4
Int J Res Med. 2014; 3(1);4-8 e ISSN:2320-2742 p ISSN: 2320-2734A hospital based study on the prevalence of low birth weight in newborn babies
and its relation to maternal health factors
Krupal Joshi
1*, Kishor M. Sochaliya
2, Atul V. Shrivastav
3, Divyesh M. Gohel
4,
Shyamal K. Purani
5, Girija P. Kartha
51Resident, 2Assistant Professor 5Professor, Department of PSM, C.U. Shah Medical College Surendranagar, Gujarat 3Assistatn Professor, Department of Pathology, C.U. Shah Medical College Surendranagar, Gujarat
4Resident, Department of Paediatrics, C.U. Shah Medical College Surendranagar, Gujarat
INTRODUCTION
Intrauterine growth and development is one of the most vulnerable processes in the human life cycle and its aberrations can result in profound and lasting influence in later life. In the context of developing countries, intrauterine growth has been invariably assessed by birth weight1. The birth weight of an infant is the single most significant determinant of its chances of survival, healthy growth and development2. Low birth weight is one of the most serious challenges in maternal and child health in both developed and developing countries. Its public health significance may be ascribed to numerous factors – its high incidence, its association with mental retardation and a high risk of perinatal and infant mortality, human wastage and suffering, the very high cost of special careand intensive care unit
and its association with socioeconomic
underdevelopment2. Low birth weight is considered as a sensitive index of Nation’s health and development4. The NFHS 3 reports association of LBW to place of residence (urban or rural), age of
*Corresponding Author
Dr. Krupal J. Joshi
87, “Aashutosh”, Sanjivani Society, Ratanpur Surendranagar-363020
Email:
dr_krupal@yahoo.co.in
mother, religion and caste, birth order of the baby, education, wealth and use of tobacco5. The incidence of LBW babies (< 2500 gm) continues to be high in India at about 30% in contrast to 5-7% in developed countries6. Preterm babies account for only 10% LBW babies, the rest being term intrauterine growth retarded (IUGR) infants7. With this background, the present study was conducted with following objectives.
Objectives: The objectives of the study were; 1. To estimate the prevalence of low birth weight
among new born babies.
2. To identify various maternal factors associated with low birth weight of newborns.
MATERIALS AND METHODS
The present hospital based cross-sectional study was conducted in a tertiary care teaching hospital C. U. Shah Hospital, Surendranagar, Gujarat. The period of study was 3 month (i.e. from September 2012 to November 2012). The study population comprised of mothers along with newborns delivered at C. U. Shah Hospital during the study period. Of the total 116 deliveries occurred during this 3 months, mothers of 109 new born babies were interviewed and examined using a predesigned and pretested questionnaires. The remaining 7 mothers
ORIGINAL ARTICLE
ABSTRACT
BACKGROUND: Low birth weight (LBW) is defined as birth weight of < 2.5 kg. Birth weight is a reliable index
of intra uterine growth retardation and a major factor determining child survival, future physical growth and mental development. A multifactorial inter-relationship exists between the environment in which pregnant mothers live and the growth of the fetus. Objective: To estimate the prevalence of LBW among new born babies and to study the association of LBW with maternal risk factors. MATERIALS AND METHODS: A total of 109 live new born babies delivered at Ob. & Gy. Department of C U Shah Hospital were reviewed from September to November 2012. The data was collected with the help of interview technique using predesigned and pretested questionnaires followed by thorough clinical examination and anthropometric measurements of mothers. RESULTS: The mean birth weight of newborns was 2.76 kg with a range of 2.20 to 3.32 kg. The prevalence of LBW was 55.96%. The factors which were significant for LBW were poor socio-economic status, antenatal care, gestational age, parity, inter-pregnancy interval and past H/o of maternal illness. CONCLUSION: LBW was found to be present in 61 (55.96%) newborns. The factors that found significantly associated with LBW were gestational age at delivery, number of antenatal visits, past history of maternal illness, birth interval, type of work, iron and folic acid supplementation, sex of new born, residency, socio-economic class and parity.
