Page | 1 IBP2010-15_Summary_20100325
South East Coast Ambulance Service NHS Trust
Integrated Business Plan
Page | 2 IBP2010-15_Summary_20100325
Foreword from the Chairman and Chief Executive
The ambulance service is on a journey of transformation; we have changed from a service that transported patients to treatment, to a service that is now bringing more treatment to patients. Demand continues to increase for our service – by roughly five percent each year – and the spectrum of patient need that we are now seeing is broader than ever before, ranging from critically ill and injured patients suffering from conditions such as trauma, stroke and coronary heart disease, to patients at the other end of the spectrum with less serious healthcare needs such as minor injuries and illnesses.We fully recognise that we must change and adapt in order to meet the changing needs of all of our patients – no matter what their condition or healthcare need – and deliver continuous improvements in patient care. South East Coast Ambulance Service NHS Trust (SECAmb) is committed to driving that change in order to deliver the best possible care, and therefore outcomes, for patients across Surrey, Sussex and Kent.
Delivering world class outcomes for patients is what we aspire to do – we want to be the best ambulance service; our patients deserve and expect nothing less. We are confident we will achieve this goal and becoming a foundation trust will help us. Foundation Trust status will give us the financial and operating freedoms needed to make the improvements that our patients need and expect at a much quicker pace, meaning higher quality care for all our patients.
Martin Kitchen Paul Sutton
Page | 3 IBP2010-15_Summary_20100325
Table of Contents
Foreword from the Chairman and Chief Executive ... 2
Table of Contents ... 3
List of Figures ... 5
List of Tables ... 6
1.
Executive Summary ... 7
1.1. Vision and Strategy ... 7
1.2. Rationale for NHS Foundation Trust status ... 7
1.3. Market assessment ... 8
1.4. Performance overview ... 8
1.5. Summary SWOT analysis ... 9
1.6. Leadership and Management ...10
2.
Trust Profile ... 11
2.1. Overview ...11 2.2. Range of services ...12 2.3. Performance ...16 2.4. Contractual information ...183.
Strategy ... 21
3.1. Trust vision ...21 3.2. Strategy ...213.3. Measuring achievement of our Strategy ...24
3.4. Aim for NHS Foundation Trust status ...24
3.5. Consultation process ...25
4.
Market Assessment ... 28
4.1. Description of local health economy ...28
4.2. Key factors driving demand ...31
4.3. Objectives of the local health economy ...34
4.4. PEST analysis ...36
4.5. Trust performance ...40
5.
Service Development Plans ... 44
Page | 4 IBP2010-15_Summary_20100325
5.2. Our Trust’s Strengths, Weaknesses, Opportunities and Threats ...44
5.3. Commentary on SWOT analysis ...46
5.4. Key service developments ...48
6.
Leadership and Workforce ... 52
6.1 Management arrangements ...52
6.2 Workforce key performance indicators ...60
6.3 Agency and recruitment arrangements ...62
6.4 Workforce and organisational development ...62
6.5 Human Resources Strategy ...64
7.
