Supported by
REPORT
Clinical and Cost Considerations
For Managing Postsurgical Pain:
Elastomeric Pumps and Continuous Catheters,
or a Single-Dose Non-Opioid Local Analgesic
P
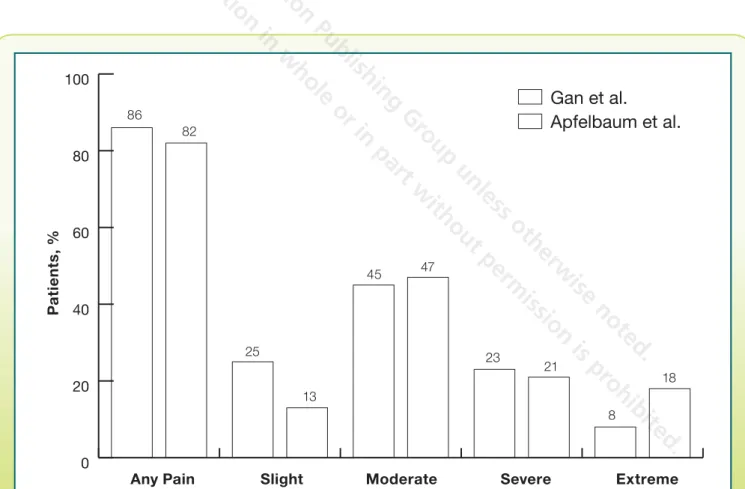
ostsurgical pain is a common phenomenon and can have a significant effect on patient outcomes and health care costs. For example, in 2003, Apfelbaum and colleagues1 conducted a survey of 250 adults who recently had undergone surgical procedures, and report-ed that 80% of patients experiencreport-ed acute pain after surgery; 86% reported moderate, severe, or extreme pain. Furthermore, 23% of patients who received painmedications experienced adverse effects (AEs). More recently, Gan and colleagues2 conducted a survey of a random sample of 300 adults who had undergone surgery within the previous 5 years. Approximately 86% experi-enced pain after surgery and of these, 75% had moderate or extreme pain during the immediate postsurgical period (Figure 1).1,2 After being discharged from the hospital, 74% reported a continuation of these pain levels.
Faculty
Susan E. Downey, MD, FACS
Clinical Associate Professor of Surgery (Plastic) Department of Surgery
University of Southern California Keck School of Medicine
Los Angeles, California
Jacob Hutchins, MD
Director, Regional and Acute Pain Program Department of Anesthesiology University of Minnesota Medical Center
Minneapolis, Minnesota
John Pilcher, MD, FACS, FASMBS
Medical Director, Bariatric Surgery TexSan Heart Hospital
San Antonio, Texas
Andrew Rogalski, PharmD, BCPS
Clinical Pharmacy Specialist
Program Director, Pharmacy Practice (PGY1) Residency University Medical Center of Princeton at Plainsboro
Plainsboro, New Jersey
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
Undermanaged postsurgical pain has broad implications for clinical care.3-5 Indeed, various studies have demonstrat-ed that undermanagdemonstrat-ed pain after surgery is associatdemonstrat-ed with longer hospital lengths of stay, a higher rate of complications (including cardiovascular, pulmonary, renal, and psycholog-ical sequelae), increased risk for developing chronic pain syndromes, and decreased patient satisfaction.3,5 Because health care utilization organizations are tracking pain-related end points as measures of quality of care in surgical patients (eg, within the Hospital Consumer Assessment of Healthcare Providers and Systems survey), these suboptimal outcomes may have a direct effect on hospital reimbursements.6
Opioids are the current mainstay of postsurgical pain man-agement but have idiosyncratic or dose-limiting side effects that can be serious.7,8 The study by Gan and colleagues showed that 88% of postsurgical patients received analge-sic medication after surgery and that opioids were the most commonly administered.2 However, 80% of those patients reported AEs. Although the most common AEs were not severe (eg, drowsiness and constipation), serious AEs, such
as respiratory depression, also were noted.8 In 2012, the Joint Commission issued a Sentinel Event Alert regarding the use of opioids in the inpatient setting. This alert described several populations that were at particularly high risk for experienc-ing AEs in response to opioids, includexperienc-ing the elderly, patients with morbid obesity, and those with sleep apnea.9-11
One strategy to obviate the effect of opioid-related AEs is to employ a multimodal analgesic approach.12 Multimodal analgesia, the use of different classes of analgesics that act on different pathways and receptors, has gained increased acceptance and use over the past decade as a potential strategy for managing postsurgical pain while simultane-ously reducing the incidence of AEs related to any single analgesic agent.13-15 Several studies have reported that a multimodal approach that reduces opioid use may result in improved outcomes, increased patient satisfaction, and lower cost of care.6,14,16 These benefits have led both the American Society of Anesthesiologists and the Joint Com-mission to endorse the use of multimodal analgesia in post-surgical patients.4,9 0 20 40 60 80 100
Figure 1.
Percentage of patients reporting various postsurgical pain levels in 2 different studies.
Based on references 1 and 2.
Any Pain
Slight
Moderate
Severe
Extreme
Gan et al.
Apfelbaum et al.
86 82 45 47 23 21 8 18 25 13Pa
ti
e
n
ts
, %
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
Elastomeric Pumps and Continuous
Catheters
Perioperative and postsurgical regional anesthesia is anoth-er strategy that uses local anesthetics or othanoth-er agents in an effort to augment pain control while simultaneously avoiding the AEs associated with opioids.17-19 However, the duration of action of traditional local anesthetics, such as bupivacaine HCl, does not match the time course of postsurgical pain.1,20
In order to offer longer-lasting pain relief compared with that offered by traditional local anesthetics infiltrated into tis-sue that may or may not be associated with a nerve block, elastomeric pumps and catheters for continuous infusions of local anesthetics were introduced in the 1990s and are increasingly used in the inpatient postsurgical setting.21-23 The utility of these strategies is promoted by the fact that these analgesic routes can be continued even when the patient is discharged from the hospital. Continuation of these advanced analgesic strategies after hospital discharge more closely mir-rors the prolonged time course of postsurgical pain.
