Computerized Order Entry With Limited Decision
Support to Prevent Prescription Errors in a PICU
WHAT’S KNOWN ON THIS SUBJECT: Prescription errors are prevalent in pediatric institutions, and error rates are even higher in PICUs. CPOE with and without a CDSS was suggested as an important tool for reducing prescription errors, but its impact in pediatrics is unclear.
WHAT THIS STUDY ADDS: CPOE combined with a CDSS limited to weight-based dosing can significantly reduce prescription error rates. However, computerized systems themselves can lead to new types of medication errors. Therefore, constant surveillance with a search for innovative solutions is necessary.
abstract
OBJECTIVE:The value of computerized physician order entry (CPOE) and clinical decision support systems (CDSSs) in preventing prescrip-tion errors in pediatrics is unclear. We investigated the change in prescription error rates with the introduction of CPOE with and without a CDSS limited to weight-based dosing in a PICU.
METHODS:In a PICU of a major tertiary-care pediatric medical center, 5000 orders were reviewed, that is, 1250 orders from each of 4 periods: period 1, before CPOE implementation; period 2, 1 year after CPOE implementation; period 3, after CDSS implementation; and period 4, after a change in pre-scription authorization. Prepre-scription errors were identified and classified into: potential adverse drug events (ADEs), medication prescription errors (MPEs), and rule violations (RVs).
RESULTS:We identified 273 errors (5.5%). The rate of potential ADEs de-creased slightly between periods 1 and 2 (from 2.5% to 2.4%) and signifi-cantly in periods 3 and 4 (to 0.8% and 0.7%, respectively;P⬍.005). The rate of MPEs decreased slightly between periods 1 and 2 (from 5.5% to 5.3%), but new types of MPEs appeared. There was a significant decrease in period 3 (to 3.8%;P⬍.05) and a dramatically significant decrease in period 4 (to 0.7%;P⬍.0005). Only 3 RVs were found. Interrater agreement (statistic) was 0.788 between evaluators.
CONCLUSIONS:CPOE implementation decreased prescription errors only to a small extent. However, the addition of a CDSS that limits doses by weight significantly reduced prescription error rates and, most impor-tantly, potential ADEs. This finding emphasizes the major impact of weight-based calculation errors in pediatrics.Pediatrics2009;124:935–940 CONTRIBUTORS:Gili Kadmon, MD,aEfrat Bron-Harlev,
MD,aElhanan Nahum, MD,aOfer Schiller, MD,aGali Haski,
BA,band Tommy Shonfeld, MDa
aPediatric Intensive Care Unit andbPharmacy Department, Schneider Children’s Medical Center of Israel, Petach Tikva, Israel
KEY WORDS
medication error, patient safety, computer physician order entry, clinical decision support, pediatrics, adverse drug events
ABBREVIATIONS
ADE—adverse drug event
MPE—medication prescription error RV—rule violation
CPOE— computerized physician order entry CDSS— clinical decision support system CI— confidence interval
www.pediatrics.org/cgi/doi/10.1542/peds.2008-2737
doi:10.1542/peds.2008-2737
Accepted for publication Feb 20, 2009
Address correspondence to Gili Kadmon, MD, Schneider Children’s Medical Center of Israel, Pediatric Intensive Care Unit, Petach Tikva 49202, Israel. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
of medication errors on patient mor-bidity and mortality and medical costs.1–10Studies have shown a higher
rate of medication errors in pediatric patients, most of them being dosing er-rors in the prescription stage.5–18
Pre-scription error rates are even higher in the pediatric intensive care set-ting11–13 for several reasons: (1) the
large number of drugs prescribed to each patient; (2) the high incidence of organ failure, which requires dose ad-justments; and (3) the dramatic weight changes that critically ill pediatric pa-tients undergo. Errors in the prescrip-tion stage can be divided into potential adverse drug events (ADEs), medica-tion prescripmedica-tion errors (MPEs), and rule violations (RVs)5(Table 1).
Many medical associations have en-dorsed computerized physician order entry (CPOE) as an important tool in reducing medication errors.2–8,16
Clini-cal studies in adults support this ap-proach.1–4,19 In children, however, the
data are limited. The few studies per-formed in the pediatric setting re-ported an overall decrease in pre-scription errors when CPOE was applied.5,6,17 There was a statistically
significant drop in MPEs and RVs, but potential ADEs were reduced to a lesser extent or not at all. Others found that specific types of prescrip-tion errors were computer relat-ed.7,20 Han et al8 reported that, in 1
pediatric hospital, the mortality rate unexpectedly increased after CPOE was implemented.
