fibers in the splanchnic nerve and in postganglionic fibers of cardiac nerves.5In addition, it acts directly at α2-receptors in the lower brainstem region to suppress sympathetic outflow.6Clonidine also stimulates parasympathetic outflow, resulting in prolongation of the refractoriness of the atrioventricular node. It is through this shift in the balance of sympathetic and parasympathetic tone that clonidine may benefit patients with atrial fibrillation. So far, findings from a placebo-controlled study have suggested that clonidine is effective when used to control ventricular responses in patients with new-onset rapid atrial fibrillation.7We set out to test the hypothesis that clonidine effectively reduces heart rate in this patient group. We also wished to determine whether it is as effective as traditional treatments for acute rate control.
Methods
We conducted a randomized, nonblinded clinical trial com-paring clonidine with digoxin and verapamil in the treatment of new-onset rapid atrial fibrillation (see Table I for the medica-tion protocol). Patients were assigned to 1 of 3 medicamedica-tion treatments in an unconcealed manner (assignments were based on the final digit of patients’ hospital identification num-bers). Patients were followed up for a 6-hour period. The
api-Despite extensive literature on the subject, the acute management of rapid atrial fibrillation remains contro-versial. Pharmacologic management for acute rate con-trol has consisted primarily of treatment with digitalis, calcium channel blockers, and β-blockers.1-3 Sympa-thetic tone is known to play an important role in the genesis and maintenance of atrial fibrillation, as well as in the degree of atrioventricular node conduction and ventricular response.4It seems reasonable therefore to postulate that efforts to reduce sympathetic tone may result in better control of the ventricular rate in atrial fibrillation and perhaps also contribute to the restora-tion of sinus rhythm. Clonidine, an imidazoline, decreases discharges in sympathetic preganglionic
From the aDivision of Cardiology, Department of Medicine, Queen’s University, Kingston, Ontario, and the Departments of bMedicine and cCommunity Health Sci-ences, University of Calgary, Calgary, Alberta, Canada.
W. A. G. was funded as a Population Health Investigator by the Alberta Heritage Foundation for Medical Research, Edmonton, Alberta, Canada.
Submitted September 27, 2000; accepted April 26, 2001.
Reprint requests: Christopher S. Simpson, Kingston General Hospital, Division of Car-diology, Level 3, Kidd Wing, 76 Stuart St, Kingston, Ontario K7L 2V7, Canada. E-mail: [email protected]
Copyright © 2001 by Mosby, Inc.
1097-6744/2001/$35.00 + 0 4/90/116761 doi:10.1067/mhj.2001.116761
Clinical assessment of clonidine in the treatment of
new-onset rapid atrial fibrillation: A prospective,
randomized clinical trial
Christopher S. Simpson, MD, FRCPC, FACC,aWilliam A. Ghali, MD, MPH, FRCPC,b,cAnthony J. Sanfilippo, MD,
FRCPC, FACC,aSabine Moritz, Dipl Biol MSc,cand Hoshiar Abdollah, MB, ChB, FRCPC, FACCaKingston, Ontario,
and Calgary, Alberta, Canada
Purpose
The role of digoxin and verapamil in the control of ventricular response in rapid atrial fibrillation is well estab-lished. This study investigates how clonidine compares with these standard therapies in rate control for new-onset rapid atrial fibrillation. We set out to test the hypothesis that clonidine effectively reduces heart rate in patients with new-onset rapid atrial fibrillation.Subjects and Methods
Forty patients were seen in the emergency department with new-onset (≤24 hours’ dura-tion), stable, rapid atrial fibrillation. Eligible patients were randomized to receive either clonidine, digoxin, or verapamil. Changes in heart rate and blood pressure over 6 hours, as well as frequency of conversion to sinus rhythm were recorded and analyzed.Results