However, the use of an indwelling catheter for contin-uous delivery of local anesthetics has several defined dis-advantages (Table).21,24-32 Indwelling catheter use carries a risk for catheter-related complications, such as dislodgment, migration, infection, or bleeding.24-26 Additionally, continu-ous delivery using a pump and catheter incurs financial costs associated with the equipment and the resources needed to safely manage these systems both inside and outside the hospital setting.27
Concerns Raised by the FDA and ISMP
Both the Institute for Safe Medication Practices (ISMP) and the FDA have raised concerns about the safety of elastomeric pumps in clinical practice.28,29 In May 2009, the ISMP published a report noting an association between the ON-Q® system and cartilage destruction, especially in cases in which local anes-thetic is infused into a joint rather than the surrounding tissue.28 Similarly, the FDA recommended that elastomeric infusion devic-es not be used for continuous intra-articular infusion in patients after orthopedic surgery due to the risk for chondrolysis.29
Table.
Drawbacks, Limitations, and Safety Issues Associated With Use of Elastomeric Pumps
and Indwelling Catheters for Postoperative Analgesia
Elastomeric pumps
Variable infusion rates and concentrations
Administration of additional medications instead of analgesic alone
Extended use and refilling may result in infection
Premature emptying of the bulb
Not suitable for outpatient use for individuals with suboptimal health literacy or who live alone
Costs associated with the equipment and the resources needed to safely manage these systems
Indwelling catheters Catheter dislodgment
Catheter migration
Infection and/or bleeding
Potential for cartilage destruction, especially in cases in which local anesthetic is infused into a joint rather than the surrounding tissue
Based on references 21 and 24-32.
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
In July 2009, the ISMP followed up with a report calling for safer practices with the use of ON-Q elastomeric pumps.28 In this report, the ISMP noted several other issues regard-ing the use of these pumps, includregard-ing variable infusion rates and concentrations, administration of medication including the vasoconstrictor epinephrine instead of analgesic alone, and extended use and refilling that may result in infection.28
The ISMP warned that elastomeric pump devices are filled outside of the pharmacy, typically in the operating room (OR), which raises concerns regarding accurate filling, labeling, and documentation of the administered medication.28
Clinical Experience
In a review of experience at a major regional level 1 trau-ma center, Birrer and colleagues experienced firsthand trau-many of the issues outlined in the ISMP alert.21 The investigators reported that the hospital’s pharmacy and therapeutics com-mittee did not review the use of the ON-Q system because the pumps used a medication already on the formulary
(bupivacaine). Therefore, there was a lack of training or edu-cation in use of the device, leading to a lack of involvement from the pharmacy team and increased human error by the OR staff. As a result, there were several serious incidents. In one incident, a physician inserted 2 pumps with 4 lumens into a patient with traumatic brain injury and rib fractures. In another incident, the pump’s infusion rate was unpredictable, leading to the clearing of the pump’s bulb in 36 hours, despite the fact that it was expected to last 72 hours.21
In a small pilot study evaluating the use of the Homepump Eclipse for the management of acute and chronic pain,30 investigators reported several safety incidents when using the pumps, including premature emptying of the bulb and variations in drug delivery times. They also highlighted the importance of patient selection when choosing an elasto-meric pump, noting that patients with suboptimal health lit-eracy or those who live alone are not good candidates for this strategy.30
Capdevila and colleagues studied the use of continuous
Figure 2.
Elastomeric pumps are associated with a significant incidence of out-of-target flow rates.
The gray area represents the theoretical normal range (±15%) of the set flow rate (5 mL/h).
Based on Remerand F, et al. Elastomeric pump reliability in postoperative regional anesthesia: a survey of 430 consecutive devices.
Anesth Analg. 2008;107(6):2079-2084. Reprinted with permission.
E
x
p
e
c
te
d
F
low R
a
te
, %
-90 -60 -30 0 30 60 900 100 200
300
400
Number of Elastomeric Pumps
Sept.
Nov.
Jan.
Mar.
