International Journal of Pharmaceutical Research & Allied Sciences, 2016, 5(2):510-517
Research Article
CODEN(USA) : IJPRPM
ISSN : 2277-3657
Comparison of Sensorimotor Retraining Methods by Movement Therapy Based
on Limitations in Upper Extremity Function in Patients with Chronic Stroke
Afshin Samaei
1.Mina Sadat Mirshoja
2*, Mohammad Amoozadeh Khalili, Ph.D.
2 1Department of neurology, Semnan University of Medical Sciences,Semnan, Iran2Neuromuscular Rehabilitation Research Center, Rehabilitation College, Semnan University of Medical
Sciences,Semnan, Iran Email*: [email protected]
________________________________________________________________________________________
ABSTRACT
Objective: Numbness and paralysisofhalf of the body, especially the upper extremity involvement is the most
important effects of a stroke.Given the importance of a healthy senseforperforming daily livingactivities and the use of common methods by therapists, this study is conducted with the aim of comparing two methods of sensorimotor training and movement therapy based on limitingthe upper extremity function in patients with chronic stroke.
Materials and Methods:The study is conducted in the form of a simple randomized and clinical trialamong patients
admitted to Tehran clinics. The study is performed on two groups of sensorimotor training for 2 weeks and 5 days a week and the group of movement therapybased on limitingthe normal upper extremity. In this group, the subjects are asked to divide into 5 days a week for six hours over two weeks. Then, they were analyzed before and after therapeutic interventions in separate days of therapeutic sessions. The applied test include 9-HOLE peg test, Wolf motor function evaluation ، Haptic object Recognition Test and two-points differentiation.
Findings: The results indicate the reduction of 9-HPT test run time, which represents an increase in the hand speed
sensorimotor retraining group. The reduction in average errors inHORT test reflects the increasing in the sensoryability to touch and evaluating the objects by removing the vision ability. The Astereognosis scores increased.In addition, increasing the WMFT test performance scores and reduction of the time to do activitiesrepresent the increase in operating speed andimproving movement in the upper extremities.Results showed a significant difference in all the tests before and after sensorimotor retraining at p<0.005.
Discussion and conclusion: The results of this study showed CIMT and sensory-motor retrainin retraining improve
the upper extremity motor sensory function and reducing the dependence in daily activities and increasing the satisfaction and quality of life.
Keywords: sensorimotor retraining, movement therapy based on limitations, upper extremity function, chronic stroke
_____________________________________________________________________________________________
INTRODUCTION
sensory and motorimprove together (13).There are various therapies for these patients.Sensorimotor retraining therapy is one of the new proposed therapies that emphasizes on improving the sensory and motor (14,15).Sensorimotor retraining therapy uses the activities that require the active discover of hands and differentiated sensory and facilitate the recovery of fine motor sensory (16,17). In addition, CIMT is one of the effective therapeutic interventions based on Neuroplasticity and cortical reconstruction.This method increases the use of the affected extremity in daily activities of life by limiting the healthy upper extremity function. Various exercises that cause reusing the affected member facilitatethe reconstruction of cortical andimprove the function of organs (18).
The review article showed the effectiveness of sensory therapy in upper extremity functionand improving the sense of hypesthesia, proprioception, two-pointdifferentiation, the perception of depth and distance, and Astereognosis. Chen et al. (2005) compared thestandard therapies using thermal methods.This study was conducted on 29 patients in the twotreatment and control groups. Thetreatment group received the intervention program of thermalmodalities to 5 days per week for 6 weeks.Each session was 30 minutes.Brunnstrom recovery stage test, grip strength, wrist
bending, monofilament sensory evaluation, Ashworth Tone Assessment Scale were used. Results showed a
significant improvement in the treatment group.Ben-Shabat et al. (2005) performed a research to evaluate sensory function after receiving brain's sensory interventions.The results of this study show an improvement in brain sensory function in the treatment group.Accera et al. (2007)applied mirror therapywithsensorimotorassignments on 40 patients in two 20-member control and treatment groups. The treatment group received 14 days therapy 20-30 minutes per session.There was a significant difference in the treatment group in the assessments of grip strength, pain reduction, and upper extremity motor function (12). Nasser Amini et al. (2012) conducted a study with the aim of assessing the impact of CIMT on the quality of life, function, and range of motion of upper extremity stroke patients. In this study, the healthy upper extremity of 15 patients was limited 3 days per week for 8 hours and 6 weeks with the orthopedic sling. The test results showed a significant improvement in SF-36,and Box and Block tests (19).Abdol Wahab et al. (2009) investigated the effects of CIMT on the activities of daily living.Barthel test and armfunctional test were used to evaluate the upper extremity function in activities of daily living. Results showed a significant difference after 8 weeks, 3 days per week for 8 hours limit in healthy upper extremity (20).