5
Int J Res Med. 2014; 3(1);4-8 e ISSN:2320-2742 p ISSN: 2320-2734were excluded due to immediate transfer, non response, non co-operation for examination and
incomplete information. The World Health
Organization (WHO) definition of LBW was used, i.e., birth weight less than 2500g3. The birth weight of new born was recorded within 1 hour of delivery. Modified Prasad’s classification was used to grade the socio-economic status of the respondents. Study variables included were birth weight and sex of baby, maternal socio-demographic profile, mother’s anthropometric & reproductive profile like height and weight, parity, inter-pregnancy interval, gestational age, number of ANC visits, iron and folic acid supplementation, hemoglobin status and past history of maternal illness. The information thus collected was analysed using SPSS windows. Simple proportions and chi-square were used to analyse the data.
RESULTS
Table 1: Distribution of new borns according to birth weight (n = 109)
Birth weight(kg) No. of newborns Percentage Mean Weight SD < 2.5 kg 61 55.96 1.9 kg ± 0.34
2.5-3.5 kg 46 42.20 2.8 kg ± 0.21
≥ 3.5 kg 2 01.84 3.6 kg ± 0.14
Total 109 100 2.76 kg ± 0.56
Table 2: Relationship between LBW and maternal socio-demographic factors (n = 109)
Material SD factors No. of new Born Normal Babies LBW X2 P Valu e No. %
Maternal age
< 20 13 6 7 53.84
0.057 0.999
21-25 53 23 30 56.60
26-30 32 14 18 56.25
31-35 10 5 5 50.00
> 35 1 0 1 100.0 Type of Residence
Urban 29 20 9 31.03
9.964 0.001
Rural 80 28 52 65.00 Maternal Education
Illiterate 60 21 39 65.00
5.823 0.054
Primary 44 23 21 47.73
Secondary 5 4 1 20.00 Maternal Occupation
Farmer 27 9 18 66.67
10.12 0.017
Housewife 50 30 20 40.00
Laborer 30 8 22 73.33
Home
business 2 1 1 50.00
Socio Economical status
Class 1 0 0 0 00.00
12.77 0.005
Class 2 1 1 0 00.00
Class 3 21 16 5 23.81
Class 4 59 22 37 62.71
Class 5 28 9 19 67.86
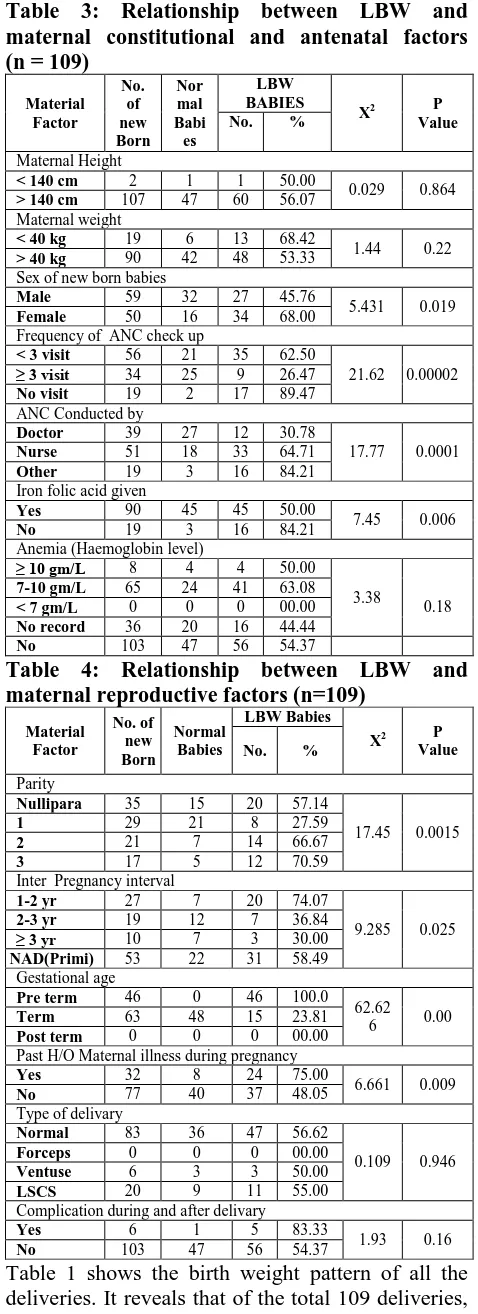
Table 3: Relationship between LBW and maternal constitutional and antenatal factors (n = 109)
Material Factor No. of new Born Nor mal Babi es LBW BABIES
X2 P
Value No. %
Maternal Height
< 140 cm 2 1 1 50.00
0.029 0.864
> 140 cm 107 47 60 56.07 Maternal weight
< 40 kg 19 6 13 68.42
1.44 0.22
> 40 kg 90 42 48 53.33 Sex of new born babies
Male 59 32 27 45.76
5.431 0.019
Female 50 16 34 68.00 Frequency of ANC check up
< 3 visit 56 21 35 62.50
21.62 0.00002
≥ 3 visit 34 25 9 26.47
No visit 19 2 17 89.47 ANC Conducted by
Doctor 39 27 12 30.78
17.77 0.0001
Nurse 51 18 33 64.71
Other 19 3 16 84.21 Iron folic acid given
Yes 90 45 45 50.00
7.45 0.006
No 19 3 16 84.21
Anemia (Haemoglobin level)
≥ 10 gm/L 8 4 4 50.00 3.38
0.18
7-10 gm/L 65 24 41 63.08
< 7 gm/L 0 0 0 00.00
No record 36 20 16 44.44
No 103 47 56 54.37
Table 4: Relationship between LBW and maternal reproductive factors (n=109)
Material Factor No. of new Born Normal Babies LBW Babies
X2 P
Value No. %
Parity
Nullipara 35 15 20 57.14
17.45 0.0015
1 29 21 8 27.59
2 21 7 14 66.67
3 17 5 12 70.59
Inter Pregnancy interval
1-2 yr 27 7 20 74.07
9.285 0.025
2-3 yr 19 12 7 36.84
≥ 3 yr 10 7 3 30.00