May
Easypump (n=300) Infusor LV5 (n=130)
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
peripheral nerve block to manage pain in 1,416 patients after orthopedic surgery.24 They reported that this strategy was associated with a significant risk for AEs, most of which were related to the catheter and its associated devices (eg, kinked catheter, inadvertent withdrawal of the catheter, and unde-sired stoppage of the pump). Bacterial colonization of the catheters also was a common occurrence.24
Grant and colleagues also reviewed their experience with 32 elastomeric pumps.31 After excluding data from 1 pump due to a leak, the investigators reported a pattern of over infu-sion in 7 of the pumps in the first hour after refilling. Further-more, they reported that pump infusion flow-rate accuracy was variable over time.31
In a study of 430 pumps, Remerand and colleagues found a variety of issues with both the pumps and the catheters (Figure 2).33 For example, 20.5% of pumps did not deflate correctly, and 2 catheters were obstructed. Spontaneous deflation occurred in 40 cases at 6 to 43 hours after connec-tion. These dysfunctions were associated with a decrease in analgesic efficacy during the first postsurgical night, lead-ing to many catheters belead-ing removed by the anesthesiologist after 11 to 72 hours.33
EXPAREL—A Long-Acting Single-Dose
Formulation of Bupivacaine
The bupivacaine in EXPAREL® (bupivacaine liposome
inject-able suspension) is encapsulated within multivesicular lipo-somes (DepoFoam®) that slowly break down and release the agent over a longer period of time than with a convention-al bupivacaine formulation, thereby producing longer-lasting analgesia without the need for a continuous catheter.34,35 Due to the DepoFoam carrier matrix, there is only minimal uptake of bupivacaine into the lymphatics and systemic circulation after injection, reducing systemic exposure and toxicity.34 In several studies, administration of EXPAREL led to prolonged concen-trations of bupivacaine through 72 hours with plasma levels detectable up to 96 hours, which more closely matches the time course of postsurgical pain.20,36
EXPAREL has demonstrated safety and efficacy in 2 pivotal Phase III trials of patients undergoing bunionectomy or hem-orrhoidectomy.37,38 In both cases, EXPAREL was delivered via wound infiltration at the conclusion of the surgical procedure. Results showed that patient satisfaction and pain scores were significantly better for EXPAREL than for placebo at the primary end point (72 hours for hemorrhoidectomy, 24 hours for bunionectomy), and the opioid requirements were reduced when compared with placebo.37,38
In another study, pooled safety data were generated from an analysis of 10 randomized, double-blind studies including 823 patients who received EXPAREL at the surgical site.39 The most common AEs in the EXPAREL arms were nausea, constipation, and vomiting.39 Serious AEs were reported in 2.7% of patients receiving EXPAREL, and in 5.4% and 1.1% of patients who received bupivacaine HCl and placebo, respec-tively. Additionally, 6.4% of patients experienced a cardiac
AE consisting of either tachycardia or bradycardia; howev-er, the cardiac events were mild or moderate in severity, and none required therapeutic intervention.39
Studies of EXPAREL suggest that it does not adversely affect wound healing. For example, in a review of all 10 Phase II and III studies of the efficacy and tolerability of EXPAREL when admin-istered into the surgical site, investigators found that EXPAREL did not adversely affect wound or bone healing for up to 2 years in some patients. There were also no reported instances of chondrolysis, although the number needed to detect this is quite large.40 Additionally, the investigators reported that infec-tions occurred in 5% of patients administered bupivacaine HCL, 3% of patients administered EXPAREL, and 2% of patients administered placebo.40 These are all critical factors to consid-er when choosing the optimal postsurgical analgesic regimen.
Based on these and other studies, the FDA approved the use of EXPAREL in October 2011 for single-dose infiltration into the surgical site to produce postsurgical analgesia.41 EXPAREL is supplied in a ready-to-use aqueous suspension.42 The vol-ume can be expanded with up to 280 mL preservative-free nor-mal sterile saline as necessary to accommodate administration into a larger surgical site, allowing for a single maximum dose containing 20 mL of EXPAREL without the need for a cathe-ter or pump.43
A Review of the Recent Literature
Several studies in 2013 and 2014 reported more recent experience with EXPAREL since its approval for clinical use. For example, Hollander and colleagues compared the effica-cy of EXPAREL (diluted with 40 mL normal saline and inject-ed subfascially before closure of the fascia) versus subfascial continuous local anesthesia (SFCLA; subfascial tunneled catheters and a ropivacaine pump) and patient-controlled analgesia (PCA; morphine) in 195 patients undergoing lap-aroendoscopic single-site donor nephrectomy.32 Patients managed with PCA required more supplemental narcot-ics than those on EXPAREL (63.3 vs 29.4 mg; P<0.01) or SFCLA (vs 32.9 mg; P<0.01), but narcotic use was similar between patients treated with EXPAREL and those receiv-ing SFCLA. Pain control (as demonstrated by maximal pain score according to the visual analog scale [VAS]) was com-parable between patients receiving EXPAREL and SFCLA (6.3 vs 6.2). Operating time was longer for SFCLA compared with EXPAREL (219.8 vs 199.3 minutes; P<0.01) and PCA (vs 202 minutes; P<0.01). Based on these data, the investigators concluded that EXPAREL was as effective as SFCLA for peri-operative analgesia and also was associated with decreased costs and operative time, likely due to its comparative ease of administration.32
Emerson and colleagues compared continuous femoral nerve block (FNB) to wound infiltration with EXPAREL as part of a multimodal pain program in 72 patients undergoing total knee replacement.44 On average, patients receiving EXPAREL required significantly lower amounts of opioid medication dur-ing their inpatient stay than those treated with an FNB (hydro-codone equivalent doses: 82.2 vs 176.6 mg; P<0.001), and
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
requested fewer narcotic doses (7.5 vs 14.3; Figure 3).44 There was a trend (P= 0.09) toward lower inpatient VAS pain scores with EXPAREL compared with FNB (1.8 vs 2.3; P= 0.09). In the EXPAREL group, investigators found no incidence of quadri-ceps weakness, a common drawback to administering tradi-tional local anesthetics via continuous FNB. The investigators concluded that wound infiltration with EXPAREL yielded equiv-alent postsurgical analgesia compared with a continuous FNB and with significantly less narcotic medication. As a result, they suggested that use of EXPAREL would replace the traditional opioid-reliant model of postsurgical analgesia.44
In another study, Richard and colleagues compared EXPAREL to the ON-Q system in controlling pain at the extraction and stapler insertion sites in patients undergoing
laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass (RYGB).45 Patients in the EXPAREL group used significantly less narcotics (hydrocodone/acetaminophen) in the immediate postsurgical period than patients in the ON-Q group (<10 vs 30 mg; P= 0.001).45
Additionally, in a single-institution, single-surgeon, retro-spective study of 108 patients undergoing robotic-assisted laparoscopic urologic surgeries, Walker and colleagues com-pared the efficacy of 0.5% ropivacaine delivered via an ON-Q pump (through 2 catheters placed under the fascia at the wound sites at the end of the surgery) versus wound infil-tration with EXPAREL (injected subcutaneously into the inci-sion sites and circumferentially along the trocars above and below the fascia down to the peritoneum).46 The investigators
0 50 100 150 200
EXPAREL FNB
176.6
82.2
P
<0.001
Figure 3.