Given the importance of a healthy senseforperforming daily livingactivities and the use of common methods by therapists, this study is conducted with the aim of comparing sensorimotor training and movement therapy based on limitingthe upper extremity function in patients with chronic stroke.
Materials and Methods
The study is conducted in the form of a simple randomized and clinical trialamong patients admitted to Tehran clinics.Before the start of the study, the patients were evaluated in terms of inclusion criteria. Inclusion criteria included the experience of the first stroke, passing at least 6 months from the injury time (21), not one-sided visuospatial neglect (Star cancellation> 44) (22), having sensorimotor retraining conditions(returning a light touch sensation in the fingers in acceptable mono filaments levels of 3.84-4.31 and two-pointdifferentiation of 7-10mm) in the hands of the patients (21),having the least upper extremity motor ability based on five or more stages brunstrum test, lack of muscle tone above one based on Ashworth criteria in the hands of the patients (23),the absence of pathology (24) (Mini mental status examination> 21), the age range of 45-60. Exclusion criteria included stroke, orthopedic problems, repeated rheumatology and neurologyduring the therapeutic intervention, absenteeism and lack of desire to continue treatment.The purpose of the study was expressed with participants’ satisfaction. Measurement tools includedAstereognosis tests, Haptic object Recognition Test, 9 - HOLE peg test, The Wolf Motor Function Test, and the two-pointdifferentiation.
Activities were planned and executedfor all the samples in consecutive sessions. They were arranged from easy to hard in association with the sensory function of participants.They were asked todo the activities with the affected hand. If the person was not able to do with that hand, the therapistcould give the least help. In addition, the therapist gave the necessary guidelinesduring the implementation oftraining. Restingwas allocated between two to five minutes at the request of the participants in the exercise (23).Mandatory usingtherapyof the affected upper extremity was done by limiting the healthy upper extremity, and the person was asked to do the planned activities five days a week for 6 hours by the affected hand. In this study, two therapists -one familiar to therapeutic intervention and the other as an assessor whowas not aware of the treatment- were used.All patientswere evaluatedbefore and after therapeutic interventions on separate therapy sessions.
The applied test include 9-HOLE peg test with the test-retestreliability of 0.83-0.99 (1), Wolf motor function evaluation with the test-retestreliability of 0.9 (2), Haptic object Recognition Test with the reliability of 1.3-1.8 (3,4), adequate reliability of two-points differentiation (5,6), and Astereognosis (7).
Paired T-test and Wilcoxon test were used in 18-SPSS software for data analysis.
Results and Discussion
This study was done in the form of quasi-experimentalbefore and after without control on 36 chronic stroke patients in two groups of sensorimotor and movement therapy groups (limiting the upper extremities). 18 right hemiparesis and 18left hemiparesis in terms of gender between men and women were selected nonspecific from the admitted patients of Tehran rehabilitation clinics. The average age range was 58.47 years old who has passed 45.5 months from the disease. All participants have a sense of protection and they were in the fifth and sixth stages of brunstrum test. Other demographic data are given in Table 1.
