) and to help improve symptoms (49%); 34% indicated it was to support the patient’s wishes.
Half the oncologists surveyed said that it made no difference what type of treatment the patient was receiving in relation to their likelihood of recommending a CAM, while 15% were more likely to recommend a CAM when the patient was receiving supportive care only. Another 15% indicated they would only recommend CAM when the patient was receiving active anti-cancer treatment with palliative intent and 3% when the patient was only receiving active anti-cancer treatment with curative intent. The remaining 16% stated that they
Table 2. How often oncologists ask patients about their use of complementary and alternative medicines (CAM) during different stages of treatment
Frequency with which oncologists are asking patients about CAM
Number of oncologists - n (%)
Pharmacological/ingestible CAM Non-pharmacological CAM
Active anti-cancer treatment with curative intent Active anti-cancer treatment with palliative intent Best Supportive care only Active anti-cancer treatment with curative intent Active anti-cancer treatment with palliative intent Best Supportive care only Never/not often/
rarely 11 (15) 11 (15) 16 (22) 23 (33.5) 20 (29) 25 (36) Sometimes 17 (23.5) 21 (28.5) 27 (37) 28 (40.5) 30 (43.5) 25 (36)
Often 18 (24.5) 17 (23.5) 13 (17.5) 9 (13) 10 (14.5) 10 (14.5)
Very Often/
never recommended CAM.
Most oncologists believed CAMs were more helpful when the patient was being treated with palliative rather than curative intent; although 1.5% - 3% thought diet therapy (eg macrobiotic, juicing), herbal therapies/ naturopathy/homeopathy and osteopathic manipulation were more helpful in patients with potentially curable disease. Approximately 86% thought massage was helpful in the palliative setting and 72% in the curative setting. Other therapies considered beneficial by the majority of oncologists were acupuncture, meditation/relaxation/ visual imagery, yoga, art/music/dance, tai chi and chi gong. (Figure 2)
Approximately 65% of respondents believed coffee enemas/colonic irrigation were harmful to patients
regardless of whether they were being treated with curative or palliative intent. Many thought antioxidants were harmful, especially in the curative setting (52%). Invasive therapies were more often considered harmful: this included psychic surgery, iscador/mistletoe therapy, leatrile/amygdalin therapy, diet therapy, ozone therapy, microwave/tronado therapy and osteopathic and chiropractic manipulation.
Oncologists reported they were better informed about yoga, massage, meditation/relaxation/visualization, acupuncture, and antioxidants/high dose vitamin C/ nutritional supplements. The least known therapies were cellular therapy, psychic surgery, magnetotherapy and immune enhancing therapy with 28-43% of oncologists never having heard of these treatments. (Figure 1).
Table 3. Oncologists estimates of how many patients are using either a pharmacological or non-pharmacological complementary and alternative medicine (CAM) during different stages of cancer treatment
Percentage of patients using CAM
Number of oncologists predicting certain level of use (n)%
Patients receiving active anti-cancer treatment
with curative intent
Patients receiving anti-cancer treatment with
palliative intent
Patients receiving the best supportive care only