Patients receiving EXPAREL
required significantly lower amounts of
opioid medication during their inpatient
stay than those treated with an FNB
(hydrocodone equivalent doses: 82.2 vs
176.6 mg;
P
<0.001).
FNB, femoral nerve block Based on reference 44.
A
v
e
ra
g
e N
a
rc
o
ti
c
s U
s
e
d
, m
g
0 50 100 150 200EXPAREL ON-Q
186.0
Figure 4.
Comparison of the efficacy of
wound infiltration with EXPAREL versus
0.5% ropivacaine delivered via the ON-Q
system following robotic-assisted
laparo-scopic urologic surgery.
Based on reference 46.
M
e
a
n T
im
e t
o F
ir
s
t O
p
io
id U
s
e, m
in
63.9
P
=0.0043
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
reported that the mean morphine equivalent dose was less in the EXPAREL group than in the ON-Q group (23.8 vs 65.9;
P<0.0001). Furthermore, the mean time to first opioid use was delayed in favor of EXPAREL (186.0 vs 63.9 minutes;
P= 0.0043; Figure 4).46 Of particular note, 5 patients in the EXPAREL group and 1 in the ON-Q group did not require any supplemental opioids. Based on these data, the investigators concluded that the use of EXPAREL was an effective strate-gy for postsurgical analgesia in patients undergoing minimally invasive surgery and was associated with a significant reduc-tion in narcotic use.46
Conclusion
Postsurgical pain is common and is associated with worse patient outcomes and higher health care costs. Although the use of local anesthetics as part of a multimodal analgesic approach can reduce opioid use and its associated AEs, the use of elastomeric pumps and continuous catheters needed to
match the protracted time course of postsurgical pain is asso-ciated with a variety of potential complications for the patient and can be generally inconvenient and costly to clinicians and institutions. Furthermore, some patients may not be sufficiently health care literate to manage these devices on their own after being discharged, and the devices may require valuable time in the office to be removed if the patient prefers not to do so.
The duration of action of EXPAREL more closely matches the time course of postsurgical pain through a single adminis-tration. Multiple trials, both clinical and “real world,” have dem-onstrated that wound infiltration with EXPAREL is effective at reducing pain for up to 72 hours after surgery while simulta-neously reducing opioid requirements. Furthermore, EXPAREL administered via wound infiltration obviates the need for elas-tomeric pumps and continuous catheters and their associat-ed complications and limitations. As a result, EXPAREL is well suited for use as a part of the multimodal analgesic approach across a wide range of patients and procedures.
Case Study 1
A 66-year-old woman presented for open total abdominal hysterectomy, bilateral
salpingo-oophorectomy, periaortic lymphadectomy, and omentectomy for ovarian cancer.
Jacob Hutchins, MD
T
he patient had a history of an abnormal right ovary with ele-vated CA-125. She had no other past medical history and this was her first surgery. She declined to have an indwelling catheter to manage postsurgical pain because neither she nor her husband felt comfortable removing it at home. The deci-sion was made to provide postsurgical analgesia with bilater-al classic transversus abdominbilater-al plane (TAP) infiltration with EXPAREL. Before surgery, in the preoperative block area, the patient received bilateral ultrasound-guided TAP infiltration. She received 30 mL total volume per side (10 mL EXPAREL and 20 mL normal saline). She was then taken to the OR where she was induced with 100 mg propofol, 100 mcg fentanyl, 100 mg lidocaine, and 50 mg rocuronium. She received a total of 400 mcg of fentanyl intraoperatively and 1 mg hydromorphone for a procedure that lasted 264 minutes. Final pathology showed stage IIc adenocarcinoma of the right fallopian tube.The patient’s postoperative pain was well controlled, with her maximal pain score in the postanesthesia care unit (PACU) at 3 out of 10 on the NRS. While in the PACU, she received 50 mcg fentanyl and 1 mg hydromorphone IV. During her first 24 hours postoperatively, her maximal pain score was 3 out of 10 and she received 0.1 mg IV hydromorphone, 5 mg oxyco-done, 30 mg IV ketorolac, and 325 mg oral acetaminophen.
During the first postoperative 24 to 48 hours, her maximal pain score was 4 out of 10 and she used only 15 mg ketorolac IV and 1,200 mg ibuprofen. She denied nausea or vomiting during the entire postoperative period. She was discharged home with oral opioids and enoxaparin injections 40.15 hours after surgery. When contacted on postoperative day (POD) 2, she reported continued good pain control without the need for additional opioids and was satisfied with the method of pain management.
Commentary
Continuous TAP instillation with a pump and catheter pro-vides incisional pain coverage and can be continued once dis-charged, but may be contraindicated or not desired in certain patients. By using TAP infiltration with EXPAREL instead of a continuous catheter and pump, a similar duration of analgesia can be provided and all postoperative anticoagulation needs can be met. Additionally, those with limited mental ability or assistance can still receive up to 72 hours of incisional pain relief. This technique also eliminates the potential for accidental catheter removal. With the change to EXPAREL, we have been able to provide postoperative incisional pain control to a more diverse population of total abdominal hysterectomy patients.
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
Case Study 2
A 44-year-old man undergoing a skin graft following multiple surgeries.
