The development, delivery and evaluation of a physical
activity maintenance intervention.
SCOTT, Sarah E.
Available from Sheffield Hallam University Research Archive (SHURA) at:
http://shura.shu.ac.uk/20806/
This document is the author deposited version. You are advised to consult the
publisher's version if you wish to cite from it.
Published version
SCOTT, Sarah E. (2014). The development, delivery and evaluation of a physical
activity maintenance intervention. Doctoral, Sheffield Hallam University (United
Kingdom)..
Copyright and re-use policy
- w v i
ate Crescent Campus
ProQuest Number: 10702910
All rights reserved
INFORMATION TO ALL USERS
The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a com plete manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uest
ProQuest 10702910
Published by ProQuest LLC(2017). Copyright of the Dissertation is held by the Author.
All rights reserved.
This work is protected against unauthorized copying under Title 17, United States C ode Microform Edition © ProQuest LLC.
ProQuest LLC.
789 East Eisenhower Parkway P.O. Box 1346
THE DEVELOPMENT, DELIVERY AND EVALUATION OF A PHYSICAL ACTIVITY MAINTENANCE INTERVENTION
Sarah E. Scott
A thesis submitted in partial fulfilment of the requirements of Sheffield Hallam University for the degree of Doctor of Philosophy
Abstract
The number of adults living with chronic health conditions and co-morbidities (e.g., diabetes and depression) is expected to rise by 2035 resulting in significant health and social care challenges (Department of Health, 2012). Supporting people with long-term conditions into better physical and mental health is a public health priority (NICE, 2009). One common approach used to manage or prevent a range of chronic health conditions is physical activity (PA). Evidence supports the short-term effects of PA interventions but a decline in PA levels occurs after an intervention ends (Foster, et al., 2012). Considering the lack of long-term effectiveness of interventions, this thesis explored the active ingredients of PA maintenance (e.g., determinants and behaviour change techniques [BCTs]) through the development, delivery and evaluation of a theory-based PA maintenance intervention. The intervention was developed using intervention mapping principles (Bartholomew, Parcel, Kok, & Gottlieb, 2006).
A scoping review explored the intervention components, theories, determinants and BCTs for PA maintenance across at least six months in clinical populations. Multiple theories, determinants and BCTs were found meaning the important components for intervention development were inconclusive. Research gaps were identified, which was addressed through a qualitative study (Study 1). Study 1 investigated the determinants and strategies for successful and unsuccessful maintenance in completers of physical activity referral schemes (PARS). Determinants included: congruence between outcome expectations, experiences and values; social support; and, overcoming barriers. Multiple cognitive-behavioural strategies for PA, condition management and coping were identified, including self-monitoring and pacing. Recommendations included interventions to adopt a person-centred integrative approach, such as motivational interviewing (Miller & Rollnick, 2013) and cognitive-behavioural techniques (MI-CB; Naar-King et al., 2013; Hogden et al., 2012).
Candidate’s Statement
I declare that the work in this thesis was carried out in accordance with the regulations of the Sheffield Hallam University and is original except where indicated by the specific reference in the text. No part of the thesis has been submitted as part of any other academic award. The thesis has not been presented to any other education institution in the United Kingdom or overseas.
Any views expressed in the thesis are those of the author and in no way represent those of the University.
Acknowledgements
Without the support of a number of people, this thesis and PhD process would not have been possible and I would like to express my gratitude here. Firstly, I would like to thank my PhD supervisors, Jeff Breckon and Rob Copeland, whose expertise and vast knowledge and skills have helped me develop as a researcher. I would also like to thank you both for your empathic encouragement and persistent patience during the academic writing and publication process, without which I would not have achieved my goals. I would also like to thank Andrew Hutchison for his expert guidance in qualitative research. I am truly grateful for his continual input during the publication process and conference presentations despite the fact that he left to pursue a doctorate in clinical psychology during my first year. Additionally, there are a number of excellent academics that I would like to thank for the valuable time they have given to listen to me work through my ideas or offer practical suggestions with regards to intervention development, quality assurance, and physical activity measurement, including: Maddy Arden, Helen Crank, Garry Tew and David Broom. I am also truly grateful for the fundamental role that David Birds, Mark Goodhead and Kevan Riggett (the physical activity referral scheme co-ordinators) played during study recruitment and the intervention implementation phase. I would also like to thank all the participants for the time they invested in this research and for their stories and tears shared. Without you all, this thesis would not have been possible.
Published Material from this Thesis Publications:
Scott, S.E., Breckon, J. D., Hutchison, A., & Copeland, R. J. (in press). Determinants and strategies for physical activity maintenance in chronic health conditions: A qualitative study. Journal o f Physical Activity & Health.
Conference Presentations:
Scott, S. E., Breckon, J. D., & Copeland, R. J. (2014). An Integrated Motivational-
Interviewing and Cognitive-Behavioural Intervention for Physical Activity Maintenance: A Pilot Study. International Conference on Motivational Interviewing 4th Annual Conference. Amsterdam, Netherlands, 16th-18th June.
Scott, S.E., Breckon, J. D., Hutchison, A., & Copeland, R. J. (2013). Determinants and
strategies for physical activity maintenance in chronic health conditions. Midlands Health Psychology Network 9th Annual conference. Birmingham University, 14th February.
Scott, S.E., Breckon, J. D., Hutchison, A., & Copeland, R. J. (2012). Determinants and
Contents
Abstract... I Candidate’s Statement...II Acknowledgements...Ill Published material from this Thesis... IV Contents...V List of Tables...VIII List of Figures...X Abbreviations...XI
Chapter 1: Thesis Introduction and Background: Physical Activity Maintenance. 1
1.1 Introduction...2
1.2 Purpose of Thesis...8
1.3 Thesis Structure... 9
1.4 Content of this Thesis... 10
Chapter 2: Promoting Physical Activity Maintenance for Adults with Chronic Health Conditions: A Scoping Review of the Literature...14
2.1 Introduction...15
2.2 Review Aims and Research Questions... 22
2.3 Methods...22
2.4 Results... 25
2.5 Discussion...50
2.6 Limitations...58
2.7 Chapter Summary...59
Chapter 3: Study 1: Determinants and Strategies for Physical Activity Maintenance in Chronic Health Conditions: A Qualitative Study...60
3.1 Introduction...61
3.2 Background: Determinants and Strategies...61
3.3 Study Aims...65
3.4 Methods... 65
3.5 Results... 69
3.6 Discussion...79
3.7 Limitations...85
3.8 Chapter Summary...95
Chapter 4: Development of an Integrated Motivational Interviewing and Cognitive Behavioural (MI-CB) Intervention for Physical Activity Maintenance: An Intervention Mapping Approach...88
4.1 Introduction...89
4.2 Background to Intervention Development...90
4.4 Methods...93
4.5 Results...96
4.6 Discussion...119
4.7 Limitations... 122
4.8 Chapter Summary...123
C hapter 5: Study 2(a): Efficacy and Feasibility of an Integrated M otivational Interviewing and Cognitive-behavioural Intervention for Physical Activity M aintenance: A pilot random ised controlled tria l... 125
5.1 Introduction... 126
5.2 Background... 127
5.3 Study Aims...132
5.4 Hypotheses...132
5.5 M ethod... 133
5.6 Results... 143
5.7 Discussion...161
5.8 Limitations...173
5.9 Chapter Summary...175
C hapter 6: Study 2(b): Treatm ent Fidelity of an Integrated M otivational Interviewing and Cognitive Behavioural Intervention for Physical Activity M aintenance...177
6.1 Introduction... 178
6.2 Background: Treatment Fidelity... 179
6.3 Study Aims...187
6.4 Research Questions... 187
6.5 M ethod... 188
6.6 Results... 197
6.7 Discussion... 209
6.8 Limitations... 219
6.9 Chapter Summary... 220
C hapter 7: Thesis Synthesis, Recommendations, Reflections and Conclusions.... 222
7.1 Introduction... 223
7.2 The Theories, Determinants and Strategies for Physical Activity Maintenance .... 223
7.3 Synthesis of Findings from Chapter 5 (Study 2a): The MI-CB Intervention 227 7.4 Synthesis of Findings from Chapter 6 (Study 2b): Treatment Fidelity...230
7.5 Implications for Practice and Research... 232
7.6 Limitations of this Thesis... 237
7.7 Reflexive Practice... 238
7.8 Thesis Conclusions...240
Appendix A: Institutional Ethics Approval (Study I ) ...288
Appendix B: Participant Information Sheet (Study 1)...290
Appendix C: Background Information Sheet (Study 1)... 294
Appendix D: Consent Form (Study 1)... 296
Appendix E: Interview Guide (Study 1 ) ...299
Appendix F: Example Transcript (Study 1)... 302
Appendix G: Example Process Map from Study 1 ... 327
Appendix H: Full Matrices of Change Objectives for the MI-CB Intervention... 329
Appendix I: Materials for the MI-CB Intervention... 341
Appendix J: Ethics Approval (Study 2a & Study 2b)...349
Appendix K: Participant Information Sheet (Study2a &2b)...351
Appendix L: Risk Assessments (Study 1, 2a & 2b)... 355
Appendix M: Cognitive-behavioural Technique Delivery Checklist... 360
Appendix M: Additional Treatment Fidelity Questionnaires...363
Table 2.1
Table 2.2 Table 2.3 Table 2.4 Table 2.5.