CPOE to check drug prescriptions for incorrect dosing, potential drug-drug interactions, and patient allergies, but their value remains controversial. Some studies have shown an addi-tional reduction in prescription errors with CPOE that included a CDSS,3–5,17
whereas others have not.21,22We found
no studies that evaluated the isolated impact of the CDSS. Walsh et al17
dem-onstrated only a minor reduction in prescription errors in a children’s hos-pital using a CPOE with dosing check-ing alerts. Most of the doscheck-ing errors were not intercepted by the computer because the dosing limits were appro-priate for adults but not for children. Given that most prescription errors in children are weight-based errors in dosing calculations,5–18 we sought to
determine whether CPOE with and without a CDSS limited to weight-based dosage surveillance is effective in re-ducing prescription errors in a PICU.
METHODS
Setting
The study was conducted in a 12-bed PICU in a tertiary children’s hospital (Schneider Children’s Medical Center of Israel) with⬃1100 admissions per year. The mean (SD) age of our pa-tients was 6.5 years (⫾7.5 years). As part of the unit’s routine protocol, the drug-order list of every patient is re-viewed daily by a senior physician dur-ing morndur-ing rounds and again by a pharmacist on weekdays.
In November 2004, a computerized in-formation system that includes CPOE (Metavision [iMDsoft, Tel Aviv, Israel]) was implemented in our PICU. Its main purpose, according to the unit’s team, was to reduce prescription errors. However, when dosage errors contin-ued to be found 1 year later, decision-support tools that checked medication dosages were added. Each drug was assigned 2 dosage limits: normal and legal. A normal limit was defined as
⬎10% deviation from the recom-mended dosage (eg, 65 mg/kg of ceftri-axone intravenously) according to ac-cepted drug databases (eg, Medline, Epocrates, and the Drug Book of the General Health Services, the largest health management organization in the country, which runs the Schneider Children’s Medical Center of Israel). A legal limit was defined as a dose that is highly unlikely to be prescribed inten-tionally in any medical circumstance, usually 2 to 3 times the normal limit (eg, 200 mg/kg of ceftriaxone intrave-nously). The limits determined were for every single dose prescribed (as opposed to a daily cumulative dose). If a physician prescribed a drug at a dose above its normal limit, the com-puter issued a warning before it ac-cepted the order; if a physician pre-scribed a drug at a dose above its legal limit, the computer did not accept the order at all. Underdosing, as opposed to overdosing, could not be prevented by the CPOE. In addition, a default pre-scription was customized for each drug that automatically appeared in the prescription form when a physi-cian entered the drug (ie, recom-mended dose in units per kilogram, frequency of administration, route, and recommended dose adjustments according to organ failure). The imple-mentation of the decision-support tools was completed in July 2006. At
TABLE 1 Types of MPEs
Potential ADE Incorrect prescription that could cause harm to the patient if executed, including wrong drug (eg, no indication, patient allergy, or drug interaction), wrong dose (eg, according to weight, age, or organ dysfunction), wrong units, wrong interval, and wrong route
MPE Incomplete or illegible prescription that requires further clarification in order to be executed, including missing rate of administration, missing units, and illegible handwriting
present, our computerized informa-tion system contains no other CDSS el-ements, such as drug interactions or drug allergy alerts.
After implementation of the CPOE sys-tem, we found that, in a high percent-age of cases, prescriptions had been signed electronically by a nurse in-stead of a physician. This MPE oc-curred when a physician entered the order while a nurse was logged on to the computer. Therefore, in July 2007, the CPOE settings were adjusted such that drugs could be prescribed only by a physician. This allowance limitation did not include over-the-counter drugs (eg, oral antipyretics).
Study Design
In this retrospective study, we calcu-lated the prescription error rates be-fore and after CPOE implementation and after our limited CDSS implemen-tation. The study was approved by the institutional review board; the need for informed consent was waived by the board. A total of 5000 PICU drug pre-scriptions were reviewed, consisting of 1250 consecutive prescriptions in each of the following months: period 1, September 2004, 1 month before CPOE implementation; period 2, September 2005, 1 year after CPOE implementa-tion; period 3, September 2006, at com-pletion of CDSS implementation; and period 4, September 2007, after the drug allowance limitation.