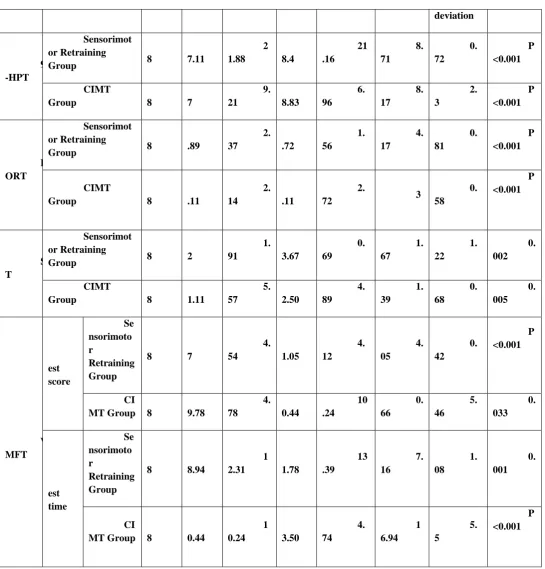
Table 2 shows the distribution of sensorimotor retraining group tests. The results indicate the reduction of 9-HPT test run time, which represents an increase in the hand speed.The reduction in average errors inHORT test reflects the increasing in the sensoryability to touch and evaluating the objects by removing the vision ability. The Astereognosis scores increased.In addition, increasing the WMFT test performance scores and reduction of the time to do activitiesrepresent the increase in operating speed andimproving movement in the upper extremities.Results showed a significant difference in all the tests before and after sensorimotor retraining at p<0.005.
Data normality was evaluated in sensorimotor Retraining. The Paired t-test was used to compare data before and after treatmentin normal data and the Wilcoxon test was used for abnormal data.
Table 3 shows the distribution indicators in limitation therapy group tests. The results indicate the reduction in 9-HPT test average time, reduction in the average error inHORT test, increasing in Astereognosismean scores, increasing in hand performance scores, and reduction in WMFT test performance scores.Since no data of this group have a normal distribution, Wilcoxon test was usedto compare data before and after treatment. Resultsshowed a significant difference in all the tests before and after treatment in both groups at p<0.005.
Discussion
participating in the study, the small number of participants in research.In addition, the assignment source is not specifiedin this study, thus, it is possible that the type of assignments affects the healing.
The previous studies, which have investigated the impact of CIMT on upper extremity motor function in hemiplegic patients, have used Vogel Meier, Minnesota, and Wolf test. The results of the study are consistent with the findings of Bonifer et al., Wulf Kong et al., Abdul Wahab et al., and Pitch et al. (10,19).Evidence shows that an active practice leads to neuroplasticity of the brain motor cortex and improving the motor function in patients with chronic stroke.Patients with stroke should learn the voluntary control of purposeful movements. Practice-based movement learning is a repeated experience that will lead tosustainable changes in the ability of individuals (41).
According to theconsistence of the results in this study and increasing the mean scores of hand motor function test, it can be said at 95% confidence level that the sensorimotor trainingtherapy and CIMT therapy improve the upper extremity function in patients with chronic stroke.However,we achieve more meaningful results by using larger samples and prolonging the treatment time. It is recommended to conduct this study on more statistical samples with spending more time. The two treatment and control groups should be used in the study. The effectiveness of this therapy can be compared with other common rehabilitation approaches such as Rood and Brunnstromapproaches, etc. The effectiveness of this therapy can be evaluated in patients diagnosed with other disorders such as traumatic brain injury, Parkinson's disease, orthopedic problemsand even elderly healthy subjects. Since the type of treatmentwas based on play activities,the interventionstype caused less cooperation in a number of people at the beginning and in the following of the study. The similarity of some depression and therapeutic intervention cases reduced the tolerance of some participants during treatment. Due to the type of interventions, it was not possible to follow and perform similarexercises at home to achieve better results.
