Copyrightq1997, American Society for Microbiology
Hepatitis C Virus Replicative Levels and Efficiency of
Genotyping by Specific PCR and Antibody Assay
NOBUKAZU YUKI, NORIO HAYASHI,* EIJI MITA, HIDEKI HAGIWARA, KAZUYOSHI OHKAWA, KAZUHIRO KATAYAMA, YUTAKA SASAKI, AKINORI KASAHARA, HIDEYUKI FUSAMOTO,
ANDTAKENOBU KAMADA
First Department of Medicine, Osaka University Medical School, Suita 565, Japan
Received 12 June 1996/Returned for modification 29 August 1996/Accepted 10 February 1997
We studied factors which influence the detection of hepatitis C virus genotypes by the group-specific PCR of the sequence within the core region gene and by the newly developed genotype-specific NS4 antibody assay. Genotyping was performed on 75 hepatitis C virus carriers in Japan, where patients with hepatitis C viremia are exclusively infected with genotypes 1b, 2a, and 2b. PCR failed to identify genotypes in 8 (11%) patients, whereas 12 (16%) patients, including the 8 patients mentioned above, could not be genotyped by the serological assay. Serological genotypes showed almost complete agreement with those found by the PCR except that double infection was revealed in only two of the eight patients serologically judged to be coinfected with genotypes 1 and 2. In each assay, disease activity and levels of viremia assessed by a competitive reverse transcription PCR assay were significantly lower in patients infected with untypeable isolates than in those infected with typeable ones (P < 0.01). The PCR could identify the genotypes of isolates from all 64 patients with levels of viremia of>106copies/ml, and the genotype-specific antibody responses were found in 60 (94%)
patients. In contrast, isolates from only 3 (27%) of 11 patients with low levels of viremia (<106copies/ml) could
be genotyped by the PCR (P < 0.00001), and these patients showed the genotype-specific antibody responses (P < 0.00001). These findings suggest that low levels of hepatitis C virus replication may reduce the efficiency of genotyping by serological assay as well as by PCR.
Hepatitis C virus (HCV) is a single-stranded RNA virus whose genomic structure resembles that of the flaviviruses (2). The viral genome has one large open reading frame, with three
regions that appear to encode structural proteins at the 59end
(the core, E1, and E2/NS1 regions); these are followed by four
regions that probably encode nonstructural proteins at the 39
end (the NS2, NS3, NS4, and NS5 regions). Since the cloning of the HCV genome, markedly divergent sequences have been found among distinct isolates, suggesting the existence of HCV genotypes (3, 5, 19).
In the currently proposed nomenclature for HCV genotyp-ing (13), HCV can be classified into six major genotypes on the basis of extensive sequence comparisons of the HCV core, E1, and NS5 regions. The prevalence of HCV genotypes differs considerably among geographical regions. Genotype 1a is pre-dominant in North America and Europe, while genotype 1b is the major type in Japan. HCV carriers in Japan are exclusively infected with HCV of genotypes 1b, 2a and 2b (17).
Currently, genotypes of HCV are of considerable interest because of their relevance to responses to interferon therapy for chronic HCV infection. Patients infected with HCV of genotypes 2a and 2b show better responses to interferon ther-apy than those infected with genotypes 1a and 1b (16, 21). Thus far, the group-specific PCR has been the principal means for genotyping HCV isolates (1, 7, 11, 14). However, its drawbacks are its complexity and expense. To overcome these problems, serological genotyping based on detection of antibodies to genotype-specific core region or NS4 region antigens has re-cently been developed (9, 12, 20). Some reports have suggested that the results of serological genotyping correlate well with
those of PCR-based genotyping and that serological assays may replace PCR-based ones (9, 12, 20). However, serological genotyping relies on host humoral immune responses, and further studies are necessary to validate its sensitivity and spec-ificity in comparison with those of PCR-based genotyping. At present, the factors which affect the detection of HCV geno-types by serological assays have not been clearly established. It remains to be worked out whether levels of HCV replication, which may influence the typeability of PCR-based assays, also influence that of serological assays.
In this study, HCV genotyping was performed for Japanese patients at various stages of chronic HCV infection by using the group-specific PCR within the core gene and the genotype-specific NS4 antibody assay, and the efficiencies of the two assays were compared in relation to clinical characteristics and levels of HCV replication as assessed by the concentration of HCV RNA in serum.
