Dominika Klimkiewicz-Blok
1, Jerzy Florjański
1, Jerzy Zalewski
2, Radosław Blok
3Analysis of the Concentrations of Interleukin 15
in Amniotic Fluid in the Second
and the Third Trimesters of Pregnancy*
Analiza stężeń interleukiny 15 w płynie owodniowym
w II i III trymestrze ciąży
1 2nd Department of Gynecology, Obstetrics and Neonatology, Wroclaw Medical University, Poland
2 Department of Gynecology and Obstetrics, Division of Public Health, Wroclaw Medical University, Poland 3 1st Department of Gynecology and Obstetrics, Wroclaw Medical University, Poland
Abstract
Background. Cytokines play an essential role in the regulation of immunological responses. Interleukin 15 (IL-15) is a glycoprotein secreted primarily by macrophages and monocytes. IL-15 plays a key role in the immunological response of the cellular type.
Objectives. The objective of this study was to evaluate changes in the concentration of interleukin 15 in amniotic fluid in the second and the third trimesters of a normal pregnancy.
Material and Methods. The study included 74 pregnant women who were subjected to a diagnostic amniocentesis in order to extract amniotic fluid samples. The patients were divided into two groups: group I – 45 pregnant women in the 2nd trimester, subjected to genetic amniocentesis during the 15th through 19th weeks. The results of the cytogenetic
tests were found to be normal in all the fetuses. Group II: 29 pregnant women in their 3rd trimester, were subjected
to amniocentesis in order to determine the biological maturity of the fetuses. The concentration of IL-15 was marked with the ELISA method using a kit made by the R&D company. Method sensitivity was > 2 pg/ml.
Results. The average concentration of IL-15 in the amniotic fluid of 2nd trimester pregnancies was 6.54 pg/
ml, whereas in the 3rd trimester it rose to 18.62 pg/ml. Discrepancies were found to be statistically significant
(p < 0.05).
Conclusions. The presence of IL-15 in the amniotic fluid in the second trimester of gestation indicates an early activation of the fetus’s defensive mechanisms. An average concentration of IL-15 in the amniotic fluid is signifi-cantly higher in the third trimester of pregnancy than in the second trimester, which can mean about the develop-ment of the immune response in the fetus (Adv Clin Exp Med 2012, 21, 1, 75–79).
Key words: interleukin 15, amniotic fluid.
Streszczenie
Wprowadzenie. Interleukiny odgrywają istotną rolę w regulacji odpowiedzi immunologicznej organizmu. Interleukina 15 (IL-15) jest glikoproteiną wydzielaną głównie przez makrofagi i monocyty. IL-15 odgrywa kluczo-wą rolę w odpowiedzi immunologicznej typu komórkowego.
Cel pracy. Ocena zmian w stężeniu IL-15 w płynie owodniowym w II i III trymestrze ciąż o przebiegu prawi-dłowym.
Materiał i metody. Badaniami objęto 74 ciężarne, u których wykonano amniopunkcje diagnostyczne, pobierając płyn owodniowy. Badane podzielono na dwie grupy: Grupa I – 45 ciężarnych w II trymestrze ciąży, poddane amniopunkcji genetycznej między 15. a 19. tygodniem. U wszystkich płodów wynik badania cytogenetycznego był prawidłowy.Grupa II – 29 ciężarnych w III trymestrze ciąży, u których amniopunkcję wykonano w celu oceny dojrzałości biologicznej płodów. Stężenia IL-15 oznaczano metodą immunoenzymatyczną, zestawem firmy R&D. Czułość metody wynosiła > 2 pg/ml.
Adv Clin Exp Med 2012, 21, 1, 75–79 ISSN 1899-5276
ORIGINAL PAPERS
© Copyright by Wroclaw Medical University
Cytokines play an essential role in the regu-lation of immunological responses. They interact within a complex network of connections within which the production of one particular cytokine influences the secretion of another cytokine [1].