Governance Arrangements ... 66
7.1 Stakeholder interests ...66
7.2 Corporate governance and management ...68
7.3 Internal control ...71
7.4 Risk management ...71
7.5 Performance management reporting framework ...72
7.6 Financial controls and reporting ...73
7.7 Audit arrangements ...73
7.8 Compliance Framework ...74
7.9 IT systems ...75
List of acronyms ... 77
Page | 5 IBP2010-15_Summary_20100325
List of Figures
Figure 1.1 - Summary SWOT analysis ... 9
Figure 2.1 - Operational Dispatch Areas and Hospital Locations ...12
Figure 2.2 - Management of 999 calls ...14
Figure 3.1 - Strategy Focus ...23
Figure 3.2 - Stakeholder analysis ...27
Figure 4.1 - Emergency calls by month for 2007-09 ...29
Figure 4.2 - Emergency responses by month for 2007-09 ...29
Figure 4.3 - Number of emergency ambulance calls / conveyances 1998 - 2009 ...31
Figure 4.4 - Calls by MPDS code 2007/08 and 2008/09 ...32
Figure 4.5 - PEST analysis ...37
Figure 4.7 - Return of Spontaneous Circulation (ROSC) on arrival at hospital ...41
Figure 4.8 - Care bundle provided for STEMI ...42
Figure 4.9 - MORI Survey: Satisfaction with SECAmb compared with wider NHS ...43
Figure 5.1 - SWOT analysis ...45
Figure 8.1 - Board and Team of Directors ...53
Page | 6 IBP2010-15_Summary_20100325
List of Tables
Table 1.1 - Historic Annual Health Check performance... 8
Table 2.1 - Proportion of income ...13
Table 2.2 - A&E activity (by incidents) ...14
Table 2.3 - PTS activity (number of journeys) ...15
Table 2.4 - Annual Health Check ratings ...16
Table 2.5 - Annual Health Check: Quality of Services performance 2008/09 ...17
Table 2.6 - National Performance Targets: Existing Commitments ...18
Table 2.7 - Annual Health Check: Quality of Financial Management 2008 – 2009 ...18
Table 3.1 - Background of respondents ...25
Table 3.2 - Issues identified during public consultation and Trust response ...26
Table 4.1 - Population breakdown by PCT area ...30
Table 6.1 - Workforce ...60
Table 7.1 - Proposed governors ...68
Page | 7 IBP2010-15_Summary_20100325
1. Executive Summary
This section:
Outlines our vision and strategy and how we will achieve this
Explains why we want to become a Foundation Trust and the benefits we believe this will bring
Summarises the key elements from our Integrated Business Plan
The key points from this section are:
The Trust has a clear vision and strategy
The Trust has the appropriate supporting mechanisms in place to deliver this vision and strategy
1.1. Vision and Strategy
Our vision is to match and exceed international clinical excellence through embracing innovation and putting the patient at the heart of everything we do.
Our strategy to achieve this is to strengthen and extend our core activities To implement our strategy, we have identified six
strategic objectives underpinned by business implementation measures and key service developments. Our six strategic objectives are:
Improve on the Trust‟s performance standards and reduce variation
Deliver excellence in leadership and development
Improve access and outcomes to match international best practice
Improve satisfaction and experience for all stakeholders
Be an organisation that people seek to join and are proud to be a part of
Convert all available pounds / resources to maximise patient benefit
1.2. Rationale for NHS Foundation Trust status
Foundation Trust status is a mechanism that enables us to deliver the system and cultural change required to become a world class provider of emergency and urgent care. There are many benefits to us becoming an FT – for patients, local people and for our staff. Our key reasons for becoming a Foundation Trust are:
Structural change – Increased local ownership and accountability;
Investment in innovation – Ability to reinvest funds to innovate to improve patient care; Commercial opportunities – Ability to react promptly to opportunities within the
marketplace.
The concept of high
performance is based on four
co-dependent “pillars” that
focus on reducing waste by
maximising efficiency. This
supports the delivery of high
quality, clinically focussed
services for our patients and
the local population.
Page | 8 IBP2010-15_Summary_20100325
1.3. Market assessment
We cover a geographical area of 3,600 square miles, providing Accident & Emergency (A&E) services to the population of Brighton & Hove, East Sussex, Kent, Medway, Surrey and West Sussex and to selected geographic areas within Berkshire and North East
Hampshire on the Surrey County boundary. We serve a resident population of c. 4.3 million people, however, on an annual basis there are approximately 15 million visitors who stay for one night or more, and 96 million day visitor, who may also call on our services. In 2008/09 we responded to more than 500,000 emergency calls; approximately a call every minute. In addition, we provide non-emergency patient transport services in parts of East Sussex, Kent and West Sussex. Our Commercial Services Department provides training, paramedic cover and a private ambulance service to outside organisations. We provide a portfolio of products that cover three distinct markets; Emergency care, Unscheduled Urgent Care and Non-Emergency Care.
1.4. Performance overview
We have a history of strong financial performance since the Trust was formed in 2006. In 2008/09 we generated a surplus of £0.7m on a £149m budget.
In 2008/09 we achieved a rating of “Good” for Quality of Financial Management and “Fair” for Quality of Services in the Care Quality Commission‟s Annual Health Check ratings. Our aim is to improve on this for 2009/10, by achieving a “Good” assessment for both
components. Historic performance against the Annual Health Check rating is shown in Table 1.1.