MATERIALS AND METHODS
Patients.Seventy-five Japanese patients with chronic HCV infection who were positive for HCV RNA in serum according to the results of PCR were studied. Each patient was a native Japanese citizen, and none of the patients was an immigrant from another country. The patients comprised 43 males and 32 fe-males ranging in age from 21 to 79 years. All patients were negative for hepatitis B virus surface antigen and showed no evidence of alcoholic, autoimmune, or drug-induced liver disease. Fifty-nine patients were positive for HCV RNA in their serum, had chronic HCV infection, and had had elevated serum alanine aminotransferase (ALT) levels for more than 6 months. Among this group of patients, 48 consecutive patients without hepatocellular carcinoma and 11 pa-tients with hepatocellular carcinoma, which was proven by imaging procedures, were enrolled separately. The remaining 16 patients were asymptomatic volun-teer blood donors who were positive for HCV RNA in their serum and who had normal ALT levels in their serum. These latter serum samples were obtained from the Osaka Red Cross Blood Center (Osaka, Japan). Liver histology infor-mation was available for the 48 patients with chronic hepatitis C without hepa-tocellular carcinoma, showing chronic persistent hepatitis in 19 patients, chronic active hepatitis in 7 patients, and liver cirrhosis in 22 patients. Of these 75 patients, 16 patients with chronic hepatitis C had had blood transfusions 5 to 34 years earlier. However, none of the patients in this study had a history of * Corresponding author. Mailing address: First Department of
Med-icine, Osaka University Medical School, Yamadaoka 2-2, Suita 565, Japan. Phone: 06-879-3636. Fax: 06-879-3639.
1184
on May 15, 2020 by guest
http://jcm.asm.org/
transfusion of imported blood products. Serum samples drawn from each patient were tested for HCV genotypes and HCV RNA levels. The assays for HCV genotypes and HCV RNA levels were performed in a blinded manner.
Detection and quantification of HCV RNA in serum.HCV RNA was extracted from 100ml of serum samples, copied into cDNA by reverse transcription (RT), and amplified by PCR as described elsewhere (4). Primers were derived from the 59noncoding region of the published sequence (18), which is highly conserved among HCV clones (antisense primer, 59-ATGGTGCACGGTCTACGAGACC TCC-39; sense primer, 59-CACTCCCCTGTGAGGAACTACTGTC-39). The PCR mixtures were amplified in a DNA thermal cycler (Perkin-Elmer Cetus, Norwalk, Conn.) for 40 cycles (948C for 0.5 min, 558C for 1 min, and 728C for 1 min), followed by a 10-min final extension at 728C. A portion of the PCR products was fractionated by agarose gel electrophoresis, transferred onto a nylon membrane, hybridized to a32P-labelled HCV cDNA fragment between the two primers, and autoradiographed. Because of the extreme sensitivity of PCR, great care was taken to prevent false-positive results, and the contamination avoidance measures of Kwok and Higuchi (6) were strictly applied throughout this study. In each assay, we included nine test samples, two negative control serum samples from healthy individuals without risk factors for HCV infection, and one sample of distilled water to monitor for false-positive results. Further-more, the assay was repeated at least twice for each sample, and the reproduc-ibility of the results was confirmed. The sensitivity of the HCV RNA PCR was also investigated with synthetic mutant HCV RNA, as described below. We could constantly detect 30 copies of HCV RNA per sample, and under the best conditions we could detect 5 copies.
To quantify HCV RNA in positive serum samples, a competitive RT-PCR assay was performed as described elsewhere (4). Mutant HCV RNA was pro-duced from an HCV cDNA (M642) to have a novel EcoRI site after amplifica-tion by PCR. RT-PCR was performed with serum samples in the presence of serial 100.5-fold amounts of mutant HCV RNA. Portions of the PCR products were fractionated by agarose gel electrophoresis after digestion with EcoRI, transferred onto a nylon membrane, hybridized to a32P-labelled HCV cDNA, and autoradiographed. The amounts of HCV RNA in serum were estimated from the equilibrium of the signal intensity of a 306-bp undigested DNA frag-ment derived from HCV RNA in serum and that of a 108-bp EcoRI-digested DNA fragment derived from defined amounts of mutant HCV RNA. Compared with other quantitative PCRs based on the amount of HCV cDNA, the advan-tages of this assay are that quantification is independent of many variables influencing the efficiency of RT-PCR. In preliminary experiments, the quantities obtained by the competitive RT-PCR assay were shown to correlate well with those obtained by the branched DNA assay (Chiron Corporation, Emeryville, Calif.) (22), thus indicating that both assays are useful in estimating the relative amount of HCV RNA in serum. Compared with the branched DNA assay, the competitive RT-PCR assay is also advantageous in that it can measure low HCV RNA titers and is unlikely to underestimate HCV RNA titers in patients infected with HCV of genotype 2 (8).
