Original Article
Antibiotic-associated diarrhea: a systematic review with two decades of
experience
Suraj Gupte
ABSTRACT
Objective: To put in perspectives the scattered information in the literature with inputs from our 2 decades of experience on antibiotic-associated diarrhea (AAD)- a by and large neglected condition.
Resource and Design: Systematic review of literature together with our own experience spread over 2 decades.
Salient Features: AAD is defined as the diarrhea that has no known cause other than an antibiotic therapy given concurrently or discontinued at the most 4 weeks preceding it. By and large, each and every antibiotic, though some are decidedly high-risk, is capable of causing diarrhea. No doubt, C. difficile is responsible for most cases of severe AID (i.e. colitis), in some cases S. aureus and C. perfringens may well be the causative agents. Diagnosis is by and large clinical. Most important first-aid measure in AAD is withdrawal of the offending antibiotic and offering supportive measures to maintain fluid and electrolyte balance and nutrition. As a therapeutic measure (as and when considered warranted), metronidazole (preferably oral) should be considered the drug of first choice.Alternatively, ornidazole or nitazoxanide may be given. The somewhat superior in efficacy, though expensive, alternative is vancomycin. At times, the two drugs may be given simultaneously. Good food and water hygiene, meticulous hand-washing, and proper environmental cleaning are helpful. Incorporation of probiotics may have both a preventive and therapeutic role.
Conclusion: Judicious use of antibiotics is the most important preventive measure in AAD. Treatment modalities include withdrawal of the offending agent and administration of metronidazole, ornidazole or nitazoxanide. In case of poor response, vancomycin yieds gratifying response. Administration of probiotics may be helpful. A vaccine against C. difficile may well be around the corner.
INTRODUCTION
N
o doubt, the discovery of penicillin in 1928 by Alexander Fleming and multitude of other antibiotics subsequently has revolutionized the scenario of the infectious diseases, with a welcome increase in man’s lifespan.1 However, widespread use of antibiotics, often irrational, has led to appearance of multidrug-resistant (MDR) strains and emerging and re-emerging opportunistic infections.One such adverse byproduct of disturbing the ecosystem of the gut has been the antibiotic-associated diarrhea. According to
the WHO/UNICEF, there is hardly any known antibiotic that potentially is not diarrheagenic in pediatric practice1 though some antibiotics are decidely high-risk.2 Nevertheless, diarrheal manifestations are not always significant. Practically each and every antibiotic has the inherent property of provoking diarrhea-like manifestations, usually by interference with the normal ecosystem of the gastrointestinal tract.2-6 The problem is more frequent in infancy and childhood.
The incidence varies from 5 to as high as 25%. The patients administered with an antibiotic for a short duration are less likely to develop AAD as compared to those on longer duration.
International Journal of
Gastroenterology, Hepatology,
Transplant & Nutrition
Professor and Head, Postgraduate Department of Pediatrics, Mamata Medical College/Mamata General and Super speciality Hospitals, Khammam, Telangana, India.
Address for Correspondence Dr. Suraj Gupte
E-mail: [email protected]
Access this article online QR Code
Website: www.journal.pghtn.com
Key words: dif
Antibiotic-associated diarrhea, C.difficile, C. perfringens, Metronidazole, Nitazoxanide, Ornidazole, Probiotics, S. aureus,
7-15
Every other pediatric subject put on an antibiotic, in our own experience, develops loose motions of variable magnitude.16 In a small proportion of the cases, these may well be severe enough to cause concern.2,17-23
In most cases diarrhea is mild, resolving without any treatment whatsoever. There is no noteworthy adverse effect on the health status of the child. Those with moderate diarrhea need discontinuation of the offending antibiotic. In others, it may be fulminant and bloody, often refractory to discontinuation of the offending antibiotic and even additional therapeutic and supportive measures. In between the two extremes, different grades of diarrhea with or without blood may be seen.
According to one estimate, risk of ADD varies from 5 to 25% with different antibiotics.3 Pseudomembranous colitis associated with C. difficile occurs in 10 to 20% of all AAD cases and most of the severe AAD cases. It is also termed “C. difficile-associated diarrhea/colitis”.
