African
Journal
of
Urology
Official
journal
of
the
Pan
African
Urological
Surgeon’s
Association
web
page
of
the
journal
www.ees.elsevier.com/afju www.sciencedirect.com
Review
Management
of
anterior
urethral
strictures
with
buccal
mucosa:
Our
pioneering
experience
Abdelwahab
Elkassaby
∗,
Mohamed
Kotb
DepartmentofUrology,FacultyofMedicine,AinShamsUniversity,Egypt
Received21January2016;accepted25January2016 Availableonline2March2016
KEYWORDS
Anteriorurethralstrictures;
Urethroplasty;
Buccalmucosagraft
Abstract
Urethralstricturemanagementisachallengingsurgery.Multiplicityoftechniquesmeansthatnoneofthem isideal.Nosingletechniqueisappropriateforallsituationsandthesuccessfulsurgeonshouldhaveastore ofoperationstochoosefromaccordingtoeachspecificcase.Thisreviewaimstoprovideanupdateonthe differentusesofbuccalmucosalgraftasareconstructiveandreplacementtoolforanteriorurethralstrictures management.
©2016PanAfricanUrologicalSurgeons’Association.ProductionandhostingbyElsevierB.V.Allrightsreserved.
Historicalbackground
Buccalmucosagraft(BMG)wasfirstuseasaurethralreconstructing toolbyHumbyin1941.Heusedalowerlipgraftforapatientwith multiplehypospadiasrepairpresentedwithpenoscrotalfistula[1]. Thiswasfollowedbyalongperiodofinactivity.
In1978,westartedusingbuccalmucosalgraftsformanagement ofcrippled hypospadias.Preliminaryresultswere not encourag-ing.ThefirstpublishedserieswerebyBurgeretal.,in1992,who describedtheuseofbuccalmucosalgraftinsixpatients;threeof themwithpriorfailedhypospadiasrepairandshortageofgenital
∗Correspondingauthor.
PeerreviewunderresponsibilityofPanAfricanUrologicalSurgeons’ Association.
skin[2].Againtheresultswereunsatisfactorytill1995,when Duck-ettetal.successfullyusedbuccalmucosaforurethralreconstruction afterhypospadias,epispadiasandurethralstrictures[3].
In 1993, El-Kassabyetal. publishedthe first seriesforanterior urethralstricture repair usingbuccalmucosal grafts.20 patients underwent1-stagecorrectionofananteriorurethralstrictureusing a buccalmucosapatch graft.This techniquewas usedforshort strictures(1–2cm)thatusuallyrequireda2–4cmrepair.Results weresuccessfulin18patients,while2redosurgeryforrecurrent stricture[4].
Anatomicandhistologicconsiderations
Theoralmucosaisthemucousmembraneliningtheinneraspect ofthemouth.Ithastwomajorlayers,namelytheepitheliumand theunderlyingconnectivetissue(termedlaminapropria).Another http://dx.doi.org/10.1016/j.afju.2016.01.003
Masticatorymucosaisformedofkeratinizedstratifiedsquamous epithelium,found on thedorsum of thetongue, hardpalateand attachedgingiva.Itsstructureallowsittoresisttheabrasionofrough foodparticles.
Lining mucosa is formed of nonkeratinized stratified squamous epithelium,foundalmosteverywhereelseintheoralcavity, includ-ingbuccal,labialandalveolarmucosa[5,6].
• Buccalmucosareferstothemembraneliningoftheinner sur-faceofthecheeksfromthelineofcontactoftheopposinglips anteriorlytothelineofthepterygomandibularraphe(lateralto retromolartrigone)posteriorly.Themedialboundaryisthelineof attachmentofthebuccalmucosatotheupperandloweralveolar ridgessuperiorlyandinferiorly.Itconsistsofstratifiedsquamous epithelium(oralepithelium)andanunderlyingconnectivetissue (laminapropria)[7].
• Labialmucosareferstotheinsideliningofthelips.
• Alveolarmucosareferstothemucosabetweenthegumsandthe buccal/labialmucosa.
Specializedmucosafoundspecificallyintheregionsofthetastebuds onlingualpapillaeonthedorsalsurfaceofthetonguethatcontains nerveendingsforgeneralsensoryreceptionandtasteperception [5,6].
Anteriorurethralstrictures
Theanteriorurethralstrictureequalsnarrowingoftheanterior ure-thra.Thepathologyisexplainedmainlybyfibrosisandscarringof theurethralepitheliumtogetherwiththespongyerectiletissueof corpusspongiosum[8].
