B
EATAR
OSTKOWSKA−N
ADOLSKA1, K
ATARZYNAP
AZDRO−Z
ASTAWNY1, P
IOTRZ
IÓŁKOWSKI2,
E
LŻBIETAG
AMIAN2, M
ARZENAJ
AWORSKA1, M
AREKB
OCHNIA1, A
GNIESZKAJ
ABŁONKA1Expression of Basic Fibroblast Growth Factor
in Nasal Polyps
Ekspresja zasadowego czynnika wzrostu fibroblastów w polipach nosa
1Department of Otolaryngology, Silesian Piasts University of Medicine in Wrocław, Poland 2Department of Pathological Anatomy, Silesian Piasts University of Medicine in Wrocław, Poland
ISSN 1230−025X University of Medicine in Wrocław
Abstract
Background.The pathogenesis of nasal polyposis remains unclear. The proliferation of fibroblasts contributes to their development and growth. Basic fibroblast growth factor (bFGF) is a member of the heparin−binding growth factor family and may be involved in various pathological processes, including tissue lesion in the upper respira− tory tract.
Objectives. The aim of this study was to determine the role of bFGF in the pathogenesis of nasal polyps by com− parative analysis of its expression in neutrophilic and eosinophilic polyps, including patients with aspirin triad.
Material and Methods. The study group included 28 patients (20 males and 8 females) with nasal polyposis undergoing polypectomy. The control group consisted of 10 normal nasal mucosa specimens from patients under− going septoplasty. Twenty of the nasal polyps were histopathologically classified as eosinophilic and eight as neu− trophilic. Immunohistochemistry was used to examine the expression of bFGF in the nasal polyp tissues.
Results.bFGF immunostaining was detected both in the neutrophilic and eosinophilic polyp tissues. Particularly intense immunolabeling of bFGF was present in the nasal polyps with a high degree of neutrophil infiltration.
Conclusions.The expression of bFGF was more intense in nasal polyp tissues than in normal mucosa. The exam− ined factor was mainly localized in the vascular endothelium and inflammatory cells. Considering the stimulatory properties of bFGF on epithelial blood vessels and fibroblast proliferation, this growth factor seems to be involved in the pathogenesis of nasal polyposis (Adv Clin Exp Med 2008, 17, 1, 33–40).
Key words:nasal polyps, basic fibroblast growth factor, immunohistochemistry, aspirin triad.
Streszczenie
Wprowadzenie.Patogeneza polipów nosowych nie jest dokładnie poznana. Uznaje się, że proliferacja fibrobla− stów może przyczyniać się do ich powstawania i wzrostu. Zasadowy czynnik wzrostu fibroblastów (bFGF) nale− ży do rodziny białek wiążących heparynę. bFGF może wpływać na wiele fizjologicznych i patologicznych proce− sów biologicznych, włączając w to uszkodzenie tkanek w górnych drogach oddechowych.
Cel pracy.Określenie roli zasadowego czynnika wzrostu fibroblastów (bFGF) w patogenezie polipów nosa za po− mocą analizy porównawczej jego ekspresji w polipach neutrofilowych i eozynofilowych, a także u osób z triadą aspirynową w porównaniu z prawidłową błoną śluzową.
Materiał i metody.Materiał do badań stanowiło 28 tkanek polipów nosowych pobranych od pacjentów (20 męż− czyzn i 8 kobiet) podczas polipektomii. Grupę kontrolną stanowiło 10 wycinków prawidłowej błony śluzowej no− sa pobranych podczas zabiegu septoplastyki. Pod względem histopatologicznym 20 polipów było rozpoznawanych jako eozynofilowe, a 8 jako neutrofilowe. Badany bFGF oznaczono metodą immunohistochemiczną.
Wyniki.Zarówno w tkankach polipów neutrofilowych, jak i eozynofilowych uzyskano ekspresję bFGF. Szczegól− nie intensywny odczyn występował w polipach z przeważającym naciekiem neutrofilów. Poziom ekspresji był wyż− szy w tkankach polipów niż w prawidłowej błonie śluzowej.
