New daily persistent headache in the paediatric population
E Kung1, SJ Tepper2, AM Rapoport3, FD Sheftell4& ME Bigal1,51Department of Neurology, Albert Einstein College of Medicine, Bronx, NY,2Cleveland Headache Center at Cleveland Clinic, Cleveland, OH, 3Department of Neurology, University of California at Los Angeles, Los Angeles, CA,4The New England Center for Headache, Stamford, CT,
and5Merck Research Laboratories, Whitehouse Station, NJ, USA
Kung E, Tepper SJ, Rapoport AM, Sheftell FD & Bigal ME. New daily persistent headache in the paediatric population. Cephalalgia 2009; 29:17–22. London. ISSN 0333-1024
We conducted a clinic-based study focusing on the clinical features of new-onset chronic daily headaches (CDH) in children and adolescents. The clinical records and headache diaries of 306 children and adolescents were reviewed, to identify 187 with CDH. Relevant information was transferred to a standardized form that included operational criteria for the diagnoses of the headaches. Since we were interested in describing the clinical features of these headaches, we followed the criteria A and B of the 2nd edn of the International Classification of Headache Disorders (ICHD-2) and refer to them as new daily persistent headaches (NDPH) regardless of the presence of migraine features (therefore, this is a modified version of the ICHD-2 criteria). From the 56 adolescents with NDPH, most (91.8%) did not overuse medications. Nearly half (48.1%) reported they could recall the month when their headaches started. NDPH was more common than chronic tension-type headache in both adolescents overusing and not overusing medication. Individuals with NDPH had headaches fulfilling criteria for migraine on an average of 18.5 days per month. On most days, they had migraine-associated symptoms (one of nausea, photophobia or phonophobia)). NDPH is common in children and adolescents with CDH. Most subjects do not
overuse medication. Migraine features are common.䊐New daily persistent
head-ache, chronic daily headaches, adolescents
Marcelo E Bigal, MD, PhD, Merck Research Laboratories, 1 Merck Drive,
Whitehouse Station, NJ 18901, USA. E-mail [email protected] Received 16 December 2007, accepted 22 March 2008
Introduction
About 4% of the adult population has primary
headaches lasting >4 h/day, for >15 days/month
(1, 2). This syndrome is known as chronic daily headache (CDH) and it affects 30–84% of adult patients seen in headache clinics (3–6). CDH is subdivided into specific headache diagnoses, all of them addressed by the 2nd edn of the International Classification of Headache Disorders (ICHD-2) (7). The most important subtypes are chronic migraine (CM), chronic tension-type headache (CTTH) and new daily persistent headache (NDPH). Hemicrania continua (HC) is usually considered a CDH subtype, although its correct nosological position is still disputed (8).
CM and CTTH are the chronic forms of migraine
and episodic tension-type headache, whereas
NDPH is characterized by the relatively abrupt onset of an unremitting primary CDH. A common feature is that the patient often remembers the circumstances, place and date that the headache began. It is the new onset of this primary daily headache that is the most important feature (9).
CDH is also a significant problem in children and adolescents (10–12). In recent years, several studies have explored the issue of CDH in adolescents, including the proportion and clinical features of CTTH in tertiary care, the clinical characteristics and subtypes of CDH, and particularities and utility of ICHD-2 in the classification of CDH in this age range (13–16). For example, ICHD-2 requires
that, in NDPH, most headache days fill criteria for tension-type headache and not for migraine. In adults, however, it has been demonstrated that an important proportion of NDPH sufferers have fre-quent migraine symptoms, although most attacks do resemble tension-type headache (17).
Since NDPH is still poorly described, and studies on this disorder in the paediatric population are scarce, we conducted a clinic-based study focusing on the clinical features of NDPH in the paediatric population. We contrasted children and adolescents with NDPH, CTTH and transformed migraine (TM). We used TM instead of CM since most ado-lescents sought care in our headache clinic before the publication of the ICHD-2.
Methods
This study was conducted in a tertiary headache centre during the year 2006. We generated a random list of children and adolescents seen at the centre from 1989 to 2005, in order to identify a representative sample of patients in this age range seen in the clinic.
A total of 306 patients aged 6–18 years with a primary headache diagnosis were selected. Age and diagnosis were determined as of the date of first visit. Patients with primary headaches were
divided into episodic headache (<15 days of
head-aches per month) and CDH (ⱖ15 days of headache
per month). CDH diagnosis was subdivided into
without medication overuse (CDH-) and with
medication overuse (CDH+).