Table 2.6
Table 2.7
Table 3.1
Table 4.1
Table 4.2
Table 4.3 Table 4.4 Table 4.5
Table 4.6
Table 5.1 Table 5.2
Table 5.3
Table 5.4
List of Tables
Bibliography of Included Articles in the Scoping Review...26
Sample Characteristics of Scoping Review...31
Intervention Characteristics in Scoping Review...35
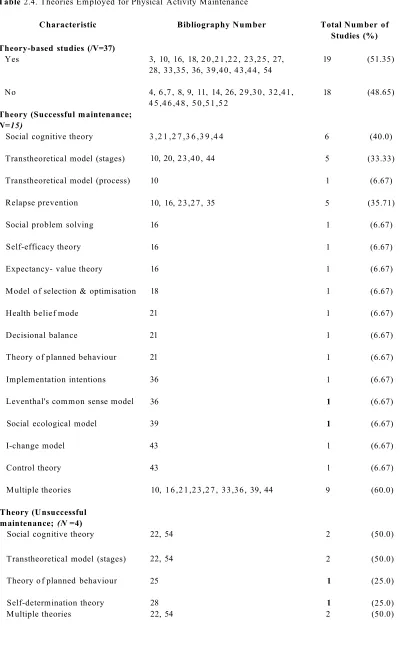
Theories Employed for Physical Activity Maintenance...40
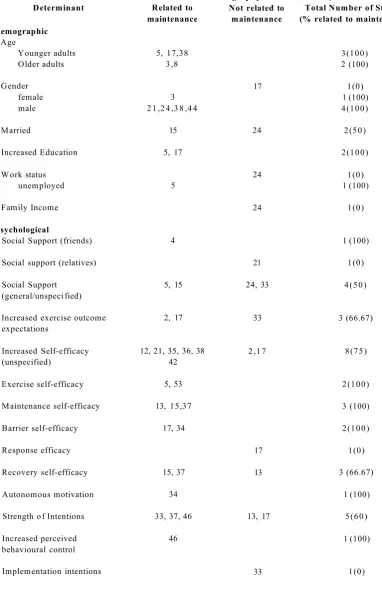
Determinants for Physical Activity Maintenance...43
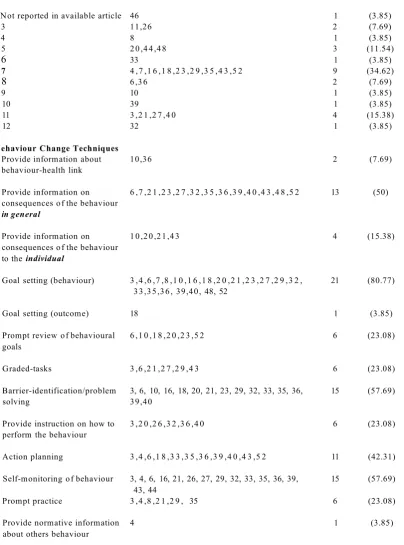
The Behaviour Change Techniques Associated with Physical Activity Maintenance...47
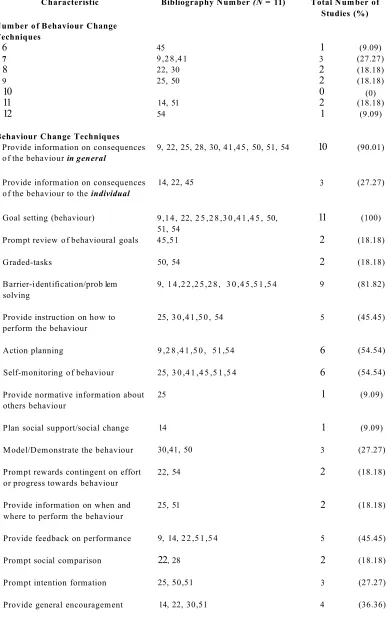
The Behaviour Change Techniques Employed in Ineffective Interventions...49
Thematic Framework of Determinants, Barriers, and Strategies for Successful (SM) and Unsuccessful (UM) Physical Activity Maintainers...70
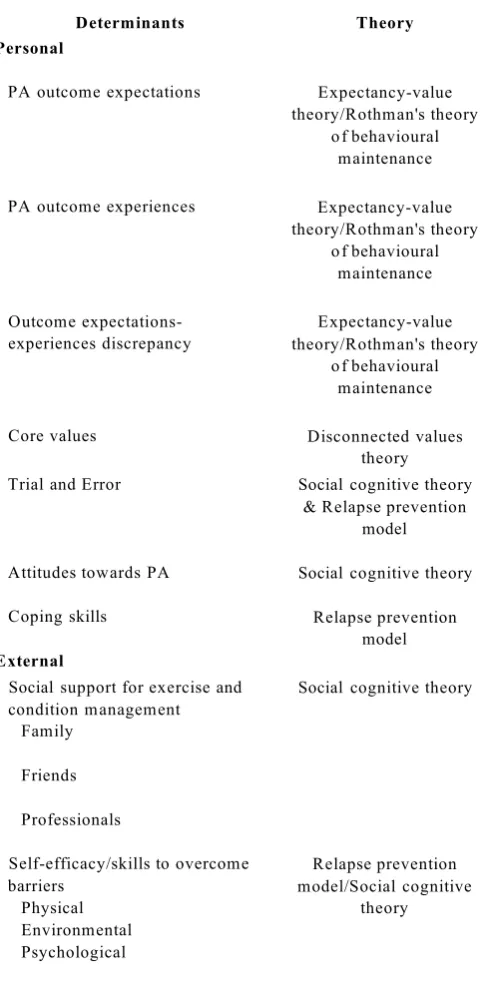
Evidence of Importance and Theory of the Personal and External Physical Activity Maintenance Determinants...98
Performance Objectives for Maintaining Physical Activity ...100
Example of the Matrices of Change Objectives...101
Cognitive-behavioural Techniques in MI-CB Intervention...103
Parameters of Use for MI-CB Integration and Performance Objectives...110
MI-CB Intervention Session Content, Aims, and Example Cognitive-behavioural Techniques...115
Theory-derived Determinants Used in The MI-CB Intervention...136
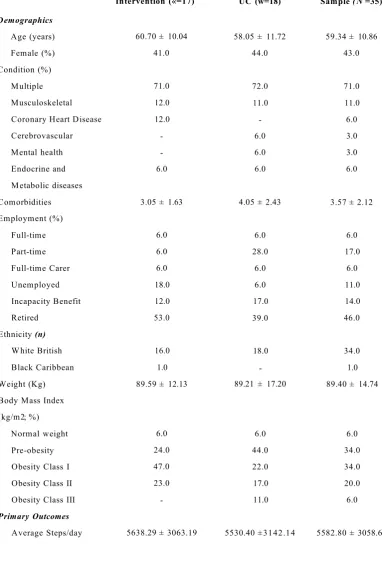
Means, Standard Deviations, and % of Baseline Characteristics for Total Sample and Treatment Groups for the KASY Trial...144
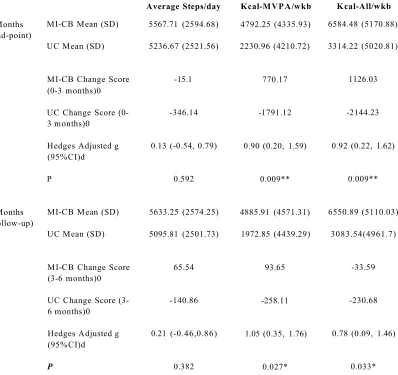
Descriptive Statistics (mean, SD), Raw Change Scores (within treatment group), Significance Levels (between treatment groups), and Standardised Mean Differences (Hedges adjusted g) with 95% Confidence Intervals for the Primary Outcomes at 3 and 6 Months between Treatment Groups...147
Table 5.5
Table 5.6
Table 5.7
Table 6.1 Table 6.2
Table 6.3
Table 6.4
Table 6.5
Table 6.6
Table 6.7
Table 6.8
Table 6.9
Table 6.10
Descriptive Statistics (mean, SD), Significance Levels (between treatment groups) a, and Standardised Mean Differences (Hedges adjusted g) With 95% Confidence Intervals for Secondary Outcomes at 3 and 6 Months between Treatment Groups...152
Pearson's r Correlation Coefficients between Psychological and Physical Activity Outcomes for MI-CB Intervention...156
Sample Size Estimates for rmANOVA and ANCOVA...160
Definitions of Treatment Fidelity Framework Components...180
Ratio and Percentage Thresholds for Level of Competency in MI Skills for the MITI...189
Treatment Fidelity Definition and Methods for Assessing for Design of Study...193
Treatment Fidelity Definition and Methods for Assessing Provider Training...194
Treatment Fidelity Definition and Methods for Assessing Intervention Delivery...195
Treatment Fidelity Definition and Methods for Assessing Intervention Receipt...196
Treatment Fidelity Definition and Methods for Assessing
Enactment...197
Mean, SD, and Total Amount of Cognitive-behavioural Techniques Delivered During the MI-CB Intervention...206
Cognitive-behavioural (CB) Techniques That Were Not Applicable to Participants...207
List of Figures
Figure 1.1 Structural diagram of the thesis...10
Figure 2.1 Flow chart of article selection and exclusion from database search...25
Figure 5.1 Flow diagram of the intervention delivery...135
Figure 5.2 (a) Adjusted for baseline means for Kcal-MVPA/wk means at baseline, 3,
and 6 months by treatment group... 148
Figure 5.2 (b) Adjusted for baseline means for Kcal-All/wk means at baseline, 3, and 6
months by treatment group... 148
Figure 5.2 (c) Adjusted for baseline means for average steps/day at baseline, 3, and 6
months by treatment group...148 Pilot study recruitment and retention flow diagram...159
Results of coding task assessing MI-CB integration... 203
Figure 5.3
Abbreviations
BARSE Barrier Self-efficacy
BCC Behaviour Change Consortium BCTs Behaviour Change Techniques BHF British Heart Foundation
BMI Body Mass Index
BPL Barnsley Premier Leisure BPS British Psychological Society
CB Cognitive-behavioural
CBT Cognitive-behavioural Therapy
CEMI Client Evaluation of Motivational Interviewing
CHAMPS The Community Healthy Activities Model Programme for Seniors Scale
COPD Chronic Obstructive Pulmonary Disease CVD Cardiovascular Disease
DoH Department of Health
E-P-E Elicit-Provide-Elicit method GIS Geographical Information Systems GPS Global Positioning Systems HRQoL Health Related Quality of Life
IPAQ International Physical Activity Questionnaire KASY Keep Active South Yorkshire Trial
MET-minute Metabolic Equivalent of Task per Minute MI Motivational Interviewing
MI-CB Integrated Motivational Interviewing and Cognitive-Behavioural Techniques
MISTS Motivational Interviewing Supervision and Training Code
MITI Motivational Interviewing Treatment Integrity