Etiologyofanteriorurethralstrictures
Toomanycausesparticipateinthisprocess.Infection,traumaand lichensclerosisareconsideredasthemostcommonetiologies. How-ever,mostcausesofurethralstricturesremainunknown,butthey areprobablyduetoaremoteunrecognizedperinealtraumaor recur-rentattacksofurethralmildinfections(asNeisseriagonorrheaor Chlamydia)[9].
Thepathologicalprocessincludesinjurytotheurethralepithelium ortheunderlyingcorpusspongiosumleadingtohealingbyascar whichendsbyananteriorurethralstricture.Trauma,usually strad-dle,eitherpresentsasacuteretentionandurethralbleeding,ormore oftengoesunrecognizedandpresentslaterwithobstructive void-ingcomplaints.Iatrogenictraumatotheurethracouldbethecause, ascatheterizationandendoscopicprocedures,butitdecreaseswith finemanipulationoftheurethra[10].
Lichensclerosusetatrophicusisanothercommonchronic inflam-matory conditionthat affectsthe anteriorurethra as wellas the foreskinandglans.Itisconsideredasafrequentcauseofphimosis, meatalstenosisandlonganteriorstrictures.
Lichensclerosischaracterizedwithuncertainetiology,varied pre-sentation,andmultipletreatments.Inearlystages,ashortcourseof steroids,topicalorsystemic,cancontrolthediseaseandprevent progression.Surgical treatmentby circumcision canbecurative ifthe diseaseistreatedearlywhenstilllocalized.Progressionto longsegmentstrictureorpanurethralstricturewillnecessitatemore sophisticatedmanagement[12].
Presentationofurethralstricturepatients
Thesepatientsusuallypresentwithlowerurinarytractobstructive symptomsorrecurrenturinarytractinfectionssuchasprostatitis orepididymitis.Somepatientsalsopresentwithurinaryretention. Butwithdetailedhistory,mostofthesepatientsarefoundtohave toleratednotablevoidingobstructivesymptomsforalongperiodof timebeforeprogressingtocompleteobstruction[10].
Evaluationofanteriorurethralstrictures
Tostart treatment, the natureof the stricture includingstricture anatomyshouldbeaccuratelydetermined.Thelocationandlength ofthestrictureisdeterminedusingradiography[13],urethroscopy, flexiblecystoscopy[14]andultrasonography[15].Thedepthand densityofthescarinthespongytissueismoredifficulttoestimate butitcouldbemeasuredbyultrasonographyormagneticresonance imaging.MoreyandMcAninchfoundthatultrasonography accu-ratelydefinestheextentofspongiofibrosisinbulbarurethra[15].It usuallyexceedstheappearanceofthestricturelengthmeasuredin thecontraststudies.Itisverybeneficialforreconstructiveurologists toattendtheurethrographyordoingitbythemselves.
Evenbytheuseofallofthesetools,thefinalandmostaccurate evaluationofstricturewillbeavailableduringsurgeryassistedby antegradeorretrogradeendoscopy.
Managementofanteriorurethralstrictures
Ithasbeensaidthatthereisnotissuebetterthantheurethratoreplace the urethra. Thisis trueforshort stricturein the bulbar urethra amenableforexcisionandprimaryanastomosis.Butthisis how-evernotpossibletoachievewithlongerstricturestoavoidtherisks ofexcessivemobilizationandpenilecurvature.That’swhy urolo-gistsshouldbefamiliarwiththeuseofmanysurgicaltechniquesto dealwithanyconditionoftheurethraduringsurgery.
Amongthesetechniques,penilegraftshavebeenusedtoreconstruct theurethrainthosestrictures.Toimprovethesurvivaland vascu-larity,theuseoflocalflapshasalsobeenadvocated.Flapshowever aretechnicallydemanding,andarenotsuitableincasesofLichen Sclerosis.
Inpursuit forthebestgraftmaterial,bladdermucosaandbuccal mucosalgraftshave been used. The useof the latter hasmany advantages[4,16].
Figure1 AugmentedRussellTechniqueshowingclosureoftheroofusingbuccalmucosalgraftafterexcisionofstricturedsegment[18].
Treatmentoptionsforanteriorurethralstrictures
Differenttreatmentoptionsareavailableformanagementof ante-riorurethralstricturesdependingonstricturesiteandlength.This includes:
1. Excisionwithpartial anastomosis:Heusner,Dugas,Hamilton Russell.
2. Excisionwithprimaryanastomosis:Heitz,Boyer,Marion. 3. Stagedrestoration.
4. Flapreconstruction.
5. Graftreconstruction(Skin,BladderandBuccal) 6. Recently:tissueculture,acellularmatrices.
Augmentationandsubstitutionurethroplasty
Excisionwithpartialanastomosis Heusner,Dugas,HamiltonRussell
Theuseofexcisiontechniquesinthetreatmentofurethralstrictures wassummarizedbyHamiltonRussellin(1915).Thesetechniques arenotpreferredbymanysurgeonsbecausefurtherstricture forma-tiongavedisappointinglong-termresults[17].