Since we were interested in describing the clinical features of NDPH, we followed criteria A and B of ICHD-2 and did not consider the presence of migraine features (therefore, this is a modified version of the ICHD-2 criteria). CTTH was classi-fied according to ICHD-2. TM was classiclassi-fied according to the Siberstein–Lipton criteria (3) for the reasons described in the Introduction. Never-theless, the classification of TM and CM in its
revised form overlaps in >92% of cases (18). As
noted, all subjects with any CDH subtype (NDPH, TM, CTTH and HC) were further divided into with or without acute medication overuse.
Diagnoses were assigned based on information collected using standardized intake forms and daily headache calendars. The standardized forms also included information on all current medications (not just headache medications), including dose, schedule, duration of use, degree of relief and adverse events, as well as all previous headache medications including preventive and acute care
medications. The information from these question-naires was abstracted by one study author (E.K.). To be included in this study, patients had to have been followed in the clinic with one of the subtypes of
CDH for>3 months, providing headache calendars
for this time.
Analyses
Data were summarized using frequency counts and descriptive statistics. We first categorized by the number of adolescents seeking care who had epi-sodic headaches compared with those with CDH. Among the CDH subtypes, we then contrasted NDPH with TM and CTTH, regarding the number of days with severe headache, number of days with migraine headaches, and number of days with migraine-associated symptoms (nausea, photopho-bia and phonophophotopho-bia). We compared proportions with the two-tailed Fischer’s exact test. The Fischer
was used instead of c2 since some expected values
were likely to be small (<5).
This study was approved by an Investigation Review Board.
Results
Of the 306 children seen at the initial visit, 67% were female and 33% male. Age ranged from 6 to 18 years (mean 14). The vast majority were White (99%). The demographics of our sample are described in Table 1.
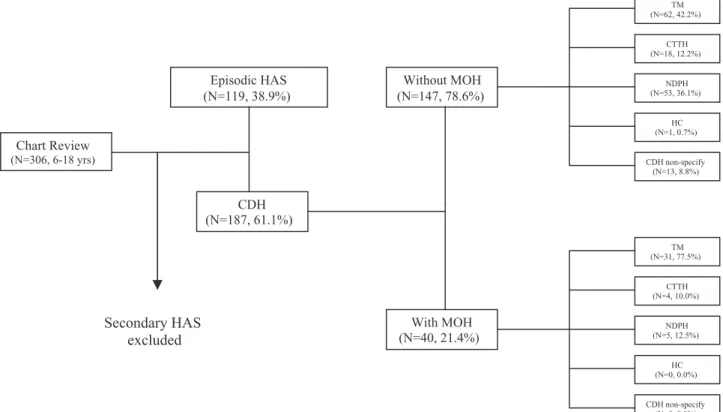
Of the 306 patients, 187 (61.1%) had CDH. Of these, 147 (78.6%) were not overusing medications
(CDH-), whereas the remaining 21.4% were (Fig. 1).
Although overall most children and adolescents with CDH did not overuse medications, the pro-portion of adolescents meeting the modified defi-nition of NDPH and medication overuse (8.7% of
Table 1 Demographics of the sample
Age, mean 14.0 Age, mean (S.D.) 1.0 Gender Male, n 100 Male, % 33 Female,n 206 Female, % 67 Race White,n 302 White, % 99 Non-White, n 4 Non-White, % 1
the NDPH) was significantly lower than that
observed in TM (33.3%,P<0.01) and CTTH (18.2%,
P<0.05) (Fig. 2).
NDPH was more common than CTTH in both the
CDH-and CDH+groups. Among individuals with
CDH-, whereas TM happened in 48.1% of children
and adolescents, NDPH was the diagnosis of 53 (36.2%). CTTH occurred in 12.2%. HC was the diag-nosis of one subject; 8.8% had another diagdiag-nosis.
The vast majority of individuals with CDH+ had
TM (77.5%). NDPH with medication overuse occurred in five individuals (12.5%); another four (10%) had CTTH (Fig. 3). Nearly half (48.1%) of the individuals with NDPH reported that they could recall the month when their headaches started.
Chart Review (N=306, 6-18 yrs) Episodic HAS (N=119, 38.9%) CDH (N=187, 61.1%) Secondary HAS excluded Without MOH (N=147, 78.6%) With MOH (N=40, 21.4%) TM (N=62, 42.2%) CTTH (N=18, 12.2%) NDPH (N=53, 36.1%) HC (N=1, 0.7%) CDH non-specify (N=13, 8.8%) TM (N=31, 77.5%) CTTH (N=4, 10.0%) NDPH (N=5, 12.5%) HC (N=0, 0.0%) CDH non-specify (N=0, 0.0%)
Figure 1 Flowchart of the study. TM, transformed migraine; NDPH, new daily persistent headache; CTTH, chronic tension-type headache; CDH, chronic daily headache; MOH, medication overuse headache.