Typing HCV isolates by PCR.HCV RNA-positive serum samples were sub-jected to genotype analysis by the PCR method described previously (8). The HCV isolates were classified into four genotypes (genotypes 1a, 1b, 2a and 2b) on the basis of variations in nucleotide sequences within restricted regions in the putative HCV core region gene. Briefly, a core region sequence was amplified by
PCR with a universal primer pair, and then selective amplification of the first-stage PCR products was performed with a nested pair of a genotype-specific antisense primer and a universal sense primer. The genotype-specific primers were chosen to amplify a sequence of a different size for each genotype. The product of the second-stage PCR was electrophoresed in agarose, and HCV genotypes were identified by the length of the amplified sequence.
Serological genotyping.Group I (genotypes 1a and 1b) and group II (geno-types 2a and 2b) HCV geno(geno-types were further determined by a newly developed serological genotyping assay with genotype-specific recombinant NS4 proteins (20). Group I and II HCV cDNA clones encoding 85 amino acids (amino acids 1676 to 1760) within the NS4 region were expressed in Escherichia coli and were used as group I HCV-specific (C14-1) and group II HCV-specific (C14-2) anti-gens. Antibodies to C14-1 and C14-2 were detected by an enzyme-linked immu-nosorbent assay, and their levels (cutoff index) were measured by the antibody titer assay, as described previously (20). Serum samples with a cutoff index of greater than 1.0 were judged to be positive. Samples with a C14-1/C14-2 cutoff index ratio higher than 2:1 were judged to be group I HCV positive, and those with a C14-2/C14-1 cutoff index ratio higher than 2:1 were judged to be group II HCV positive. When samples had both C14-1 and C14-2 antibodies with a C14-1/C14-2 cutoff index ratio of 0.5 to 2, possible coinfection with group I and group II HCVs was suspected.
Statistical analysis.Statistical analysis for group comparisons was done by the
x2method and the Wilcoxon nonparametric test. A P value of,0.05 (two-tailed) was considered to indicate significance.
RESULTS
Of the 75 patients with chronic HCV infection, the HCV genotypes of the isolates in 67 (89%) patients could be iden-tified by the group-specific PCR of the sequence within the core region gene. Isolates of genotypes 1b, 2a, and 2b were identified in 49 (65%), 13 (17%), and 2 (3%) patients, respec-tively. Three (4%) patients had double infection (genotypes 1b and 2a in two patients and genotypes 1b and 2b in one patient). None of the patients was infected with an isolate of genotype 1a. On the other hand, the HCV genotype(s) could not be determined for the remaining 8 (11%) patients. For these patients, the core region could not be amplified by the first-stage PCR with a universal primer pair.
Table 1 presents the clinical and virological features of the study population in relation to the typeability of the HCV genotypes by PCR. No differences by sex or the incidence of previous blood transfusions were found between the 67 pa-tients with typeable isolates and the 8 papa-tients with untypeable ones, while the patients with untypeable isolates were younger
[image:2.612.58.559.90.279.2]than the patients with typeable ones (P50.001) and showed
TABLE 1. Comparison of clinical and virological features of 75 patients with chronic HCV infection according to detection of their infecting viral genotype by means of the group-specific PCRa
Feature
Typeable by PCR
Untypeable
(n58) P value
Genotype 1b
(n549) Genotype 2a or 2b(n515) Mixed genotypes(n53) (nTotal567)
Age (yr) 53.4611.3 49.6616.1 51.3610.0 52.5612.4 35.969.1 0.001
Sex (no. of males/no. of females) 27/22 12/3 1/2 40/27 3/5 0.42
Previous blood transfusion (no. [%] of patients) 10 (20) 4 (27) 2 (67) 16 (24) 0 0.27
ALT level (U/liter) 85669 92695 71634 86674 1368 0.00003
Diagnosis (no. of patients)b
ASC 5 3 0 8 8
CPH 13 5 1 19 0
CAH 5 1 1 7 0 ,0.00001
Cirrhosis 17 4 1 22 0
HCC 9 2 0 11 0
HCV RNA titers (log10copies/ml of serum) 7.560.8 7.561.1 7.760.8 7.560.9 4.660.5 ,0.00001
aQuantitative data are expressed as means6standard deviations.
bASC, asymptomatic carrier; CPH, chronic persistent hepatitis; CAH, chronic active hepatitis; HCC, hepatocellular carcinoma.