In2007,El-Kassabyandcolleaguespresenttheir10-yrexperience withone-stagerepairoflongbulbarurethralstricturesusing aug-menteddorsal strip anastomosis in >234 cases. Bulbarurethral strictureshadameanof4.2cmofwhichameanof2.8cmdiseased urethralsegmentwasincised.Followedbyexcisionofmostofthe fibrosedspongiosum,suturingoftheroof(Russell)andgraftingthe floorwithBuccalmucosalgraft.Theoverallsuccessrateexceeded 93%[18](Fig.1).
Ventraldefectin“AugmentedRussel DorsalstripAnastomosis” couldbecoveredusingfreegraftofnonhirsutegenitalskin,buccal mucosa,bladdersubmucosa,orabipedicledpenileskinflap(Fig.2).
Excisionwithprimaryanastomosis Heitz,BoyerandMarion
AppliedbyMarionin(1912)andHeitz-Boyerin(1922),excision ofthestenosedsegment,end-to-endanastomosis,andsuprapubic cystostomyimprovedthesuccesswithstricturesurgery.In1975,
TurnerWarwickreportedexcellentresultsofanobliqueend-to-end anastomosisinthebulbousurethra[17].
Stagedrepairtechniques
Stagedrepairoflongbulbarurethralstricturesisoneoftheoldest formsofurethralreconstruction.Multistagereconstructioninvolves exposureoftheurethratotheoutsidewithorwithoutexcisionand grafting.3–12monthslater,aftertheinflammationsettlesdownand thegraftbecomeswelltaken,thedefectisclosed.
In1911,HamiltonRussellusedexternalurethrotomyfortherelief oflongrecurrenturethralstricturesespeciallyanteriorurethral stri-ctures.Heincisedtheurethraforthewholelengthofthestricture andthensuturedtheedgesoftheurethratotheadjacentskin,thus creatinganartificialhypospadius[17].
An extension ofthe Hamilton Russeltechnique,the buried-skin techniquewasintroducedbyDenisBrownein(1949).DenisBrowne establishedthatastripofpenileskinwouldinevitablyformatube ifleftinsituandburiedbyclosingtheskinoverit.
JohnSwinney(1952)excisedthestrictureandallscartissueand thenclosedtherawareawithadjacentskin.Thesecondstagewas aTheirsch-Duplay[17].
Recently,stagedrepairislimitedtosomespecificindications.This includesstricturesassociatedwithchronicinflammation,previous recurrentinfectionsorabscess,radiation,spinalcordinjuries, fis-tulas,false passages, urethral diverticula, and failed priorrepair [19].
Stagedrepairincludesexcisionofunhealthytissuesfollowedby bridgingofthedefectbyagraftandlatertubularization[20](Fig.3). WeuseFull-thicknessskingrafts(FTSG),Split-thicknessskingrafts (STSG)orbuccalgraftsintheseprocedures.
Flapreconstruction
Thefirstdescriptionofanislandofskinwithanaxialbloodsupply usedforurethralreconstructionwasbyDuckettein1980[21].
Figure2 “AugmentedRusselDorsalstripAnastomosis”showingaugmentationoftheventralfloordefectusingventral penileflap.
Figure3 Secondstagerepairoflongurethralstricturefollowingfirststagebuccalmucosalgrafting.
Quartey(1983)describedasimilartechniqueusingtheflapto recon-structtheurethrafollowingstricturesanywherefromtheexternal meatustotheprostaticurethra[22].
Graftreconstruction Skingrafts
Since(1953)PresmanandGreenfield,usedpreputialskingraftto manageabulbarurethralstricture[23].LaterDevineandHorton popularizedthetechniqueusingfreefullthicknesshairlessskingraft toreconstructtheurethrainaone-stagerepairofhypospadias[24]. Extrapenilefullthicknessskinhasnotbeenapopulargrafttissue forurethralreplacementduetosuboptimalresults[25].
Barbaglietal.(1996),followingtheconceptadvocatedbyMonseur, introducedthe dorsallyplaced graft.Itallowsbettermechanical supportforthegraft withanadequatevascular bedforthegraft fromtheunderlyingcorporealbodies[26].