Wnioski. Badany czynnik występował przede wszystkim w komórkach endotelialnych wokół naczyń krwiono− śnych, a także w komórkach nacieku zapalnego. Ze względu na swoje właściwości stymulujące proliferację ko− mórek zarówno śródbłonka naczyń, jak i fibroblastów wydaje się, że czynnik ten ma znaczenie w patogenezie poli− pów nosowych (Adv Clin Exp Med 2008, 17, 1, 33–40).
Nasal polyps, antral choanal polyps, and sinonasal polyps develop in patients with dis− turbed local homeostasis of the nasal mucosa. The etiology of nasal polyposis remains unclear. One of the main pathophysiological mechanisms lead− ing to polyp formation is a local inflammatory process accompanied by immune–system disor− ders [1]. Surgical procedures remain the most pop− ular treatment option for this pathological condi− tion and are usually effective in patients with sim− ple sinusitis with nasal polyps. However, in patients with atopic symptoms or those who are acetylsalicylic acid (ASA) sensitive it gives only temporary improvement and recurrences remain an important clinical problem in these cases. Histologically, nasal polyps consist of columnar ciliated and stratified squamous epithelium cover− ing the connective tissue with its basic structural elements, i.e. fibroblasts, infiltrated by a number of inflammatory cells, predominantly including, in most specimens, eosinophils, lymphocytes, plas− ma cells, and neutrophils.
Basic and acidic fibroblast growth factors (bFGF and aFGF, respectively) are members of the heparin−binding growth factor family. Both aFGF and bFGF have been isolated from a wide range of human and animal tissues. They promote angio− genesis and mitogenesis in various cell types, including fibroblasts and smooth muscle, epithe− lial, and endothelial cells [2]. bFGF (FGF−2) was one of the first identified members of this family of growth factors and is one of its best described. Increased expression of bFGF was detected in blood vessel endothelial cells adhering to a wide range of neoplastic cells as well as to vessels par− ticipating in inflammatory processes [3–5]. bFGF may be involved in various physiological and pathological processes, including tissue lesion in the upper respiratory tract [6, 7]. It has increased expression in nasal polyps compared with the nor− mal mucosa. It is expressed in blood vessel walls, basement membrane, basal epithelial cells, and inflammatory cells. These studies suggest that bFGF contributes to the formation of nasal polyps as well as to polyp growth through the induction of fibroblast proliferation [8, 9].
The aim of this study was to determine the role of basic fibroblast growth factor (bFGF) in the pathogenesis of nasal polyps by comparative analy− sis of its expression in neutrophilic and eosinophilic polyps, including patients with aspirin triad.
Material and Methods
The study group consisted of 28 patients (20 males and 8 females) 21–79 years of age with nasal polyposis undergoing polypectomy. The
control group consisted of 10 normal nasal mucosa specimens from patients undergoing septoplasty. Twenty of the nasal polyps were histopathologi− cally classified as eosinophilic and eight as neu− trophilic polyps. In the group with eosinophilic polyps, ten patients had multiple polypectomies and suffered from aspirin triad. Deparaffinized sections 4 µm thick were rehydrated and digested with 0.05% pronase. After blocking endogenous peroxidase activity by using a blocking reagent (DakoCytomation), the sections were rinsed twice in distilled water for 5 minutes before incubation with normal serum for 30 minutes. Then they were incubated with the primary antibody (rabbit anti–basic fibroblast growth factor (FGF–2) poly− clonal antibody, Chemicon International) diluted 1:30 for 30 minutes; this was followed by a double PBS wash for 5 minutes. The samples were incu− bated for 15 min with a biotinylated secondary anti− body and then rinsed twice in PBS for 5 minutes. Immunostaining was performed using a three−stage avidin–biotin complex (ABC) immunoperoxidase technique (LSAB+ System−HRP, Dako). The slides were washed again two times for 5 minutes in PBS. Visualization was carried out with DAB+ chromogen, after which the slides were rinsed twice in distilled water for 5 minutes. The nuclei of the cells were stained by hematoxylin. Then the samples were rinsed in running tap water for 10 minutes. Finally the slides were dehydrated and covered with glass. The intensity of staining was graded as: (+) weak, (++) moderate, (+++) strong, or (–) no staining.