NAD(Primi) 53 22 31 58.49 Gestational age
Pre term 46 0 46 100.0 62.62
6 0.00
Term 63 48 15 23.81
Post term 0 0 0 00.00 Past H/O Maternal illness during pregnancy
Yes 32 8 24 75.00
6.661 0.009
No 77 40 37 48.05
Type of delivary
Normal 83 36 47 56.62
0.109 0.946
Forceps 0 0 0 00.00
Ventuse 6 3 3 50.00
LSCS 20 9 11 55.00 Complication during and after delivary
Yes 6 1 5 83.33
1.93 0.16
No 103 47 56 54.37
6
Int J Res Med. 2014; 3(1);4-8 e ISSN:2320-2742 p ISSN: 2320-2734LBW with the different socio-demographic factors of the mother. The factors which were found to be significantly associated with the low birth weight of the newborns were type of residence, type of work and socio-economic status. However, age of the mother at the time of conception and maternal education were found insignificant in the present study. The birth weight is found to be lowest in the babies of mothers in the age group of 21-30 years. Higher prevalence of LBW neonates were found among mothers who were living in rural areas (65%) compared to urban area (31.03%). The birth weight of newborn babies was also influenced by educational status of mothers, as 65 % of illiterate mothers delivered their babies with LBW. Majority of the mothers having LBW babies involved in the hard work like labor (73.33%) and farming (66.67%). And it was observed that maximum mothers born LBW babies were belongs to socio-economic class IV and V (62.71% and 67.86% respectively). Table 3 depicts that the LBW rate was high among mothers with height >140 cm (56.07%) & body weight <40 kg (68.42%). Out of all the registered mothers’ outcome was better in mothers who were going for ANC check up 3 or more times compared to no or less than 3 visits. Similarly, the birth weight of babies seems to be influenced significantly by the person who conducts ANC. As LBW rate was higher among mothers whose antenatal checkup was conducted by nurse or other staff compared to doctor. The prevalence of LBW was also higher among mothers who did not consume IFA tablets during pregnancy (84.21%) compared to those who consumed IFA tablets (50%). Maximum numbers of LBW babies were born to mothers’ with hemoglobin level 7-10 gm/L (63.08%) followed by more than 10 gm/L (50%). The data of table 4 reveal that the rate of LBW babies were high among the mothers with parity three (70.59%) and it decreases with the decrease of parity. The association of parity and LBW babies was also found statistically significant. More number of LBW babies (74.07%) were born to mothers whose inter pregnancy interval was 1-2 year compared to 2-3 year (36.84%) and more than 3 years (30%). Maximum numbers of LBW babies (100%) were born pre-term, which is also statistically significant. Similarly mothers with history of any of the maternal illness during pregnancy delivered more number of LBW babies (75%) compared to no such history. Majority (56.62%) of LBW babies were delivered normally followed by LSCS (55%) and ventuse (50%). Table 5 shows the bivariate analysis of maternal constitutional and reproductive factors among the study subjects.