MVPA Moderate-Vigorous Intensity Physical Activity
NHS National Health Service
NICE National Institute of Health and Care Excellence
OARS Open-ended questions, Affirmations, Reflections and Summaries
OERS Outcome Expectations and Realisations for Physical Activity
Scale
PA Physical Activity
PARS Physical Activity Referral Scheme
RCT Randomised Controlled Trial
SM Successful Physical Activity Maintainer
SMART Specific, Measurable, Achievable, Realistic and Timely
(Goal-setting)
SPAQ Scottish Physical Activity Questionnaire
TF Treatment Fidelity
TTM Transtheoretical Model
UC Usual Care
UK United Kingdom
UM Unsuccessful Physical Activity Maintainer
Chapter 1
Chapter 1: Thesis Introduction and Background: Physical Activity Maintenance
1.1 Introduction
This chapter provides an overview of the prevalence of physical inactivity and the importance of physical activity (PA) maintenance for promoting health benefits in adults with chronic health conditions. The chapter also outlines the context for the intervention conducted as part of this thesis; Physical Activity Referral Schemes (PARS) and provides the definition of PA maintenance used throughout the thesis. The methodological limitations of current PA interventions are discussed and future research directions, which this thesis will explore, are set-out. The chapter concludes with the purpose of the thesis, including the content, direction and structure.
1.1.1 The Impact of PA and Inactivity on Public Health
Physical inactivity has been described as a pandemic negatively affecting the world's population as it contributes to major chronic health diseases, including cardiovascular disease (CVD), specific cancers, and type 2 diabetes (Lee et al., 2012). In the UK, inactivity accounts for 37% of CVD risk factors and costs the NHS an estimated £1.06 billion per annum with wider estimated costs of £9 billion per annum to society and the economy (Allender, Foster, Scarborough, & Rayner, 2007; Townsend et al., 2012). Specifically across Yorkshire and the Humber, inactivity produces costs of an average of £20 million per annum (UK Active, 2014). Inactivity contributes to premature deaths and evidence suggests that PA can help prevent or manage chronic conditions, including: CVD and associated risk factors, stroke, cancers, obesity, diabetes, and musculoskeletal conditions (DoH, 2011; Piepoli et al., 2010). Consequently, more needs to be done to promote PA at a local and national level (DoH, 2011).
1.1.2 PA Guidelines for Health Benefits
(DoH, 2011). MVPA is defined as running and swimming. It is also recommended that adults should undertake resistance training on at least two days a week to improve muscle and bone strength (DoH, 2011). Resistance-based exercise consists of exercising with weights or carrying heavy loads, such as groceries. Evidence supports that these activities can account for 30% or 27% reduction in all-cause mortality rates in 'healthy' adults and adults with chronic health conditions respectively (Schoenbom & Stommel, 2011; Warburton, Charlesworth, Ivey, Nettlefold, & Bredin, 2010). Specifically, it is recommended that adults accumulate the activity in short bouts across the day (i.e., >10 minutes; Barr-Anderson, Au-Young, Whitt-Glover, Glenn & Yancey, 2011) because the 'law of diminishing returns' applies, suggesting that longer durations (i.e., > 1 hour) of exercise does not necessarily produce additional health benefits (Moore et al., 2012). Therefore, it is important that interventions and health professionals encourage adherence to the government PA guidelines to produce health benefits.
Despite clear recommendations and health benefits, not all adults are meeting the guidelines. Health Survey for England (2012) demonstrated that 67% men and 55% women achieved 150 minutes of moderate activity per week (Scholes & Mindell, 2012). Specifically across Yorkshire and the Humber, statistics suggest that an average of 30.42% of the population engages in less than 30 minutes of moderate activity per week (UK Active, 2014). In terms of the guidelines for muscle and bone strength, 34% men and 24% women engaged in resistance based exercises (Scholes & Mendell, 2012). What is more, when objective data is collected instead of self-reported data, the evidence reveals that adults are even less active as only 6% men and 4% women have been shown to be active (Health and Social Care Information Centre, 2013).
itself, is a barrier to PA engagement (Busetto et al., 2009). With reduced physical function and quality of life, comorbidities are likely to develop, such as depression, anxiety and other physical illnesses, making it even harder to engage in activity (Schoenbom & Stommel, 2011). Therefore, interventions need to do more to promote PA in adults with chronic health conditions, whilst taking into consideration comorbidity.