Historical Considerations
The Bulletin of the John Hopkins Hospital of 1893 recorded the earliest documentation of AAD.3 The cause of the severe form of AAD, i.e. pseudomembranous colitis, remained elusive over many decades. This was referred to as “staphylococcal enterocolitis”, reflecting the belief that the disease was commonly caused by staphylococci. Only in 1970s, important clinical observations of clindamycin-associated pseudomembranous colitis and the demonstration of the potent cytopathic effects of C.difficile-derived toxin in animal models established the cause and pathogenesis of this condition.2
Presently, the term, ADD, usually (but not always) refers to a benign, self-limiting diarrhea following the use of antimicrobials. Typically, no pathogens are identified and the diarrhea is caused by changes in the composition and function of the intestinal flora. Most patients respond to supportive measures and discontinuation of antibiotics.
On the other hand, C. difficile-associated diarrhea (that should be considered as a severe form of AAD) refers to a wide spectrum of diarrheal illnesses caused by the potent toxins produced by this organism, including cases of severe colitis with or without the presence of pseudomembranes.
Terminology
The other semantics employed for AAD include:
1. Antibiotic-induced diarrhea (AID) or colitis (AIC) 2. Antibiotic-related diarrhea (ARD) or colitis (ARC) 3. Pseudomembranous colitis (PMC)
Truly speaking, the term, PMC, should be reserved for the advanced stage of the disease in which bloody stools, secondary to development of pseudomembrane, are characteristically seen.
Definition
suggested that ARD should be restricted to diarrhea occurring only during the course of antibiotic administration. This has been challenged by other groups.6-8 At present, the most widely accepted definition appears to be:
Diarrhea that has no other known cause than antibiotic therapy given concurrently or discontinued at the most 4 weeks preceding it.
Contrary to the usual impression, this definition in no way stresses on the presence of blood in stools. The most plausible implication is that, in AAD, stools may be frequent, watery and voluminous with or without gross blood or mucus.
Incidence/Frequency
In one multicentric prospective study from Sweden, incidence of AAD was found to be 4.9%.2 Fecal samples were positive for C. difficile cytotoxin B in 55.4%. Subjects treated with antibiotics for 3 days had a significantly (p value = 0.009) lower frequency of diarrhea than those treated for longer durations. Treatment with cephalosporins, clindamycin or broadspectrum penicillins was associated with an increased risk of diarrhea.
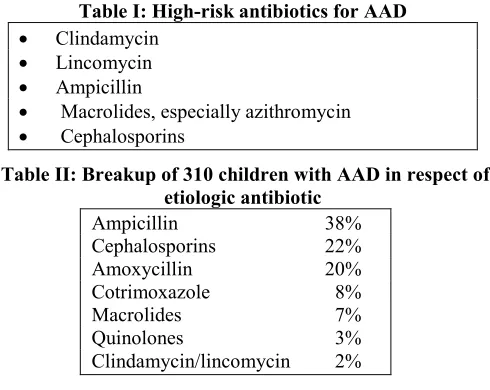
An analysis of published data as also our own experience shows frequency of AAD around 15-20%. The majority of the AAD subjects have IV antinbiotics as the cause. Table I lists the high-risk antibiotics for AAD.9,16 In our own experience, comprising around 310 cases of AAD, the breakup is as shown in Table II.
Table I: High-risk antibiotics for AAD
Clindamycin
Lincomycin
Ampicillin
Macrolides, especially azithromycin
Cephalosporins
Table II: Breakup of 310 children with AAD in respect of etiologic antibiotic
Ampicillin 38%
Cephalosporins 22%
Amoxycillin 20%
Cotrimoxazole 8%
Macrolides 7%
Quinolones 3%
Clindamycin/lincomycin 2%
Though clindamycin and lincomycin are known to have a high potential for causing AAD, in our series of 310 children with AAD, these antibiotics were responsible for it in just 2% of the cases. Reason: These antibiotics were employed in only a small number of cases. However, their extraordinary potentiality for causing AAD receives support from the observation that every third child treated with them developed AAD in our series.
Etiopathogenesis
methotrexate, antiviral agents, etc. especially when administered orally, may particularly cause serious disease in the form of pseudomembranous colitis.
Very rarely, even vancomycin and metronidazole, which are employed for treatment of PMC, may cause this condition.1 Though clindamycin was the first antibiotic blamed for severe diarrhea (PMC), most cases appear to be secondary to ampicillin and cephalosporin administration because of a very extensive use of these agents in clinical practice.