Interleukin 15 (IL-15) is a glycoprotein secret-ed primarily by macrophages and monocytes. The gene that codes IL-15 has its locus in the
chromo-some 4q31 [2]. As far as molecular structure and
biological characteristics are concerned, IL-15 is similar to IL-2 [2–6]. IL-15 plays an important role in the immunological response of the cellu-lar type. IL-15 acts as a stimulator for prolifera-tion and activity of the T lymphocyte and the NK (Natural Killer) cells. In tandem with IL-2, IL-15 stimulates the secretion of other cytokines: in-terferon (IFN)-gamma and TNF (tumor necrosis factor) by NK cells [2, 4, 5, 7-9]. IL-15 also plays a key role outside the immunological system – it is a stimulating factor in the angiogenesis process as well as a strong apoptosis inhibitor [10, 11]. It has been shown that the concentration of IL-15 and mRNA IL-15 in the placental tissue in pregnancies complicated by high blood pressure is significant-ly lower in comparison with pregnancies that are physiologically normal, which confirms the role of IL-15 in the process of human placenta invasion as a factor facilitating the process of angiogenesis [10]. IL-15 is present in the amniotic fluid begin-ning with the third trimester of gestation [12].
IL-15 and mRNA IL-15 has also been proven to be found in fetal membrane – the amniotic, am-niochorial and deciduous membranes, as well as in the placenta [3, 9, 12–14]. Expression of IL-15 and its mRNA in the endometrium during the secre-tory phase as well as in the deciduous membrane points to the role of this cytokine in a regular monthly cycle as well as in gestation development during the phase of blastocyst implantation as well as the early phase of trophoblast invasion by way of stimulation of the proliferation of deciduous NK cells [7, 8, 15, 16]. IL-15 synthesis in the endo-metrium and decidua are hormonally controlled – primarily by progesterone [7, 8, 16].
The objective of this study was to evaluate the fetus’s defense mechanisms on the basis of an analysis of the concentration of interleukin IL-15 in the amniotic fluids in the second and third tri-mesters of normal gestation.
Material and Methods
The clinical material consisted of 74 samples of amniotic fluid taken by way of amniocentesis from pregnant women being treated at the Clinic for Fetal Development Disorders of the Medical University Wrocław during 2004–2006. The study had the approval of the Bioethical Committee of the Medical University of Wroclaw.
The gathered material was divided into two groups:
Group I – 45 pregnant women in their second trimester who had qualified for genetic amniocen-tesis due to: their age (over 35 years old), an in-creased risk of fetal defects as shown in double or triple testing, an abnormal ultrasonogram exami-nation of the nuchal translucency and/or a high-risk genetic medical history.
The age of the pregnant women was between 24 and 46 years of age (with an average of 38.5 years old). Genetic amniocentesis was carried out
in the second trimester between the 15th and 19th
weeks. The amniotic fluids were sent to the Ge-netic Laboratory of the Wroclaw Medical Univer-sity in order to determine the karyotype of the fetuses under examination. There were no abnor-malities found in the results of the fetal cytoge-netic tests.
Group II – 29 pregnant women in their third
trimesters (between the 36th and 40th weeks) who
had qualified for diagnostic amniocentesis in or-der to evaluate the biological maturity of the fe-tus. The age of the pregnant women was between 22 and 38 years old (with an average of 28.5).
The amniotic fluid samples were centrifuged at a speed of 3,000 spins per minute for 10 min-utes, and then were refrigerated at a temperature
of –82o Celsius until such time as measurement
were made. The concentration of IL-15 was marked with the ELISA method using a kit made by the R&D company. Method sensitivity was > 2 pg/ml.
Absorbance value was read at a wavelength of 450 nm.
Based on the Shapiro-Wilk test thwew is no reason to reject the hypothesis of normal schedule. The calculations were performed by using system STATISTICA 8.0, StatSoft, Inc. 2007. IL-15 con-centration in the study groups were compared
Wyniki. Średnie stężenie IL-15 w płynie owodniowym w II trymestrze ciąży wyniosło 6,54 pg/ml, a w III trymestrze wzrastało do 18,62 pg/ml. Różnice okazały się znamienne statystycznie (p < 0,05).
Wnioski. Obecność IL-15 w płynie owodniowym w II trymestrze ciąży wskazuje na wczesne uruchomienie mecha-nizmów ochronnych przez płód. Średnie stężenie IL-15 w płynie owodniowym jest znacząco większe w III tryme-strze ciąży niż w II trymetryme-strze, co może świadczyć o rozwoju mechanizmów immunologicznych u płodu (Adv Clin Exp Med 2012, 21, 1, 75–79).
with each other using the Student t-test. The value p < 0.05 was assumed as statistically significant.