1.1.3 Physical Activity Referral Schemes for Adults with Chronic Health Conditions
A common treatment option available to adults with chronic health conditions within the UK is Physical Activity Referral Schemes (PARS). A comprehensive description of PARS in general can be found elsewhere (BHF, 2010). Briefly here; PARS aims to support adults (aged 18+) that are sedentary and have one or more stable conditions (e.g., stable angina, hypertension, chronic obstructive pulmonary disease [COPD], multiple sclerosis, depression, and back pain; Pavey et al., 2011). Individuals are generally referred (by a GP or health professional) to an exercise professional, often within a local authority leisure facility, for either free or reduced cost exercise sessions, usually available for 12-weeks. While best practice guidelines exist for the commissioning of PARS (cf. National Institute of Health & Clinical Excellence [NICE], 2006), no delivery framework exist and there is little evidence on the most effective interventions to be delivered to PARS participants (Pavey et al., 2011). As a result, the precise nature of service structure and delivery content varies greatly between providers (British Heart Foundation [BHF], 2010).
The effectiveness of PARS has been questioned as evidence suggests that, while PARS can generate short-term increases in PA, they fail to promote long-term behaviour change (Harrison, Roberts, & Elton, 2004; Pavey et al., 2011). Additionally, PARS might be better at improving PA in certain conditions such as cardiac patients, as opposed to those with mental health conditions (Murphy et al., 2012). Given that PARS accepts referrals from individuals with a range of chronic health conditions and comorbidities, there is a clear need to understand the commonalities of effective PA maintenance promotion across health conditions (Piette, Richardson, & Valenstein, 2004). An understanding of the common factors for PA promotion can enhance services that target such a heterogeneous population.
Another reason for the lack of effectiveness has been concerned with the fact that PARS is largely exercised based rather than a psychological behaviour change intervention (Pavey et al., 2011). NICE recommend counselling and psychological approaches to promote PA behaviour change over purely exercise-based interventions in individuals with chronic conditions (NICE, 2009). Therefore, the influence of a psychological or counselling based intervention for PA promotion warrants further attention within a PARS setting.
1.1.4 The Importance of PA Maintenance
To achieve health benefits that positively impact on a health condition, one must adopt PA as a lifestyle change and maintain it (DoH, 2011). Even if one initiates PA for a length of time (e.g., three months), a relapse or reduction in PA across as little as 10 days can reverse any improvements in health (Elley, Bagrie, & Arroll, 2006; Mujika & Padilla, 2000a; Sonne et al., 2010). Evaluations of PA interventions have provided evidence for their efficacy in promoting initial short-term increases in PA but are rarely effective beyond three to six months after intervention cessation (Buckworth & Dishman, 2002; Foster, Hillsdon, Thorogood, Kaur, & Wedatilake, 2012; Marcus et al., 2000; 2006; Muller-Riemenschneider, Reinhold, Nocon, & Willich, 2008). Consequently, NICE proposed research guidelines emphasising the need to develop effective interventions that promote PA maintenance post-intervention (NICE, 2006).
1.1.5 Defining PA Maintenance
be used throughout this thesis. Typically, researchers agree that any individual who regularly engages in PA for at least six months has successfully maintained PA (e.g., Amireault, Godin, & Vezina-Im, 2012; Eakin, Lawler, Vandelanotte, & Owen, 2007; Fjeldsoe, Neuhaus, Winkler, & Eakin, 2011; Kroeze, Werkman, & Brag, 2006; Marcus et al., 2000; 2006). Specifically, PA maintenance is suggested to occur in two ways: (1) the individual adopts and maintains PA independently without external intervention; or, (2) if an intervention was delivered, the individual must maintain PA for at least six- months after the intervention ends (Amireault, et al., 2012; Marcus et al., 2000). Therefore, the definition of PA maintenance used within this thesis is those who have maintained PA for six months post-intervention. It must be noted that adults with chronic health conidtions and disabilities might not be able to achieve the guidelines for PA (Tudor-locke et al., 2011) and therefore PA maintenance will be measured in accordance with the purpose and methods of each study. Overall, by exploring the factors that influence PA maintenance after an intervention, recommendations for future research and healthcare practice can be made.
1.1.6 Promoting PA Main ten an ce
policy documents (e.g., NICE, 2011). Therefore, further research is needed to understand the mechanisms that influence PA maintenance, which can help develop more effective interventions and inform healthcare practice.
1.1
.7
Limitations of Current PA Interventionsdecisions about how best to promote PA in this population (Tinetti, Stephanie, & Studenski, 2011). Further research is needed to understand long-term PA behaviour change within a clinical population given that PA is a core component to treatment (Piepoli et al., 2010). By addressing the above methodological limitations, the effective (or ineffective) mechanisms for the PA maintenance phase can begin to be identified in adults with chronic health conditions.
1.2 Purpose of Thesis.
This thesis aims to advance knowledge of the mechanisms influencing PA maintenance in adults with chronic health conditions. Such mechanisms concern the theory, determinants, strategies, intervention components and the five areas of treatment fidelity (i.e., design, training, delivery, receipt and enactment). To achieve this, a theory-driven PA maintenance intervention will be developed, delivered and evaluated within the context of PARS to assess PA maintenance (or relapse) across six months post-PARS. Intervention mapping is used to systematically guide the intervention development, implementation and evaluation (Bartholomew, Parcel, Kok, & Gottlieb, 2006). Briefly, intervention mapping consists of six steps, including: (1) conducting a needs assessment (e.g., exploration of the problem, theories, determinants and strategies); (2) identifying intervention objectives and change objectives (based on step 1); (3) identifying theoretical methods (e.g., self-monitoring from control theory) and practical strategies (e.g., self-monitoring of PA); (4) intervention development (e.g., materials); (5) consideration of the methods for intervention adoption and implementation; and, (6) intervention evaluation (outcomes and processes).
(Breckon et al., 2008); and, (5) conducting a comprehensive evaluation of the five areas of TF (i.e., design, training, delivery, receipt and enactment) to identify 'what works' in the PA maintenance intervention (Bellg et al., 2004). By addressing the limitations of current PA maintenance interventions, this thesis will produce recommendations for future research and for practice for public health promotion, training, and health service development.
1.3 Thesis Structure
Chapter 1: Introduction
Chapter 7: Thesis Synthesis, Recommendations, Reflections and
Conclusions
Phase 2: Intervention Development & Delivery
Chapter 6: (Study 2b)
Treatment Fidelity of an Integrated MI- CB Intervention for PA Maintenance: Chapter 3: (Study 1) Determinants and
strategies for PA maintenance in adults with chronic health conditions: A
qualitative study
Phase 3: RCT Pilot of MI-CB Intervention, Evaluation and Treatment Fidelity
Chapter 2: Interventions Promoting Physical Activity Maintenance for Adults with Chronic Health Conditions: A scoping review of the literature.
Phase 1: Needs Assessment: The Problem, Theory, Determinants, & BCTs
Chapter 5: (Study 2a): Efficacy and Feasibility of an Integrated MI-CB Intervention for Physical
Activity Maintenance: A Pilot Randomised Controlled Trial.
Chapter 4: Development of an Integrated Motivational Interviewing
and Cognitive-behavioural (MI-CB) Intervention for Physical Activity Maintenance: An Intervention Mapping
Approach
Figure 1.1 Structural diagram of the thesis.
1.4 Content of this Thesis
1.4.1 Chapter 2: Promoting Physical Activity Maintenance for Adults with Chronic Health Conditions: A scoping review of the literature.
A broad systematic scoping review adopting semi-quantitative analysis (Hutchison & Breckon, 2011) is conducted to explore the intervention components, theories, determinants, and BCTs for PA maintenance in adults with chronic health conditions (e.g., cardiovascular disease and diabetes). Included in the review are RCTs with at least a six months post-intervention follow-up or longitudinal prospective cohorts with duration of at least six months conducted between the years 2000 to 2013. The review also aims to identify research gaps within the literature, which provide justification for further research to explore the determinants and strategies underpinning successful and unsuccessful PA maintenance within adults with chronic health conditions (Study 1).