Twomaintypesofskingraftsareavailableaccordingtothethickness ofgrafttaken;split-thicknessandfullthicknessskingrafts. split-thicknessgraft (STG)includesthe epidermis andthe superficial dermal(intradermal)plexus.Afull-thicknessgraft(FTG)includes theepidermis, the superficialdermisand the deepdermis. They aremoredurableanddoesnotcontractasSTG.Extragenital full-thicknessskingraftscarryincreasedmass,whichgenerallymakes themmorefastidiousthangenitalfull-thicknessgrafts(i.e.,preputial andpenileskingrafts)[27].
Bladderepithelialgraft
Memmelaar(1947)wasthefirsttoreporttheuseofbladder epithe-liumforurethralreconstruction[28].
Bladderepitheliumhasbeenanattractivematerialforconstruction oftheneourethrainrepeatrepairsofhypospadiasandother com-plexurethralanomalies.Theytendtohavemorefavorablevascular
Figure4 Lowerlipbuccalmucosalgraft.
characteristics.Itisaccustomedtoexposuretourine,resists shrink-age,andisreadilyavailableinadequateamounts[29].
Therewasa highincidenceofmeatalproblems withthe useof bladderepitheliumasaurethralsubstitute.Theexposedepithelium behavessimilartotheexstrophybladderepithelium,which hyper-trophies,becomessticky, andeventually metaplastic.Itdevelops mucin-secretingglands, leadingto prolapseand/or stenosis[30]. Weavoidedthisinourongoingseriesofpanurethralstricturerepair followingLichensclerosis.Ourtechniqueincludestheproximaluse ofbladdermucosaandthedistalrepairusingbuccalmucosalgraft withniceresultsyet.Futurestudiesshouldtakeinconsiderationthat randomizationisnotpossiblebecausedifferenttechniquesarenot suitableforallcases.
Buccalmucosalgraft
Advantagesofbuccalmucosalgrafts. Variousfactorshave con-tributedtotheacknowledgementofbuccalmucosalgrafts(BMGs) asanidealsubstituteforthe urethra,includingeasyaccessibility andmanualhandling,resistancetoinfection,compatibilitywitha wetenvironment,athickepitheliumandathinlaminapropria,and favorablegrafthostvascularrelationshipallowingearly inoscula-tion.
Buccalmucosalgrafthasa‘panlaminarplexus’,whichprovides optimalvasculartake[27].
Thebuccalmucosapatchgraftishairlessandcantoleratetrauma andinfectionadequatelywithhighpowerofregeneration[4]. Theoralmucosaalsoprotectsthehostagainstinvadingpathogens throughtoughlaminapropriathatprovidesresistancetotearforces andprotectagainstmicroorganisms.Thisprotectionfrom microor-ganismsisalsoduetocellsheddingfromthesurfacelayer,therefore minimizingcolonization.Theoralmucosa containsacompetent immunesystemkeepingtheoralmucosainahealthystatedespite theheavymicrobialloadusuallyfoundintheoralcavity[31,32]. Buccalmucosadiffersfromintestinalmucosainthatitdoesnothave anadsorptivecapacity,althoughdifferencesinpermeabilityexistin directcorrelationtothethicknessoftheepithelialbarrier[5,33]. Surgicaltechnique
1. Graftharvest 2. Position
3. UrethroplastywithBuccalMucosalGraft(Exposure, Mobiliza-tion,Graftplacement,Closure,Post-operativecare).
Harvestingofbuccalmucosalgraft Donorsite
Atthebeginningofourexperience,westartedbyharvestingalower lipgraftthenshiftedtocheekoneortwosides(Fig.4).NowLip
Figure5 Dingmanmouthgagwith3bladesforcheekbuccalmucosal graftharvesting.
graftsarelimitedtolongstrictures,ifneeded,togetherwithbilateral cheekgraft.Werarelyuselingualmucosa.
Technique
The technique of harvesting the graft has been variable; some authorspreferharvestofthegraftbeforeexposingthestrictureto shortenthetimeinlithotomyposition[34].
Ourpreferenceisthe2-teamapproach.Thisdecreasesthetimingof thesurgerybutitneedsproperdecisionmakingbeforethesurgery. Generalanesthesiabynasalintubationispreferred.Followedby sterilizationanddrapingoftheoralcavityandtheperinealfieldin thesametime.Sterilizationofthemouthusingchlorhexidineand Betadinefortheperioralarea.
WealsopreferusingtheDingmanmouthgagwith3blades(Fig.5). Othersimplermouth retractorsare alsoavailable. Thiscouldbe helpedbysomestayand/orevertingsuturestothelipsifneeded. Stensenductismarked.Alsothegraftismarkedonthecheekand/or the lower lip.A mixtureof lidocaine and epinephrine couldbe injectedalongthelateralbordersofthegraft tostretchthegraft anddecreasebleeding.
Thegraft is separatedfrom theunderlying buccinatorwithcare to avoid deeper dissectionin the muscle wherethe branches of neurovascularplanelies.