Results
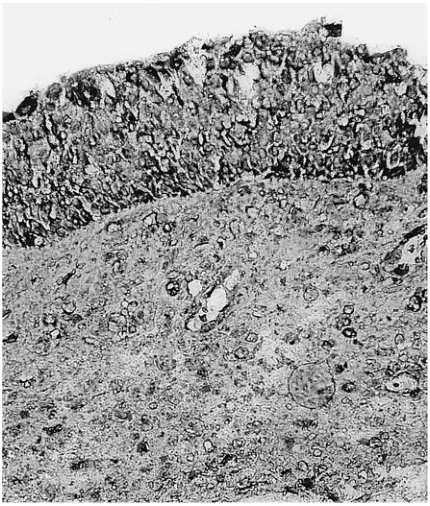
Tables 1 and 2 show the obtained results. The strongest immunostaining (+++) was observed in the epithelium, endothelium, and inflammatory cells of the neutrophilic polyps (7/8) (Fig. 1). Moderate bFGF expression (++) in all the tissue components mentioned above was shown in the eosinophilic polyps from patients with aspirin triad. Weak immunostaining was seen in the epithelium and endothelium and there was no staining in the inflammatory cells in the nasal polyps from patients without aspirin triad (Fig. 2). Weak staining was seen in the epithelium of polyps from the control slides (Fig. 3).
Discussion
was regarded mainly as a potent stimulator of angiogenesis, but further studies revealed its mul− tifunctional properties. bFGF has been described as an important neurotrophic factor whose expres− sion is regulated by neural activity [10]. In skin, bFGF may contribute to melanogenesis and to the morphogenesis of keratinocytes [11]. In the eye, bFGF is involved in the process of signal trans− duction in photoreceptors [12]. FGFs have been identified as the strongest mesoderm−inducing fac− tors [13]. Along with other growth factors, it may supply signals required for the development of mesoderm induction and maintenance and also for limb bud formation [14]. Moreover, abnormal function of bFGF and its receptor may contribute to the pathogenesis and development of some dis− eases. For example, the proliferation of neointima at the initial phase of the arteriosclerotic process is closely linked to a dysfunctional regulation of FGF−2 expression [15]. Missense mutations in the genes encoding fibroblast growth factor receptor−1 (bFGF R1), receptor−2 (bFGF R2), and receptor−3 (bFGF R3) have been associated with several craniostenosis conditions, including Pfeiffer [16], Crouzon [17], Jackson−Weiss [17] and Apert [18] syndromes, achondroplasia [19], and thanatophor− ic dwarfism [20].
Administration of bFGF may be a potential therapeutic strategy, for example in patients with ischemic cardiovascular disease or acute ischemic insult. Intracoronary and intravenous delivery of
this growth factor enhances myocardial collateral blood vessel perfusion and myocardial function in these conditions [21]. bFGF stimulates and improves the healing of duodenal ulcers and sig− nificantly accelerates wound repair in several experimental models, especially in dermatology and ophthalmology. Some of bFGF’s therapeutic applications are still in preclinical study [21, 22]. As a mitogenic factor for various cell types, including fibroblasts, and one of the most potent inducers of the formation of mesenchyme and new blood vessels, bFGF contributes to the develop− ment of chronic human transplant rejection. The expression (localization) of bFGF in nasal polyps has been described by Powers et al. [9]. Both bFGF and its receptor have been identified by immunohistochemistry in the normal mucosal epithelium of human bronchial tissue [3]. In vivo studies have demonstrated that bFGF has a mito− genic activity towards a wide variety of cell types, including epithelial cells. Local administration of this factor enhances epithelial regeneration in het− erotropic rat tracheal transplant models [23].