1.4.2 Chapter 3: Determinants and Strategies for Physical Activity Maintenance in Chronic Health Conditions: A qualitative study
techniques (MI-CB), such as goal-setting and self-monitoring. Additional recommendations for future research and intervention development are proposed.
1.4.3 Chapter 4: Development of a Physical Activity Maintenance Intervention for Chronic Health Conditions
Chapter 4 details the methods of the systematic development of a theory-based integrated MI-CB intervention for PA maintenance and forms Phase 2 of the thesis. This method section is discussed in accordance with the six steps of intervention mapping (Bartholomew et al., 2006) outlined previously. Multiple theoretical components are selected, such as expectancy-value theory (Janis, 1984) and social cognitive theory (Bandura, 1986) to inform the determinants (e.g., congruence between PA outcome expectations, experiences and values). Example methods of how MI-CB aims to change such theoretical determinants are outlined. A pilot RCT with a usual care control group is proposed for intervention evaluation, including an assessment of behavioural, psychological and epidemiological outcomes and processes (i.e., treatment fidelity). The RCT is called the Keep Active South Yorkshire trial. The advantages and limitations of intervention mapping and the development of the MI-CB intervention are discussed.
1.4.4 Chapter 5: Efficacy and Feasibility of an Integrated Motivational Interviewing and Cognitive-Behavioural Intervention for Physical Activity Maintenance: A Pilot Randomised Controlled Trial.
Lancaster, Dodd, & Williamson, 2004), such as feasibility of recruitment, efficacy of the randomisation procedure, intervention retention, adherence, suitability of measures, and estimation of sample size calculation for future large scale trials. The chapter discusses the potential efficacy and feasibility of the MI-CB intervention for promoting PA maintenance and the impact on psychological determinants. Limitations and recommendations for future research and practice are highlighted.
1.4.5 Chapter 6: Treatment Fidelity of an Integrated Motivational Interviewing and Cognitive Behavioural Intervention for PA Maintenance
Chapter 6 presents the second part of phase 3 of the thesis (Study 2b) and details the five areas of TF: design, training, delivery, receipt, and enactment (Bellg et al., 2004; Breckon et al., 2008). Given that MI-CB intervention demonstrated efficacy for promoting self-reported PA and some determinants (e.g., barrier self-efficacy) but not for other determinants (e.g., coping strategies), this chapter explores the factors that contribute to successful and unsuccessful intervention components. The results reveal further insight with regards to developing effective interventions and propose that the common factors of psychological interventions (e.g., therapeutic alliance, intervention provider competence, on-going training, participant comprehension, satisfaction and enactment with intervention techniques) might be more important for PA maintenance than the theoretical determinants and BCTs (Messer & Wampold, 2002). The implications for future research, practice, and MI-CB refinements are discussed.
1.4.6 Chapter 7: Thesis Synthesis
,
Recommendations,
Reflections and ConclusionsChapter 2
Promoting Physical Activity Maintenance for
Adults with Chronic Health Conditions: A
Chapter 2: Promoting Physical Activity Maintenance for Adults with Chronic Health Conditions: A scoping review of the literature.
2.1 Introduction
The introduction to the thesis (Chapter 1) highlighted the negative impact of physical inactivity on health and demonstrated the importance of PA maintenance for achieving long-term health outcomes (cf. DoH, 2011). Specifically, it was suggested that PA can help manage and/or prevent a range of chronic health conditions (e.g., diabetes and CVD) if maintained in the long-term. Adults with chronic health conditions, however, are less likely to engage in or maintain sufficient PA to achieve health benefits (Marcus et al., 2000). Furthermore, a decline in PA after an intervention ends suggests that individuals struggle with the transition from PA initiation to PA maintenance (Foster et al., 2012). Interventions need to do more to promote long-term PA (NICE, 2006) yet the lack of knowledge about the mechanisms for promoting PA maintenance hinders the ability to design and deliver effective interventions (NICE, 2008). Therefore, the aim of this thesis is to contribute to the PA maintenance knowledge base by developing, delivering and evaluating a PA maintenance intervention using intervention mapping principles (Bartholomew et al., 2006).
2.1.1 Rationale for a Scoping Review
A scoping review is a way of collecting and organising important background information which can be used to map the existing literature (Davis, Drey, & Gould, 2009). According to Armstrong, Hall, Doyle, & Waters (2011), there are a number of differences between a scoping review and a systematic review, which informed the decision to adopt a semi-quantitative scoping review within this chapter. First, although a scoping review can be systematic, the types of research questions are often more broad than a systematic review, which are used to identify existing research gaps and summarise research findings. Second, a scoping review can include a range of research designs and, thus, a quality assessment is not the initial priority compared to a systematic review. Third, as a result of the broad research questions, the data synthesis within a scoping review is less extensive and more qualitative/narrative compared to the quantitative nature of a systematic review. Given that there are four broad areas that need to be understood before a PA maintenance intervention can be developed (e.g., intervention design, theory, determinants and BCTs), studies with different research designs will be reviewed and analysed using a semi-quantitative approach (Hutchison & Breckon, 2011). A scoping review allows for this unlike a systematic review, which often includes only RCTs and focuses on effectiveness (e.g., Fjeldsoe et al., 2011). Additionally, an understanding of the existing literature is needed, including the gaps within the research. Therefore, to review the scientific evidence, and address a broad range of research questions, a scoping review is an appropriate method.
2.1.2 Intervention Design Characteristics
found no relationship between effectiveness and mode of intervention delivery (e.g., face-to-face) or number of contacts at one year follow-up. A reason for the inconsistent findings could be that Fjeldsoe et al., (2011) explored both PA and dietary behaviour changes but the authors argued that the factors that influence maintenance for diet and PA need to be explored separately. Additionally, both reviews included healthy and chronically ill adults but evidence suggests that adults with chronic health conditions need different interventions as they face different barriers to PA, such as illness (Piette & Kerr, 2006; Schoenbom & Stommel, 2011). Therefore, the effective intervention components could differ between these populations and for the maintenance of different health behaviours which warrants research to focus solely on PA maintenance for adults with chronic health conditions.
2.1.3 Theoiy for PA Maintenance
A large focus of the intervention mapping process is to ensure that the intervention is derived from theory (Bartholomew et al., 2006). Theory-derived interventions are found to be more effective than interventions without a theoretical underpinning (Michie & Abraham, 2004; Michie & Prestwich, 2010). A behaviour change theory should define the causal mechanisms which influence behaviour initiation, maintenance and cessation and specify the BCTs which regulate the hypothesised mechanisms or determinants of change (Michie & Abraham, 2004). Nevertheless, selecting a theory to inform an intervention is not easy because more than 20 theories, with multiple theoretical constructs, have been identified to exist (Michie, et al., 2005). Within PA research, the most widely used theories are social cognitive theory (Bandura, 1986) and the Transtheoretical model ([TTM] Prochaska & DiClemente, 1983) as previous evidence suggests (cf. Breckon, Johnston, & Hutchison, 2008; Hutchison, Johnston, & Breckon, 2012). To provide examples of behaviour change theories, social cognitive theory and the TTM will be briefly described below.
techniques to enhance self-efficacy, such as mastery, verbal persuasion and vicarious experience (Conner & Norman, 2005). Nevertheless, the theory is criticised for not specifically focusing on behavioural maintenance and, therefore, does not outline the mechanisms or strategies for this phase of behaviour change (Hutchison et al., 2012). Social cognitive theory has been described in detail elsewhere (cf. Conner & Norman, 2005).
Alternatively, the TTM (Prochaska & DiClemente, 1983) is a stage based model developed from multiple psychotherapeutic approaches. The theory has multiple constructs: stages of change, processes of change, decisional balance (i.e., the pros and cons of behaviour change), and temptation and confidence. The stage of change component of the theory has received the most attention within the PA literature (Hutchison, Breckon, & Johnston, 2009). The stages have a temporal dimension and include: pre-contemplation (i.e., has no intention of performing the behaviour), contemplation (i.e., intends to start the behaviour within six months), preparation (i.e., intends to take action within the next month and has made some preparatory behaviours), action (i.e., has performed the behaviour for less than six months) and maintenance (i.e., has engaged in the behaviour for at least six months). The strategies of change, known as the processes of change, are also outlined and divided into experiential and behavioural processes. The experiential processes include consciousness raising (e.g., increases awareness about consequences of behaviour using education, feedback, and media). The behavioural processes include stimulus control (e.g., re-engineering the environment to make conducive for behaviour change). The theory is described in detail elsewhere (Conner & Norman, 2005).
unlikely to be effective if certain components of the theory are omitted and is applied to behavioural adoption, such as PA.