Thedonorsiteisinspectedforhemostasisusingbipolarcauteryand epinephrinesoakedgauzesarelefttostayforfewminuteswhilethe
Figure6 CompletePerineopenileDegloving.
graftisdefattened.Thegraftisheldforde-fatteningasthishelps thegrafttakeattherecipientsite.
Thegraftishandedtotheurethraltraytable,andthedonorsiteis closedusingcontinuous3-0vicryl.Theepinephrinesoakedcottonis leftatthedonorsitewhichwillberecheckedattheendofthesurgery beforedischargetorecovery.Somesurgeonspreferonlyhemostasis forthegraftwithsomeedgesutureswithoutapproximatingthetwo opposingedges.Thisispreferredinwidegraftsespeciallyfromthe lips.
Weuseanantibioticsolutiontosoakthegraftafterharvest.
Patientpositioning
In Ain ShamsUniversity, weaccess to the perineumthrough a lowlithotomy positionwhilesome surgeonspreferthe exagger-atedlithotomy[35].Compartmentsyndromeismorefrequentin thelowlithotomyposition,thisresultfromcalfcompression lead-ingtodecreasedvenousoutflowandincreasedpressurewithinthe legcompartmentsresultingindecreasedarterialinflowandischemic injury.Sopressureonthecalfmusclesespeciallybytheassistant surgeonshouldbeavoided.
Urethroplastyusingbuccalmucosalgraft Exposure
Shortanteriorurethralstricturescouldbemanagedthroughapenile deglovingincisionfollowedbyurethralmobilizationandpenileskin graft.
Forlongerstrictures,especiallythoseduetolichensclerosisorwith deficientnon-hirsutepenileskin,buccalmucosacouldbeusedwith differentincisionapproach:
Perinealincision:alambdashapedincisionissharplyoutlinedin theperineum(somesurgeonspreferalongitudinalincision) Kulkarnietal. describedin 2000anew,fulllength(penile and bulbar),one-stageoralmucosalgrafturethroplastyinpatientswith panurethralstricturesduetolichensclerosus[36].
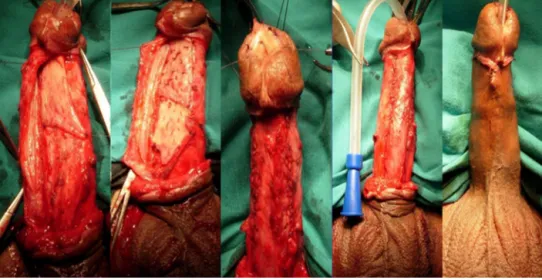
Ourtechniqueformanagementofsuchstricturesincludesperineal incisiontogetherwithanothersubcoronalpeniledeglovingincision. Thisallowsfullpenileretrievalthroughtheperineuminwhatwe call“CompletePerineopenileDegloving”(Fig.6).Thistechnique offerseasierrepairofpanurethralstricturedowntothemeatus.
Figure7 Theurethraisexposedbyretractionoftheischiocavernosus muscles.
Mobilization
Dissectioniscarrieddowntothemidlinefusionofthe ischiocaver-nosusmuscles,whichiscompletelyseparatedfromthespongiosum (Fig.7).
Thecorpusspongiosumisdetachedfromitsbondtotheperineal body,andtheproximalbloodsupplyisdivided.Thedissectionis carriedproximallyasfarasthemembranousurethra(Fig.8). Distallythe corpus spongiosum is detached from the triangular ligamenttothemidscrotallevel,andseparatedfromthecorpora cavernosa,withexcisionofpartsofBuck’sfascia(Fig.9). In 2009, Barbagli modified his own technique [37]; combining theuseofmuscleandnervesparingbulbarurethroplastywiththe fulllengthdorsalurethralopeningfromKulkarni’stechnique.This offerspreservationofthelateralvascularsupplytotheurethra,the centraltendonoftheperineum,thebulbo-spongiosummuscleand itsperinealinnervations[38].
Graftplacement Dorsalgrafting
Theproximalendofthestrictureislocalizedusingcautious ante-gradepassageofcurvedurethralmetaldilator.Thisisveryimportant especiallyinlongstricturesreachingthemembranousorproximal
Figure8 Theurethramobilizedfromthecorporaandfromthe peri-nealbody.
Figure9 Distaldissectionoftheurethra.
bulbararea.Anothermethodincludestheuseofantegradeflexible cystoscopy.
Localizationofthedistalsegmentisusuallybylargecaliberneleton plasticcatheter.Thisgoalcouldbealsoachievedusingretrograde urethroscopy.Alsosterilemethyleneblueinjectioninthedistalend willgivebetteridentificationofthehealthymucosaespeciallyin longstrictures.