Table 1.1 - Historic Annual Health Check performance
2006/07 2007/08 2008/09
Quality of Services Fair Good Fair
Quality of Financial Management Fair Good Good
We are working to develop our Quality Account that will become mandatory from 2010/11. This is a mechanism by which the Board can assess quality and address its improvement, and by which all NHS healthcare providers can be held accountable for the quality of care provided by commissioners, patients and the public.
Page | 9 IBP2010-15_Summary_20100325
1.5. Summary SWOT analysis
Strengths
Available 24 hours a day, seven days a week
Strong reputation and positive public image
History of innovation Mobile healthcare provider
Historic performance of category A and call taking standards
Responsive to clinical change
Robust, tested business continuity plans
Weaknesses Higher than average costs
Uni-professional workforce (limited skill mix of staff)
Staff satisfaction Environmental impact
Opportunities Urgent, unscheduled care provision Improving outcomes and experience Diagnostic technology
Managing demand in the whole health economy
Releasing cost improvements in the whole health economy
Foundation Trust status will increase local ownership amongst patients, public and staff
Community cohesion
General health Management
Threats
Payment by Results could result in a disincentivisation to “do the right thing” for patients
Competition from alternative providers Resistance/ difficulty delivering large scale cost improvement programmes
Page | 10 IBP2010-15_Summary_20100325
1.6. Leadership and Management
We have a strong commitment to education, with an increasing focus on the
professionalisation of the workforce. Our vision for leadership development aims to develop our staff to lead improvements through others and this is supported by a series of
organisational development programmes, targeted at different groups of staff throughout the Trust.
Page | 11 IBP2010-15_Summary_20100325
2. Trust Profile
This section:
Provides an overview of how the Trust operates
Sets out the services the Trust provides
Indicates the levels and trends of activities within the Trust
The key points from this section are:
The Trust is an innovative, patient focused organisation The organisation‟s portfolio covers three distinct markets
2.1. Overview
South East Coast Ambulance Service NHS Trust is an innovative, patient focused organisation providing emergency, unscheduled urgent and non-emergency care. We respond to 999 calls from the public, urgent calls from healthcare professionals and, in Kent and Sussex, provide non-emergency patient transport services (pre-booked patient journeys to and from healthcare facilities).
We currently provide services in Kent, Surrey and Sussex, and also to a small geographic area within North East Hampshire and in Berkshire. The Trust was formed in July 2006, following the merger of Kent Ambulance Service NHS Trust, Surrey Ambulance Service NHS Trust and Sussex Ambulance Service NHS Trust.
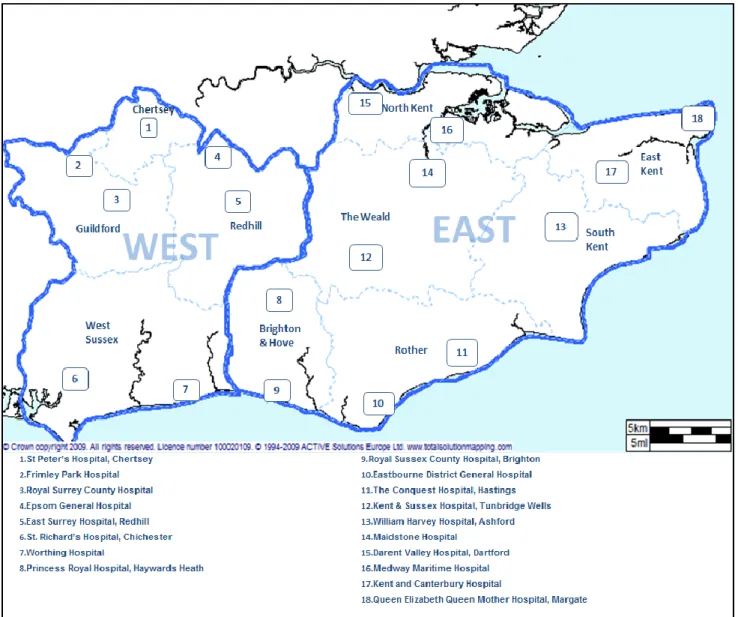
We have a strong track record of improving patient services through the adoption and implementation of innovative clinical practices and equipment, the development of specialist clinical roles and the roll out of new technologies and systems; all aimed at improving patient outcomes, experience and safety, improving the quality of care for the patients we treat. We employ 3,138 members of staff, of which 83.5% are operational, either as front-line members of staff, or within our Emergency Dispatch Centres, with the remaining 16.5% providing support services and management functions. The Trust operates from 65 sites. Operationally, the services are divided into two divisions, East and West, and further into ten Operational Dispatch Areas (ODAs), which are served by three Emergency Dispatch Centres (EDCs). These divisions are based on patient flows into acute hospitals (see Figure 2.1).