Instead of choosing one single theory to inform an intervention, it has been argued that multiple theoretical constructs are needed to explain the behaviour in question (Bartholomew et al., 2006; Brag et al., 2005). Particularly, it has been highlighted that a number of theories and constructs can distinguish between the PA initiation and maintenance phase to promote long-term PA (Amireault, Godin, & Vezina-Im, 2012). For example, Rothman's theory of health behaviour maintenance (2000) specifies that favourable outcome expectations influence behavioural initiation but behavioural maintenance is likely to require perceived satisfaction of the outcomes. The emerging evidence largely supports this theory (cf. Fleig, Lippke, Pomp, & Schwarzer, 2011; Rhodes & Plotnikoff, 2006; Rhodes, Plotnikoff, & Coumeya, 2008; Sweet, Tulloch, Fortier, Pipe, & Reid, 2011; Williams et al., 2008). In addition to favourable outcome expectations, individuals must be able to manage/overcome threats, risks and barriers which prevent intentions from translating into behaviour; known as the intention-behaviour gap (cf. Sheeran, 2002). A number of theories and constructs have been used to address the intention-behaviour gap, such as relapse prevention (Marlatt & Donovan, 2005), and action and coping planning (Sniehotta, Schwarzer, Scholz, & Schiiz, 2005). Such theoretical constructs aim to enable individuals to plan, cope, and solve high risk situations and barriers that would otherwise cause a lapse in behaviour. A criticism of applying such theories to PA maintenance is that each theory does not specify the precise mechanisms for this specific behavior. In response to this, a theory for PA maintenance was created based on the known mechanisms and constructs (e.g. self-efficacy, goal-setting and motivation) that support long-term PA (Nigg, Borrelli, Maddock, & Dishman, 2008). To date, however, there is little empirical evidence supporting such theory.
or theoretical components contribute to long-term PA within adults with chronic health conditions and further research is needed.
2.1.4 Determinants for PA Maintenance
When designing interventions, it is important to select the appropriate theoretical determinants for the behaviour change in question and is often informed by behaviour change theories (Bartholomew et al., 2006). Given the multiple theoretical constructs that are involved in explaining PA maintenance, it follows that multiple determinants will also be involved. Nevertheless, reviews of the PA literature largely focus on initiation of PA (e.g., Trost, Owen, Bauman, Sallis & Brown, 2002) and are criticised for including cross-sectional studies or failing to differentiate from PA initiation and maintenance (van Stralen, De Vries, Mudde, Bolman, & Lechner, 2009). Consequently, few reviews draw conclusions regarding the effective determinants for PA maintenance, particularly in adults with chronic health conditions.
The reviews that have explored the determinants for PA maintenance have identified a number of categories of determinants (cf Amireault, et al., 2012; van Stralen et al., 2009; van Stralen, Lechner, Mudde, de Vries, & Bolman, 2010). These categories are: socio-demographic (e.g., being married, male, older and a good health status), psychological (e.g., self-efficacy, realisation of outcome expectations, perceived benefits, decreased barriers, coping planning, and readiness to change and positive attitudes towards PA), behavioural (e.g., previous and current exercise behaviour), social (e.g., social support from an exercise professional) and environmental determinants (e.g., access to PA facilities; cf. Amireault, et al., 2012; van Stralen et al., 2009; van Stralen et al., 2010).
the reviews by van Stralen et al (2009; 2010) focused specifically on older adults (i.e., average of > 50 years). Therefore, different determinants could contribute to PA maintenance depending on age and between 'healthy' and in a clinical population, which warrants a review without the inclusion of 'healthy' adults.
2.1.5 Behaviour Change Techniques for PA Maintenance
The effective behaviour change techniques (BCTs) that promote PA maintenance also need to be selected and implemented within an intervention to regulate the theoretical determinants of change (Abraham & Michie, 2008). A BCT is defined as an active ingredient of behaviour change (e.g., self-monitoring), which alters the determinants or mechanisms that regulates a behaviour (Michie et al., 2011a). The BCTs to promote a specific behaviour should be outlined by a behaviour change theory but this is not always the case, making it difficult to understand which techniques to implement (Brug et al., 2005). Additionally, many studies have been criticised for inadequately reporting BCTs and intervention components, thus making interventions non-replicable (Michie & Abraham, 2008).
Nevertheless, the taxonomy was developed using only 'healthy adults' and adults with chronic health conditions could require other techniques for PA maintenance such as condition management. Evidence suggests that the relationship between inactivity and poor condition management can lead to a cyclic pattern of functional decline (Plow, Finlayson, Motl, & Bethoux, 2012). For example, in adults with multiple sclerosis, poor fatigue management can lead to a decline in PA. Inactivity, can then lead to the onset of other health conditions or symptoms (e.g., depression), which, in turn, makes it more difficult to engage in PA (Plow et al., 2012). Therefore, it is likely that adults with chronic health conditions require condition management and PA strategies simultaneously to promote PA in addition to those outlined by the taxonomy (Michie et al., 201 lb) and warrants further research.
2.2 Review Aims and Research Questions
The primary aim of the scoping review was to understand the extent to which the existing literature explores PA maintenance in adults with chronic health conditions to develop a PA maintenance intervention. By exploring longitudinal studies and RCTs that focus on PA maintenance or include a long-term follow-up, four broad research questions are presented: (1) what are the intervention design characteristics of effective PA maintenance interventions?; (2) what theories are used in effective and ineffective interventions in terms of PA maintenance?; (3) what are the determinants that are associated with PA maintenance?; and, (4) what are the effective and ineffective BCTs that promote PA maintenance? The secondary aim was to identify any gaps within the literature and provide directions for further research.
2.3 Methods
2.3.1 Search Strategy
review articles were identified, backward search method was used to identify relevant reviewed articles and forward search methods were used to identify relevant subsequent articles. Where articles reported a trial name, forward and backward searching was conducted using Google Scholar to search for related articles. All searches were limited to adults > 18 years, peer-reviewed scientific articles, and English language.
2.3.2 Study Inclusion Criteria
The flow chart of article selection and exclusion is displayed in Figure 2.1. Studies were included if they directly explored PA/exercise maintenance across at least six months or evaluated a PA intervention with at least six months follow-up post intervention (consistent with the definition employed within this thesis). Studies were included if the sample had a diagnosed chronic health condition (e.g., musculoskeletal or cardiovascular) or a diagnosed clinical risk factor (e.g., hypertension or impaired glucose intolerance) rather than being 'at risk' (e.g., a smoker). A number of study designs were included: randomised controlled trials, prospective pre-post cohorts and longitudinal prospective cohorts delivered across at least six months. Studies were included if they directly assessed PA as a primary outcome for at least two data- collection points. Intentions to behave or readiness were not accepted as measures of physical activity. For the RCTs, articles were included if they reported between-group differences for PA at all data collection points including post-intervention. Additionally, articles were excluded if they included samples with cognitive impairment, severe mental ill-health (e.g., chronic schizophrenia or personality disorders) or dementia. Only articles that were available electronically were selected.
2.3.2.1 Definition o f PA Maintenance
PA measures which are not comparable (Fjeldsoe et al., 2011). Additionally, for the purpose of this review, intervention effectiveness is also defined as a significant difference between control and experimental conditions at the longest follow-up point within RCTs.
2.3.3 Procedure
All relevant publications were scanned for eligibility and hard copies obtained for included studies. Given that this review consisted of a broad range of research designs adding to the variability of results, a descriptive and semi-quantitative approach was adopted and has been used within other scoping reviews (Hutchison & Breckon, 2011). This approach adds an objective, systematic and analytical point of view to what would otherwise be a subjective narrative literature review. Each study or intervention was coded with a bibliography number {cf. Table 2.1). Bibliography numbers were used to identify the variables of interest within this review, which were: (1) sample characteristics, including sample size, health condition, study length, study design, and gender; (2) intervention design, including intervention duration, length of follow up, number of contacts, interventionist and whether PA maintenance was achieved at follow-up; (3) theoretical content; (4) effective and ineffective determinants or correlates; and, (5) BCTs.