Results
Comparison of IL-15 concentration levels in amniotic fluids of groups I and II, i.e., in the sec-ond and third trimesters of gestation, are present-ed in Table 1.
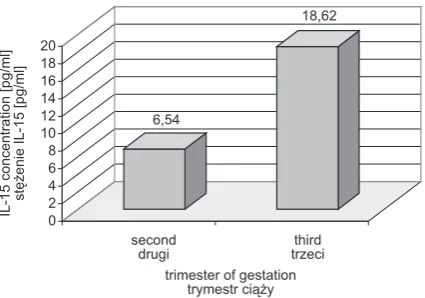
The average level of IL-15 concentration in the amniotic fluid in second trimester gestation was 6.54 pg/ml, whereas in the third trimester it was 18.62 pg/ml. These differences were found to be statistically significant (p < 0.05) – Fig. 1.
Discussion
The presence of cytokine and changes in their concentration in amniotic fluids (IL-1alfa, IL-1beta, IL-4, IL-6, IL-8, TNF – tumor necrosis factor) were analyzed primarily in light of their role in the development of intrauterine infection, risk of preterm birth, or preterm rupture of fetal membranes [17–23]. In accordance with the data presented in the literature, the concentration of proinflammatic cytokines (IL-1alfa, IL-1beta, IL-6, Il-8, IL-16, TNF) as well as IL-4 and IL-10 in the amniotic fluid are significantly higher in pregnan-cies affected by chorioamnionitis and are associ-ated with an increased risk of preterm contraction activity [17–24].
Studies by Witczak et al. [23] showed that there is no correlation between levels of interleu-kin concentration (IL-1, IL-6, IL-8) in the amniot-ic fluid and that in the serum of pregnant women with complications of premature rupture of mem-branes. The authors suggest that there is a barrier that makes it impossible for cytokine to transfer through the placenta, meaning that there are two
environments, that of the mother and that of the fetus, that function independently of each other and in which interleukin is secreted through the cells of the immunological system.
The development of the fetal immunological system begins at a very early stage of gestation – at
about the 7th week. During this period,
multi-po-tential cells develop into precursory cells for each of the specific lines of the immunological system. During its intrauterine development period, the undeveloped fetus is capable of immunological responses and of activating its own mechanisms of humoral and cellular defense, but the immuno-logical response of the fetus and the newborn is not fully developed and therefore not fully effec-tive [25].
Publication regarding interleukin 15 (IL-15) concentration in the amniotic fluid are few and are not unanimous [3, 12, 13]. The values of IL-15 concentration in the amniotic fluid in gestation development that the current study showed differ
Table 1. IL-15 concentration in the amniotic fluid for specific groups
Tabela 1. Stężenie IL-15 w płynie owodniowym w badanych grupach
IL-15
Concentration (Stężenie IL-15) (pg/ml)
Minimum value
(Wartość minimalna) Maximum value (Wartość maksymalna) Median (Mediana) SD
Group I (Grupa I) (n = 45)
2.31 15.87 5.73 3.24
Group II (Grupa II) (n = 29)
2.59 42.45 18.07 10.33
p < 0.05. p < 0,05.
6,54
18,62
0 2 4 6 8 10 12 14 16 18 20
IL-15 concentration [pg/ml
]
stężenie IL-15 [pg/ml
]
second
drugi trzecithird trimester of gestation
trymestr ciąży
Ryc. 1. Porównanie średnich wartości stężeń IL-15 w płynie owodniowym w grupie I (drugi trymestr) i grupie II (trzeci trymestr)
from those found by the authors of other studies, though the current authors feel that it must be em-phasized that the literature has very little to say on this subject.
The current study results confirm those re-ported by Fortunato et al. [12], namely, that IL-15 is present in the amniotic fluid from the be-ginning of the second trimester of gestation. Ac-cording to Fortunato et al. the concentration of IL-15 in the amniotic fluid is highest during the second trimester of gestation (115 pg/ml), and in at term pregnancies (third trimester), one can ob-serve a significant drop in the level of concentra-tion to 61 pg/ml. The current study showed that the IL-15 concentration in the amniotic fluid was decidedly lower compared with the results given by Fortunato et al. and were 6.54 and 18.62 pg/ml in the second and third trimesters, respectively. Furthermore, the current study found that there was a significant increase in IL-15 concentration in the amniotic fluid as gestation progressed, a fact that was not observed by Fortunato et al.