The growth of a spore-forming gram-positive anaerobic bacillus, Cl. difficile, which is ubiquitous in the environment in the soil, is responsible for the PMC. It is normally found in 70% neonates, 20 to 50% infants and only 3% of adolescents and adults. It is by no means invasive. Though, most of its strains are toxic, producing two toxins which cause a plethora of adverse effects (Table III).
Table III: Adverse effects produced by toxins of C. difficile
• Inflammation
• Loss of proteins
• Exaggerated peristalsis
• Hemorrhages
• Enhanced fluid and electrolyte secretions
• Cytotoxicity
Enterotoxin (toxin A) acts on the intestinal mucosa to produce diarrhea. Cytotoxin (toxin B) enhances vascular permeability in low doses, but in higher doses it may prove lethal. Toxin B is 1,000 times more powerful and have 100 fold greater enzymatic activity than toxin A. Occasional strains of the pathogen may produce only one or neither toxin. The significant mechanisms of production of diarrhea by C. difficile are listed in Table IV.
Table IV: Mechanism of production of diarrheal symptoms by C. difficile
• Overgrowth of the organisms with suppression of normal gut flora by antibiotics
• Interaction of the organisms with other flora of the gut
• Actual triggering of production of the toxin by organisms by the antibiotics
• Production of enzyme, beta-lactamases, by resistant organisms, which inactivate antibiotics and facilitate growth of C. difficile.
Majority of pediatric AAD is not due to C. difficile though it is an important cause of severe AAD in the form of PMC. S. aureus, Clostridium perfringens, and Klebsiella oxytoca are other pathogens identified as potential causes of C.
difficile-negative AAD in the form of hemorrhagic colitis when
predominant in stool samples, should also be considered a possible etiologic agent for AAD.
Pathophysiology
Among the several posulations put forward to explain the pathophysiology of PMC, the significant ones are listed in Table V.
The so-called ‘pseudomembranous nodules’ (also termed ‘plaques’) develop in rectum, sigmoid colon or distal colon. In some cases, these may be noticed in cecum and transverse colon only. The lesions appear as greyish-white exudates that are surrounded by edematous and erythematous inflammatory response. These are only weakly adherent to the underlying tissue.
Table V: Various postulations for pathophysiology of pseudomemanous colitis
• Changes in intestinal microbial flora
• Direct effects of antibiotics and their metabolites
• Localized Schwartzman reaction
• Hypersensitivity reaction
• Intravascular coagulopathy
• Elaboration of toxins by intestinal flora and production of enzyme, beta lactamase, by resistant organisms, which inactivate antibiotics and facilitate growth of C. difficile.
Until recently, it was held that C. difficile does not cause diarrhea unless the subject is administered an antibiotic. However, strains of C. difficile (around 8%) have been recognized that cause diarrhea even without preceding antibiotic administration.
Enough evidence is also available that any factor that disrupts the normal bowel flora (antibiotics) or bowel motility (bowel stasis, Hirschsprung disease, bowel surgery) predisposes to C. difficile-associated diarrhea. Uremia, anesthesia and dietary changes also render the child vulnerable to pseudomembranous colitis. Today, there is evidence that Staphylococcus aureus and C. perfringens too are capable of causing AAD.
Clinical Manifestations4
Clinical manifestations, which are variable, range from mild self-limited diarrhea without pseudomembrane through explosive watery diarrhea with occasional blood to severe hemorrhagic colitis with classical picture of blood and mucus accompanied by toxemia.
The toxemic patient may have pyrexia, cramps, crampy abdominal pain, nausea and vomiting, dehydration with dyselectrolytemia, protein-losing enteropathy, hypoalbuminemia. Such serious complications as toxic megacolon, colonic perforation, peritonitis and shock my occur. Even death may result.
Diagnosis15-17
High index of suspicion in a patient with significant diarrhea or colitis in the setting of prior or current antibiotic therapy remains critical in the diagnosis of AAD.3
Diagnosist is established by demonstrating C. difficile or its toxins in the stools (usually the latter).