Prescriptions were reviewed by Dr Kadmon, a senior PICU physician. A randomly selected 10% of prescrip-tions from each time period were also independently reviewed by Ms Haski, a clinical PICU pharmacist, and the level of agreement with the PICU physician was determined. Prescription errors of all types were identified and classi-fied as potential ADEs, MPEs, or RVs. A potential ADE was defined as an incor-rect prescription that could cause harm to the patient if executed (ie,
in-correct drug, dose, units, interval, or route). A dosing error was defined as a
⬎10% deviation from the recom-mended dose according to accepted drug databases (described above). An MPE was defined as an incomplete or illegible prescription that required ad-ditional clarification to be executed. An RV was defined as a prescription writ-ten in a manner that was not compliant with institutional regulations (eg, use of abbreviations). The PICU mortality rate for each year of the study was cal-culated as well.
Statistical Analysis
Assuming a prescription error rate of 10%,3,9,12,13,18 we calculated that we
needed to reviewⱖ1100 orders from each time period of the study to achieve a statistical power of 80% to detect an absolute risk reduction in the prescription error rate of 3% in time periods 2, 3, and 4 each, with a 2-sided significance level of .05. We de-cided to review 1250 orders from each time period, for a total of 5000 orders.
Data were analyzed by using BMDP sta-tistical software (University of Califor-nia, Los Angeles, CA). Pearson’s2test
was used to compare differences in rates of prescription errors between periods. The statistic was used to evaluate interrater reliability. APvalue ofⱕ.05 was considered significant.
RESULTS
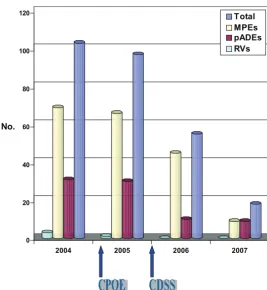
Among the 5000 prescriptions re-viewed, 273 (5.5%) contained prescrip-tion errors (Table 2). The implementa-tion of CPOE was associated with only a
slight and nonsignificant decrease in the prescription error rate (between periods 1 and 2; P ⫽ .66). The de-creases in the rate of prescription er-rors after CDSS implementation (be-tween periods 2 and 3) and after prescription authorization (between period 3 and 4) were statistically sig-nificant (P⬍.0005 for both). Overall, prescription errors were reduced by 83% (Fig 1).
Potential ADEs
The rates of potential ADEs were sim-ilar in periods 1 and 2. In period 3, there was a significant decrease (from 2.4% to 0.8%;P⬍.005), which persisted in period 4. Overall, poten-tial ADEs were reduced by 72%. Most were caused by dose errors, in all of the time periods: 24 (77%) of 31 in period 1; 25 of (83%) 30 in period 2; 6 (60%) of 10 in period 3, and 5 (55%) of 9 in period 4. Because of the CDSS alerts of overdosages, from period 3 onward, most of the potential ADEs were attributed to underdosages (eg, 6 mg/kg per dose of vancomycin intravenously). Nondosing prescrip-tion errors that were not prevented by the CPOE were mainly errors in dose frequency or infusion rate (eg, intravenous platelet infusion over 24 hours instead of 1 hour).
Medication Prescription Errors
The rate of MPEs dropped slightly and not significantly between period 1 and 2, from 5.5% to 5.3%, and then consid-erably in period 3, to 3.8% (P⬍.05). A significant decrease also occurred in
TABLE 2 Prescription Errors Rates According to Type and Time Period
Variable Period 1, 2004 (Pre-CPOE),
n(%)
Period 2, 2005 (CPOE)
Period 3, 2006 (CPOE⫹CDSS)
Period 4, 2007 (Allowances
Changes)
n(%) P n(%) P n(%) P
Total errors 103 (8.2) 97 (7.8) .66 55 (4.4) .0004 18 (1.4) ⬍.0001
Potential ADEs 31 (2.5) 30 (2.4) .9 10 (0.8) .0014 9 (0.7) .82
MPEs 69 (5.5) 66 (5.3) .79 45 (3.8) .04 9 (0.7) .0001
RVs 3 (0.002) 1 (0.001) .3 0 (0) .3 0 (0) 1
period 4, to 0.7% (P⬍.0005). In period 1, most of the MPEs consisted of in-complete orders. In periods 2 and 3, all of the orders were complete, and most of the MPEs consisted of a nurse’s elec-tronic signature instead of a physi-cian’s. This type of error disappeared in period 4.
Rule Violations
Three RVs were identified in period 1, before CPOE implementation, and only 1 thereafter.