Page | 12 IBP2010-15_Summary_20100325
Figure 2.1 - Operational Dispatch Areas and Hospital Locations
2.2. Range of services
We provide a range of services to ensure that we best meet the needs of patients within the communities we serve. These are grouped as Accident and Emergency Services, Patient Transport Services, Commercial Services and Emergency Preparedness. The income
generated from each of these, as well as the proportion this represents in relation to our overall turnover of £156 million in 2009/10 is shown in Table 2.1.
Page | 13 IBP2010-15_Summary_20100325
Table 2.1 - Proportion of income
Income £ million
Proportion of turnover
Accident & Emergency service 139 89%
Patient Transport Service 11 7%
Commercial Services and other non-NHS income 6 4%
2.2.1. Accident and Emergency Service
Patients range from the critically ill and injured, to those with minor healthcare needs that can be treated at home or in the community. Calls are received in our Emergency Dispatch Centre via the 999 system, and triaged in accordance with the Advanced Medical Priority Dispatch System (AMPDS), to
determine the most appropriate response based on clinical need. Calls are categorised as follows:
Category A – Life threatening conditions where speed of response may be critical in saving life or improving outcome for the patient e.g. heart attack or serious bleeding
Category B – Conditions which need to be attended quickly, but which are not immediately life-threatening
Category C – Non life-threatening conditions that may be appropriate for referral to an alternative care pathway
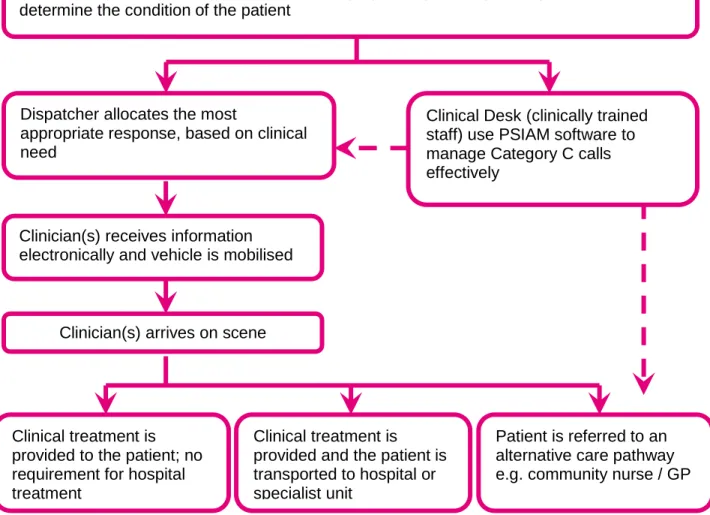
Figure 2.2 provides an illustrative example of the management of 999 calls through our systems.
We currently provide four different products within our A&E service: 999 Call-taking
The function undertaken within our Emergency Dispatch Centre of answering and initial triage (via AMPDS) of the call.
Hear & Treat
Those situations, generally Category C calls, where advice is provided directly to the patient over the phone by a clinically trained member of staff within the Emergency Dispatch Centre. This may include identification of an alternative care pathway.
See & Treat
Where a clinician attends and provides treatment to the patient, but there is no requirement to transport the patient to hospital (or other healthcare facility).
See, Treat & Convey
As with See & Treat, the clinician attends and provides treatment to the patient, however there is the need to transport the patient to hospital (or other healthcare facility) for further treatment.
Our innovative
approach to
infection control,
“Make Ready” won
the 2009 Regional
Best of Health
Awards for patient
safety
Page | 14 IBP2010-15_Summary_20100325
In line with national trends, A&E activity is increasing year on year (NHS Information Centre, 2009). Analysis of trends relating to population, epidemiology and healthcare confirm that demand for ambulance services is likely to continue to rise in line with historical trends. Table 2.2 highlights increasing demand for our A&E service. We attended 532,893 incidents in 2008/09, an increase of 5.8% increase on 2007/08 activity.