In the present study it was investigated whether bFGF may be involved in the growth of inflamed ostiomeatal complex tissue in the middle nasal meatus. The present results demonstrate intense immunostaining of bFGF in epithelium and inflammatory cells in the vascular endotheli− um of nasal polyps compared with the nasal mucosa. Coste et al. reported similar results. In Tissue Eosinophilic polyps Neutrophilic polyps Normal mucosa
(Rodzaj tkanki) (Polipy eozynofilowe) (Polipy neutrofilowe) (Prawidłowa błona śluzowa)
aspirin no aspirin triad triad (triada (triada obecna) nieobecna)
Epithelial cells ++ + +++ +
(Komórka nabłonka)
Endothelial cells ++ + +++ +/––
(Komórka śródbłonka)
Inflammatory cells ++ –– +++ ––
(Komórki zapalne)
Tabela 1.Obecność bFGF w różnych typach komórek w polipach nosa w porównaniu z prawidłową błoną śluzową
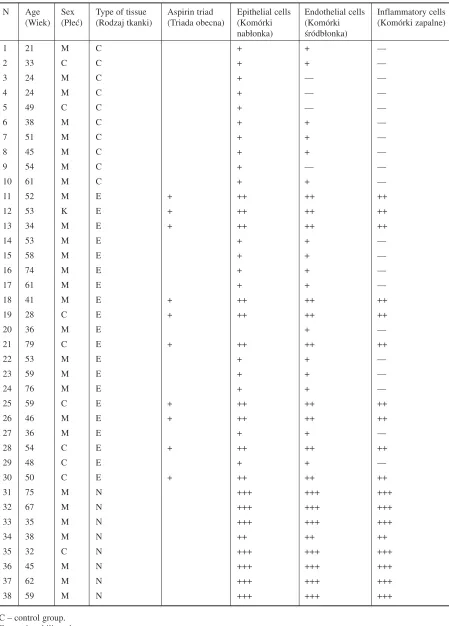
N Age Sex Type of tissue Aspirin triad Epithelial cells Endothelial cells Inflammatory cells (Wiek) (Płeć) (Rodzaj tkanki) (Triada obecna) (Komórki (Komórki (Komórki zapalne)
nabłonka) śródbłonka)
1 21 M C + + ––
2 33 C C + + ––
3 24 M C + –– ––
4 24 M C + –– ––
5 49 C C + –– ––
6 38 M C + + ––
7 51 M C + + ––
8 45 M C + + ––
9 54 M C + –– ––
10 61 M C + + ––
11 52 M E + ++ ++ ++
12 53 K E + ++ ++ ++
13 34 M E + ++ ++ ++
14 53 M E + + ––
15 58 M E + + ––
16 74 M E + + ––
17 61 M E + + ––
18 41 M E + ++ ++ ++
19 28 C E + ++ ++ ++
20 36 M E + ––
21 79 C E + ++ ++ ++
22 53 M E + + ––
23 59 M E + + ––
24 76 M E + + ––
25 59 C E + ++ ++ ++
26 46 M E + ++ ++ ++
27 36 M E + + ––
28 54 C E + ++ ++ ++
29 48 C E + + ––
30 50 C E + ++ ++ ++
31 75 M N +++ +++ +++
32 67 M N +++ +++ +++
33 35 M N +++ +++ +++
34 38 M N ++ ++ ++
35 32 C N +++ +++ +++
36 45 M N +++ +++ +++
37 62 M N +++ +++ +++
38 59 M N +++ +++ +++
Table 2.The presence of bFGF in various tissue components from nasal polyps and from normal mucosa
Tabela 2. Obecność bFGF w różnych typach komórek w tkankach polipów nosa oraz prawidłowej błony śluzowej
their study, immunohistochemistry was used to evaluate the expressions of bFGF and PCNA (pro− liferating cell nuclear antigen) in nasal polyps [24]. Increased cell proliferation in the epithelium of nasal polyps compared with the inferior turbinate mucosal epithelium was detected. Coste states that the intense immunostaining of bFGF along the basal and suprabasal epithelial cells sug−
gests that bFGF may contribute to the proliferation of epithelial cells and thus to the formation of nasal polyposis. Norlander et al. analyzed the amount of bFGF in nasal polyp tissues and inferi− or turbinate mucosal tissues obtained from 17 patients using ELISA and immunohistochemistry. Significantly higher levels of this growth factor were identified in nasal polyps than in the turbinate mucosa. According to the authors, con− tinuous chronic inflammation of damaged polyp mucosal epithelium induces the increased produc− tion and secretion of bFGF by macrophages. This, in combination with other mediators, may induce the process of neovascularization and reproduction of epithelial cells [8].