In addition Fortunato et al. indicated that in the case of regular uterine contractions at term as well as in the case of pregnancies with a higher risk of preterm birth the concentration of IL-15 in the amniotic fluid could reach a value as high as 179–224 pg/ml.
A study by Heikkinen et al. [13] observed IL-15 concentration levels in the amniotic fluid in the second trimester of gestation at an average value of 47 pg/ml which was completely at odds with
those indicated by Fortunato et al. [12] (2.4 times lower) as well as with the current study (almost 8 times higher). Heikkinen et al. did not observe any significant differences in the level of IL-15 in am-niotic fluid over the course of gestation (median – 42 pg/ml), which also differs from observations by both Fortunato and the current study.
Searle et al. [26] reported that while one may observe the presence of IL-15 (average concentra-tion – 41 pg/ml) in the amniotic fluid in the sec-ond trimester, it does not show full biological ac-tivity, and enhancement of cytotoxic lymphoblasts to proliferation takes place solely by way of a beta-chain being a fragment of IL-15.
On the basis of the literature cited here and their own study, the authors can state that IL-15 is present in the amniotic fluid at the beginning of the second trimester of gestation, though the value of concentration in the second and third trimesters provided by different authors does dif-fer significantly. Neither do the relevant studies concur as regards changes in the level of IL-15 in the amniotic fluid over the course of the gestation period.
The authors concluded that the presence of IL-15 in the amniotic fluid in the second trimes-ter of gestation indicates an early activation of the fetus’s defensive mechanisms. An average concen-tration of IL-15 in the amniotic fluid is significantly higher in the third trimester of pregnancy than the second trimester, which can indicate the develop-ment of the immune response in the fetus.
References
[1] Hopkins SJ: The pathophysiological role of cytokines. Legal Med2003, 5, 45–57.
[2] Carson WE, Giri JG, Lindemann MJ, Linett ML, Ahdieh M, Paxton R, Anderson D, Eisenmann J, Grabstein K, Caligiuri MA: Interleukin 15 is novel cytokine that activates human natural killer cells via components of the IL-2 receptor. J Exp Med 1994, 180, 1395–1403.
[3] Agarwal R, Loganath A, Roy AC, Wong YC, Ng SC: Expression profiles of interleukin 15 in early and late gesta-tional human placenta and in pre-eclamptic placenta. Mol Hum Reprod 2001, 7, 97–101.
[4] Choi SS, Chhabra VS, Nguyen QH, Ank BJ, Stiehm ER, Roberts RL: Interleukin-15 enhances cytotoxicity, recep-tor expression and expansion of neonatal natural killer cells in long-term culture. Clin Diag Lab Immunol 2004, 9, 879–888.
[5] Kennedy MK, Park LS: Characterization of interleukin-15 /IL-15/ and the receptor complex. J Clin Immunol 1996, 16, 134–143.
[6] Lin SJ, Chao HCh, Kuo ML: The effect of interleukin 12 and interleukin 15 on CD69 expression of T-lymphocytes and natural killer cells from umbilical cord blood. Biol Neonate 2000, 78, 181–185.
[7] Kitaya K, Yasuda J, Yagi I, Tada Y, Fushiki S, Honjo H: IL-15 expression at human endometrium and deciduas. Biol Reprod 2000, 63, 683–687.
[8] Verma S, Hiby SE, Loke YW, King A: Human decidual natural killer cells express the receptor for and respond to the cytokine Interleukin-15. Biol Reprod 2000, 62, 959–968.
[9] Waldmann TA, Tagaya Y: The multifaceted regulation of interleukin 15 expression and the role of this cytokine in NK cell differentiation and host response to intracellular pathogens. Annual Rev Immunol 1999, 17, 19–49.
[10] Angiolillo AL, Kanegane H, Sgadari C, Reaman GH, Todsato G: Interleukin-15 promotes angiogenesis in vivo. Biochem Biophys Res Commun 1997, 7, 231–237.