Table 2.2 - A&E activity (by incidents)
2006/07 2007/08 2008/09 Projected
2009/10
A&E activity 483,360 503,700 532,893 559,538
Growth N/A 4.21% 5.80% 5.00%
Figure 2.2 - Management of 999 calls
Clinical Desk (clinically trained staff) use PSIAM software to manage Category C calls effectively
Dispatcher allocates the most
appropriate response, based on clinical need
Clinician(s) receives information electronically and vehicle is mobilised
Clinician(s) arrives on scene
999 call or call from a healthcare professional received by the Emergency Dispatch Centre
Call Taker uses the Advanced Medical Priority System (AMPDS) to triage the call and determine the condition of the patient
Clinical treatment is provided to the patient; no requirement for hospital treatment
Clinical treatment is provided and the patient is transported to hospital or specialist unit
Patient is referred to an alternative care pathway e.g. community nurse / GP
Page | 15 IBP2010-15_Summary_20100325
2.2.2. Patient Transport Service (PTS)
Non-emergency patient transport services for the movement of patients to and from NHS facilities includes the transportation of ambulant, wheelchair bound and stretcher patients, plus infectious cases. The types of journeys undertaken include inpatient admissions, out-patients and day patients from the patient‟s place of residence, including nursing homes, to NHS facilities and non urgent transfers between hospitals and discharges from hospitals to home. We employ Ambulance Care Assistants (ACAs), who operate either single or double crewed vehicles to transport these patients.
Additionally, a volunteer-operated ambulance car service supports the Patient Transport Service.
Within our Patient Transport Service, we provide two different products: High Acuity PTS
The patient may require some degree of clinical care during transportation. Low Acuity PTS
The patient does not require clinical care during transportation.
Table 2.3 shows that demand for PTS services continues to decrease over time. However, evidence suggests that the level of acuity of the patients using these services is increasing. Table 2.3 - PTS activity (number of journeys)
2006/07 2007/08 2008/09 2009/10 2010/11 2011/12
PTS activity 455,602 451,634 438,220 433,837 429,498 425,202
Growth N/A -0.88% -2.97% -1.00% -1.00% -1.00%
2.2.3. Commercial Services
In addition to the provision of front-line clinical services, we have developed a number of areas of expertise for commercial development opportunities. These include event work, insurance work, training, education and workshops. This work is currently co-ordinated by our
Commercial Services department.
The Private Ambulance Service (PAS) currently provides First Aid, clinical and pre hospital emergency cover to a range of public events across Surrey, Sussex and Kent and further afield, with the capability to provide HSE approved
First Aiders, Paramedics and Technician crews, registered nurses, paramedic practitioners and the paramedic Cycle Response Unit. By attending events we are able to deal with injuries and illnesses on scene and ensure patients are discharged to appropriate follow-on care, preventing acute services becoming overwhelmed as a result of large public gatherings.
PAS undertakes both private and NHS patient transfer work. In 2008/09 we undertook over
We are currently developing our
first ever community education
programme which will see
frontline staff educating the
public about how to identify
potentially life threatening
conditions and what actions to
take to save lives
Page | 16 IBP2010-15_Summary_20100325
400 patient transfers commissioned by local PCTs, other NHS Trusts and private hospitals and patients.
As part of our commercial training department we provide accredited First Aid at Work courses to a number of external clients, with the capacity to run bespoke courses for AED, oxygen and entonox and first aid emergency care training for specific needs such as cave rescue and fire and rescue.
We are commissioned by Surrey Police to provide a 24/7 service for urgent and emergency care needs for detained patients located in the four custody suites across Surrey, which provides a source of non-NHS income. This model of care is considered best practice by both the Home Office and local mental health teams. In line with the current contract, we provide two response cars that can be deployed at any time to custody suites across Surrey, staffed by paramedics.
2.2.4. Emergency Preparedness
We are a Category 1 responder under the terms of the Civil Contingencies Act 2004, and as such we have six statutory duties:
Assess local risks and use this to inform emergency planning;
Put in place emergency plans;
Put in place Business Continuity arrangements;
Put in place arrangements to make information available to the public about civil protection matters and maintain arrangements to warn, inform and advise the public in the event of an emergency;
Share information with other local responders to enhance co-ordination;
Co-operate with other local responders to enhance co-ordination and efficiency. The Patient Transport Service (PTS) is integral to the resilience of the Trust in terms of
providing flexibility in the event of either a Major or Business Continuity Incident. PTS allows an additional pool of vehicles and staff to be available to support the core A&E activity in the event of a crisis.