Kowalski et al. demonstrated a significant dif− ference in the metabolism of arachidonic acid in nasal polyp epithelial cells cultured from patients with aspirin triad compared with patients without aspirin triad. The study showed a decrease in PGE2 production in nasal polyps from aspirin−sen− sitive patients and a different response to incuba− tion with aspirin, as there was an increase in pro− duction and 15−HETE release compared with aspirin−tolerant patients. These results may sug− gest that nasal polyp epithelial cells from aspirin− sensitive and aspirin−tolerant patients may gener− ate differential mechanisms of responses to aspirin or develop another pathomechanism of the chron− ic inflammatory process [25]. In the present study, expression of bFGF in the nasal polyps from patients with aspirin triad was stronger than in polyps from the patients without aspirin triad. As significant differences were not detected in immunostaining intensity, further research is need− ed. When analyzing nasal polyps obtained from patients with and without aspirin triad, one cannot
Fig. 1. Strong (+++) staining of bFGF in epithelial, endothelial, and inflammatory cells of neutrophilic polyps, magnification is ×200
Ryc. 1.Silny odczyn (+++) bFGF w komórkach nabłonkowych, śródbłonkowych i zapalnych w poli− pach neutrofilowych, powiększenie 200×
Fig. 2. Moderate (++) immunolabeling of bFGF in epithelial, endothelial, and inflammatory cells of eosinophilic polyps from patients with aspirin triad, magnification is ×200
Ryc. 2.Pośredni odczyn bFGF w komórkach
nabłonkowych, śródbłonkowych i zapalnych w polipach eozynofilowych, powiększenie 200×
Fig. 3.Weak (+) bFGF expression in epithelial and endothelial cells of normal mucosa, magnification is ×400
forget the aspect of polyposis recurrence. In the present study, polyps from patients with aspirin triad demonstrated rapid tissue growth, most of these patients having undergone multiple polypec− tomies. The nasal polyps obtained from the aspi− rin−insensitive patients were primary.
Caye−Thomasen showed that the level of immunohistochemical expression of bFGF in non− −recurrent compared with recurrent nasal polyps was similar. This suggests, according to the authors, that bFGF cannot be recognized as a prog− nostic factor for recurrent polyposis [26]. Li demonstrated stronger immunostaining of bFGF in large (grade III) polyps than in small ones (grades I and II). bFGF was located mainly in the inflam− matory and epithelial cells around the basilar mem− brane and inflammatory and endothelial cells around the vessel [27]. The stronger immunostain− ing of bFGF in neutrophilic than eosinophilic nasal polyps detected in the present study may be a result of an interaction of bFGF and neutrophils. Takagi et al. examined the effect of bFGF on human neu− trophil functions in vitrousing flow cytometry and monoclonal antibodies. In their study, an increase in the expression of the leukocytic integrin CD11 and a decrease in the expression of L−selectin on neutrophils was demonstrated. According to the authors, the results suggest that bFGF participates in the inflammatory process by modulating the sur− face expression of the effector cell molecules and stimulating respiratory burst activity in neutrophils [28]. Totani et al. reported increased expression of bFGF in endothelial cell cultures after incubation with human blood neutrophils [29]. Zhang showed that simulation of human umbilical vein endothe−
lial cells by bFGF increases neutrophil adhesion to endothelial cells [30]. Besides bFGF, other stimu− lators of neutrophil adhesion are known. According to Tokushige, enhanced expression of ICAM−1 (intercellular adhesion molecule−1) and E−selectin on endothelial cells after stimulation with IL−1b leads to increased adhesion of neutrophils [31]. Shimomura confirmed this in his studies by finding a correlation between ICAM−1 expression in mucosal microvascular endothelial cells and infil− tration of neutrophils [32]. Also, in Itoh’s experi− ment, IL−1b induced the adhesion of neutrophils in human nasal microvascular endothelial cell cul− tures [33]. Yamamoto investigated the role of the proinflammatory cytokines IL−1β and TNF−α in human nasal endothelial cell cultures. In his stud− ies, increased expressions of VCAM−1, E−selectin, and ICAM−1 after stimulation with IL−1b and TNF−α were found [34]. These findings indicate that the adhesion of neutrophils is the result of var− ious stimulating mechanisms, including bFGF stimulation.
The authors conclude that the results of the present study indicate a stronger expression of bFGF in nasal polyps than in normal nasal mucosa. Particularly intense immunostaining for bFGF was present in nasal polyps with neutrophil infiltration. Considering the stimulatory properties of bFGF on epithelial blood vessels and fibroblast proliferation, this growth factor seems to be involved in the pathogenesis of nasal polyposis, but its biological role is undoubtedly supported by other growth fac− tors or protein modulators. Further studies are required to determine the precise role of bFGF in the pathogenesis of nasal polyposis.