Susan E. Downey, MD, FACS
T
he patient was previously healthy and had developed chest pain. His medical history was notable for hypertension but he was not on medication. Stress test confirmed an ascend-ing aortic aneurysm. He underwent elective ascendascend-ing aortic replacement with a femoral artery cut down and repair. Later that same day he began to complain of severe calf pain and was found to have a compartment syndrome in his left calf. He was taken back emergently to the OR and underwent fas-ciotomies of the calf. A week later, he developed shortness of breath and was found to have a pericardial effusion. This required another return to the OR and subxiphoid drainage. Two weeks later, a plastic surgery consultation was obtained for a skin graft for the fasciotomy wounds on his calf.The nursing staff and the rest of his medical team were con-cerned about his postoperative pain management because he had been on narcotics in the ICU for several weeks. Due to his many complications and surgical procedures in such a short peri-od of time, the patient was having pain control issues. The Pallia-tive Care Department had been consulted and was following him with the diagnosis of “intractable pain.” He was maintained on a hydromorphone PCA 0.9 mg per hour continuous drip with 0.3 mg every 10 minutes as needed and a 3-mg per hour lockout.
The patient was taken to the OR and a split-thickness skin graft was harvested from his upper thigh using a dermatome.
The dermatome was set at 18/100,000 of an inch. EXPAREL 20 mL with 40 mL saline (total volume 60 mL) was injected into the donor site. The donor site was dressed with xeroform and a bulky dressing. The skin graft was secured to the recipient site with staples and Adaptic gauze. No local anesthetic was injected into the recipient site.
Immediately after the skin graft procedure, the PCA was stopped and the patient was switched to hydromorphone IV push 0.5 mg every 3 hours as needed for pain. Oxycodone/ acetaminophen was administered for breakthrough pain. He was discharged home 2 days after the skin graft procedure on oral oxycodone/acetaminophen alone.
Commentary
When harvesting skin grafts, the donor site can be as painful as a second-degree burn. It can take days or even weeks for the pain to subside, and an injection of marcaine or lidocaine only lasts a few hours. A pain pump cannot be used because the harvesting of the skin graft does not leave a cavity for a catheter. The patient was informed that EXPAREL would be used in the donor site before surgery to minimize his postoperative pain. After surgery, the patient was found to be resting comfortably and reported no pain in the donor site.
Case Studies 3 and 4
53- and 46-year-old women undergoing Roux-en-Y gastric bypass.
John Pilcher, MD, FACS, FASMBS
The 53-Year-Old Woman: Using an ON-Q Pump and Catheter
T
he patient suffered from many years of weight gain despite regular diet and exercise. Her medical prob-lems included hypertension, hyperlipidemia, asthma, chronic low back pain, and knee pain. She had previously undergone laparoscopic cholecystectomy and total abdominal hysterec-tomy. She also had a history of atrial fibrillation and spontane-ous deep vein thrombosis 4 years before her initial encounter with the bariatric surgical team. She took ibuprofen regularly for moderate knee and back pain, but was not taking any nar-cotic pain medication before surgery. Her height was 163 cm and her weight was 113 kg, with a body mass index (BMI) of 43 kg/m2. Medications before surgery included lisinopril,metoprolol, spironolactone, atorvastatin, and cetirizine. The bariatric surgical team recommended RYGB to treat the patient’s progressive metabolic obesity disease. The surgery was performed laparoscopically, without any unusual events. The gastrojejunal anastomosis was accomplished using a size 25 circular stapler, which was introduced into the abdomen by removing the left flank trocar and dilating the site to accom-modate the device. At the end of the procedure, the fascia and muscle at the site that had been dilated were closed using a single vicryl suture. The other trocars (all nonbladed) were sim-ply removed and no fascial closure was deemed necessary. No drains were deemed necessary.
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
Bupivacaine 0.5% plus epinephrine was infiltrated preemp-tively at each trocar site after the abdomen was prepped and draped, and an additional 20 mL was infiltrated at the end of the procedure into the left flank fascia where the suture closure was accomplished. An ON-Q catheter was threaded into the pre-peritoneal plane on the left flank, lateral to the site of the suture closure. The 48-hour elastomeric ON-Q pump was charged with a 120-mL volume of bupivacaine 0.25%, which infused gradually through the catheter during the 2-day hospital stay.
The patient received the standard postoperative pain and nausea regimen, which included 2 mg PCA morphine in 10-minute intervals with 30/4-hour lockout; 15 to 30 mL of hydrocodone/acetaminophen elixir (7.5/500 mg per 15 mL) orally every 4 hours as needed for pain; 4 doses of 30 mg IV ketorolac every 8 hours beginning at 4 hours postsurgery; 4 doses of 4 mg IV ondansetron every 6 hours (standing), then 8 mg IV every 6 hours as needed for nausea; and 10 mg of IV metoclopramide every 6 hours as needed for nausea, if ondan-setron was not effective.
The postoperative stay was unremarkable, and the patient was discharged home on POD 2. During her hospital stay she received 26 mg morphine via PCA, 120 mL hydrocodo-ne/acetaminophen elixir; ketorolac as scheduled; ondansetron as scheduled followed by 2 additional doses of ondansetron as needed; 20 mg of metoclopramide (2 doses as needed as backup for ondansetron); and bupivacaine via ON-Q catheter, with catheter removal just before discharge.
At time of discharge, the patient received a standard pre-scription for additional hydrocodone/acetaminophen elixir. At her first follow-up visit, the patient reported that she took the as-needed prescription “very regularly” for the first few days at home, obtained the permitted refill (each fill = 1 pint), then used “about one-fourth” of the second pint. Approximately 1 week post-discharge the patient experienced very severe constipa-tion, requiring 2 enemas and self-disimpaction.