The mean reduction in heart rate over 6 hours was 44.4 beats/min (95% confidence interval [CI] 28.4-60.4 beats/min) in the clonidine group, 52.1 beats/min (95% CI 40.8-63.4 beats/min) in the digoxin group, and 41.8 beats/min (95% CI 22.5-61.0 beats/min) in the verapamil group. Analysis of variance of the heart rate changes in the 3 groups after 6 hours was not significant (P= .55). At 6 hours, 7 of 12 clonidine patients, 8 of 15 digoxin patients, and 7 of 13 verapamil patients remained in atrial fibrillation (P= .962 on χ2).Conclusion
Clonidine controls ventricular rate in new-onset atrial fibrillation with an efficacy comparable to that of standard agents. (Am Heart J 2001;142:e3.)cal heart rate, a 12-lead electrocardiogram, blood pressure, heart rhythm, and symptoms were all recorded at 0, 0.5, 1, 2, 3, 4, and 6 hours. At 6 hours subjects exited the study. Adult patients seen in the emergency departments of the 2 acute-care hospitals in Kingston, Ontario, Canada, were considered for entry into the study if they were in atrial fibrillation with a ventricular response exceeding 100 beats/min and if the symptoms had begun within the preceding 24 hours. Patients were specifically excluded if they had significant hemody-namic instability, were unable to take oral medications, had a pre-excitation syndrome, were currently on one of the three study drugs, or were unable or unwilling to give informed consent. The trial protocol was reviewed and approved by the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board.
Analysis
The primary end point of the study was heart rate reduction. We also examined blood pressure changes and the rate of con-version to normal sinus rhythm. Changes in heart rate and blood pressure within groups between time 0 and time 6 hours were analyzed with the paired ttest. These changes were also evaluated with 95% confidence intervals (CIs). Intergroup com-parisons were made by analysis of variance (ANOVA) and unpaired ttests with Bonferroni correction of the calculated P values. The incidence of conversion to normal sinus rhythm was analyzed with the χ2test. An αvalue of .05 was used in all statistical tests. Power calculations showed that, with an aver-age of 13 patients per treatment group, we had 81% power (ie, type II error rate 0.19) to detect between-group heart rate dif-ferences of 10 beats/min (assumptions for this calculation: µ1= 95 beats/min, µ2= 105 beats/min, σ= 9 beats/min).
Results
Study population
Patients were enrolled between May 7, 1994, and Janu-ary 1, 1996. During this time 141 patients were admitted with a primary diagnosis of rapid atrial fibrillation. Of
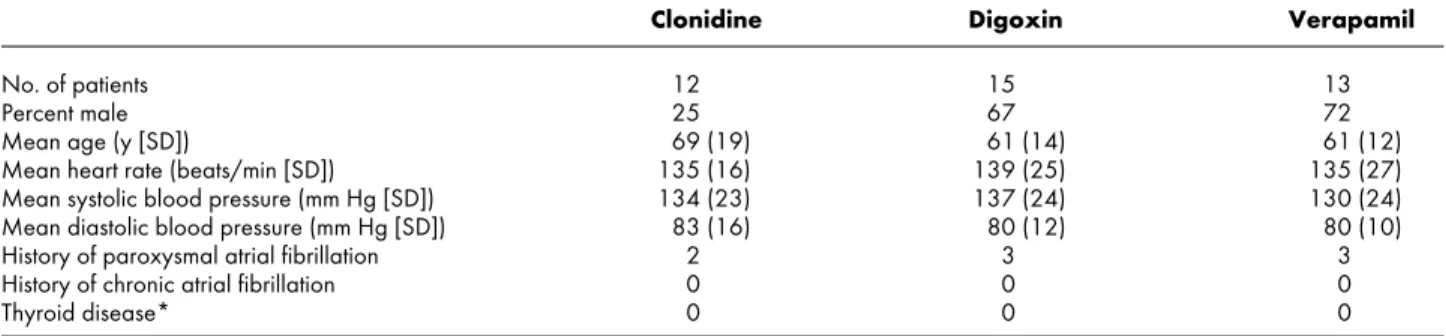
those, 82 were treated before they could be considered for enrollment. The remaining 59 were evaluated and considered for entry into the study. Forty-two of the 59 met eligibility criteria and were asked to participate in the study; 40 agreed to do so. Of the 17 who did not meet eligibility criteria, 6 were already on digoxin and 11 had atrial fibrillation that, by history, had been present for more than 24 hours. The eligibility criteria were therefore satisfied by 71% of those referred for considera-tion. All 40 patients were recruited from the emergency departments, all were admitted to the hospital, and all completed the 6-hour protocol. The baseline characteris-tics of the study patients are shown in Table II. Despite the randomization process, a greater proportion of women was randomized to the clonidine group com-pared with the other 2 groups.