C. difficile and its cytotoxin B may be identified by tissue culture with appropriate neutralization by antitoxin or toxicity to cultured fibroblasts. It is advisable to inoculate stool specimens on cycloserine cetoxitin fructose agar. Following incubation anaerobically, C. difficile can be isolated. Unfortunately, diagnosis of C. difficile by culture is difficult and time-consuming because of strict anaerobic nature of the organism.
The application of enzyme immunoassay (EIA) for detection of C. difficile has turned out to be a highly sensitive and specific method for diagnosis of PMC, giving results in just 3 hours. This should be considered the method of choice, and, perhaps, the gold-standard test, for rapid diagnosis of C. difficile-induced diarrhea. Toxin A can be identified by ELISA or latex agglutination assay. On rectosigmoidoscopy/colonoscopy, the usual findings are mucosal edema, friability and ulceration of varying grades. Pseudomembranous nodules/plaques are seen in advanced cases only. Infrequently, these observations spare the rectum and the sigmoid colon, but may be seen proximal colon.
We strongly feel that this investigation should be reserved for atypical cases only.
Four stages of AAD may be recognized based on picture of the colonic mucosa (Table VI). Most children suffer from stage II, which is characterized by mild erythema and edema of the colonic mucosa. Some fecal leukocytes can be detected in around half of the cases whereas a large number of red cells in feces are almost a rule. Histopathology of PMC nodules/plaques reveals mushroom-like lesion with massive fibrin, red cells and leukocytes.
Table VI: Stages of AAD based on appearance of colon (on recto-sigmoidoscopy /colonoscopy
Stage One: Normal appearance Stage Two: Mild erythema and edema
Stage Three: Granular, friable or hemorrhagic mucosa Stage Four: Pseudomembrane formation.
Differential Diagnosis2,5,10,15
Differential diagnosis of AAD is from diarrhea due to
• Shigella, Salmonella,
• inflammatory bowel disease,
• neutropenic colitis/typhlitis,
• malabsorption and
• bloody diarrhea due to parasites such as L. giardia, E. histolytica, H. nana, S. stercoralis and T. trichiura.
For dependable diagnosis of AAD, it is appropriate that these
one or more of these factors plus the AAD is not unusual in resource-limited communities.
Therapeutic Approach and Outcome2,13,20
Immediate Measures
The cornerstone of treatment is immediate withdrawal of the antibiotic(s), provided that it is workable and offering supportive treatment in the form of fluid and electrolyte replacement and adequate nutrition.
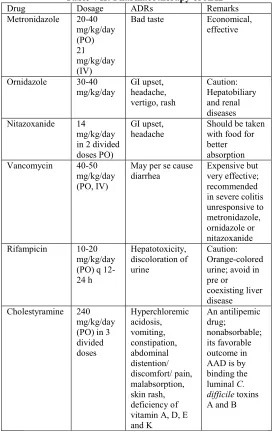
Table VII: Pharmacotherapy of AAD
Drug Dosage ADRs Remarks
Metronidazole 20-40
mg/kg/day (PO) 21 mg/kg/day (IV)
Bad taste Economical,
effective
Ornidazole 30-40
mg/kg/day
GI upset, headache, vertigo, rash
Caution: Hepatobiliary and renal diseases
Nitazoxanide 14
mg/kg/day in 2 divided doses PO)
GI upset, headache
Should be taken with food for better absorption
Vancomycin 40-50
mg/kg/day (PO, IV)
May per se cause diarrhea
Expensive but very effective; recommended in severe colitis unresponsive to metronidazole, ornidazole or nitazoxanide
Rifampicin 10-20
mg/kg/day (PO) q 12-24 h
Hepatotoxicity, discoloration of urine
Caution: Orange-colored urine; avoid in pre or
coexisting liver disease
Cholestyramine 240
mg/kg/day (PO) in 3 divided doses
Hyperchloremic acidosis, vomiting, constipation, abdominal distention/ discomfort/ pain, malabsorption, skin rash, deficiency of vitamin A, D, E and K
An antilipemic drug;
nonabsorbable; its favorable outcome in AAD is by binding the luminal C. difficile toxins A and B
Pharmacotherapy (Table VII)
In our considered opinion, oral metronidazole should be the preferred agent since it is less expensive and yet very effective and cuts down the emergence of vancomycin-resistant enterococci, which can become a problem in hospitalized children.