0-19% 5 (7) 1 (1.5) 1 (1.5)
20-39% 13 (19) 5 (7) 5 (7)
40-59% 21 (31) 17 (25) 18 (26.5)
60-79% 21 (31) 25 (37) 23 (34)
80-100% 8 (12) 20 (29.5) 21 (31)
Table 4. Oncologists’estimates of Complementary and Alternate Medicine (CAM) usage by cancer patients compared with self-reported usage from a survey of patients (Oh B5)
CAM Percentage use predicted by Oncologists – n(%) Actual PatientUse 5 (%) 0-19% 20-39% 40-59% 60-79% 80-100%
Hypnotherapy 41 (63) 18 (27.5) 2 (3) 3 (5) 1 (1.5) 1
Faith Healing/Spiritualism 36 (55.5) 21 (32.5) 4 (6) 4 (6) 0 (0) 22.5* Meditation/Relaxation/Visual
Imagery 12 (18.5) 23 (35.5) 25 (38.5) 5 (7.5) 0 (0) 19
Psychic Surgery 62 (95.5) 2 (3) 1 (1.5) 0 (0) 0 (0) N/A
Progressive Muscle
Relaxation 39 (60) 17 (26) 8 (12.5) 1 (1.5) 0 (0) 8
Art/Music/Dance Therapy 22 (34) 30 (46) 11 (17) 2 (3) 0 (0) 4
Coffee Enemas/Colonic
Irrigation 51 (78.5) 13 (20) 1 (1.5) 0 (0) 0 (0) 1
Tai Chi & Chi Gong 34 (52.5) 23 (35.5) 4 (6) 4 (6) 0 (0) 8
Yoga 18 (27.5) 31 (48) 14 (21.5) 1 (1.5) 1 (1.5) 9
Chiropractic Manipulation 35 (54) 20 (31) 8 (12) 2 (3) 0 (0) 4
Massage 9 (14) 28 (43) 19 (29) 8 (12.5) 1 (1.5) 15
Osteopathic Manipulation 41 (63) 17 (26) 7 (11) 0 (0) 0 (0) 2
Reflexology 46 (71) 15 (23) 3 (4.5) 1 (1.5) 0 (0) 3
Reiki 43 (66) 16 (24.5) 5 (8) 1 (1.5) 0 (0) 3
Magnetotherapy 60 (92.5) 3 (4.5) 1 (1.5) 0 (0) 1 (1.5) N/A
Cellular Therapy 62 (95.5) 1 (1.5) 1 (1.5) 0 (0) 1 (1.5) N/A
Microwave/Tornado Therapy 56 (86) 7 (11) 1 (1.5) 0 (0) 1 (1.5) 0
Ozone Therapy 59 (91) 4 (6) 1 (1.5) 0 (0) 1 (1.5) 1
Aromatherapy 19 (29) 29 (44.5) 10 (15.5) 7 (11) 0 (0) 4
Most oncologists believed that at least 60% of patients were using at least one type of CAM. (Table 3). The oncologists’ estimation of the individual CAM usage is outlined in Table 4. The CAM that oncologists believed were used most commonly were meditation/ relaxation/visual imagery, antioxidants/high dose vitamin C/nutritional supplements (vitamins, minerals and enzymes), and herbal therapies/naturopathy/homeopathy.
Forty-five percent of the oncologists reported that they had never personally used a CAM, with 29% using a CAM no more than a few times a year, 22% weekly to monthly, and 5% daily. Of those oncologists who had used a CAM in the past three months, meditation, massage, yoga, and vitamin and mineral supplements were most commonly used.
The main sources of oncologists’ information about the latest informationand possible side-effects of CAM were journal articles (66%), internet (65%) and conferences (46%), with 36% stating they had no set resource. Forty-three percent of oncologists updated their knowledge on CAM no more frequently than yearly, 36% did so six monthly and 22% weekly to monthly.
Almost two thirds of oncologists (62%) indicated that more educational resources should be available about CAM use. A large proportion (88%) believed additional evidence about the efficacy or otherwise of CAM needed to be available, and 86% indicated they would like more information on specific herb-drug interactions. One
third requested more information about the prevalence of use of CAM in cancer patients. Thirty-seven percent believed professional education sites on the internet was the best way to disseminate information to oncologists, with 26% indicating journal articles as an alternate source. A further 25% stated updates at oncology conferences could be a helpful source of information.