33.3% 8.7% 18.2% 0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50% TM NDPH CTTH TM NDPH CTTH
Figure 2 Proportion of individuals with chronic daily headaches overusing acute medication in adolescents. TM, transformed migraine; NDPH, new daily persistent headache; CTTH, chronic tension-type headache.
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% + H D C -H D C TM CTTH NDPH HC Other
Figure 3 Distribution of the diagnosis among adolescents with chronic daily headache with and without medication overuse. CDH-, chronic daily headache without
medication overuse; CDH+, chronic daily headache with medication overuse; TM, transformed migraine; NDPH, new daily persistent headache; CTTH, chronic tension-type headache; HC, hemicrania continua.
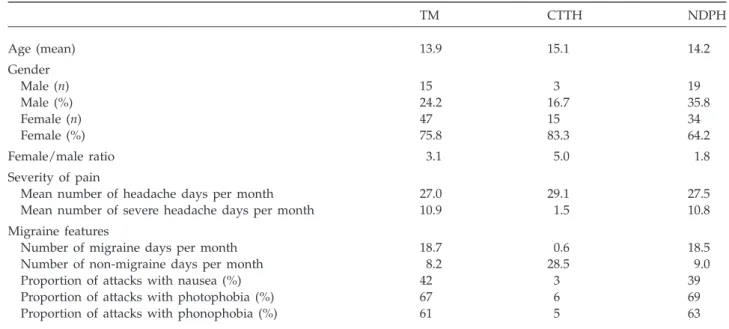
Table 2 compares, in individuals without medica-tion overuse, NDPH, TM and CTTH. NDPH was proportionally more common in boys than the other CDH subtypes. The female:male ratio was 1.8 in NDPH vs. 3.1 in TM and 5 in CTTH. The age at the time of first consultation was similar. Individuals with NDPH had headaches on virtually every day, similar to what was seen in those with TM and CTTH. However, the number of days with severe headache per month was significantly higher in those with NDPH than in CTTH (10.8 vs. 3.2,
P<0.01) and was very similar to TM. Furthermore,
individuals with NDPH had headaches fulfilling criteria for migraine on an average of 18.5 days per month, similar to TM (18.7) and significantly more
frequently than with CTTH (3.6, P<0.01). Indeed,
non-migraine headaches happened on a minority of the days (mean of 9 days/month). A significantly higher proportion of NDPH attacks were accompa-nied by nausea, photophobia and phonophobia, compared with CTTH. The pattern was very similar to what was seen in TM (Table 2).
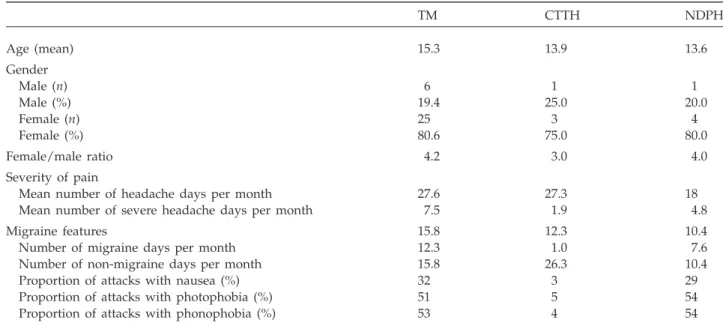
Table 3 contrasts the same features in individuals
with CDH+. Comparisons are limited by the
smaller sample of this group. Nevertheless, indi-viduals with NDPH had a mean of 18 headaches per month, whereas individuals with TM and CTTH had headaches on an almost daily basis. Similar to what was seen in those not overusing
medications, migraine headaches occurred on most of the headache days (57.7%), vs. 57.2% in TM.
Discussion
CDH is a significant problem in children and ado-lescents (12–16). The epidemiology is unclear, in part because definitions have not been uniform. Nonetheless, previous studies have shown that there are several differences between CDH in chil-dren and in adults (11, 12, 15). The relative fre-quency of TM seems to be lower in adolescents than in adults, whereas NDPH and CTTH are more common. Furthermore, medication overuse is far less common in adolescents than in adults. It has been suggested that children may develop CDH in the absence of medication overuse, because they are at increased biological risk (11, 16).