In case of the child failing to respond to one, it may be substituted by the other. Such drugs as ornidazole, and nitazoxanide may be as effective as metronidazole and can easily be used as a substitute. The experience with a relatively new agent, fidazoxamicin, (though recommended) remains limited.
In yet more critical situations (toxic megacolon, adynamic ileus), the two drugs (metronidazole and vancomycin) may well be given simultaneously (intravenously). Alternatively, vancomycin may well be substituted with a tetracycline in older children. Response to treatment, as a rule is excellent, usually over 70 to 95%. However, a proportion of patients (say 5 to 30%) are likely to have a recurrence within 1 to 2 week. Another course of therapy usually resolves their problem.
In our experience, even children with severe AAD (including pseudomembranous colitis) show gratifying response to metronidazole. Institution of vancomycin or metronidazole plus vancomycin therapy is necessitated in only an occasional case.
Probiotics23-37
Probiotics are friendly or health-enhancing microorganisms consumed as a food or dietary supplement. Yoghurt and fermented milks are the most common foods that serve as probiotics. Dietary supplements serving as probiotics are available as powder, tablets and capsules. Whereas their important role in rotavirus diarrhea stands by and large established,26 their beneficial effect in AAD is very likely to be due to the following two factors:
• Restoration of the normal gut flora
• Direct effect on the C. difficile colitis.
In addition, probiotics have several other health-friendly benefits. Over and above, lactobacilli, some other nonpathogenic organisms have also been employed in the therapy of AAD (Table VIII). Table IX lists the advantages of probiotics as such as also in AAD in particular.
Table VIII: Non-pathogenic organisms employed in treatment of AAD
• Lactobacilli: L. acidophillus (readily available, economic though less potent), L. bulgaricus L. GG (most potent, but expensive)
• Bifidobacterium longum
• Enterococcus faecium
• Streptococcus thermophilus
• Saccharomyces boulardii
Table IX: Health-friendly benefits of probiotics General
• Nutritional enhancement
• Promotion of weight gain
• Control of intestinal infections
• Control of lactose intolerance
• Control of hypercholesterolemia
• Control of colonic cancer
• Control of ethanol-induced liver damage
• Treatment of food allergies
• Immunomodulation.
Specific in AAD
• Restoration of normal flora of the gut
• Inhibition of growth of C. difficile
Refractory Cases
In a small group of patients who continue to have further recurrence(s), it is advisable to give trials of oral cholestyramine, rifampicin (along with vancomycin), bacitracin, immune globulin, probiotics (lactobacilli and bifidobacterium species) for reconstitution of bowel flora, and baker’s yeast. Even instillation of fecal flora by tube feeding or enemas has been recommended.23,30 In our experience, such a desperate situation never arose.
Outcome and Prognosis
High index of suspicion, identification, discontinuation of the suspected antibiotic and timely management are usually accompanied by a favorable outcome.32,33
Prevention
Generally speaking, the following measures may well be helpful in prevention of AAD:15,16
• Food and water hygiene
• Hand hygiene
• Proper environmental cleaning
• Judicious use of antibiotics.
• Routine use of probiotic-rich diet or as medicinal supplement, especially during the course of antibiotic administration. Enough evidence is available supporting the preventive role of Lactobacillus GG in AAD.
Prevention in PICU: Prevention of AAD in PICU revolves around avoidance of overuse of antibiotics. For prevention of C. difficile and other agents responsible for AAD, improved hygiene (single room, private bathrooms, use of gloves and hand washing) are helpful.9,13 In order to safeguard against nosocomial spread, contact isolation of the patients is mandatory. Else, they may spread the infection to others.
CONCLUSIONS
Antibiotic-associated diarrhea is defined as the diarrhea that has no known cause other than an antibiotic therapy given concurrently or discontinued at the most 4 weeks preceding it. By and large, each and every antibiotic, though some are decidedly high-risk, is capable of causing diarrhea.
C. difficile is responsible for most cases of severe AAD (i.e. colitis), in some cases S. aureus and C. perfringens may well be the causative factors.
Most important first-aid measure is withdrawal of the offending antibiotic and offering supportive measures to maintain fluid and electrolyte balance and nutrition. Good food and water hygiene, meticulous hand-washing, and proper environmental cleaning are helpful. Incorporation of probiotics may have both a preventive and therapeutic role in AAD.