on May 15, 2020 by guest
http://jcm.asm.org/
lower disease activity. The 8 patients with untypeable isolates were all asymptomatic HCV carriers, whereas 8 (12%) of the 67 patients with typeable isolates were asymptomatic HCV
carriers (P,0.00001), and serum ALT levels were significantly
lower in the group with untypeable isolates than in the group
with typeable isolates (13 6 8 versus 86 6 74 U/liter; P 5
0.00003). Serum HCV RNA titers expressed as log10(copy
numbers of HCV RNA per milliliter of serum) were also significantly lower in the group with untypeable isolates than in
the group with typeable isolates (4.6 60.5 versus 7.56 0.9;
P,0.00001). All eight patients with untypeable isolates had
low levels of viremia (,106copies/ml). On the other hand, only
3 (4%) of the 67 patients with typeable isolates had such low levels of viremia and the other 64 (96%) patients had high
levels of viremia ($106copies/ml) (P,0.00001). In the group
with typeable isolates, the patients’ clinical and virological fea-tures had no relation to the HCV genotypes.
Serological genotyping was further performed for isolates from the 75 patients. Sixty-three (84%) had antibody to either C14-1 or C14-2. Neither antibody was detected in the remain-ing 12 (16%) patients includremain-ing the 8 patients whose isolates could not be genotyped by PCR, and serological genotyping could not be done. According to the levels of C14-1 and C14-2 antibodies, 42 of the 63 patients with C14-1 and/or C14-2 antibodies were judged to be infected with group I (genotypes 1a and 1b) HCV isolates, and 13 were judged to be infected with group II (genotypes 2a and 2b) HCV isolates. The other 8 patients had both C14-1 and C14-2 antibodies, but the ratio between the two antibody levels did not exceed twofold. Thus, coinfection with group I and II HCVs was suspected in these patients.
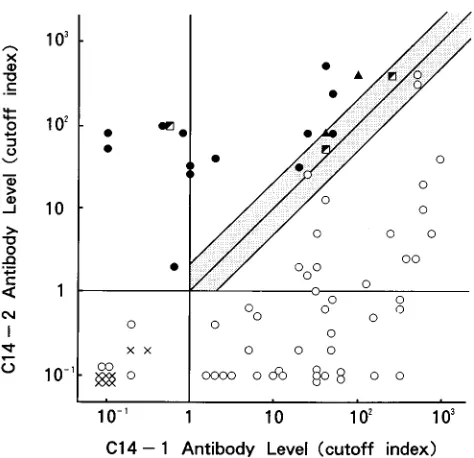
Figure 1 shows the relation between the results of serolog-ical genotyping and those of PCR genotyping. All 42 patients serologically judged to be group I HCV positive were shown by PCR to be infected with genotype 1b isolates. Of the 13 pa-tients found to be infected with group II HCV isolates by the serological assay, genotype 2a and 2b isolates were identified by PCR in 11 and 1 patient, respectively, and the remaining 1 patient was infected with both genotypes 1b and 2b. As for the eight patients in whom coinfection with group I and II HCVs was suspected, PCR genotyping revealed coinfection in only two (25%) patients (genotypes 1b and 2a in both patients) and infection with a single genotype in six (75%) patients (geno-type 1b in three patients, geno(geno-type 2a in two patients, and genotype 2b in one patient). In this study, however, all 44 patients who tested positive for C14-1 antibody with a C14-1/
C14-2 cutoff index ratio of.1 were infected with isolates of
genotype 1b. On the other hand, all 18 patients positive for
C14-2 antibody with a C14-2/C14-1 cutoff index ratio of .1
were infected with isolates of genotype 2a or 2b, although 3 of these 18 patients were also infected with isolates of genotype 1b. Thus, C14-1 and C14-2 antibodies were fairly specific for their corresponding genotypes.
We further investigated the clinical and virological features of the study population in relation to the detection of the genotype-specific antibodies (Table 2). The 12 patients
nega-tive for C14-1 and C14-2 antibodies were younger (P50.005)
and showed lower disease activity than the 63 patients positive for C14-1 and/or C14-2 antibodies. Eight (67%) of the 12 antibody-negative patients were asymptomatic HCV carriers, whereas 8 (13%) of the 63 antibody-positive patients were
asymptomatic HCV carriers, (P 5 0.0001), and serum ALT
levels were significantly lower in the antibody-negative group
than in the antibody-positive group (29636 versus 88675
U/liter; P5 0.0002). A significant difference in serum HCV
RNA titers was also seen between the two groups. The levels of
viremia were lower in the antibody-negative group than in the
antibody-positive group (5.6 6 1.6 versus 7.5 6 0.9; P 5
0.0004). Clinical and virological features in the 63 patients with C14-1 and/or C14-2 antibodies had no relation to the serolog-ical genotyping results.