Interrater Reliability
Using the measured number of errors, total and by category, identified by the 2 evaluators, we calculated the inter-rater reliability (statistic) to be 0.788 (95% confidence interval [CI]: 0.638 – 0.938) for total errors, 0.676 (95% CI: 0.432– 0.952) for potential ADEs, and 0.943 (95% CI: 0.832–1.000) for MPEs. The agreement was 1.000 for RVs. These values indicate substantial (⫽
0.61– 0.80) to almost complete ( ⫽ 0.81–1.00) agreement between the 2 evaluators.
Mortality
The annual PICU mortality rate was 2.79% in 2004 (period 1), 3.87% in 2005 (period 2), 3.30% in 2006 (period 3), and 2.37% in 2007 (period 4). There were no statistically significant dif-ferences in mortality rates by time period.
DISCUSSION
The present study indicates that, in our PICU, CPOE implementation re-duced the prescription error rate only slightly. After the addition of CDSS tools that limited medication doses according to weight, the rate of prescription errors dropped sig-nificantly. Most importantly, the rate of potential ADEs decreased to⬍1%. The reduction in dose errors at our center is in contrast to the findings
use of weight-based limits (ex-pressed in milligrams per kilogram) in our system, whereas in the system reviewed by Walsh et al,17limits were
based on the maximum adult doses (eg, the upper limit for acetamino-phen defined as 25 mg/kg per dose at our center rather than 1 g per dose). Therefore, our system prevented most of the dosage errors in chil-dren, which were still within the ac-cepted limits for adults.
The reason for the decrease in MPEs after implementation of CPOE is obvi-ous: computerized orders cannot be il-legible or incomplete. Also, the de-crease may be partly explained by the learning curve and the consequent im-provement in staff expertise in CPOE use. However, the decrease in the MPE rate was not as considerable as we had expected because of the emer-gence of a new type of MPE, the elec-tronic signature error. Once its source was identified and corrected, this er-ror also disappeared, and a dramatic decrease in MPEs was achieved. This emphasizes the need for constant sur-veillance for prescription errors. The latter findings are consistent with a previous study on new types of medi-cation errors that have emerged with the introduction of computerized prescriptions.7
One study reported an increase in the patient mortality rate after im-plementation of CPOE.8However, this
study had several methodologic pit-falls: (1) other changes in the work routine were introduced simulta-neously with CPOE; (2) medications were moved from the unit to the pharmacy, significantly increasing the time needed to obtain them, es-pecially resuscitation drugs; and (3) during resuscitation, drugs had to be prescribed through the computer, with no oral or handwritten alterna-FIGURE 1
tive in emergency situations. In our PICU, some medications, including frequently used antibiotics and re-suscitation drugs, are stored in the unit. Our annual PICU mortality is 3%, and this rate did not change after CPOE implementation.
Our study has 2 main limitations. The first is the focus of our study on pre-scription errors, excluding other types of medication errors, mainly at the ad-ministration stage. As mentioned pre-viously, the main goal of implementing the computerized information system in our unit was to reduce prescription errors, and this goal was successfully achieved. However, the effect of this
implementation on other types of med-ication errors in our unit remains to be examined.
The second limitation is the retro-spective nature of the work. A few recent studies of medication errors used a prospective, direct-observation method for error detection.12,18This
re-quires that the observer be present on the ward and follow the process of drug prescription, transcription, prep-aration, and administration to detect different errors in the various stages. However, for the detection of prescrip-tion errors alone, a retrospective chart review is accepted as a reliable design.6–8,10,14,15
CONCLUSIONS
CPOE combined with a CDSS limited to weight-based dosing can signifi-cantly reduce prescription error rates in the PICU, most importantly, potential ADEs. Physicians should be aware that the newly implemented computerized systems can them-selves lead to new types of medica-tion errors. Therefore, constant sur-veillance with a search for innovative solutions is necessary.
ACKNOWLEDGMENTS
We thank Pearl Lilos for help with the statistical analysis and Gloria Ginzach for the English-language editing.
REFERENCES
1. Bates DW, Leape LL, Cullen DJ, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors.JAMA.1998;280(15):1311–1316
2. Shulman R, Singer M, Goldstone J, Bellingan G. Medication errors: a prospective cohort study of hand-written and computerized physician order entry in the intensive care unit.Critical Care.