References
[1] Pawankar R:Nasal polyps: an update: editorial review. Curr Opin Allergy Clin Immunol 2003, 3, 1–6.
[2] Bikfalvi A, Klein S, Pintucci G, Rifkin DB:Biological roles of fibroblast growth factor−2. Endocr Rev 1997, 18, 26–45.
[3] Hughes SE, Hall PA:Immunolocalization of fibroblast growth factor receptor 1 and its ligands in human tissues. Lab Invest 1993, 69, 173–182.
[4] Kanazawa S, Tsunoda T, Onuma E, Majima T, Kagiyama M, Kikuchi K:VEGF, basic−FGF, and TGF−beta in Crohn’s disease and ulcerative colitis: a novel mechanism of chronic intestinal inflammation. J Gastroenterol 2001, 96, 822–828.
[5] Gravdal K, Halvorsen OJ, Haukaas SA, Akslen LA:Expression of bFGF/FGFR−1 and vascular proliferation related to clinicopathologic features and tumor progress in localized prostate cancer. Virchows Arch 2005, 12, 1–7
[6] Jawerzat S, Auguste P, Bikfalvi A:The role of fibroblast growth factors in vascular development. Trends Mol Med 2002, 8, 483–489.
[7] Han R, Liu J, Tanswell AK, Post M:Expression of basic fibroblast growth factor and receptor: immunolocal− ization studies in developing rat fetal lung. Pediatr Res 1992, 31, 435–440.
[8] Norlander T, Westermark A, van Setten G, Valtonen H, Ishizaki H, Pyykko I:Basic fibroblast growth factor in nasal polyps immunohistochemical and quantitative findings. Rhinology 2001, 39, 88–92.
[9] Powers MR, Qu Z, LaGesse PC, Liebler JM, Wall MA, Rosenbaum JT:Expression of basic fibroblast growth factor in nasal polyps. Ann Otol Rhinol Laryngol 1998, 107, 891–897.
expression in keratinocytes of burn scars. Eur Cytokine Netw 2000, 11, 233–239.
[12] Hicks D, Courtois Y:Fibroblast growth factor stimulates photoreceptor differentiation in vitro. J Neurosci 1992, 12, 2022–2033.
[13] Neubauer M, Fischbach C, Bauer−Kreisel P, Lieb E, Hacker M, Tessmar J, Schulz MB, Goepferich A, Blunk T:Basic fibroblast growth factor enhances PPARgamma ligand−induced adipogenesis of mesenchymal stem cells. FEBS Lett 2004, 577, 277–283.
[14] Harduf H, Halperin E, Reshef R, Ron D:Sef is synexpressed with FGFs during chick embryogenesis and its expression is differentially regulated by FGFs in the developing limb. Dev Dyn. 2005, 233, 301–312.
[15] Ito A, Shimokava H, Fukumoto Y, Kadokami T, Nakaike R, Takayanagi T, Egashira K, Sueishi K, Takeshita A:The role of fibroblast growth factor−2 in the vascular effects of interleukin–1 beta in porcine coro− nary arteries in vivo. Cardiovasc Res 1996, 32, 570–579.
[16] Lajeunie E, Ma HW, Bonaventure J, Munnich A, Le Merrer M:FGFR2 mutations in Pfeiffer Syndrome. Nat Gen 1995, 9, 108–112.
[17] Jabs EW, Li X, Scott AF, Meyers G, Chen W, Eccles M, Mao JI, Charnas LR, Jackson CE, Jaze M:Jackson Weiss and Crouzon syndromes are allelic with mutations in fibroblast growth factor receptor 2. Nat Genet 1994, 8, 275–172.
[18] Wilkie AO, Slaney SF, Oldridge M, Poole MD, Ashworth GJ, Hockley AD, Hayward RD, David DJ, Pulleyn IJ, Rutland P:Apert syndrome results from localized mutations of FGFR2 and is allelic with Crouzon syndrome. Nat Genet 1995, 9, 165–172.
[19] Rousseau F, Bonaventure J, Legal Mallet L, Pelet A, Royet JM, Maroteaux P, Le Merrer M, Munich A:
Mutation in the gene encoding fibroblast growth factor receptor 3 in achondroplasia. Nature 1994, 371, 252–325.