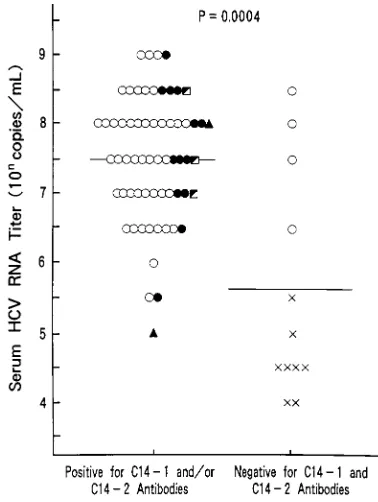
Figure 2 indicates the efficiency of PCR and serological genotyping in relation to serum HCV RNA titers. Isolates
from all 64 patients with levels of viremia of $106 copies/ml
could be genotyped by PCR, while genotype-specific antibody responses were seen in 60 (94%) of them. Four highly viremic patients, who were shown by PCR to be infected with isolates of genotype 1b, did not show any antibody response. As for the
11 patients with low levels of viremia (,106copies/ml), isolates
from only 3 (27%) patients could be genotyped by PCR, and the patients showed genotype-specific antibody responses. Thus, both PCR genotyping and serological genotyping were less efficient for the group with low levels of viremia than for
the group with high levels of viremia (P,0.00001).
DISCUSSION
PCR genotyping of the sequence within the core (11) or NS5 (1) region of the HCV genome has routinely been used in Japan. Both methods are equally efficient in our area, where isolates of genotypes 1b, 2a, and 2b are endemic. HCV isolates from more than 95% of patients with chronic hepatitis C can be genotyped by either method. However, the complexity and expense are disadvantages of PCR genotyping. Moreover, it may not yield satisfactory results in patients with low levels of viremia, which are more frequent in asymptomatic HCV car-riers with low disease activity than in patients with chronic hepatitis C (10, 22). In the current study, PCR genotyping of the sequence within the core region was very efficient for iso-lates from highly viremic patients, and isoiso-lates from all patients
[image:3.612.318.555.68.297.2]with levels of viremia of$106copies/ml could be genotyped. In
FIG. 1. Antibody levels against HCV genotype-specific proteins (C14-1 and C14-2) and infecting viral genotype(s) as defined by the group-specific PCR. Samples in the shaded area reacted to both C14-1 and C14-2, with C14-1/C14-2 cutoff index ratios of 0.5 to 2.E, genotype 1b;F, genotype 2a;å, genotype 2b; i, genotype 1b plus genotype 2a or 2b;3, untypeable by PCR.
on May 15, 2020 by guest
http://jcm.asm.org/
contrast, the HCV genotype(s) could not be determined for
73% of patients with low levels of viremia (,106 copies/ml)
and with low disease activity, thus indicating that a low viral load can reduce the efficiency of PCR genotyping of the se-quence within the core region.
Recently, an alternative serological assay for HCV genotyp-ing has been developed. This assay is based on the detection of
antibodies to genotype-specific NS4 antigens (20). This assay can distinguish group I (genotypes 1a and 1b) and II (geno-types 2a and 2b) HCV geno(geno-types and may serve as a simple method for genotyping in regions where such genotypes are prevalent. In this study, we investigated the sensitivity as well as the specificity of this serological genotyping method in Ja-pan, where HCV carriers are infected exclusively with geno-type 1b, 2a, or 2b. Genogeno-type-specific NS4 antibodies were
found in 94% of highly viremic ($106 copies/ml) patients,
while only 27% of patients with low levels of viremia (,106
copies/ml) showed genotype-specific NS4 antibody responses. These findings suggest that the efficiency of serological geno-typing may also depend on the levels of HCV replication as assessed by the levels of viremia. There have been reports suggesting that HCV carriers with low levels of viremia can show poor antibody responses toward various HCV proteins (15, 23). Taken together, a low viral load seems to cause failure in serological genotyping. In the present study, there were also patients who were highly viremic but who did not show geno-type-specific antibody responses. Thus, serological genotyping, which depends on host humoral immune responses, was not as sensitive as PCR genotyping and could not rescue the failure of PCR genotyping for patients with low levels of viremia.