Table 1. The normal distribution of mean, standard deviation of age, duration, cognitive test distinguished by two groups
Variab les
SensorimotorGr oup
CIMT Group Signifi
cance level
M ean
Standar d deviation
M ean
Standa rd deviation
Age ( YEAR)
5 8.83
10.18 5
8.11
8.35
Durati on (months)
5 4.33
32.76 3
6.67
17.93
Cogniti ve test score
2 5.56
2.68 2
5.89
3.05
V ariable s
Groups
N umber of partici pants
Before treatment After
treatment
The difference between two groups
S ignificanc e level M
ean
S tandard deviation
M ean
St andard deviation
B efore treatment
Af ter treatment
M
ean St
Table 2. The normal distribution of mean, standard deviation, the significance level of … tests distinguished by two groups deviation 9 -HPT Sensorimot or Retraining Group 1 8 4 7.11 2 1.88 3 8.4 21 .16 8. 71 0. 72 P <0.001 CIMT Group 1 8 4 7 9. 21 3 8.83 6. 96 8. 17 2. 3 P <0.001 H ORT Sensorimot or Retraining Group 1 8 8 .89 2. 37 4 .72 1. 56 4. 17 0. 81 P <0.001 CIMT Group 1 8 5 .11 2. 14 8 .11 2.
72 3
Vari ables
Groups Nu
mber of participants
Before treatment After
treatment Sig
nificance level M
ean
S tandard deviation
M ean
S tandard deviation
B efore treatment
References
1. Mathiowetz V, Weber K, Kashman N, Volland G. Adult norms for the nine-hole peg test of finger
dexterity. OTJR: Occupation, Participation and Health. 1985;5(1):24-38.
2. Wolf SL, Lecraw DE, Barton LA, Jann BB. Forced use of hemiplegic upper extremities to reverse the
effect of learned nonuse among chronic stroke and head-injured patients. Experimental neurology. 1989;104(2):125-32.
3. Kalisch T, Kattenstroth J-C, Kowalewski R, Tegenthoff M, Dinse HR. Cognitive and tactile factors
affecting human haptic performance in later life. PLoS One. 2012;7(1):e30420.
4. Kalisch T, Tegenthoff M, Dinse HR. Improvement of sensorimotor functions in old age by passive sensory
stimulation. Clinical interventions in aging. 2008;3(4):673.
M ean S tandard deviation 9-HPT Sensorimoto
r Retraining Group 18
4 7.11 2 1.88 3 8.4 2 1.16 8 .71 0
.72 P<0
.001
CIMT
Group 18
4 7 9 .21 3 8.83 6 .96 8 .17 2 .3 HOR T Sensorimoto
r Retraining Group 18
8 .89 2 .37 4 .72 1 .56 4 .17 0 .81 P<0 .001 CIMT
Group 18
5 .11 2 .14 8 .11 2
.72 3
0 .58
Aster eognosis
Sensorimoto
r Retraining Group 18
2 2 1 .91 2 3.67 0 .69 1 .67 1 .22 P<0 .001 CIMT
Group 18
2 1.11 5 .57 2 2.50 4 .89 1 .39 0 .68 WM FT T est score Sens orimotor Retraining Group
18 6
7 4 .54 7 1.05 4 .12 4 .05 0
.42 P<0
.001
CIM
T Group 18
6 9.78 4 .78 7 0.44 1 0.24 0 .66 5 .46 T est time Sens orimotor Retraining Group
18 6
8.94 1 2.31 6 1.78 1 3.39 7 .16 1
.08 P<0
.001
CIM
T Group 18
5. Catley MJ, Tabor A, Wand BM, Moseley GL. Assessing tactile acuity in rheumatology and musculoskeletal medicine—how reliable are two-point discrimination tests at the neck, hand, back and foot? Rheumatology. 2013;52(8):1454-61.
6. Cheema SA, Ahmad A. FREQUENCY OF SENSORY DEFICIT IN TERMS OF TWO POINT
DISCRIMINATION IN SPLIT THICKNESS SKIN GRAFTS AND LOCAL FLAPS FOR SOFT TISSUE DEFECTS OF FINGERS. J Ayub Med Coll Abbottabad. 2012;24(1).
7. Minoo K., Medina, H., Kazem, H., Ghorban Tez. Evaluating the level of hadn Astereognosis in children
with spastic hemiplegia and dipelgia, 3 to 6 years old.