As a therapeutic measure (as and when considered warranted), metronidazole (preferably oral) should be considered the drug of first choice. Alternatively, ornidazole or nitazoxanide may be given. The superior, though expensive, alternative is vancomycin. At times, the two drugs may be given simultaneously.
Judicious use of antibiotics is the most important preventive measure though a vaccine against C. difficile may well be around the corner.
Take-Home Messages
• Virtually all antibiotics, especially broad spectrum ones, have the potential of causing diarrhea.
• Intravenous antibiotics, especially when given for relatively prolonged period stand higher chances of causing it.
• C. difficile is responsible for most cases of severe antibiotic-associated diarrhea (i.e. colitis); in some cases S. aureus and C. perfringens may well be the causative factor
• Most important first-aid measure in AAD is withdrawal of the offending antibiotic and offering supportive measures to maintain fluid and electrolyte balance and nutrition
• Probiotics may have both a preventive and therapeutic role.
• Metronidazole, ornidazole or nitazoxanide should be considered the drug of first choice in its treatment.
• Vancomycin may be considered in cases not responding to first-line drug. At times, the two drugs may be given simultaneously
• Rational use of antibiotics is the most important preventive measure.
REFERENCES
1. Haran JP, Hayward G, Skinner S, et al. Factors influencing the development of antibiotic associated diarrhea in ED patients discharged home: Risk of administering IV antibiotics. Am J Emerg Med 2014; 32(10):1195-9. doi: 10.1016/j.ajem.2014. 07.015. Epub 2014 Jul 30.
2. World Health Organization. Diarrheal Disease. Geneva:
3. Gupte S, Pal M. The problem of antibiotic-related diarrhea (colitis) in north Indian children. Bull Trop Subtrop Med 1997; 7: 123-129.
4. Wisham J, Norrby SR, Myhre CB, et al. Frequency of antibiotic associated diarrhea in 2462 antibiotic treated hospitalized patients: A prospective study. J Antimicrob Chemother 2000; 47: 43-50.
5. Ferguson AW. Antibiotic-related diarrhea/ colitis in pediatric practice. Eur Med Bull 2001; 7: 123-129.
6. Smith E, Kennedy EA, June W. Antibiotic-related diarrheal illness. Eur Med Bull 2001; 7: 34-39.
7. Robert AS. Letter to the Editor: Antibiotic-related diarrheas. Eur Med Bull 2001; 7: 99-100.
8. Nord K, Wardhan R. Letter to the Editor: Antibiotic-related diarrheas. Eur Med Bull 2001; 7: 100-101.
9. Gorenek L, Dzer U, Besirbellioglu B, et al. The diagnosis and treatment of Clostridium difficile in antibiotic-associated diarrhea. Hepatogastroenterology 1999; 46: 343-348.
10. Gupte S. Antibiotic-associated diarrhea in children. In: Thapa BR (ed): Recent Advances in Pediatric Clinical Gastroenterology. Chandigarh: Relume Printec 2001: 42-47.
11. Gupte S, Anderson RA. Pseudomembranous colitis. In: Gupte S (ed): The Short Textbook of Pediatrics, 12th edn. New Delhi: Jaypee 2016: 455-456.
12. Cleary RK: Clostridium difficile-associated diarrhea and colitis: Clinical manifestations, diagnosis and treatment. Dis Colon Rectum 1998; 41: 1439-1445.
13. Bergogne-Berezin E. Treatment and prevention of antibiotic-associated diarrhea. Int J Antimicrob Agents 2001; 16: 521-526.
14. Tomar BS. Chronic diarrhea. In: Gupte (ed): Recent Advances in Pediatrics-10. New Delhi: Jaypee 2000; 163-164.
15. Gupte S: Differential Diagnosis in Pediatrics, 5th edn. New Delhi: Jaypee, 2009.
16. Sutana Q, Chaudhary NA, Munir M, Anwar MS, Tayyab M. Diagnosis of Clostridium difficile antibiotic-associated culture versus toxin assay. J Pak Med Ass 2000; 50: 246-249.
17. Gupte S, Pal M: Perspectives in antibiotic-associated diarrhea in pediatric practice (Abstract of the invited lecture). Proceedings of the International Conference on Pediatric Diarrheas, Hong Kong. Bioscience 1999; 56-57.