In this study, there were eight asymptomatic HCV carriers with low levels of viremia whose isolates could not be geno-typed. An explanation for such cases is infection with a unique viral genotype. Unfortunately, we could not determine the HCV genotypes of isolates from these patients by other means. However, HCV carriers in Japan are infected almost exclu-sively with genotype 1b, 2a or 2b, and patients infected with other rarely occurring genotypes (genotypes 1a, 3a, and 3b) often have a history of transfusion of imported blood products or are immigrants from other countries. Our study population did not include such patients. Taken together, infection with a unique viral genotype is unlikely for a small number of our patients, and failure of HCV genotyping is more likely to have relevance to a low viral load. The sensitivities of the PCR and serological genotyping methods that were used were good for patients with chronic HCV infection and abnormal
[image:4.612.73.557.91.271.2]amino-FIG. 2. HCV RNA titers in serum and detection of antibodies against HCV genotype-specific proteins (C14-1 and C14-2) in chronic HCV carriers. The results of detection of their infecting viral genotype by means of the group-specific PCR are also indicated.E, genotype 1b;F, genotype 2a;å, genotype 2b; i, genotype 1b plus genotype 2a or 2b;3, untypeable by PCR. Horizontal bars denote means.
TABLE 2. Comparison of clinical and virological features of 75 patients with chronic HCV infection according to detection of antibodies against HCV genotype-specific proteins (C14-1 and C14-2)a
Feature
Positive for HCV genotype-specific antibodiesb
Negative for antibodies
(n512) P value
Group I
(n542) Group II(n513) Groups I and II(n58) (nTotal563)
Age (yr) 53.7611.3 52.3615.4 45.9611.0 52.4612.2 41.5614.0 0.005
Sex (no. of males/no. of females) 21/21 10/3 5/3 36/27 7/5 0.84
Previous blood transfusion (no. [%] of patients) 9 (21) 4 (31) 2 (25) 15 (24) 1 (8) 0.42
ALT level (U/liter) 83670 84685 116689 88675 29636 0.0002
Diagnosis (no. of patients)c
ASC 5 2 1 8 8
CPH 11 4 3 18 1
CAH 5 0 2 7 0 0.001
Cirrhosis 14 5 2 21 1
HCC 7 2 0 9 2
HCV RNA titers (log10copies/ml of serum) 7.660.8 7.461.2 7.460.7 7.560.9 5.661.6 0.0004
aQuantitative data are expressed as means6standard deviations.
bGroup I, samples with a C14-1/C14-2 cutoff index ratio higher than 2:1; group II, samples with a C14-2/C14-1 cutoff index ratio higher than 2:1; groups I and II,
samples reacting with both C14-1 and C14-2 to a similar extent.
cASC, asymptomatic carrier; CPH, chronic persistent hepatitis; CAH, chronic active hepatitis; HCC, hepatocellular carcinoma.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:4.612.80.269.427.678.2]transferase levels (100 and 93%, respectively). In contrast, both genotyping methods were less sensitive for the asymptom-atic HCV carrier population with low disease activity, among whom patients with low levels of viremia were found more frequently. Further studies are necessary to investigate the sensitivities of various genotyping methods in this population. The serological genotyping method used is based on a com-parison between antibody responses to the two genotype-cific NS4 antigens (C14-1 and C14-2). This assay is fairly spe-cific, because isolates with HCV genotypes corresponding to the predominant antibody response were found in all patients. In this study, patients whose serum samples showed each of the two antibody responses to a similar extent (cutoff index ratio,
#2) were suspected of being coinfected with group I and II
HCVs, according to the criteria presented in an earlier report (20). However, PCR genotyping confirmed coinfection in only 25% of such patients. The reason for this discrepancy is un-clear. Further studies are necessary to elucidate whether this discrepancy is caused by very low levels of viremia of one HCV genotype which cannot be detected by PCR or by cross-reac-tivity due to epitopes shared by group I and II HCVs. More-over, one patient was serologically judged to be infected with group II HCV but was infected with both group I and II HCVs according to the results of PCR genotyping. These observa-tions indicate that the specificity and sensitivity of the serolog-ical genotyping method are problematic as far as the diagnosis of double infection is concerned.