Heart rate reduction
The change in heart rate over the 6-hour duration of the study is shown in Figure 1. The heart rate at time 0 was similar between groups (mean 135.0 beats/min, SD 15.6 beats/min for the clonidine group, mean 139.1 beats/min, SD 24.6 beats/min for the digoxin group, and mean 135.3 beats/min, SD 26.8 beats/min for the verapamil group). The mean reduction in heart rate over 6 hours was 44.4 beats/min (95% CI 28.4-60.4 beats/min) in the clonidine group, 52.1 beats/min (95% CI 40.8-63.4 beats/min) in the digoxin group, and 41.8 beats/min (95% CI 22.5-61.0 beats/min) in the vera-pamil group. ANOVA of the heart rate changes in the 3 groups after 6 hours was not significant (P= .55).
Changes in heart rate for those patients remaining in atrial fibrillation throughout the study (ie, for the entire 6-hour period) were also examined. Again, the heart rate at time 0 was similar between groups (mean 134.3 beats/min, SD 18.3 beats/min for the clonidine group, n = 7; 139.4 beats/min, SD 24.3 beats/min for the digoxin group, n = 8; and 129.7 beats/min, SD 21.2 beats/min for the verapamil group, n = 7). The mean reduction in heart rate over 6 hours was 28.7 beats/min (95% CI 12.4-45.0 Figure 1
Heart rate change over time for patients in atrial fibrillation treated with clonidine, dioxin, or verapamil.
Clonidine
0.1 mg orally at time 0
0.1 mg orally at time = 2 h if heart rate >100 beats/min Digoxin 0.5 mg intravenously at time 0 0.25 mg intravenously at time = 2 h 0.25 mg intravenously at time = 4 h Verapamil 2.5 mg intravenously at time = 0
5.0 mg intravenously at time = 5 min if heart rate >100 beats/min 5.0 mg intravenously at time = 10 min if heart rate >100 beats/min 80 mg orally at time = 2 h if heart rate >100 beats/min
Table I. Study medication protocols for patients in atrial fibril-lation treated with clonidine, digoxin, or verapamil
beats/min) in the clonidine group, 47.0 beats/min (95% CI 30.6-63.4 beats/min) in the digoxin group, and 21.6 beats/min (95% CI 6.5-36.7 beats/min) in the verapamil group. ANOVA of the heart rate changes at 6 hours for patients remaining in atrial fibrillation was significant (P= .035). Unpaired ttests with Bonfer-roni correction for pairwise comparisons were not significant with the exception of the digoxin-verap-amil comparison (P= .040).
Figure 2 shows intergroup comparisons for patients remaining in atrial fibrillation at various time intervals. The verapamil group had a greater reduction in heart rate compared with the other 2 groups at 0.5 hours (P= .007) and at 1 hour (P= .027), but no differences could be demonstrated between groups at 2, 3, or 4 hours. By 6 hours the subjects in the digoxin group who remained in atrial fibrillation had a lower mean heart rate than did subjects in the verapamil group who were still in atrial fibrillation (digoxin: mean 92.4
beats/min, SD 9.1 beats/min vs verapamil mean 108.1 beats/min, SD 15.3 beats/min), but the difference was not significant (P= .120). The clonidine group remain-ing in atrial fibrillation at 6 hours had a mean heart rate that was not significantly different than either of the other 2 groups, although there was a trend toward bet-ter control with digoxin (clonidine: mean 105.6 beats/min, SD 16.6 beats/min, vs digoxin: 92.4 beats/min, SD 9.1 beats/min; P= .242).