[11] Bulfone-Paus S, Ungureanu D, Pohl T, Lindner G, Paus R, Ruckert R, Krause H, Kunzendorf U: Interleukin-15 protects from lethal apoptosis in vivo. Nat Med 1997, 10, 1124–1128.
[13] Heikkinen J, Mottonen M, Pulkki K, Lassila O, Alanen A: Cytokine levels in midtrimester amniotic fluid in normal pregnancy in the prediction of pre-eclampsia. Scand J Immunol 2001, 53, 310–314.
[14] Amash A, Huleihel M, Eyal S, Maor E, Myatt L, Holcberg G: The expression of interleukin-15 and interleukin 18 by human term placenta is not affected by lipopolysaccharide. Eur Cytokine Netw 2007, 18(4), 188–194.
[15] Chegini N, Ma C, Roberts M, Williams RS, Ripps BA: Differential expression of interleukins /IL/ IL-13 and IL-15 throughout the menstrual cycle in endometrium of normal fertile women and women with recurrent spontaneous abortion. J Reprod Immunol 2002, 56, 93–110.
[16] Okada S, Okada H, Sanezumi M, Nakajima T, Yasuda K, Kanzaki H: Expression of interleukin-15 in human endometrium and deciduas. Mol Hum Reprod 2000, 1, 75–80.
[17] Athayde N, Romero S, Maymon E, Gomez R, Pacora P, Yoon BH, Edwin SS: Interleukin-16 in pregnancy, par-turition, rupture of fetal membranes, and microbial invasion of the amniotic cavity. Am J Obstet Gynecol 2000, 182, 135–141.
[18] Figueroa R, Garry D, Elimian A, Patel K, Sehgal PB, Tejani N: Evaluation of amniotic fluid cytokines in preterm labor and intact membranes. J Matern Fetal Neonat Med 2005, 18, 241–247.
[19] Jacobsson B, Mattsby-Baltzer I, Andersch B et al.: Microbial invasion and cytokine response in amniotic fluid in a Swedish population of women in preterm labor. Acta Obstet Gynecol Scand 2003, 82, 120–128.
[20] Jacobsson B, Mattsby-Baltzer I, Andersch B, Bokstrom H, Holst RM, Wennerholm UB, Hagberg H: Microbial invasion and cytokine response in amniotic fluid in a Swedish population of women in preterm prelabor rupture membranes. Acta Obstet Gynecol Scand 2003, 82, 423–431.
[21] Jacobsson B, Mattsby-Baltzer I, Hagberg H: Interleukin-6 and interleukin-8 in cervical and amniotic fluid: rela-tionship to microbial invasion of the chorioamniotic membranes. BJOG 2005, 112, 719–724.
[22] Romero R, Mazor M., Brandt F, Sepulveda W, Avila C, Cotton DB, Dinarello CA: Interleukin-1 alpha and interleukin-1beta in preterm and term human parturition. Am J Reprod Immunol 1992, 27, 117–123.
[23] Witczak M, Torbe A, Czajka R: Maternal serum and amniotic fluid IL-1alpha, IL-1beta, IL-6 and IL-8 in preterm and term labor complicated by PROM. Gin Pol 2003, 74, 1343–1347.
[24] Saito S, Kasahara T, Kato Y, Ishihara Y, Ischijo M: Elevation of amniotic fluid interleukin 6 /IL-6/, IL-8 and granulocyte colony stimulating factor / G-CSF/ in term and preterm parturition. Cytokine 1993, 5, 81–88.
[25] Zygmunt M, Hahn D, Kiesenbauer N, Munstedt K, Lang U: Invasion of cytotrophoblastic /JEG-3/ cell is up-regulated by interleukin-15 in vitro. Am J Reprod Immunol 1998, 40, 326–331.
[26] Searle RF, Bromage SJ, Palmer J et al.: Human amniotic fluid lacks interleukin-2 and interleukin-15 but can interact with the beta-chain of the of the interleukin-2 receptor. Immunology 2000, 99, 411–417.
Address for correspondence:
Dominika Klimkiewicz-Blok
2nd Department of Gynecology, Obstetrics and Neonatology
Wroclaw Medical University Borowska 213
50-556 Wrocław Poland
Tel.: +48 71 733 14 00 Mobile: +48 600 010 055 E-mail: [email protected]
Conflict of interest: None declared