Finally, serological assays for HCV genotyping have impor-tant practical advantages over PCR genotyping from technical and economic points of view. It has been suggested that sero-logical assays may be sensitive and specific enough to replace PCR genotyping (9, 12, 20). Thus far, the efficiencies of both assays have not been fully compared in relation to HCV rep-licative states. Our data indicate that low levels of viral repli-cation may reduce the efficiency of serological genotyping as well as PCR genotyping and that the overall sensitivity of serological genotyping, which relies on host humoral immune responses, may not be as high as that of PCR genotyping. Another problem is how to diagnose double infection. Sero-logical genotyping, which is based on a comparison of the different antibody responses elicited by different HCV geno-types, is necessarily indirect. Thus, the results of serological genotyping should be interpreted with caution, especially for double infection. Before serological assays are routinely used for HCV genotyping, further studies are necessary to improve their sensitivity and specificity. Moreover, a more geographi-cally diverse panel of patient sera should be examined to de-termine the applicability of the worldwide use of the assay because the distribution of HCV genotypes differs consider-ably among various areas of the world. A serological genotyp-ing assay such as our assay cannot be used throughout the world unless epitopes for distinguishing the various genotypes are made available. We must further emphasize that serolog-ical genotyping may not be used for testing individuals whose humoral immune responses are impaired for various reasons.
ACKNOWLEDGMENTS
This work was supported by a grant-in-aid from the Ministry of Education, Science and Culture, Japan.
We are indebted to Yohsuke Ohta and Osamu Yanagihara from International Reagents Corporation for technical assistance.
REFERENCES
1. Chayama, K., A. Tsubota, Y. Arase, S. Saitoh, I. Koida, K. Ikeda, T. Mat-sumoto, M. Kobayashi, S. Iwasaki, S. Koyama, T. Morinaga, and H.
Ku-mada.1993. Genotypic subtyping of hepatitis C virus. J. Gastroenterol. Hepatol. 8:150–156.
2. Choo, Q.-L., G. Kuo, A. J. Weiner, L. R. Overby, D. W. Bradley, and M. Houghton.1989. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science 244:359–362.
3. Choo, Q.-L., K. H. Richman, J. H. Han, K. Berger, C. Lee, C. Dong, C. Gallegos, D. Coit, A. Medina-Selby, P. J. Barr, A. J. Weiner, D. W. Bradley, G. Kuo, and M. Houghton.1991. Genetic organization and diversity of the hepatitis C virus. Proc. Natl. Acad. Sci. USA 88:2451–2455.
4. Hagiwara, H., N. Hayashi, E. Mita, T. Takehara, A. Kasahara, H. Fusamoto, and T. Kamada.1993. Quantitative analysis of hepatitis C virus RNA in serum during interferon alfa therapy. Gastroenterology 104:877–883. 5. Kato, N., M. Hijikata, Y. Ootsuyama, M. Nakagawa, S. Ohkoshi, T.
Sug-imura, and K. Shimotohno.1990. Molecular cloning of the human hepatitis C virus genome from Japanese patients with non-A, non-B hepatitis. Proc. Natl. Acad. Sci. USA 87:9524–9528.
6. Kwok, S., and R. Higuchi. 1989. Avoiding false positives with PCR. Nature 339:237–238.
7. McOmish, F., P. L. Yap, B. C. Dow, E. A. C. Follett, C. Seed, A. J. Keller, T. J. Cobain, T. Krusius, E. Kolho, R. Naukkarinen, C. Lin, C. Lai, S. Leong, G. A. Medgyesi, M. Hejjas, H. Kiyokawa, K. Fukada, T. Cuypers, A. A. Saeed, A. M. Alrasheed, M. Lin, and P. Simmonds.1994. Geographical distribution of hepatitis C virus genotypes in blood donors—an international collaborative survey. J. Clin. Microbiol. 32:884–892.
8. Mita, E., N. Hayashi, H. Hagiwara, K. Ueda, Y. Kanazawa, A. Kasahara, H. Fusamoto, and T. Kamada.1994. Predicting interferon therapy efficacy from hepatitis C virus genotype and RNA titer. Dig. Dis. Sci. 39:977–982. 9. Mondelli, M. U., A. Cerino, F. Bono, A. Cividini, A. Maccabruni, M. Arico`,
A. Malfitano, G. Barbarini, V. Piazza, L. Minoli, and E. Silini.1994. Hep-atitis C virus (HCV) core serotypes in chronic HCV infection. J. Clin. Microbiol. 32:2523–2527.
10. Naito, M., N. Hayashi, H. Hagiwara, N. Hiramatsu, A. Kasahara, H. Fusamoto, and T. Kamada.1994. Serum hepatitis C virus RNA quantity and histological features of hepatitis C virus carriers with persistently normal ALT levels. Hepatology 19:871–875.
11. Okamoto, H., Y. Sugiyama, S. Okada, K. Kurai, Y. Akahane, Y. Sugai, T. Tanaka, K. Sato, F. Tsuda, Y. Miyakawa, and M. Mayumi.1992. Typing hepatitis C virus by polymerase chain reaction with type-specific primers: application to clinical surveys and tracing infectious sources. J. Gen. Virol. 73:673–679.