8. Higgins J, Mayo NE, Desrosiers J, Salbach NM, Ahmed S. Upper-limb function and recovery in the acute
phase poststroke. J Rehabil Res Dev. 2005;42(1):65-76.
9. Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, et al. Executive summary: heart
disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121(7):948.
10. Mazloum, Seyed Reza, Bahrami, Mahnaz, Zadeh H., Farzaneh, et al. the impact of mirror theraphy on
motor ability of patients after stroke. Journal of Evidence-based care. 2013; 3 (3): 7-18.
11. Pendleton HM, Schultz-Krohn W. Pedretti's occupational therapy: practice skills for physical dysfunction:
Elsevier Health Sciences; 2013.
12. Doyle S, Bennett S, Fasoli SE, McKenna KT. Interventions for sensory impairment in the upper limb after
stroke. The Cochrane Library. 2010.
13. Blanton S, Wolf SL. An application of upper-extremity constraint-induced movement therapy in a patient
with subacute stroke. Physical therapy. 1999;79(9):847-53.
14. Szaflarski JP, Page SJ, Kissela BM, Lee J-H, Levine P, Strakowski SM. Cortical reorganization following
modified constraint-induced movement therapy: a study of 4 patients with chronic stroke. Archives of physical medicine and rehabilitation. 2006;87(8):1052-8.
15. Yekutiel M, Guttman E. A controlled trial of the retraining of the sensory function of the hand in stroke
patients. Journal of Neurology, Neurosurgery & Psychiatry. 1993;56(3):241-4.
16. Carey L, Macdonell R, Matyas TA. SENSe: Study of the Effectiveness of Neurorehabilitation on Sensation
A Randomized Controlled Trial. Neurorehabilitation and neural repair. 2011;25(4):304-13.
17. Byl NN, Nagajaran S, McKenzie AL. Effect of sensory discrimination training on structure and function in
patients with focal hand dystonia: a case series. Archives of physical medicine and rehabilitation. 2003;84(10):1505-14.
18. Oujamaa L, Relave I, Froger J, Mottet D, Pelissier J-Y. Rehabilitation of arm function after stroke.
Literature review. Annals of physical and rehabilitation medicine. 2009;52(3):269-93.
19. Amini, Naser, Bagheri, Hossein, Abdul Wahab, Baghestani, et al. Evaluating the impact of CIMT on the
quality of life, function and range of motion of upper extremity stroke patients are adults. Modern Rehabilitation. 2012; 6 (3): 1-4.
20. Abdul Wahab, Bagheri, Hossein, Movahedian, Maryam, Aliyaei, et al. Evaluating the impact of CIMT on
the quality of life, in hemiplegic adult patients. Modern Rehabilitation. 2009; 3 (1): 28-32.
21. Hejazi sham, Azad, A, Taghi, Zagh, Shen Street, M Square, M Boulevard, et al. Evaluating the impact of
22. Bailey MJ, Riddoch MJ, Crome P. Evaluation of a test battery for hemineglect in elderly stroke patients for use by therapists in clinical practice. NeuroRehabilitation. 2000;14(3):139-50.
23. Bird T, Choi S, Goodman L, Schmalbrock P, Nichols-Larsen DS. Sensorimotor Training Induced Neural
Reorganization After Stroke: A Case Series. Journal of neurologic physical therapy: JNPT. 2013;37(1):27.
24. Hamedi, D., Delavari, L., Ghomashchi, H., Binesh, M., Taghi, Zagh,University of Pt, et al. The effect of
induced movement therapy technique using wedge on weight bearing symmetry and balance of functional chronic hemiparesis.
25. Volpe B, Krebs H, Hogan N, Edelstein L, Diels C, Aisen M. A novel approach to stroke rehabilitation
Robot-aided sensorimotor stimulation. Neurology. 2000;54(10):1938-44.
26. Scalha TB, Miyasaki E, Lima NMFV, Borges G. Correlations between motor and sensory functions in