18. Suvarna J. Antibiotics and diarrhea. In: Gupte S, Horvath K (eds): Pediatric Gastroenterology, Hepatology and Nutrition. New Delhi: Peepee 2009; 210-219.
associated with antibiotic therapy (original article in French). Pathol Biol (Paris) 1999; 47: 415-421.
20. Johnson S. Epidemics of diarrhea caused by a clindamycin-resistant strain of Clostridium difficile in four hospitals. N
Engl J Med 1999; 341: 1645-648.
21. Geridon DN: Clostridium difficile-associated diarrhea and colitis. Infect Control Hosp Epidemiol 1995; 16: 459-463.
22. Gravet A, Rondeau M, Harif-Monteil C. Predominant Staphylococcus aureus isolated from antibiotic associated diarrhea is clinically relevant and produces enterotoxin A and bicomponent toxin LukE-LukD. J Clin Microbiol 1999; 37: 4012-4019.
23. Gopalan S. Prebiotics and probiotics: A possible beneficial role in diarrhea. In: Thapa BR (ed): Recent Advances in Pediatric Clinical Gastroenterology. Chandigarh: Relume Printec 2001: 48-54.
24. Gandhi DN, Nambudripad VKN. Implantation of Lactobacillus acidophilus in the intestines of adults suffering from gastrointestnal disorders. Sci Reporter 1977; 584-585.
25. Raza S, Graham SM, Allen SG, et al. Lactobacillus GG promotes recovery from acute nonbloody diarrhea in Pakistan. Pediatr Infec Dis 1995; 14: 107-111.
26. Saavedra J. Probiotics and infectious diarhea. Am J Gastrornterol 2000; 95: S16-S18.
27. Donohue DC, Salminen S. Safety of probiotic bacteria. Asia Pacific J Clin Nutr 1996; 5: 25-28.
28. Gibsoin GR, Roberfroid MB. Dietary modification of the human colonic microbiota: Introducing the concept of probiotics. J Nutr 1995; 125: 1401-1412.
29. Salminen S, Isolauri E, Salminen E. Clinical uses of probiotics for stabilizing the gut muosal barrier: Successful strains and future challenges. Asia PacificJ Clin Nutr 1996; 5: 53-56.
30. Salminen S. Human studies on probiotics: Aspects of scientific documentation. Scand J Clin Nutr 2001; 45: 8-12.
31. Benson AW, Woodruff E: Antibiotic-related diarrheal colitis. In: Benson AW (ed): Pediatric Gastroenterology and Nutrition, 2nd edn. London: Smith and Smith 2000: 198-199.
32. Arvola T, Laiho K, Tarkkeli S, et al. Prophylactic Lactobacillus GG reduces antibioticassociated diarrhea in children with respiratory infections: A randomized study.
Pediatrics 1999; 104: 64. Available at:
http://www.pediatrics.org. Accessed on: 22 October 2011.
33. Vanderhoof JA, Whitney DB, Antonson DL, Hanner TL, Lupo JV, Young RJ. Lactobacillus GG in the prevention of antibiotic-associated diarrhea in children. J Pediatr 1999; 135: 535-537.
34. Henry CA: Epidemiologic and preventive aspects of diarrheas. In: Benson AW (ed): Pediatric Gastroenterology
and Nutrition, 2nd edn. London: Smith and Smith 2000; 222-231.
35. Gupte S. Health education in diarrheal disease. Indian J Pediatr 2001; 68: 474-475.
36. Musher DM, Logan N, Hamill RJ, et al. Nitazoxanide for the treatment of Clostridium difficile colitis. CID 2006; 43: 421-427.
37. Sabaiha M, Wren B, Mullany P, et al. The multidrug-resistant human pathogen, Clostridium difficile has a highly mobile mosaic genome. Nat Genet 2006; 38: 779-786.
38. Sougioultzis S, Kyne I, Drudy D, et al. Clostridium difficile toxoid vaccine in recurrent C. difficile-associated diarrhea. Gastroenterology 2005; 128: 764-770.
39. Ghose C. Clostridium difficile infection in twenty-first century. Emerg Microb Infec 2013; 2, e62; doi:10.1038/emi.2013.62 Published online 18 September 2013