Our data support prior findings. We have previ-ously found that most adolescents with CDH did not overuse medication, and that NDPH was common in this group, more common than usually described in adults (1, 2, 12). Furthermore, we found that, in contrast to what is proposed by ICHD-2, in adoles-cents with NDPH most days do not meet criteria for tension-type headache, but for migraine instead. An important fraction of the days are severe, and most attacks have associated symptoms.
Table 2 New daily persistent headache, contrasted with other subtypes of chronic daily headaches, in individuals not overusing acute medication
TM CTTH NDPH Age (mean) 13.9 15.1 14.2 Gender Male (n) 15 3 19 Male (%) 24.2 16.7 35.8 Female (n) 47 15 34 Female (%) 75.8 83.3 64.2 Female/male ratio 3.1 5.0 1.8 Severity of pain
Mean number of headache days per month 27.0 29.1 27.5
Mean number of severe headache days per month 10.9 1.5 10.8
Migraine features
Number of migraine days per month 18.7 0.6 18.5
Number of non-migraine days per month 8.2 28.5 9.0
Proportion of attacks with nausea (%) 42 3 39
Proportion of attacks with photophobia (%) 67 6 69
Proportion of attacks with phonophobia (%) 61 5 63
In a past study conducted in adults, we had found that about half of patients with abrupt onset of CDH had too many migraine features to meet ICHD-2 criteria for NDPH (17, 18). We then pro-posed that NDPH should be classified based on the abrupt onset of an unremitting CDH, regardless of the phenotype of pain, with CM, CTTH and HC excluded. Based on our current study, this state-ment applies to children and adolescents also.
Our findings were supported by other studies, mainly in adults. For example, Li and Rozen inves-tigated 40 women and 16 men with NDPH, with an age ranging from 12 to 78 years. A total of 82% were able to pinpoint the exact day their headache started. The duration of daily headache ranged from 1.5 to 24 h; 79% were continuous. Nausea occurred in 68% of patients, photophobia in 66%, phonophobia in 61% and lightheadedness in 55%. They concluded that NDPH appears to be a female-predominant disorder, marked by a continuous daily headache with associated migrainous symp-toms (19).
A clinic-based study conducted in Japan found that NDPH may be primary or secondary (20). In that study, the onset of NDPH occurred in relation to a stressful life event in 16%, systemic infection in 12% and extracranial surgery in 7%. However, pre-cipitating events could not be identified in approxi-mately two-third of patients (65%). Although most patients had headaches described as dull and/or pressure-like, one-third had throbbing pain.
Finally, in a paediatric study conducted in India, 15 children with NDPH were identified. Nearly half resembled CM, whereas the others resembled CTTH. Heightened levels of anxiety mostly related to academic stress and achievement were noted in the majority (21).
Limitations must be considered when interpret-ing our results. First, as mentioned, we did not strictly follow the ICHD-2 definition of NDPH, mainly because we were interested in assessing the proportion of individuals with new-onset CDH that had migraine features. Second, results were derived from a clinic-based study in which the influence of referral bias is difficult to assess. Additionally, refer-ral bias may be of particular importance in the paediatric population. Third, this study was retro-spective. However, throughout the study, the clinic has used standardized questionnaires and headache calendars. To be included in this study, at least three consecutive monthly headache calendars had to be present. Fourth, because this study was conducted in a headache clinic, our data cannot be generalized for other levels of medical care or for the popula-tion. Finally, our study is descriptive and we did not assess risk factors for NDHP in adolescents (e.g. psychiatric comorbidity, exposures). One reason it was decided not to do so is because not all indi-viduals in our sample supplied validated question-naires for the assessment of comorbidities in
adolescents. This important issue should be
explored in subsequent studies.
Table 3 New daily persistent headache, contrasted with other subtypes of chronic daily headaches, in individuals overusing acute medication
TM CTTH NDPH Age (mean) 15.3 13.9 13.6 Gender Male (n) 6 1 1 Male (%) 19.4 25.0 20.0 Female (n) 25 3 4 Female (%) 80.6 75.0 80.0 Female/male ratio 4.2 3.0 4.0 Severity of pain
Mean number of headache days per month 27.6 27.3 18
Mean number of severe headache days per month 7.5 1.9 4.8
Migraine features 15.8 12.3 10.4
Number of migraine days per month 12.3 1.0 7.6
Number of non-migraine days per month 15.8 26.3 10.4
Proportion of attacks with nausea (%) 32 3 29
Proportion of attacks with photophobia (%) 51 5 54
Proportion of attacks with phonophobia (%) 53 4 54
NDPH is the least studied form of CDH. A better understanding of this disorder is required, since its most peculiar aspect, abrupt onset of a frequent form of pain, may reveal neurophysiological aspects regarding pain onset and modulation. We found that most adolescents with NDPH do not overuse acute medication. Additionally, most have prominent migraine features. Therefore, diag-nostic criteria should require abrupt onset of a primary CDH of long duration as the sole require-ment for CDH diagnosis. In individuals with strictly unilateral abrupt onset CDH, HC should be ruled out first.