Table 5: Bivariate analysis of maternal risk factors of low birth weight (n = 109)
Factor MEAN ±SD
95% Confidence
Interval
Level of significa nce Maternal age 25 ± 4.13 (19 - 39) NS
ANC frequency 1.58 ± 1.108 (0 - 3) HS
Inter pregnancy
interval 1.193 ± 1.36 (0 - 5) S Maternal height 150 ± 4.03 (140 - 160) NS
Maternal weight 45.58 ± 7.39 (36 - 71) NS
Anaemia 6.90 ± 3.85 (0 - 12) NS
*HS – Highly significant, S – Significant, NS – Non significant
DISCUSSION
7
Int J Res Med. 2014; 3(1);4-8 e ISSN:2320-2742 p ISSN: 2320-2734also reported by AR Mahmood et al18. The prevalence of LBW was observed maximum among the mothers weighted less than 40 kg (68.42%). And the data has also been supported by the findings of Dhall and Bagga19. LBW was strongly associated with inadequate or no antenatal care, which was supported by PS Thomre et al14. Deshmukh et al17 documented that mothers who were anemic were more prone to have LBW and our findings are in conformity with their observations. Parity of mother is usually associated with birth weight. However, after attaining a maximum weight at fourth or fifth parity a decrease in birth weight with subsequent parity has been seen20, 21. In this work, higher weighted babies are observed in first parity, after which the birth weight is declining with subsequent parity. Present study also revealed that the percentage of low birth weight decreases with increasing inter pregnancy interval. Similar finding were also observed by Ghosh et al (1969)22, Das et al (1977)23 and Deswal BS et al (1999) 24 in their study. In this work strong positive association of gestational age of baby to birth weight is observed. Prevalence of LBW baby is very high in preterm baby than its counterpart. This finding is also corresponds to finding of other workers11, 25. The relationship between maternal diseases and low birth weight is a controversial subject. Maternal diseases, both infectious and chronic diseases, in the present study, were found to be significantly associated with higher proportion of LBW (p=0.009).
CONCLUSION
Birth weight remains an important factor affecting infant and child morbidity and mortality. Babies of low birth weight are also more prone to perinatal morbidities. As there are several factors interacting in this phenomenon, so it is not feasible to single out any particular factor affecting low birth weight. From the present study, it was revealed that the maternal factors like rural locality, laborious work, low economic class, inadequate/no utilization of
antenatal services, inadequate IFA tablets
consumption, multiparity, short inter pregnancy interval, pre-term delivery and past history of maternal illness are found to be significantly associated with LBW.
Recommendation:
The results of the present
study suggest that for reducing the burden of
LBW, it is the need to strengthen the existing
maternal services at the basic level of
community i.e., at door steps of the
beneficiaries if possible. The factors that should
be more focused are maternal literacy and
nutrition status, socio-economic development,
teenage pregnancy, awareness regarding birth
spacing and increasing the use of health care
services during pregnancy.
Limitation:
1. The result of the study cannot be generalized because the present study was a hospital based
study. Other governmental and
non-governmental health sectors were not involved. 2. Precise information regarding weight gain of the
women during pregnancy could not be obtained as majority women are illiterate coming from rural area and not aware about the significance of weight records.
Acknowledgement:
We acknowledge the cooperation extended by Department of Obstetrics and Gynecology and Management of C. U. Shah Medical College and Hospital, Surendranagar.REFERENCES
1.
Sachdev HPS. Low birth weight in South Asia. Int J Diab Dev Countries 2001; 21(1):13-33.2.
Park K. Text book of Preventive and Social Medicine. 22nd edition. Jabalpur Banarsidas Bhanot Publishers, 2013. p. 495-497.3.