2.3. Performance
The Annual Health Check conducted by the Care Quality Commission assesses performance on two criteria; Quality of Services and Quality of Financial Management. Our performance against these two components is shown in Table 2.4. A detailed breakdown of our performance against the Quality of Services component is provided in Table 2.5.
Table 2.4 - Annual Health Check ratings
2006/07 2007/08 2008/09
Quality of Services Fair Good Fair
Page | 17 IBP2010-15_Summary_20100325
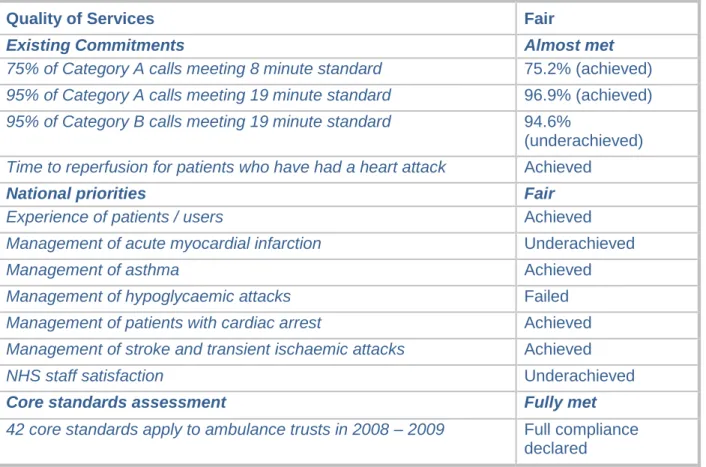
Table 2.5 - Annual Health Check: Quality of Services performance 2008/09
Quality of Services Fair
Existing Commitments Almost met
75% of Category A calls meeting 8 minute standard 75.2% (achieved) 95% of Category A calls meeting 19 minute standard 96.9% (achieved) 95% of Category B calls meeting 19 minute standard 94.6%
(underachieved) Time to reperfusion for patients who have had a heart attack Achieved
National priorities Fair
Experience of patients / users Achieved
Management of acute myocardial infarction Underachieved
Management of asthma Achieved
Management of hypoglycaemic attacks Failed
Management of patients with cardiac arrest Achieved Management of stroke and transient ischaemic attacks Achieved
NHS staff satisfaction Underachieved
Core standards assessment Fully met
42 core standards apply to ambulance trusts in 2008 – 2009 Full compliance declared
We were disappointed in the deterioration in our performance for the “Quality of Services” criteria, although this mirrored the trend across the ambulance sector, identifying some need for improvement in data analysis and reporting at a national level. We aim to improve on our rating in 2009/10, by focussing on the following areas:
Existing commitments – Category B performance: Work is ongoing to improve delivery of the Category B target. Analysis of the Category B incident level is reviewed daily as part of the operations management processes.
National priorities – Clinical indicators (including Management of acute myocardial infarction and Management of hypoglycaemic attacks): Work is underway at a national level to influence the approach used for analysis of the Clinical Performance indicators, and we are involved with these discussions with other ambulance trusts and
representatives from the CQC. In addition, we are introducing a new Patient Clinical Record (PCR) to facilitate data capture relating to clinical outcomes. Our performance on the clinical performance indicator (CPI) relating to Return of Spontaneous Circulation (ROSC) shows that the Trust is performing significantly above any other trusts nationally (see Figure 4.6).
National priorities – staff satisfaction: We have established a working group to address areas of weakness within the staff survey, including staff satisfaction.
The Trust has a good history of sustaining and improving performance against standards, as evidenced in Table 2.6. National performance targets are also monitored by the Trust at PCT level.