Thelimitofthestrictureismarkedontheurethraandusingasharp scalpeltheurethraisopeneddorsally.Urethralstrictureiseither inciseddorsallyifthestricturecaliberiswideoritisexcised.The edgesarecheckedanddébridedofanyfibroustissue,theurethra isthenspatulateddorsally. Thegraft isthenspread fixedto the triangularligamentandcorporacavernosa.
Thegraftismeshedusingasharpscalpelthentheedgeofthegraftis suturedtothespatulatedurethra.Theflooroftheurethrais reapprox-imated.Thisisdonebyholdingthe2lateralendstogetherby3-0
PDSavoidingepithelium,thenepitheliumisclosedby6-0Vicryl andthecorpusspongiosumissuturedtogetherby4-0PDS.Also somesurgeonsprefersuturingfullthicknessurethralwallinstead ofdoublelayeredsuturing.
Thelateraledgesofthestricturotomyarethensuturedtothegraft using4-0Vicrylthuscompletingtheonlay(Fig.10).
Ventralgrafting
Theurethraisopenedventrally.Theurethraisthespatulated ven-trally.
Thegraftisthenplacedandmeticulouslysewntotheepithelium. Withthegraftinplacethebulkofthecorpusspongiosumisthen suturedtothegrafttobeginthespongioplasty.Thiswilladd bet-tergraft revascularizationand “Take”.Finallytheadventitiaand theremainingbulkofthecorpusspongiosumaresuturedbyPDS sutures.
Ventral,dorsalorlateralgrafts
Thedorsalonlayprocedureforbulbarstricturesgotsome advan-tagesovertraditionalventralonlayurethroplasty.Fixingthegraft totheundersurfaceofthecorporalbodiesappearstoprovideboth anexcellentbloodsupplyandgoodmechanicalsupport,reducing shrinkage,chordeeformationandventralgraftsacculation[26]. Lat-eralgraftingalsoprovidesminimalunilateraldissectionandshould betakeninconsiderationinsomecases.Thethreeapproaches; ven-tral,dorsalorlateral[39]graftpositioning,hasprovidedthesame successratesandstricturerecurrencerate[40].
Urethralsubstitutionwithbuccalgraft
Inlongstrictures,ifinvolvingthepenileurethraandcausingpenile curvature,thepenileurethrashouldbeexcisedandtotallyreplaced bybuccalmucosalgraftasafirststagerepairthenretubularization ofthe graftin the secondstagebecausetube replacementisnot recommendedanymore.Thisisaformofsubstitutionurethroplasty. Incaseof“Multistageurethroplasty”ofthepenileurethrabybuccal graft,careshouldbetakentofacilitatereconstructionofthebedof theappliedgraftsbyputtingthepeniledartosinthelateralpartsof theappliedgrafts.Sothegraftshouldnotbeapplieddirectlyonthe tunicaalbugineaofthepenilecorpora.Thewillfacilitatesthefuture tubularizationofthetakengraftsinthesecondstagefromthelateral sides.
Closure
Foleysiliconurethralcatheterispassedbeforeclosingthe anasto-mosis.Itshouldbeofsmallercaliberthantheneletoncatheterused forrepair.Hemostasisisreassuredthenclosureofwoundinlayers leavingsmallcalibersuctiondrain.
Postoperativecare
1. Patientremainsinbedrestforthefirst48hthenallowed ambu-latingwithassistance;activityislimitedtowalkingandreclining inthebedwithnoprolongedsitting.Thepatientisadvisedto maintainmildactivitytillthecathetersareremovedin4weeks.
Figure10 Urethraldorsalgraftingwithbuccalmucosalgraftforlongpenileurethralstrictureduetolichensclerosis.
Figure11 Theofacellularcollagenmatrixgraftingasanofftheshelfengineeredtissueinmanagementofurethralstrictures.
2. Dietisallowedastoleratedwithnorestrictions,stoolsofteneris givenfor10days.Oralgelcouldbeusedandcoldsoftfoodtill healingoforalgraftbed.
3. AntibioticcoveringgramnegativeorganismisgivenIVfor48h thenthepatientisstartedonsuppressivetherapyfor4weeks. 4. Neurovascularchecksforcompartmentsyndrome, as wellas
DVTandatelectasisprophylaxisistakenintoaccount. 5. In4weeksthepatientreturnsforthevoidingtrialafterremoval
of the urethralcatheter. The suprapubic tubeis plugged and removedin2days.