World Health Organization (1992)International Statistical classification of diseases and related health problems. Geneva.
4.
Idris MZ, Gupta A, Mohan U, Srivastava AK, Das V. Maternal health and low birth weight among institutional deliveries. Indian Journal of Community Medicine.2000; 25(4):156-160. 5.http://hetv.org/india/nfhs/nfhs3/NFHS-3-Chapter-09-Child-Health.pdf/[accessed on Aug 20th 2013]
6. Bhargava SK. Perspectives in Child Health in India. Indian Pediatr 1991; 28: 1403-1410. 7. Villar J, Alobelli L, Kestler E, Belizan J.
Health priority for developing countries. The prevention of chronic fetal malnutrition. Bull World Health Organ 1986; 64: 847-851. 8. International Institute of Population Sciences,
National Family Health Survey, India. 2005-06 (NFHS-3, Vol. 1) 2007:225.
9. Joshi SM, Pai NP. Effect of the maternal Bio-Social Determinant on Birth Weight in A Slum Area of Greater Mumbai. Indian Journal of Community Medicine 2000; 25(3):121-23.
10. BT Rao, Arun Kumar Aggarwal, Rajesh
Kumar. Dietary intake in third trimester of pregnancy and prevalence of LBW: A community based study in a rural area of Haryana. Indian Journal of Community Medicine 2013; 32(4): 272-276.
11. Das JC, Khanam ST. Maternal determinants of
8
Int J Res Med. 2014; 3(1);4-8 e ISSN:2320-2742 p ISSN: 2320-273412. Ahmed FU, Das AM, Mostafa MG.
Association of maternal biological factors with birth weight in Bangladesh. JOPSOM 1994; 13(2): 52-57.
13. Gagan A, Sartaj A, Kapil G, Vijay Kumar, Parul G, et al. Maternal Risk Factors Associated with Low Birth Weight Neonates in a Tertiary Care Hospital, Northern India. J
Community Med Health Educ 2012;
2:177.doi:10.4172/2161-0711.1000177.
14. Thomre PS, Borle AL, Naik JD, Rajderkar SS.
Maternal risk factors determining birth weight of newborns: A tertiary care hospital based study. International Journal of Recent Trends in Science And Technology, ISSN 2277-2812 E-ISSN 2249-8109, Volume 5, Issue 1, 2012 pp 03-08.
15. Kramer MS. Determinant of low birth weight:
Methodological assessment and Meta analysis. Bull WHO 1987; 65(5): 663-737.
16. Hirve SS, Ganatra BR. Determinants of low birth weight: a community based prospective cohort study. Indian Pediatr 1994; 31:1221-5.
17. Deshmukh JS, Motghare DD, Zodpey SP,
Wadhva SK. Low birth weight and associated maternal factors in an urban area. Indian Pediatr. 1998; 35:33-6.
18.
A R Mahmood, G M Sharful Haque, Tahera Parvin, S R Karim, K Osman, S K Ferdousi. Birth Weight Status of the New Born Babies born at Dhaka Medical College Hospital. The journal of teachers association RMC, Rajshahi, December 2004; 17(2): 95-98.19. Dhall K, Bagga R (1995). Maternal
determinants of birth weight of north Indian babies. Indian J Pediatr 62: 333-344.
20. Oni GA. The effect maternal age, education and parity on birth weight in a Nigerian community: The comparison of results from Bivariate and multivariate analysis. J Trop Pediatr 1986; 32: 295-300.
21. Makhija K, Murthi GVS, Kapoor SK, Lobo J.
Sociobiological determinants of birth weight. Indian J of Pediatr 1989; 56: 639-643.
22. Ghosh S, Hooja V, Mittal SK, Verma RK. Bio-Social Determinant of Birth Weight. Indian Pediatrics 1977;14(2):107-114.
23. Das K, Ganguly SS, Saha R, Ghosh BN.
Interrelation of birth weight with certain biological and Socio-economic factors. Indian Journal of Public Health 1981; 25 (1): 11-19. 24. Deswal BS, Singh JV, Kumar D. A study of
risk factors for low birth weight. Indian Journal Community Medicine 1999; 24 (3): 127-131.