Page | 18 IBP2010-15_Summary_20100325
Table 2.6 - National Performance Targets: Existing Commitments
Standard Target 2006/07 2007/08 2008/09
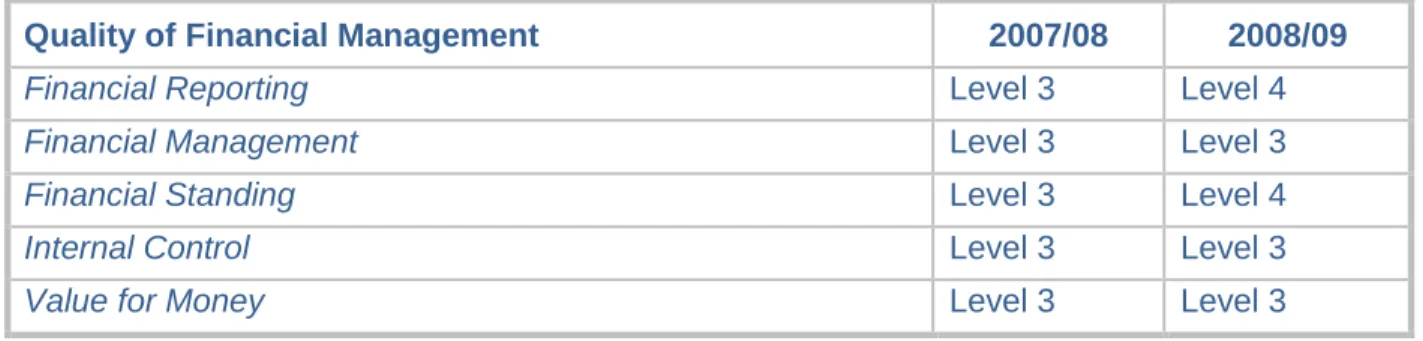
75% of Category A calls meeting 8 minute standard 75% 75.1% * 77.2% 75.2% 95% of Category A calls meeting 19 minute standard 95% 97.6% 97.6% 96.9% 95% of Category B calls meeting 19 minute standard 95% 93.8% 95.2% 94.6% * The 2006/07 figure for Category A performance uses a different method for measurement Table 2.7 - Annual Health Check: Quality of Financial Management 2008 – 2009
Quality of Financial Management 2007/08 2008/09
Financial Reporting Level 3 Level 4
Financial Management Level 3 Level 3
Financial Standing Level 3 Level 4
Internal Control Level 3 Level 3
Value for Money Level 3 Level 3
2.4. Contractual information
A&E services are commissioned on a consortium basis from the eight PCTs in the South East Coast region, along with Hampshire PCT and Berkshire East PCT for a small geographic area within Berkshire and North East Hampshire on
the Surrey County boundary.
The PCTs have financial and risk sharing arrangements in place, which are overseen by the Specialist Commissioning Group (SCG) Board, which has senior representation from all the commissioners. Day to day management of the contract is via a lead commissioner, which is hosted by West Kent PCT. The contract is managed through monthly meetings between the trust and representatives from all the
commissioning bodies. We also work with individual commissioners on a number of local initiatives and developments which reflect individual commissioning priorities. A Commissioning Strategy for Ambulance Services 2008-12 has been developed and was signed off by the SCG in December 2007. Alongside this strategic document there is an
annual commissioning plan, linked to the PCTs Local Delivery Plans. This defines the activity and specific changes required for the service to enable a contract to be agreed by the lead commissioner (NHS West Kent), through the SCG Board on behalf of all parties.
PTS has historically been commissioned by other health service providers such as acute, mental health and community trusts. From April 2009 responsibility for the commissioning of
In line with our workforce
and fleet strategies, last
year we recruited more than
200 new frontline
operational staff as well as
additional Emergency
Dispatch Centre staff,
including emergency call
takers. We also deployed
37 new ambulances and 26
new rapid response
vehicles – more staff and
more vehicles responding
to local patients
Page | 19 IBP2010-15_Summary_20100325
PTS moved to PCTs and is aligned with the introduction of a national contract for both A&E and PTS services.
There are no plans for ambulance services to become subject to tariff arrangements at the present time. We are working with commissioners to develop the framework that will allow the introduction of variations to price paid based on type of patient, clinical outcome and
appropriateness of the response.
With PCT Commissioners taking over the funding for PTS from hospital trusts from April 2010, it is expected that PTS contract management will be placed higher on commissioning agendas. Commissioners have committed to continue to fund PTS until March 2010 and PTS is likely to be put out to tender during 2010.
The trust engages with a range of stakeholders to develop services that meet the needs of patients, and support government and commissioners priorities. We are uniquely placed as a provider which, on a daily basis, interfaces with all elements of health and social care.