Conversion to normal sinus rhythm
Figure 3 depicts the proportion of patients remaining in atrial fibrillation in each of the 3 groups at various time intervals. At 6 hours the proportion of patients remaining in atrial fibrillation was very similar (7/12 clonidine patients, 8/15 digoxin patients, and 7/13 ver-apamil patients remained in atrial fibrillation) and χ2 analysis did not demonstrate a statistically significant difference among groups (P= .962). However, conver-sion to sinus rhythm was achieved more quickly in the clonidine and digoxin group compared with patients in
Clonidine Digoxin Verapamil
No. of patients 12 15 13
Percent male 25 67 72
Mean age (y [SD]) 69 (19) 61 (14) 61 (12)
Mean heart rate (beats/min [SD]) 135 (16) 139 (25) 135 (27)
Mean systolic blood pressure (mm Hg [SD]) 134 (23) 137 (24) 130 (24)
Mean diastolic blood pressure (mm Hg [SD]) 83 (16) 80 (12) 80 (10)
History of paroxysmal atrial fibrillation 2 3 3
History of chronic atrial fibrillation 0 0 0
Thyroid disease* 0 0 0
*Measured thyroid-stimulating hormone at presentation outside the normal range.
Table II. Baseline characteristics of study patients in the 3 treatment groups: clonidine, digoxin, and verapamil
Figure 2
Heart rate change over time for patients remaining in atrial fi-brillation after 6 hours of treatment with clonidine, digoxin, or verapamil.
Figure 3
Percentage of patients remaining in atrial fibrillation at each time interval during treatment with clonidine, digoxin, or verap-amil.
the verapamil group, although this difference was not statistically significant (P= .40 for χ2analysis at 2 hours).
Systolic blood pressure changes
In the clonidine group a mean change in systolic blood pressure of –18 mm Hg (95% CI –29.5 to –6.5 mm Hg) was observed. Although this drop in systolic blood pressure was statistically significant, it did not result in symptoms attributable to hypotension in any of the clonidine subjects. The digoxin group had a mean change of 2.1 mm Hg (95% CI –7.9 to 12.1 mm Hg) and the verapamil group had a mean change of –7.2 mm Hg (95% CI –17.9 to 3.6 mm Hg). ANOVA for the difference in systolic pressure at 6 hours was signifi-cant (P= .023). Pairwise comparisons between groups were not significant with the exception of the compari-son between the digoxin and clonidine groups (P= .019).
Diastolic blood pressure changes
The clonidine group showed a mean change of –8.7 mm Hg, SD 19.4 mm Hg (95% CI –21.0 to 3.7 mm Hg, P= .151). The digoxin group had a mean change of –0.9 mm Hg (95% CI –6.4 to 4.5 mm Hg), and the verapamil group had a mean change of –6.8 mm Hg (95% CI –12.2 to –1.3 mm Hg). ANOVA and pairwise comparisons did not demonstrate any significant inter-group differences (P= .2897 on ANOVA).
Adverse effects
Symptoms (lightheadedness and palpitations) re-ported as “adverse effects” occurred in 2 patients from each group. All symptomatic subjects in the study reported their symptoms at time 0, before medications were administered. Four of the 6 symptomatic patients (2 in the clonidine group, 1 each in the other 2 groups) converted to sinus rhythm and their symptoms
resolved. The other 2 patients (both in the digoxin group) reported some easing of the symptoms at 6 hours. These reported symptoms therefore appeared to represent symptoms of atrial fibrillation rather than adverse effects to the medication.