12. Simmonds, P., K. A. Rose, S. Graham, S.-W. Chan, F. McOmish, B. C. Dow, E. A. C. Follett, P. L. Yap, and H. Marsden.1993. Mapping of serotype-specific, immunodominant epitopes in the NS-4 region of hepatitis C virus (HCV): use of type-specific peptides to serologically differentiate infections with HCV types 1, 2, and 3. J. Clin. Microbiol. 31:1493–1503.
13. Simmonds, P., A. Alberti, H. J. Alter, F. Bonino, D. W. Bradley, C. Brechot, J. T. Brouwer, S. W. Chan, K. Chayama, D. S. Chen, Q. L. Choo, M. Colombo, H. T. M. Cuypers, T. Date, G. M. Dusheiko, J. I. Esteban, O. Fay, S. J. Hadziyannis, J. Han, A. Hatzakis, E. C. Holmes, H. Hotta, M. Houghton, B. Irvine, M. Kohara, J. A. Kolberg, G. Kuo, J. Y. N. Lau, P. N. Lelie, G. Maertens, F. McOmish, T. Miyamura, M. Mizokami, A. Nomoto, A. M. Prince, H. W. Reesink, C. Rice, M. Roggendorf, S. W. Schalm, T. Shikata, K. Shimotohno, L. Stuyver, C. Trepo, A. Weiner, P. L. Yap, and M. S. Urdea.1994. A proposed system for the nomencla-ture of hepatitis C viral genotypes. Hepatology 19:1321–1324. 14. Stuyver, L., R. Rossau, A. Wyseur, M. Duhamel, B. Vanderborght, H. Van
Heuverswyn, and G. Maertens.1993. Typing of hepatitis C virus isolates and characterization of new subtypes using a line probe assay. J. Gen. Virol. 74:1093–1102.
15. Sugitani, M., G. Inchauspe´, M. Shindo, and A. M. Prince. 1992. Sensitivity of serological assays to identify blood donors with hepatitis C viraemia. Lancet 339:1018–1019.
16. Takada, N., S. Takase, N. Enomoto, A. Takada, and T. Date. 1992. Clinical backgrounds of the patients having different types of hepatitis C virus ge-nomes. J. Hepatol. 14:35–40.
17. Takada, N., S. Takase, A. Takada, and T. Date. 1993. Differences in the hepatitis C virus genotypes in different countries. J. Hepatol. 17:277– 283.
18. Takamizawa, A., C. Mori, I. Fuke, S. Manabe, S. Murakami, J. Fujita, E. Onishi, T. Andoh, I. Yoshida, and H. Okayama.1991. Structure and orga-nization of the hepatitis C virus genome isolated from human carriers. J. Virol. 65:1105–1113.
19. Takeuchi, K., Y. Kubo, S. Boonmar, Y. Watanabe, T. Katayama, Q.-L. Choo, G. Kuo, M. Houghton, I. Saito, and T. Miyamura.1990. The putative nu-cleocapsid and envelope protein genes of hepatitis C virus determined by comparison of the nucleotide sequences of two isolates derived from an experimentally infected chimpanzee and healthy human carriers. J. Gen. Virol. 71:3027–3033.
20. Tanaka, T., K. Tsukiyama-Kohara, K. Yamaguchi, S. Yagi, S. Tanaka, A. Hasegawa, Y. Ohta, N. Hattori, and M. Kohara.1994. Significance of specific antibody assay for genotyping of hepatitis C virus. Hepatology 19:1347–1353.
on May 15, 2020 by guest
http://jcm.asm.org/
21. Yoshioka, K., S. Kakumu, T. Wakita, T. Ishikawa, Y. Itoh, M. Takayanagi, Y. Higashi, M. Shibata, and T. Morishima.1992. Detection of hepatitis C virus by polymerase chain reaction and response to interferon-a ther-apy: relationship to genotypes of hepatitis C virus. Hepatology 16:293– 299.
22. Yuki, N., N. Hayashi, T. Takehara, H. Hagiwara, N. Hiramatsu, M. Naito, Y.
Kawanishi, K. Katayama, A. Kasahara, H. Fusamoto, and T. Kamada.1994. Serum hepatitis C virus RNA levels and liver injury in volunteer blood donors. Am. J. Gastroenterol. 89:1462–1466.
23. Yuki, N., N. Hayashi, A. Kasahara, H. Hagiwara, K. Ohkawa, H. Fusamoto, and T. Kamada.1994. Hepatitis C virus replication and antibody responses toward specific hepatitis C virus proteins. Hepatology 19:1360–1365.