[20] Rousseau F, Saugier P, Le Merrer M, Delezoide AL, Maroteaux P, Bonaventure J:Stop codon FGFR3 muta− tions in thanatophoric dwarfism type 1. Nat Genet 1995, 10, 11–12.
[21] Laham RJ, Garcia L, Baim DS, Post M, Simons M:Therapeutic angiogenesis using basic fibroblast growth fac− tor and vascular endothelial growth factor using various delivery strategies. Curr Interv Cardiol Rep 1999, 1, 228–233.
[22] Ma Y, Zhao H, Zhou X:Topical treatment with growth factors for tympanic membrane perforations: progress towards clinical application. Acta Otolaryngol 2002, 122, 586–599.
[23] Mayer E, Cardoso PF, Puskas JD, De Campos K, Oka T, Dardick I, Patterson GA:The effect of basic fibrob− last growth factor and omentopexy on revascularization and epithelial regeneration of heterotopic rat tracheal iso− grafts. J Thorac Cardiovasc Surg 1992, 104, 180–188.
[24] Coste A, Rateau J−G, Roudot−Thoraval F, Chapelin C, Gilain L, Poron F, Peynegre R, Bernaudin J−F, Escudier E:Increased epithelial cell proliferation in nasal polyps. Arch Otolaryng Head Neck Surg 1996, 122, 432–436.
[25] Kowalski LM, Pawliczak R, Woźniak J, Siuda K, Poniatowska M, Iwaszkiewicz J, Kornatowski T, Kaliner MA:
Differential metabolism of arachidonic acid in nasal polyp epithelial cells cultured from aspirin−sensitive and aspirin−tolerant patients. Am J Respir Crit Care Med 2000, 161, 391–398.
[26] Caye−Thomasen P, Larsen K, Tingsgaard P, Tos M:Basic fibroblast growth factor expression in recurrent ver− sus non−recurrent nasal polyposis. Eur Arch Otorhinolaryngol 2004, 261, 321–325.
[27] Li H, Xu G, Li Y, Xie M, Xu R:Expressions of vascular endothelial growth factor and basic fibroblast growth factor in nasal polyp and its role. Zhonghua Er Bi Yan Hou Ke Za Zhi 2001, 36, 87–89.
[28] Takagi S, Takahashi K, Katsura Y, Matsuoka T, Ohsaka A:Basic fibroblast growth factor modulates the sur− face expression of effector cell molecules and primes respiratory burst activity in human neutrophils. Acta Heamatol 2000, 103, 78–83.
[29] Totani L, Piccoli A, Pellegrini GG, Di Santo A, Lorenzet R:Polymorphonuclear leukocytes enhance release of growth factors by cultured endothelial cells. Arterioscler Thromb 1994, 14, 125–132.
[30] Zhang H, Issekutz AC:Growth regulation of neutrophil−endothelial cell interactions. J Leukoc Biol 2001, 70, 225–232.
[31] Tokushige E, Itoh K, Ushikai M, Katahisa S, Fukuda K:Localization of IL−1B mRNA and cell adhesion mol− ecules in the maxillary sinus mucosa of patients with chronic sinusitis. Laryngoscope 1994, 104, 1245–1250.
[32] Shimomura A, Ikeda K, Suzuki H, Nakabayashi S, Oshima T, Furukawa M, Takasaka T, Ando N, Ohtani H, Nagura H: The expression of adhesion molecules in nonalllergic chronic sinusitis. Laryngoscope 1997, 107, 1519–1524.
[33] Itoh K, Katahira S, Matsuzaki T, Ohyama M, Fukuda K:Retention fluids of chronic sinusitis induce neu− trophil adherence to microvascular endothelial cells. Acta Otolaryngol (Stockh) 1992, 112, 882–889.
[34] Yamamoto Y, Ikeda K, Watanabe M, Shimomura A, Suzuki H, Oshima T, Imamura Y, Ohuchi K, Takasaka T:
Address for correspondence:
Beata Rostkowska−Nadolska Department of Otolaryngology Silesian Piasts University of Medicine Chałubińskiego 2
50–368 Wrocław Poland
Tel.: +48 607 301 229 E−mail: [email protected]
Conflict of interest: None declared