DISCUSSION
Oncologist estimations of CAM usage among patients was relatively accurate with the rates of CAM usage self-reported by patients in a recent study for two thirds of the CAMs compared5 (Table 4). Oncologists tended to overestimate the use of some of the more commonly used therapies, including meditation/relaxation/visual imagery, herbal therapies/naturopathy/homeopathy, yoga, massage and acupuncture. They also overestimated patient use of aromatherapy and art/music/dance therapy. The majority estimated that 40-59% of their patients used antioxidants/ high dose vitamin C/nutritional supplements (vitamins, minerals and enzymes), which was consistent with patient self-report figures.5 This is important as this group of CAMs are those most commonly used by patients, with potential to affect some conventional cancer treatment regimens.11
Only 8% of oncologists reported knowing “lots” about herbal therapies/naturopathy and homeopathy (Figure 1), despite the majority of oncologists thinking that 40-59% Immune enhancing therapy 40 (61.5) 17 (26) 5 (8) 2 (3) 1 (1.5) N/A
Iridology 55 (84.5) 7 (11) 3 (4.5) 0 (0) 0 (0) N/A
Antioxidants/High Dose Vitamin C/Nutritional Supplements (Vitamins, Minerals and enzymes)
9 (14) 15 (23) 19 (29) 17 (26) 5 (8) 47
Diet Therapy (eg Gerson,
Macrobiotic, Gawler, Juicing) 23 (35.5) 19 (29) 13 (20) 9 (14) 1 (1.5) 20 Shark Cartilage Therapy 44 (67.5) 12 (18.5) 7 (11) 1 (1.5) 1 (1.5) 3 Herbal Therapies/
Naturopathy/
Homeopathy 12 (18.5) 9 (14) 24 (37) 16 (24.5) 4 (6)
Chinese Herbal Medicine – 12% Homeopathy – 4.5% Laetrile/Amygdalin 51 (78.5) 10 (15.5) 1 (1.5) 1 (1.5) 2 (3) 1
Iscador/Mistletoe therapy 56 (86) 7 (11) 0 (0) 0 (0) 2 (3) 6** N/A – not available (not surveyed in comparison study 5)
* surveyed as “Prayer or spiritual practices”
of their patients were using treatments from this group of CAMs. Although this was an overestimate of usage (Table 4), this is an important group of CAMs for oncologists to be adequately educated about as some of these agents may interact with conventional treatment regimens. For example, Black Cohosh is a herbal medication which may increase the cytotoxicity of chemotherapy agents doxorubicin and docetaxel12 and Kava Kava is a herbal supplement which can lead to hepatotoxicity and should be used with caution by cancer patients.3 Emerging evidence that the polyphenols in green tea may decrease the therapeutic benefits of bortezomib, used in the treatment of multiple myeloma, also needs further investigation.13 This popular herbal supplement has previously been known for its anticarcinogenic effects and is widely used by cancer patients. With only 11% of oncologists indicating they thought herbal therapies/ naturopathy/homeopathy “harmful”, this is an area where oncologists may need further education.
Oncologists reported knowing “some” or “lots” about most of the commonly used therapies, with the exception of faith healing/spiritualism where 48% knew “very little” or had “never heard of it”. This was the only CAM therapy where oncologists underestimated patient usage, although in the figures obtained from patients this was classified as prayer/spiritual practices5 so a direct comparison was not possible.
A comparison of current oncologist’s self-reported CAM knowledge showed that oncologists reported that they knew less about CAMs than oncologists did in 1997.7 We expect that it is not that oncologists CAM knowledge has decreased but rather that with increasing numbers of patients using a wider range of non-conventional therapies, oncologists may be more prepared to accept they have gaps in their knowledge as they become alert to the importance of knowing about herb-drug interactions. In our study 62% of oncologists indicated they would like to learn more about CAM, which is consistent with findings in previous studies.10
There was an increasing acceptance of CAM use with oncologists now more likely to report CAMs as being less harmful than a decade ago.7 Perhaps this is because many have now stood the test of time without serious side-effects, along with increasing knowledge about various physical types of CAMsas their popularity increases. The one exception was antioxidants/high dose vitamin C/ nutritional supplements where 52% thought they were “harmful” in patients being treated with curative intent compared with 30% in the past.7 Again, this may reflect
increasing knowledge about their potential interactions with radiotherapy and some chemotherapy regimens.6
While approximately half of the oncologists said they would recommend a CAM at least monthly, our results were consistent with previous studies showing oncologists often do not ask patients about their CAM usage. The majority of oncologists indicated they were most likely to discuss CAMs with their patients if the patient first indicated they may be taking something non-conventional, however as most patients expect their clinician to initiate the discussion if it may be important to their treatment,14 it is likely that CAM usage is frequently overlooked. In the past it has been found that a barrier to doctors initiating discussion was the belief that their own understanding of CAM was insufficient to discuss practices or provide evidence-based advice to patients.14 Studies however have suggested that as long as the discussion is carried out in a non-judgmental manner, patients do not expect their clinicians to be experts in CAM.14
Our study showed that 65% of oncologists had personally used a CAM. Previous research found that physicians were more likely to initiate discussion about CAM with a patient if they have used one themselves.10
Physicians have indicated in the past they would like more information about CAM so they can dissuade patients from using an unsafe or ineffective therapy.10 The majority of oncologists surveyed indicated they would like more education on the topic with easily accessible, high quality resources either on education sites on the internet, in journals or at conferences. Although there has been an increase in evidence-based resources such as the Memorial Sloan Kettering Cancer Centre About Herbs, Botanicals and Other Products website15 there remains a paucity of good quality evidence available about efficacy and herb-drug interactions relevant to oncology. Well-designed, adequately powered, high quality studies are needed to provide this information, with expansion of evidence-based resources so that oncologists can improve their knowledge of CAM and become more at ease initiating discussions on the subject with their patients.