2005;9(5):R516 –R521
3. Kaushal R, Shojania KG, Bates DW. Effects of computerized physician order entry and clinical decision support systems on medication safety.Arch Intern Med.2003;163(12):1409 –1416
4. Colpaert K, Claus B, Somers A, Vandewaude K, Robays H, Decruyenaere J. Impact of computerized physician order entry on medication prescription errors in the intensive care unit: a controlled cross-sectional trial.Crit Care.2006;10(1):R21–R30
5. Potts AL, Barr FE, Gregory DF, Wright L, Patel NR. Computerized physician order entry and medi-cation errors in a pediatric critical care unit.Pediatrics.2004;113(1 pt 1):59 – 63
6. King WJ, Paice N, Rangrej J, Forestell GJ, Swartz R. The effect of computerized physician order entry on medication errors and adverse drug events in pediatric inpatients.Pediatrics.2003; 112(3 pt 1):506 –509
7. Walsh KE, Adams WG, Bauchner H, et al. Medication errors related to computerized order entry for children.Pediatrics.2006;118(5):1872–1879
8. Han YY, Carcillo JA, Venkataraman ST, et al. Unexpected increased mortality after implementation of a commercially sold computerized physician order entry system.Pediatrics. 2005;116(6): 1506 –1512
9. Kozer E, Berkovitch M, Koren G. Medication errors in children.Pediatr Clin North Am.2006;53(6): 1155–1168
10. Taylor BL, Selbst SM, Shah AEC. Prescription writing errors in the pediatric emergency depart-ment.Pediatr Emerg Care.2005;21(12):822– 827
11. Rothschild JM, Landrigan CP, Cronin JW, et al. The critical care safety study: the incidence and nature of adverse drug events and serious medical errors in intensive care.Crit Care Med.
2005;33(8):1694 –1700
12. Kopp BJ, Erstad BL, Allen ME, Theodorou AA, Priestley G. Medication errors and adverse drug events in an intensive care unit: direct observation approach detection.Crit Care Med.2006;34(2): 415– 425
13. Ridley SA, Booth SA, Thompson CM; Intensive Care Society’s Working Group on Adverse Incidents. Prescription errors in UK critical care units.Anaesthesia.2004;59(12):1193–1200
14. Lehmann CU, Kim GR, Gujral R, Veltry MA, Clark JS, Miller MR. Decreasing errors in pediatric continuous intravenous infusions.Pediatr Crit Care Med.2006;7(3):225–230
15. Killelea BK, Kaushal R, Cooper M, Kuperman GJ. To what extent do pediatricians accept computer-based dosing suggestions?Pediatrics.2007;119(1). Available at: www.pediatrics.org/cgi/content/ full/119/1/e69
17. Walsh KE, Landrigan CP, Adams WG, et al. Effect of computer order entry on prevention of serious medication errors on hospitalized children.Pediatrics.2008;121(3). Available at: www.pediatrics.org/ cgi/content/full/121/3/e421
18. Buckley MS, Erstad BL, Kopp BJ, Theodorou AA, Priestley G. Direct observation approach for detecting medication errors and adverse drug events in a pediatric intensive care unit.Pediatr Crit Care.2007;8(2):145–152
19. Mirco A, Campos L, Falcao F, Nunes JS, Aleixo A. Medication errors in an internal medicine department: evaluation of a computerized prescription system.Pharm World Sci.2005;27(4): 351–352
20. Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors.JAMA.2005;293(10):1197–1203
21. Wolfstadt JI, Gurwitz JH, Field TS, et al. The effect of computerized physician order entry with clinical decision support on the rates of adverse drug events: a systematic review.J Gen Intern Med.2008;23(4):451– 458
DOI: 10.1542/peds.2008-2737 originally published online August 10, 2009;
2009;124;935
Pediatrics
Tommy Shonfeld
Gili Kadmon, Efrat Bron-Harlev, Elhanan Nahum, Ofer Schiller, Gali Haski and
Prescription Errors in a PICU
Computerized Order Entry With Limited Decision Support to Prevent
Services
Updated Information &
http://pediatrics.aappublications.org/content/124/3/935 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/124/3/935#BIBL This article cites 19 articles, 4 of which you can access for free at:
Subspecialty Collections
chnology_sub
http://www.aappublications.org/cgi/collection/health_information_te
Health Information Technology
sub
http://www.aappublications.org/cgi/collection/quality_improvement_
Quality Improvement
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice
Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2008-2737 originally published online August 10, 2009;
2009;124;935
Pediatrics
Tommy Shonfeld
Gili Kadmon, Efrat Bron-Harlev, Elhanan Nahum, Ofer Schiller, Gali Haski and
http://pediatrics.aappublications.org/content/124/3/935
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.