In long-term follow-up, the patient had experienced substan-tial weight loss and health improvement. There was no long-term pain, nausea, or constipation sequelae.
The 46-Year-Old Woman: Using EXPAREL
T
he patient presented to the bariatric clinic for consideration of bariatric surgical intervention. Her height was 170 cm and her weight was 129 kg, with a BMI of 45 kg/m2. Her med-ical history included gastroesophageal reflux disease, hyper-tension, obstructive sleep apnea, and depression. She also had longstanding chronic back and knee pain, for which she took approximately 15 mg hydrocodone per day as-needed. Other medications included lisinopril, duloxetine, and zolpidem. She had previously undergone right total knee replacement, and lumbar laminectomy.RYGB was selected in this case as well. The operation was accomplished laparoscopically according to routine. In the same manner as the previous case, the gastrojejunal anas-tomosis was accomplished using a size 25 circular stapler with dilation of the skin and muscle at the left flank trocar site. The fascia at this location was closed using a single vic-ryl suture, and suture closure of the other trocar sites was deemed unnecessary. No drain was deemed necessary.
A 20 mL dose of EXPAREL was combined with 100 mL sterile normal saline. Approximately 60 mL was infiltrated preemptively at the skin level and the fascia level at each trocar placement site at the beginning of the case. When the procedure was complete, 30 mL was infiltrated into the left flank fascia at the site of suture closure, and 30 mL was
infiltrated into the left TAP lateral to this fascial site. Following surgery, this patient received an updated postoper-ative pain and nausea regimen, which included 2 to 4 mg mor-phine every 2 hours as needed for pain (not PCA); 15 to 30 mL of hydrocodone/acetaminophen elixir (7.5/500 mg per 15 mL) orally every 4 hours as needed for pain; 4 doses 30 mg of IV ketorolac every 8 hours beginning at 4 hours postoperatively; 4 doses of 4 mg IV ondansetron every 6 hours (standing) fol-lowed by 8 mg IV every 6 hours as needed for nausea; and 10 mg of IV metoclopramide every 6 hours for nausea, if ondanse-tron was not effective.
The postoperative stay was unremarkable, and the patient was discharged home on POD 1. During her hospital stay she received 8 mg morphine; 75 mL hydrocodone/acetaminophen elixir; ketorolac as scheduled; ondansetron as scheduled, no as-needed doses required; and metoclopramide was available but not required.
At time of discharge, the patient received a standard prescrip-tion for addiprescrip-tional hydrocodone/acetaminophen elixir. At her first follow-up visit she reported that she took the as-needed medi-cation only twice, and was pleasantly surprised at how little pain she experienced. In long-term follow-up, the patient had expe-rienced substantial weight loss and health improvement. There was no long-term pain, nausea, or constipation sequelae.
Commentary
Although these are 2 different patients, they under-went similar procedures. However, when EXPAREL was
administered, less narcotics were used, resulting in fewer postsurgical side effects.
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
A Pharmacist’s Clinical Perspective
Andrew Rogalski, PharmD, BCPS
O
ur institution began using EXPAREL in 2012, and it is now used in general, orthopedic, and gynecologic procedures by multiple practitioners. We have seen a number of advantages throughout the institution since making it a part of our multimodal pain control strategy.In discussions with providers, caregivers, and patients there has been a nearly universal description of reduction in requirements for rescue narcotics in the postoperative peri-od, with consistent results into POD 3. Our nurses have even reported narcotic-free PACU discharges for several same-day procedures.
Operationally, we had been using considerable numbers of elastomeric infusers and CADD infusers for regional anesthe-sia and nerve blocks. Many of our surgeons have abandoned these modalities and adopted EXPAREL for its superior sim-plicity with excellent results.
When accounting for costs, we found that the acquisition costs for the infusion devices and standard anesthetics were
initially slightly less than EXPAREL, but when the cost of the catheters, tubing, and preparation time were tabulated, the costs were essentially equivalent. For example, preparation of infusers required a minimum of 12 hours of pharmacy technician resources each week, which have now virtually been eliminated.
We have elected to provide EXPAREL at room temper-ature in a centrally located automated dispensing cabinet (Pyxis) within the OR core. Because of frequency of use, we have encountered no issues with the limited beyond-use dat-ing when removed from refrigeration. Speculative concerns for look-alike issues with propofol have not been observed in our practice; however, as a precaution, our circulating nurses retrieve the EXPAREL and our anesthesiologists have no role in its administration. Our organization has seen many success-es with the adoption of EXPAREL as part of our multimodal approach to pain management. When drug, device, and oper-ational costs are considered in totality, we have found it to be at least cost-neutral to other regional anesthetic modalities.
Important Safety Information
EXPAREL is contraindicated in obstetrical paracervical block anesthesia. EXPAREL has not been studied for use in patients younger than 18 years of age.
Non–bupivacaine-based local anesthetics, including lidocaine, may cause an immediate release of bupivacaine from EXPAREL if administered together locally. The administration of EXPAREL may follow the administration of lidocaine after delay of 20 minutes or more. Other formulations of bupivacaine should not be administered within 96 hours following administration of EXPAREL.
Monitoring of cardiovascular and neurological status, as well as vital signs should be performed during and after injection of EXPAREL as with other local anesthetic products.
Because amide-type local anesthetics, such as bupivacaine, are metabolized by the liver, EXPAREL should be used cautiously in patients with hepatic disease. Patients with severe hepatic disease, because of their inability to metabolize local anesthetics normally, are at a greater risk of developing toxic plasma concentrations.
In clinical trials, the most common adverse reactions (incidence ≥10%) following EXPAREL administration were nausea, constipation, and vomiting.