or not using CAM, were more likely to participate. Oncologists’ estimates of patients’use of CAM were compared to patient self-report from a recent Australian study, but frequency of CAM use in cancer patients varies considerably across studies and between clinical situations.
The high rates of usage of CAM amongst cancer patients highlights the importance of oncologists becoming better informed about non-conventional therapies so they can ensure the alternate therapies their patients may be using are not interfering with their conventional cancer treatments and because some CAM may be beneficial. Creation of reputable internet sites for oncologists containing updated information and evidence about CAMs important to cancer treatments is indicated, as are more regular updates on the topic at conferences, in oncology and general medicine journals and incorporation into the medical curriculum. There needs to be high quality studies into the CAM most commonly used by patients to provide an evidence base for their use. As an increasing number of patients turn to CAM as a source of additional hope in their cancer journey it is important that oncological societies across the world ensure high quality resources are available.
REFERENCES
1. Begbie S, Kerestes Z, Bell D: Patterns of alternative medicine use by cancer patients. Medical Journal of Australia 165:545-548, 1996 2. Cassileth B, Deng G: Complentary and Alternative therapies for
Cancer. The Oncologist 9:80-89, 2004
3. Werneke U, Earl J, Seydel C, et al: Potential health risks of complementary alterative medicines in cancer patients. British Journal of Cancer 90:408-413, 2004
4. Etheridge A, Black S, Patel P, et al: An in vitro evaluation of cytochrome P450 inhibition and P-glycoprotien interaction with goldenseal, Gingko biloba, grape seed, milk thistle, and ginseng extracts and their constituents. Planta Medica 73:731-41, 2007 5. Oh B: Exploration of Complementary and Alternative Medicine
by Patients with Cancer and Evaluation of Medical Qigong. Presented at Australian Acupuncture and Chinese Medicine Annual Conference (AACMAC). 23-25 May 2008
6. D’Andrea G: Use of Antioxidants during Chemotherapy and Radiotherapy should be avoided. CA: A Cancer Journal for Clinicians 55:319-321, 2005
7. Newell S, Sanson-Fisher R: Australian oncologists’ self-reported knowledge and attitudes about non-traditional therapies used by cancer patients. Medical Journal of Australia 172:110-113, 2000 8. Milden S, Stokols D: Physicians’ attitudes and practices regarding
complementary and alternate medicine. Behavioural Medicine 30:73-82, 2004
9. Risberg T, Kolstad A, Bremnes Y, et al: Knowledge and Attitudes towards complementary and alternative therapies: a national multicentre study of oncology professionals in Norway. European Journla of Cancer 40:529-35, 2004
10. Winslow L, Shapiro H: Physicians want eudcation about complementary and alterative medicine to enhance communication with their patients. Archives of Internal Medicine 162:1176-1181, 2002
11. Heaney M, Gardner J, Karasavvas N, et al: Vitamin C antagonizes the cytotoxic effects of antineoplastic drugs. Cancer Research 68:8031-8, 2008
12. Rockwell S, Liu Y, Higgins S: Alteration of the effects of cancer therapy agents on breast cancer cells by the herbal medicine black cohosh. Breast Cancer Research and Treatment 90:233-9, 2005 13. Golden E, Lam P, Kardosh A, et al: Green tea polyphenols block
the anticancer effects of bortezomib and other boronic acid–based proteasome inhibitors Blood 113:5927-5937, 2009
14. Shelley B, Sussman A, Williams R, et al: They don’t ask me so I don’t tell them’: Patient-Clinician communication about traditional, Complementary, and alternative medicine. Annals of Family Medicine 7:139-147, 2009
15. Memorial Sloan-Kettering Cancer Centre 2013, About Herbs,
Botanicals and other Products, Integrative Medicine service, New