Documents included in final scoping review
7V= 70
Citations identified from searches
N = 3886
Citations excluded based on title or abstract
N =3408
Potentially relevant documents retrieved (if full text available
electronically) A = 478
Documents excluded (N = 408)
• Duplicates (N = 176)
• Not consistent with PA maintenance definition ( N= 98)
• Not chronic illness definition (N = 47)
• PA is not the primary outcome measure or includes a measure of physical function ( N= 59) • Not relevant (N = 19) • Dementia (A = 1) • Protocol (N = 3) • Qualitative (N = 5)
Figure 2.1. Flow chart o f article selection and exclusion from database search
2.4 Results
Ta bl e 2. 1. Bi bl io gr ap hy of Inc lu de d A rti cl es in the Sc op in g R ev ie w e so U X5 6 no© © &
s
se ZQ. >-* S
CD £ .2 3
s z 5
733 J2 <!
.2 ^ E D
© _c czi © E "0O ©
CL "5 2 00
'> c3 •— 3 (U
o o
o o CN © o ‘EoCL 03 oo oo X PL © X 733
2 b
.2 32
© .= — •—
Cl Ph
<
00 D < 00 X• • c < .©
© CO • - ^
© 3 0 ™^ T5 H •- O
60^ 63
2 T3 C
R § 5 ! i-; c/3 O
e c
.2 2 o ©
oo O
© .2
o to ►—> O © o
f— s 20
tq - 03 §
£ &
3 h
o y «-> Oo
© © o © c o X) © > tf03 £ © u >-T © o. oo U © /— ' o CN
£ s3 O Q C2
23c 60 O © 73O s © < 60 3 3 £ 3 o 60 3 X 00
— Cl 3 B © ,< a < >>x • s B
2
I I o © U oo c
3O ©
° Id
C/3
M § 8 I
2 o-Z .2
<oo a 73© s CN O o CN C 3 C oc U 3 'jjp 3 2 o >_ X E c 3 © © ■s 3 3 Cl 3 CL 60 C 3 3 O © "cd33 O ‘>3 X© X <L-o Pi © 3© <L-© £ x
© o 60 C o a 73C 3 ffl I d E 3 O
•c
CQ o o CN 3 © "o E < w oo o o CN w o c2 3o 3 3 CL 60 C 3 3 O U 3 Og © tz) 3
© 3 3 3. CL
3 2 © d> 2 3 rfc ©
O 60 733_3 C E 60 O © X3 3 s 33 hJ 3 © 3 O "© CL 3^ X X ■g3 CL■ © 3 § © 3 Ocz; X X ‘E W 3 © 3 O
H Cl CO
2" CO 2 X 2 O 0 O 0 0 0 CN t— O ■—0 3 . 0 tz CN «5 CN 55 00 733 733 o 73 03 0
E "3 E "3 E CN
oo CL Q >> 733 © X3 3 _3 E© X H 60 _o o Xo a
O—oi
"3 E 3 O •E m ■3-O O CN b © > < C o C/3 CL 23 a © © ■8 3 © 2© § tT O o CN © £
U £
W IS EW O M A N pr oj ec t: C ar di ov as cu la r di se as e St od da rd , Pa lo m bo , Tr op ed et al ., Jo ur na l of W om en 's H ea lth ris k re duc tio n (2 00 4) ss o U <00
O < oo D c cd <D
O <U
<
OOD cd cd u u >» 3 cd E <5 O XJ3cd £OO §&
o "O 60 _o o X Ph CD x W 13 oD-OO cd <D a H x cd 3 <D a Pi ©
3 cd
•2 EId 3
O o
3 ^ "O C
W « -C<d _ E a <
60 o o Xo 03 Oh 3O ■s XCD Pi 3 O >3 -3CD
a
3 3 3 < 3I O
T3 '43 cd £
^ S a c O Id
"cd "5 B & § # 1-53 O 3
^ 3 Cl «3
2 >3 2
W P-.
X "cd i d a 60 o 'o -3o C/3 Ph a 60 jp 'o -3 3 ;s '5cd 3 O ’>3 -3<D a aO 3 3 3 < 3 CD a 60 O o Xo 60 3 3 3 O U T333 3 O 3 -oW 3 Ph U £ o o 3
o
3(D a "O33 CD 60 333 OO O o CN C/0a 00 p'ST-g
.2 8 I Ph w OO
£ H 13CL CL o Ph £ ^
> 8
V£ °h °
5 cn
CO o o (N 3O 3 OO 3 N CO o o CM -33 £ Id >
1—r 3 - 3 u CO o o CM ID CL CU C 'Eo s ~o ’53 Pi rs ’5pi $ ~a a -X3 3 -3oo i 33 a CD 3 _o CD 60 3
<
3rs
‘53 a oO go
CM
O CD
CM N ''"7 d
•a |+H O
CD 0 0
.2
t ID0 X
* & ■S 3
° 3 a 31 3
I E _
o3 ID CO
U 600
> U O
oo N w H 3 £ 60 3 3= ts3
a
C-o o CM 3 3= CD E 3 I* o' 3 O N| oE o | 3
< Cia
60 3 60 O 3 CD E O 60 3 £ E 3360 3 X ! O ’£ U CD <c3 "O33 60 C ‘C3 "O CD X CD 60 ’ 3■5 *3 P 33
a
33a 3O ■■S 60E 3
3 3 ►2 3 W <j < 3
.3"5
433
3 =
§
.2S2 S
CD 3 3
co —
9-_cd cd
(D 4 P• CD
a s* •s X ID 60 53X 03 O P
.. o
3 3 o <D
Pi
W 03 O I d *70 60 O
a ^
r l CD
U 3 3 u5—c CD 43 C X W60 3 Xo 3C—i H C ■o .2
03 .2 2
a ' 3
^ C/3 w ►E
h a
■op 3
a
o
x
t io
p c c .E .0 3 «
343 % a C3 "£
1 .1 E g.