Please see full Prescribing Information for EXPAREL.
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
References
1. Apfelbaum JL, Chen C, Mehta SS, et al. Postoperative pain experi-ence: results from a national survey suggest postoperative pain con-tinues to be undermanaged. Anesth Analg. 2003;97(2):534-540. 2. Gan TJ, Habib AS, Miller TE, et al. Incidence, patient satisfaction,
and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin. 2014;30(1):149-160.
3. Morrison RS, Magaziner J, McLaughlin MA, et al. The impact of post-operative pain on outcomes following hip fracture. Pain. 2003; 103(3):303-311.
4. Joshi GP, Ogunnaike BO. Consequences of inadequate postopera-tive pain relief and chronic persistent postoperapostopera-tive pain. Anesthesiol Clin North America. 2005;23(1):21-36.
5. American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management.
Anesthesiology. 2012;116(2):248-273.
6. Centers for Medicare & Medicaid Services (CMS). Hospital Con-sumer Assessment of Healthcare Providers and Systems. http:// www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/HospitalHCAHPS.html. Accessed August 4, 2014.
7. Oderda GM, Said Q, Evans RS, et al. Opioid-related adverse drug events in surgical hospitalizations: impact on costs and length of stay. Ann Pharmacother. 2007;41(3):400-406.
8. Wheeler M, Oderda GM, Ashburn MA, et al. Adverse events associ-ated with postoperative opioid analgesia: a systemic review. J Pain. 2002;3(3):159-180.
9. Joint Commission. Sentinel event alert: use of opioids in the inpa-tient setting. http://www.jointcommission.org/assets/1/18/SEA_49_ opioids_8_2_12_final.pdf. Accessed August 4, 2014.
10. Jarzyna D, Jungquist CR, Pasero C, et al. American Society for Pain Management Nursing guidelines on monitoring for opioid-induced sedation and respiratory depression. Pain Manag Nurs. 2011;12(3):118-145.e10.
11. Dahan A, Aarts L, Smith TW. Incidence, reversal, and prevention of opioid-induced respiratory depression. Anesthesiology. 2010;112(1): 226-238.
12. Kehlet H, Dahl JB. The value of “multimodal” or “balanced analge-sia” in postoperative pain treatment. Anesth Analg. 1993;77(5): 1048-1056.
13. Ritchey RM. Optimizing postoperative pain management. Cleve Clin J Med. 2006;73(suppl 1):S72-S76.
14. Joshi GP. Multimodal analgesia techniques and postoperative reha-bilitation. Anesthesiol Clin North Am. 2005;23(1):185-202. 15. Jin F, Chung F. Multimodal analgesia for postoperative pain control.
J Clin Anesth. 2001;13(7):524-539.
16. Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002;183(6):630-641.
17. White PF. The changing role of non-opioid analgesic techniques in the management of postoperative pain. Anesth Analg. 2005; 101(5 suppl):S5-S22.
18. White PF. The role of non-opioid analgesic techniques in the man-agement of pain after ambulatory surgery. Anesth Analg. 2002;94(3): 577-585.
19. Kvolik S, Kristek J, Sakic K, et al. A wound infiltration as a method of postoperative analgesia. Periodicum Biologorum. 2009;111(2):241-246.
20. Hu D, Onel E, Singla N, et al. Pharmacokinetic profile of liposome bupivacaine injection following a single administration at the surgical site. Clin Drug Investig. 2013;33(2):109-115.
21. Birrer KL, Anderson RL, Liu-DeRyke X, et al. Measures to improve safety of an elastomeric infusion system for pain management. Am J Health Syst Pharm. 2011;68(13):1251-1255.
22. Food and Drug Administration. 501(k) Premarket Notification. Painbuster Infusion System. 1999. https://www.accessdata.fda. gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K980558. Accessed August 4, 2014.
23. Food and Drug Administration. 501(k) Premarket Notification. Homepump (Disp. Elastomeric Infusion Device). 1990. https:// www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn. cfm?ID=K896546. Accessed August 4, 2014.
24. Capdevila X, Pirat P, Bringuier S, et al; French Study Group on Con-tinuous Peripheral Nerve Blocks. ConCon-tinuous peripheral nerve blocks in hospital wards after orthopedic surgery: a multicenter prospective analysis of the quality of postoperative analgesia and complications in 1,416 patients. Anesthesiology. 2005;103(5):1035-1045. 25. Holmström B, Rawal N, Axelsson K, et al. Risk of catheter migration
during combined spinal epidural block: percutaneous epiduroscopy study. Anesth Analg. 1995;80(4):747-753.
26. Marhofer D, Marhofer P, Triffterer L, et al. Dislocation rates of perineural catheters: a volunteer study. Br J Anaesth. 2013;111(5): 800-806.
27. Elvir-Lazo OL, White PF. The role of multimodal analgesia in pain management after ambulatory surgery. Curr Opin Anaesthesiol. 2010;23(6):697-703.
28. Institute for Safe Medication Practices (July Alert). Process for handling elastomeric pain relief balls (ON-Q Painbuster and others) requires safety improvements. https://www.ismp.org/newsletters/ acutecare/articles/20090716.asp. Accessed August 4, 2014. 29. Food and Drug Administration. Chondrolysis reported with
continu-ously infused local anesthetics (marketed as bupivacaine, chlorpro-caine, lidochlorpro-caine, mepivachlorpro-caine, prochlorpro-caine, and ropivacaine). http:// www.fda.gov/safety/medwatch/safetyinformation/safetyalertsforhu-manmedicalproducts/ucm190496.htm. Accessed August 4, 2014. 30. Ganapathy S, Amendola A, Lichfield R, et al. Elastomeric pumps
for ambulatory patient controlled regional analgesia. Can J Anaesth. 2000;47(9):897-902.