Discussion
The role of digoxin and verapamil in the control of ventricular response in atrial fibrillation is well estab-lished.8β-Blocker therapy is also standard treatment for rate control in new-onset atrial fibrillation. In recent years intravenous diltiazem has also been established as a very safe and effective means of rate control.9-12(We did not include a diltiazem arm in our study because it was unavailable at our center at the time.) These “tried and true” therapies have firmly established themselves as safe, effective, and well tolerated. Why, then, was it necessary to study the role of clonidine in this
popula-tion? In 1992 Roth et al7published a small series that suggested a benefit of clonidine over placebo for rate control in new-onset rapid atrial fibrillation. Our aim was to place this finding in some context by comparing clonidine with standard therapies. Digoxin and verap-amil provide a valid and established benchmark for the assessment of any new rate-control strategy.
Our findings suggest that clonidine compares favor-ably with standard therapies in rate control for new-onset rapid atrial fibrillation. Despite their efficacy in ventricular rate control, however, digoxin and verap-amil have not been demonstrated to play a significant role in the restoration of sinus rhythm.13In this study clonidine showed no advantage over the standard ther-apies in this regard. Although a larger study may demonstrate statistical significance of small differences, our results suggest that a clinically significant advantage is unlikely to be found. Roth et al,7however, found that 6 of 9 patients in their clonidine group converted to sinus rhythm in 4 hours compared with 1 of 9 in their placebo group. Although this did not reach statistical significance, it was a strong trend. Rates of spontaneous conversion appear to depend on the underlying etiol-ogy of the atrial fibrillation, the duration, and the fol-low-up time. For patients presenting less than 72 hours after arrhythmia onset, as was the case in our popula-tion, the spontaneous conversion rate overall appears to be in the vicinity of 40%.14
The clonidine group in our study showed a statistically significant decrease in systolic blood pressure compared with digoxin. This is not surprising, given clonidine’s tra-ditional role as an antihypertensive agent. Although no clinically important episodes of hypotension occurred in our series, we cannot exclude the possibility that this could become a problem for some patients.
Treatment of new-onset atrial fibrillation with oral clonidine, we believe, is unlikely to establish itself as a commonly applied alternative to standard therapies. In its oral preparation, the onset of action is slower than intravenous preparations of verapamil. Interestingly, however, oral clonidine does compare favorably with intravenous digoxin (a drug still commonly used in the elderly and in patients with poor left ventricular func-tion) in terms of the time to onset of treatment effect. Although it is clear that most patients will require intra-venous treatment, this is not always necessary, and clonidine may therefore represent an opportunity to treat some patients outside the hospital setting. In addi-tion, clonidine has more recently become available in a transdermal patch form. This may offer a more rapid onset of action without the need for a visit to the emer-gency department.
This study has a few limitations. First, the use of both oral and intravenous agents made it difficult to design a double-blinded protocol. However, we felt that the out-come measures being assessed (heart rate, blood
pres-sure, and conversion to normal sinus rhythm) were objective and not likely to be subject to significant observer or subject bias. Second, randomization was not concealed. Although this has the potential to intro-duce selection bias, Table II reassuringly shows that baseline heart rate and blood pressure were similar across groups. Third, we did not use a placebo arm because this would have meant that some patients would have gone untreated for 6 hours. Roth et al,7 however, found in their placebo group a spontaneous rate change of –15 + 16.8 beats/min over 4 hours. This does not approach the magnitude of change seen in each of our 3 treatment groups. Fourth, the study was small. Although we anticipated sufficient power to detect clini-cally significant differences in the main group compar-isons, the subgroup comparisons were underpowered. Even for the main group comparisons we may have been somewhat underpowered because the SDs for heart rate were higher than the value of 9 that we had anticipated in our power calculation. Also, although the 3 medica-tions appear to be similarly efficacious with respect to rate control and conversion to normal sinus rhythm, we cannot exclude the possibility that with a larger sample size our study might have shown significance for smaller differences among the 3 groups. Last, although the dos-ing protocols for digoxin and verapamil were standard-ized in this study, the dosing of clonidine was empirically determined. A more aggressive protocol using higher or more frequent doses might have eliminated the observed trend in favor of digoxin.