<D S '
3 3 HH O
<
a a o X •o 3 a 0ic -2 60 £
.2 s
S Z
a
A D A PT : A c tiv ity , D ie t an d Bl oo d Pre ss ure Tr ia l B ur ke , Be ili n, Cu tt et al ., (2 007 ; 20 08 ) Jo ur na l of C lin ic al E pi de m io lo gy A us tr al ia Bu rk e, M an so ur , M ori e t al ., (2 008 ) H ea lth Ed uc at ion R es ea rc h cd § U cd cd c cd U cd f S u "Oc 03 < OO o cd £ J-H o z < CO D OQ O s O _c U 3 O Vi 03 >O '3s cd
o —
• *5
o cd "o o £ ^
° 3
0 o
3 1-5 ° 3o 1 cd 'X3 o c X Q- <d o o > >> i= 33 c/3 3
PM W Oh
> 3 X<u m w D 3 >3 <* XD C/3
t:o -a‘5 mX CL CO D75D
3 3 K D O 3 L.3Ob-O D '> 75
O 3 F
co XD
CQ•->3O
D 3 C+-O 33
C/3
T3D 333‘CD
E s < <
-23 O V) 3 > _o "3 3
C3 o — „
M- 15O 3 3
u c
CL d
2 > 3 2 W PU
OJ) _o oo c O 00 _o oo 5 3 3>% o x 75 x3 P-t O 75 E 3 O o oo c 3 Uo b 3 U EoCL CL 3 CO 3
XCl
Cl a U 3 X3 O ON o 3 3 _o So 5CL 23 l L O U
2 0 3= E <N M CL) Q 3 t"-O o C N ¥p*7» c <u X 00 3 ffi o 3 u oo 3 °
2 ® r 3 D
Slh 3 M—i
O D
X
'3 _o
O 3
Ph H 3 cd >. D Dr~! g ^ E o oo
U o o
<U ON
3 «
« § 3 O > £J,
3 0) 3 ’> 3 o X Ph of o 3 > o £ohJ 3 -3O o pp3: hJ
m oc0
0"0 00CN 'E p < 75 3 O X X O 3~ 3 O U o 00
’£ (U oo /-v
3 O rE °
O CN, 3 '"7
O x
> 3
O O (N w T33 cd cd C £ S CL 3 Pm
X) ^ 25 00
PC O
H O O CN .3 *Ph 3
cd ‘C 3 < PM
T3
3 3
._ Cl
.2 75C 3 H H E 04 o < -c
F-1 u
CO 3 a “
C O CD
W 2
4Pcd
+ -» C/3
cd cd D O- c/5 —
C c n O cd
£ -s
<D »-GJ S w 2
3
3
O
2 CO
9 x
3 ts 3 3
3 O
2 E .E oo3 i E w D <2 .2 3 o O
& is S & O 3 C/3 1) (D C/3
23 ^ 2 b
C (D
r9 c
U 3 3 •c H 3o O b Ph p7> ■> o
<
CD JZ H H § P U < 03 ■S 3O b D 3 b3 D >. E D 3 3 b O 00 >, 0•_CL > 3 0 O 3 3 75 .X _o r3 'vi X X PM 3 XD L. oo 3 CD C/3 3 3 O o60 E 3 (D
3 3
(D - r £ % ~ 6
.2 o
T33 D 3 ’•5 D X D T33 3 00 3 D 23 o
X) _3 Ph
00
3
3 c/i
X o CL.>
D > D E E—C C/3
X a« b >
00
o
ii z
£
CN
c 2 O U u 2 © X 5 a. TS© 88 Z
= -s bfl &
.2 s
S £
s
^ .'S < C/0 3 x W =8 C/5 d oa. C/3
3 C/3
I *
33
X X 3 •g S ■5
£ 3 s2
< ctf S
CQ oo <N cd 3 3 o !* >> J bfl § £ <L) 3 O X Q. _2<u 2<u <D 5? ^
> c/3 <-l ^(U . t 3 c/3
^ "5 *3 ^ ‘d cd
3
<u o
■si
*-« 3 x & u oo '2 *-* o
3 >= o - 3
c 3
2 .S
©
X i£ ^ I d
o <
1/3 2
o o
£ J
bfl 3C/5 © 3 £ • § .51
1/5 < X cd X 3 pci cd 3 O 2 3 CL o3 X
° 2 •“5 3
3 3 3 > 3 C/5 bfl co X PL, 3 Ph a3 On
X O3 O
ffl £S
.5 *3u cd
<
PL X © c /i 3 O « 3 (U -d X 2 PLL-C 3
o tuo 3
' v r .
X x ”© 3 ^ ffi *5 ^
S '1
ffi O
£ bo 73 'Id
O *co W
■s £ = 3 >, Cl, L- bfl
^ o o
"O — 3C 3 3 9 2 0 P
CN ON
o o
<N O O '—' CN CN
C/3 •g .SP r? Pl ©
bfl “o C L- X ^ 3 3 © X C/3 Q
3 C/3 C/3
_S x xft ° °
r2 3 3 O PL PL
O > X § 3 o
° 2
2 .2
.. 3
< > £ b ^ c ► > < u O c/3 s £
3 X 3 § u x 3 s X "cd 3 a bfl _o O Xo b*3 ON O o CN 3 o -do Ph 3 CD £ C/3 3 % a X § bfl _o o X 3 bfl 3 3 m X X s 3 u C/3 3 ©
•8
ON O O CN 3 _ 3 o O > 3 Q 3 >H X rn 3 3 2 — 3 O 3 < 3 3 3d |
a l
OP —
.2 g x .2
2 Id 3 C <D d c/3 (U £
<*} "XD
gcd C/5 C/3 /^ -N O O
II
3 ^X o
X E ■ f t — 5 3 Q pl
-O bfl
<D 3
© ©
s > w bfl o
3 . 3
< C/3 a bfl c 3 £ bfl O co 3 a & 3 > cd x U x ' 3 N O c 3 Cl 3 X 3 X X 3 3 3 C 3L- -t-> c 9 3
3 X) O 3 < bfl _ o o X 3 C/3 PL X "cd 3 X O CN X 3 3 > 3 © pci X 3 W bfl O — PL bfl 3 ’ > 13 X X bfl O a 3 X H ON
o U so CZO Xls — ■ooo o u 2 e #© 2 .£* *Cu MV fi i-o V s 3 £ >3 X
58 £ iw *2
wo g
.2 3 x z
s
C3 x03 3 03 U 0^ W) _o o 13 E 3 00 X pi 3 X 3 o Pi bb |h oo PQ 3 00 X §> oo _3 ‘o •5 3 O > 3 X (U cq 3 C 3 < r 3 <D 3 O Xu 3 XO •—! <u X 2 2 2 J*-T <+-O 2 C 0 O0 2 CN <L> WO 33 XO i O c« <U WO 3 C/3 X 3 3 <2 O E> 3 C/3 X3 00
00
C/i X3 " 3
_3 Q
X CN 3 0 ) , x 2 w o > 3 3 H O 2 _3 CN -o 3 3 00 z 3 O > 3 X 00 m 3 3 3 < E oo oq3 <
s °
£5 CN
"S ^
o f '£ o
• •
.1
3 2•c « H O § 3 2 > 3 X .3 O
> E
< in O 3 O ■ 5 3 3 O x3 3 2 3 Ph 3 '5 3 55 2o O <u 3 O X
Oh ^ (U o
2 1 S £ 3 00
. E •' S£ wo
3 2 w HH 00 CA 3 X 2 3 O 3 X X3 Xao k- X 0 0 _3 2 Xk. 3 2 3 C/3 O (U k- 3 00 O X X 3 2 00 2 0 00 3 •H-* 3 WO 3 3 00 X 3 ' 3 _3" o 2 3 3 £ i/0 U 3 2 oo XI/) o o C/3 o s o CN 3 2 x 2 OQ 3 CT •O X X 3 O 3 E 3 00 X wo 3 >3 X Ph 3 X3 3 3 u wo o
2 o 3 O o X 3 00 > 3 00 00 2 O S 3 O X. 3 ' > 00 d o 3 > 3 00 ,—, F CN 3 0 O U CN 3 E o X a. E >-2 oo C/3 P i—< OO X 2 X "3 oo X Ph 2 B ■3" < m D 3 00 X x3 3 O CN 2 2 _3 00 WO 3 3 X 3 3 ■5 3 '5b 3 O 2 r -3" 3 c/o k. 0) o 3 3 u <k-o o CN 3 CQ X 3. E 3 u oo wo 3 3 X 3 O ' > 3 X00 X X 3 3 00 X 00 <+-O 3. 3 £ _o O 2 _3 '3 3. C/0 < C/0 2 wo 3 u 3 ’c5 2 «+H o *3 £ 3 o U
S S ^ X
22 3 X 3 - 0 3 U 3 WO
CS 3 CQ
> 3 c/3 o > 3 OO 2 ”53 x 2 C3 E xa. _3 3 O 3 3 £ 2 3 o M O 03 3" 3 u to 2 3 xco
3 bb
. 3 C 2 <
X W OO S> k-3 O o 3 W o X 2 3 3 & '5b
2 | w 2 2 2
2 2
o 10 3 X3 3 3 U >3 3 3 E 00 O 3 00 SC wo _o o X wo o o X o c/3 2 3 o 3 00 X
s
_g X o 0 13 >3 s-01k. <D WO . 3 2 .bb
u o io PQ «N ~
3 X 3 O CN 3 £ Xo c/o 2 E o 2 2 <D X O 2 E < 2 O o 2 <1 c/o o 8* a3 X H •X 3 •8 3 •-c/3 -Eu X
2 2 x3 C3 cz> 3
c
o s 2 2x 3
x 3 £
r-X .5
2.4.1 Sample Characteristics
A summary of the sample characteristics (n = 54) are provided in Table 2.2. The overall sample size of the studies was 18,416 and ranged from 25 to 1674, with the majority of studies (31.48%) reporting a sample size range of 200 to 500 (M = 341.04,
SD = 378.59). The age range of the sample was 45.7 to 74 (M = 57.89, SD = 6.44). The majority of studies were conducted with men and women (90.74%) or women only (11.11%) but no studies explored PA maintenance within male only samples. The majority of studies were conducted with cardiovascular patients (27.78%