Copyright © 2014 McMahon Publishing Gr
oup unless otherwise noted.
All rights r
eserved. Repr
oduction in whole or in part without permission is pr
31. Grant CR, Fredrickson MJ. Regional anaesthesia elastomeric pump performance after a single use and subsequent refill: a laboratory study. Anaesthesia. 2009;64(7):770-775.
32. Hollander AB, Scovell JM, Mercado MA, et al. Perioperative injection of liposomal bupivacaine reduces narcotic medication requirement after laparo-endoscopic single site donor nephrectomy with shorter operating time than sub-fascial continuous local anesthesia. J Urol. 2014;191(suppl 4S):e828-e829.
33. Remerand F, Vuitton AS, Palud M, et al. Elastomeric pump reliability in postoperative regional anesthesia: a survey of 430 consecutive devices. Anesth Analg. 2008;107(6):2079-2084.
34. Howell SB. Clinical applications of a novel sustained-release inject-able drug delivery system: DepoFoam technology. Cancer J. 2001; 7(3):219-227.
35. Angst MS, Drover DR. Pharmacology of drugs formulated with DepoFoam: a sustained release drug delivery system for parenteral administration using multivesicular liposome technology. Clin Phar-macokinet. 2006;45(12):1153-1176.
36. White PF, Ardeleanu M, Schooley G, et al. Pharmacokinetics of depobupivacaine following infiltration in patients undergoing two types of surgery and in normal volunteers. Proceedings and Abstracts of the 2009 Annual Meeting of the. International Anes-thesia Research Society. March 14-17, 2009, San Diego, CA. 37. Golf M, Daniels SE, Onel E. A phase 3, randomized,
placebo-con-trolled trial of DepoFoam® bupivacaine (extended-release
bupiva-caine local analgesic) in bunionectomy. Adv Ther. 2011;28(9): 776-788.
38. Gorfine SR, Onel E, Patou G, et al. Bupivacaine extended-release liposome injection for prolonged postsurgical analgesia in patients undergoing hemorrhoidectomy: a multicenter, random-ized, double-blind, placebo-controlled trial. Dis Colon Rectum. 2011;54(12):1552-1559.
39. Viscusi ER, Sinatra R, Onel E, et al. The safety of liposome bupiva-caine, a novel local analgesic formulation. Clin J Pain. 2014; 30(2):102-110.
40. Baxter R, Bramlett K, Onel E, et al. Impact of local administration of liposome bupivacaine for postsurgical analgesia on wound healing: a review of data from 10 perspective, controlled clinical studies.
Clin Ther. 2013;35(3):312-320.
41. Pacira Pharmaceuticals, Inc. Announces US FDA Approval of EXPAREL for Postsurgical Pain Management [news release]. Parsippany, NJ. Oct 31, 2011. http://investor.pacira.com/phoenix. zhtml?c=220759&p=irol-newsArticle&ID=1913495&highlight=. Accessed August 4, 2014.
42. Pacira Pharmaceuticals, Inc. EXPAREL Website. About DepoFoam. http://www.exparel.com/how-to-use/about-depofoam.shtml. Accessed August 4, 2014.
43. Pacira Pharmaceuticals, Inc. EXPAREL Website. How to use. http://www.exparel.com/how-to-use.shtml. Accessed August 4, 2014.
44. Emerson RH, Barrington JW, Olugbode S. Comparison of a con-tinuous femoral nerve block to long-acting bupivacaine wound infiltration as part of a multi-modal pain program in total knee replacement. International Congress for Joint Reconstruction. http://icjr.net/log_in.htm?island=L3RhZ3MvdGFnNDA0Lmh0bQ==. Accessed August 4, 2014.
45. Richard F, Duperier T. Pain control in bariatric patients: a prospec-tive trial comparing the effecprospec-tiveness of Exparel to the On Q pain ball. Proceedings and Abstracts of 2013 Scientific Session of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), Baltimore, Maryland, April 17-20, 2013. Poster 423. 46. Walker PW, White MA, Morales EE, et al. Improving postoperative
pain following robotic-assisted and laparoscopic urologic surgeries: a comparison of liposome bupivacaine to ropivacaine delivered by the On-Q pain relief system. Proceedings and Abstracts of the 31st World Congress of Endourology, New Orleans, Louisiana, October 22-26, 2013. Abstract MP2B-24.
Disclosures: Dr. Downey reported that she has acted as a consultant for Allergan, Inc. and Ethicon, Inc. Dr. Hutchins reported that he has received research grants, honoraria, and has served as a consultant for Pacira Pharmaceuticals, Inc. He also reported that he has served on the speakers’ bureaus for I-Flow, LLC and Pacira Pharmaceuticals, Inc. Dr. Pilcher reported that he has served as a consultant for Ethicon, Inc., Intuitive Surgical, Inc., and Pacira Pharmaceu-ticals, Inc. Dr. Rogalski reported that he has received honoraria from the American Society of Health-Systems Pharmacists and Pacira PharmaceuPharmaceu-ticals, Inc. Disclaimer: This monograph is designed to be a summary of information. While it is detailed, it is not an exhaustive clinical review. McMahon Publishing, Pacira Pharmaceuticals, Inc., and the authors neither affirm nor deny the accuracy of the information contained herein. No liability will be assumed for the use of this monograph, and the absence of typographical errors is not guaranteed. Readers are strongly urged to consult any relevant primary literature. Copyright © 2014, McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of
reproduc-tion, in whole or in part, in any form. SR
1 4 2 3 P P -E X -US-0 2 4 2 Δ 6