References
1 Scher AI, Stewart WF, Liberman J, Lipton RB. Prevalence of frequent headache in a population sample. Headache 1998; 38:497–506.
2 Castillo J, Muñoz P, Guitera V, Pascual J. Epidemiology of chronic daily headache in the general population. Headache 1999; 38:497–506.
3 Silberstein SD, Lipton RB, Sliwinski M. Classification of daily and near-daily headaches: field trial of revised IHS criteria. Neurology 1996; 47:871–5.
4 Rapoport A, Stang P, Gutterman DL, Cady R, Markley H, Weeks R et al. Analgesic rebound headache in clinical practice: data from a physician survey. Headache 1996; 36:14–19.
5 Manzoni GC, Granella F, Sandrini G, Cavallini A, Zan-ferrari C Nappi G. Classification of chronic daily head-ache by International Headhead-ache Society Criteria: limits and new proposals. Cephalalgia 1995; 15:37–43.
6 Bigal ME, Rapoport AM, Lipton RB, Tepper SJ, Sheftell RB. Chronic daily headache in a tertiary care population. Correlation between the International Headache Society diagnostic criteria and proposed revisions criteria for chronic daily headache. Cephalalgia 2002; 22:432–8. 7 Headache Classification Committee of the International
Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias, and facial pain, second edition. Cephalalgia 2004; 24 (Suppl. 1): 1–160.
8 Matharu MS, Goadsby PJ. Functional brain imaging in
hemicrania continua: implications for nosology and pathophysiology. Curr Pain Headache Rep 2005; 9:281–8. 9 Rozen TD. New daily persistent headache. Curr Pain
Headache Rep 2003; 7:218–23.
10 Koenig MA, Gladstein J, McCarter RJ, Hershey AD, Wasiewski W, Pediatric Committee of the American Headache Society. Chronic daily headache in children and adolescents presenting to tertiary headache clinics. Headache 2002; 42:491–500.
11 Guidetti V, Galli F. Evolution of headache in childhood and adolescence: an 8-year follow-up. Cephalalgia 1998; 18:449–54.
12 Bigal ME, Lipton RB, Rapoport AM, Tepper SJ, Sheftell FD. Primary chronic daily headache and its subtypes in adolescents and adults. Neurology 2004; 63:843–7. 13 Gladstein J, Holden EW. Chronic daily headache in
chil-dren and adolescents: a 2-year prospective study. Head-ache 1996; 36:349–51.
14 Juang KD, Wang SJ, Fuh JL, Lu SR, Chen YS. Association between adolescent chronic daily headache and child-hood adversity: a community-based study. Cephalalgia 2004; 24:54–9.
15 Gladstein J. Children and adolescents with chronic daily headache. Curr Pain Headache Rep 2004; 8:71–5. 16 Bigal ME, Lipton RB, Tepper SJ, Sheftell FD, Rapoport
AM. Evolution of transformed migraine in adolescents: migraine days decline with duration of illness. Neurology 2004; 62 (Suppl. 5): 442.
17 Bigal ME, Sheftell FD, Tepper SJ, Rapoport AM, Lipton RB. Chronic daily headache: correlation between the 2004 and the 1988 International Headache Society diagnostic criteria. Headache 2004; 44:684–91.
18 Bigal M, Rapoport A, Sheftell F, Tepper S, Lipton R. The International Classification of Headache Disorders revised criteria for chronic migraine-field testing in a headache specialty clinic. Cephalalgia 2007; 27:230–4. 19 Li D, Rozen TD. The clinical characteristics of new daily
persistent headache. Cephalalgia 2002; 22:66–9.
20 Takase Y, Nakano M, Tatsumi C. [Primary new daily persistent headache (NDPH): clinical characteristics of forty-three cases in Japan]. Rinsho Shinkeigaku 2003; 43:533–8.
21 Chakravarty A. Chronic daily headache in children and adolescents: a clinic based study from India. Cephalalgia 2005; 25:795–800.