Conclusions
This study helps to place the previous study by Roth et al7in context. Clonidine results in a significant reduction in heart rate in patients with new-onset rapid atrial fibrillation, with an efficacy comparable to stan-dard treatment. It appears to be a potential alternative to standard agents in the management of these patients, although larger studies may be required to establish its safety profile, efficacy, and optimal dosing. Although its low cost, wide availability, and easy administration make it a potentially attractive addition to the pharma-cologic armamentarium against atrial fibrillation, its rel-atively slow onset of action and potential for blood pressure reduction may be a disadvantage for some patients. Given that clonidine appears to be effective as a rate-controlling drug in new-onset atrial fibrillation,
further studies may now be indicated to explore the potential for this drug as a long-term rate-controlling agent in chronic atrial fibrillation.
References
1. Repique LJ, Shah SN, Marais GE. Atrial fibrillation 1992: manage-ment strategies in flux. Chest 1992;101:1095-103.
2. NHLBI Working Group on Atrial Fibrillation. Atrial fibrillation: cur-rent understandings and research imperatives. J Am Coll Cardiol 1993;22:1830-4.
3. Gardiner MJ, Gilbert M. Heart rate control in patients with atrial fi-brillation: Canadian Cardiovascular Society Consensus Conference on Atrial Fibrillation. Can J Cardiol 1996;12(A Suppl):21-3A. 4. Allessie MA, Camers WJEP, Bonke FIM, et al. Experimental
evalua-tion of Moe’s multiple wavelet hypothesis of atrial fibrillaevalua-tion. In: Zipes DP, Jalife J, editors. Cardiac electrophysiology and arrhyth-mias. Orlando: Grune & Stratton; 1985. p. 265-75.
5. Langer SZ, Cavero I, Massingham R. Recent developments in nor-adrenergic neurotransmission and its relevance to the mechanism of action of certain antihypertensive agents. Hypertension 1980;2: 371-82.
6. Flacke JW, Bloor BC, Flacke WE, et al. Reduced narcotic require-ment by clonidine with improved hemodynamic and adrenergic sta-bility in patients undergoing coronary artery bypass surgery. Anes-thesiology 1987;67:11-9.
7. Roth A, Kaluski E, Felner S, et al. Clonidine for patients with rapid atrial fibrillation. Ann Intern Med 1992;116:388-90.
8. Waxman HL, Myerburg RJ, Appel R, et al. Verapamil for control of ventricular rate in paroxysmal supraventricular tachycardia and atrial fibrillation or flutter. Ann Intern Med 1981;94:1-6. 9. Phillips BG, Gandhi AJ, Sanoski CA, et al. Comparison of
intra-venous diltiazem and verapamil for the acute treatment of atrial fib-rillation and atrial flutter. Pharmacotherapy 1997;17:1238-45. 10. Schreck DM, Rivera AR, Tricarico VJ. Emergency management of
atrial fibrillatin and flutter: intravenous diltiazem versus intravenous dioxin. Ann Emerg Med 1997;29:135-40.
11. Ellenbogen KA, Dias VC, Cardello FP, et al. Safety and efficacy of intravenous diltiazem in atrial fibrillation and atrial flutter. Am J Car-diol 1995;75:45-9.
12. Ellenbogen KA, Dias VC, Plumb VJ, et al. A placebo-controlled trial of continuous intravenous diltiazem infusion for 24-hour heart rate control during atrial fibrillation and atrial flutter: a multicenter study. J Am Coll Cardiol 1991;18:891-71.
13. Falk RH, Knowlton AA, Bernard SA, et al. Digoxin for converting recent-onset atrial fibrillation to sinus rhythm. Ann Intern Med 1987;106:503-6.
14. Talajic M, MacDonald RG, Nattel S. Restoration of sinus rhythm in patients with atrial fibrillation. Canadian Cardiovascular Society Consensus Conference on Atrial Fibrillation. Can J Cardiol 1996; 12 Suppl A: 29A-35A.