6. After voidingtrial, they werefollowed up at3months with uroflowmetry,retrogradeurethrogram(RGU).
7. Patientswerefurtherfollowed-upwithuroflowmetryat3months intervalandRGUevery6monthsintervalforthefirst2years. Andlateronifneeded
Recurrentstrictures
Theidealtherapyforrecurrentstrictureafteropenurethroplastyhas notbeenestablished.Repeaturethroplastyisfrequentlyacomplex andlengthyprocedures.
Flaps are preferredfor substitutionurethroplastybecauseof the theoreticaladvantagethattheycarrytheirownbloodsupplyleading
tobetterviabilitychances.Recently,therehasbeenatrendtoward grafts,particularlybuccalmucosalfreegrafts.
Buccalmucosacouldbeusedinprimaryandsalvage urethroplas-ties,asdorsalonlay,ventralonlay,andastubedgraftsinurethral strictures.Thebuccalgraftisanexcellentandavailablesourceof materialforurethralreplacementincomplexurethroplasties. Multistageproceduresmayrepresentabetterchoiceinrepeated ure-throplastiesespeciallyinthepresenceofseverefibrosisorrecurrent nearinfections.
Thefutureofanteriorurethralstricturesurgery
Thefutureofanteriorurethralsubstitutesseemsto lieon Tissue Engineering.Acellularcollagenmatrixgraftingasanofftheshelf engineeredtissuewasintroducedbyElkassabyetal.in2003[41]. Thiswillobviatetheneedfortissuetransferinpatientswithlong andcomplexstrictureswithnolimitationsasregardsthequantityor qualityofurethralsubstitutesavailableinanygivenpatient(Fig.11). Goodprimitiveresultsareavailablebutlongtermfollowuptogether withcostcontrolarestillneeded.Nowadays,itisunclearwhether cellseedingcouldbeanadvantageinthenearbyfuture.
Conflictofinterests None.
Funding None. References
[1]HumbyG.Aone-stageoperationforhypospadiasrepair.BrJSurg 1941;29:84–92.
[2]BürgerRA,MüllerSC,el-DamanhouryH,TschakaloffA,Riedmiller H,HohenfellnerR.Thebuccalmucosalgraftforurethral reconstruc-tion:apreliminaryreport.JUrol1992;147(3):662–4.
[3]DuckettJW,CoplenD,EwaltD,BaskinLS.Buccalmucosalurethral replacement.JUrol1995;153(5):1660–3.
[4]El-KasabyAW,FathallaM,NoweirAM,El-HalabyMR,ZakariaW, El-BeialyMH.Theuseofbuccalmucosapatchgraftinthemanagement ofanteriorurethralstrictures.JUrol1993;149(2):276–8.
[5]NanciA.Tencate’soralhistology:development,structureandfunction. 7thed.St.Louis,MO,USA:MosbyElsevier;2008.p.411.
[6]Bath-BaloghM,FehrenbachMJ.Illustrateddentalembryology, histol-ogy,andanatomy.Elsevier;2011.p.106.ISBN-13:978-1437717303 ISBN-10:1437717306.
[7]SquierCA,KremerMJ.Biologyoforalmucosaandesophagus.JNatl CancerInst2001;(29):7–15.Monographs.
[8]AndrichDE,MundyAR.Urethralstricturesandtheirsurgical treat-ment.BJUInt2000,86571–580.580.
[9]FentonAS,MoreyAF,AvilesR,GarciaCR.Anteriorurethralstrictures: etiologyandcharacteristics.Urology2005;65(June(6)):1055–8. [10]JordanGH,SchlossbergSM.Surgeryofthepenisandurethra.In:Walsh
PC,RetikAB,VaughanJrED,editors.Campbell’surology,4,8thed. Philadelphia:WBSaunders;2002.p.3886–952.
[11]VennS,MundyA.Urethroplastyforbalanitisxeroticaobliterans.BJU 1998;81:735–7.
[12]StewartL,McCammonK,MetroM,VirasoroR.SIU/ICUD consul-tationonurethralstrictures:anteriorurethra-lichensclerosus.Urology 2014;83(3Suppl):S27–30.
[13]McCallumRW,DevineCJ.Methodofdynamicretrogradeand void-ingcystourethrographyinurethralstricture.AUAUpdateSer1991;10. Lesson12.
[14]JeziorJ,JordanGH.Managementofbulbousurethralstricture.AUA UpdateSer2003;22(1):2–7.
[15]MorreyA,McAninchJ.Sonographicstagingofanteriorurethral stri-ctures.JUrol2000;163:1070–5.
[16]BarbagliG,LazzeriM.Surgicaltreatmentofanteriorurethralstricture diseases:briefoverview.IntBrazJUrol2007;33(4).RiodeJaneiro. [17]MurphyLJT.Theurethra,inthehistoryofurology.CharlesCThomas:
Springfield,IL;1972.p.453–82.
[18]El-KassabyAW,El-ZayatTM,El-AzzazyS,OsmanT.One-stagerepair oflongbulbarurethralstricturesusingaugmentedRusselldorsalstrip anastomosis:outcomeof234cases.EurUrol2008;53:420–4.
[19]SecrestCL.Stagedurethroplasty:indicationsandtechniques.UrolClin NAm2002;29:467–75.
[20]SchreiterF,NollF.Meshgrafturethroplastyusingsplitthicknessskin graftorforeskin.JUrol1989;142:1223–6.
[21]DucketteJrJW.Transversepreputialislandflaptechniqueforrepairof severehypospadias.UrolClinNAm1980;7:423.
[22]QuarteyJKM.OneStagepenile/preputalislandflapurethroplastyfor urethralstricture.JUrol1985;134:474.
[23]PresmanD,GreenfieldD.Reconstructionoftheperinealurethrawitha freefullthicknessskingraftfromtheprepuce.JUrol1953;69:677–80. [24]DevinePC,HortonCE,DevineSrCJ,DevineJrCJ,CrawfordHH, AdamsonJE.Useoffullthicknessskingraftsinrepairofurethral strictures.JUrol1963;90:67–71.
[25]WebsterGD,BrownMW,KoefootJrRB,SihelnickS.Suboptimal resultsinfullthicknessskingrafturethroplastyusinganextrapenile skindonorsite.JUrol1984;131:1082–3.
[26]BarbagliG,SelliC,diCelloV,MottolaA.Aonestagedorsalfreegraft urethroplastyforbulbarurethralstrictures.BrJUrol1996;78:929–32. [27]JordanGH.Principlesoftissuetransfertechniquesinurethral
recon-struction.UrolClinNAm2002;29:267–75.
[28]MemmelaarJ.UseofBladdermucosainaonestagerepairof hypospa-dias.JUrol1947;58:68.
[29]KinkeadTM,BorziPA,DuffyPG,RansleyPG.Longtermfollow upofbladdermucosagraftformaleurethralreconstruction.JUrol 1994;151:1056–8.
[30]WeingartnerK,KozakewichHP,HendrenWH.Nephrogenicadenoma afterurethralreconstructionusingbladdermucosa:reportof6cases andreviewoftheliterature.JUrol1997;(September):158.
[31]NovakN,HaberstokJ,BieberT,AllamJP.Theimmuneprivilegeof theoralmucosa.TrendsMolMed2008;14:191–8.
[32]PageRC,SchroederHE.Pathogenesisofinflammatoryperiodontal disease.Asummaryofcurrentwork.LabInvest1976;34:235–49. [33]LavelleCLB.Appliedoralphysiology.2nded.CostaMesa,CA,USA:
WrightPublishingCompany;1988.p.244.
[34]MoreyA,McAninchJW.Techniqueofharvestingbuccalmucosafor urethralreconstruction.JUrol1996;155:1696–7.
[35]AngermeierKW,JordanGH.Complicationsoftheexaggerated litho-tomyposition:Areviewof177cases.JUrol1994;151:866–8. [36]KulkarniSB,KulkarniJS,KirpekarDV.Anewtechniqueof
urethro-plastyforbalanitisxeroticaobliterans.JUrol2000;163:352. [37]BarbagliG,SelliC,TostoA,PalminteriE.Dorsalfreegraft
urethro-plasty.JUrol1996;155:123.
[38]BarbagliG,DeStefaniS,AnninoF,DeCarneC,BianchiG. Mus-cleandnervesparingbulbarurethroplasty:anewtechnique.EurUrol 2008;54:335.
[39]Kulkarni S,Barbagli G,Sansalone S,LazzeriM.One-sided ante-rior urethroplasty: a new dorsal onlay graft technique. BJU Int 2009;104(October(8)):1150–5.
[40]BarbagliG,PalminteriE,GuazzoniG,MontorsiF,TuriniD,LazzeriM. Bulbarurethroplastyusingbuccalmucosagraftsplacedontheventral, dorsalorlateralsurfaceoftheurethra:areresultsaffectedbythesurgical technique?JUrol2005;174:955–7.
[41]El-KassabyAW,RetikAB,YooJJ,AtalaA.Urethralstricturerepair withanofftheshelfcollagenmatrix.JUrol2003;169(1):170–3.
![Figure 1 Augmented Russell Technique showing closure of the roof using buccal mucosal graft after excision of strictured segment [18].](https://thumb-us.123doks.com/thumbv2/123dok_us/9693074.2850752/3.918.214.716.91.353/figure-augmented-russell-technique-showing-closure-excision-strictured.webp)