Commissioners are placing greater emphasis on our role in leading change across the healthcare system. This can be on specific issues, such as the development of new patient pathways for dealing with conditions such as cardiac, stroke and trauma, and also on leading the health services response in emergency planning and preparedness. Alongside these specific issues, it is increasingly recognised that the trust has a pivotal role in developing and supporting wider-ranging strategies that will change the provision of urgent healthcare. Other procurement arrangements
In our procurement activities we take advantage of collaborative procurement through the Office of Government Commerce (OGC), national and local procurement hubs, and other collaborative framework contracts to achieve best value for money.
Payroll and pension services from the three legacy ambulance trusts have been merged
following market testing, and this has been outsourced to Equiniti ICS, who hold a strong market position and provide services to many NHS organisations.
NHS Shared Business Services is a 50:50 joint venture partnership between the Department of Health and Xansa, a leading provider of shared financial and accounting services from the private sector. NHS SBS combines knowledge and experience of the NHS with best practice processes and experience of world class technology from the private sector. This combination enables operational processes to be delivered more cost-effectively, thereby enabling the Trust to save money over the true cost of its in-house operations.
Joint venture information
The Trust currently has no formal joint venture agreements but active partnership working is an important feature of the Trust‟s way of working.
Meeting peaks in demand
In order to support peaks in demand that cannot be resourced appropriately from regular front-line resources we have arrangements in place with the Voluntary Aid Societies including British Red Cross and St John Ambulance. Their services can be flexed to support PTS provision, transfer of pre-assessed patients to hospital and front-line emergency responses. Formal arrangements are in place to ensure that clinical governance standards are met for all partnership arrangements.
Capacity Management System (CMS)
The Capacity Management System is a service that is hosted by SECAmb, and provided to NHS partners. This is funded by Service Level Agreements and each organisation funds this on
Page | 20 IBP2010-15_Summary_20100325
a capitation basis, with a total annual turnover of £794,627 for 2009/10. It is governed by a strategic board, which is constituted of five Executive Directors from the 11 ambulance trusts. This board reports to the National Ambulance Trust Chief Executive‟s Board. There is a consortium agreement to ensure that the risks to SECAmb are minimised.
Page | 21 IBP2010-15_Summary_20100325
3. Strategy
This section:
Articulates our vision and strategy
Outlines the systems we have in place in the Trust to deliver our strategy
Explains why we want to become a Foundation Trust and how this will effect how we operate
Describes the outcomes of our FT consultation process
The key points from this section are:
We have a robust strategy to support delivery of our vision Our strategy is to strengthen and extend our core activities
The principles of high performance are understood and embedded in the organisation
We have undertaken a comprehensive public consultation, and now have a public membership of 2,800
3.1. Trust vision
Our vision is to match and exceed international clinical excellence through embracing innovation and putting the patient at the heart of everything we do.
Match and exceed international clinical excellence
Patient outcomes for life threatening conditions such as stroke, trauma and heart disease are not as good as they could be in this country when we compare to centres of international clinical excellence. This is unacceptable for our patients. We therefore aspire to compete with the best healthcare organisations worldwide to deliver world class outcomes for our patients.
Embracing innovation
Matching and exceeding international clinical excellence means changing the way we work now. We need to embrace innovation; learn from the best, adapt it to make it better, be the best. Putting the patient at the heart of everything we do
We exist to serve our patients; everything we do must have them at the core. In five years time, we will be:
The first point of contact for the majority of patients seeking unscheduled urgent healthcare advice or treatment;
Changing the way services are commissioned with an emphasis on payment for results;
A key player in the delivery of whole health economy savings by reducing the duplication of healthcare offered.
3.2. Strategy
Page | 22 IBP2010-15_Summary_20100325
92% of our income funds A&E activity and the three services that we provide in this area; Hear and Treat, See and Treat and See, Treat and Convey are our core activities. Our strategy is to strengthen these services by adopting the principles of high performance:
Response time reliability – responding to the patient quickly
Clinical effectiveness – providing them with the right advice, making them better, or taking them to someone who can
Customer satisfaction – providing them with a service that is easily accessible, treating patients with dignity and respect
Economic efficiency – achieving all of this whilst delivering whole health economy savings by reducing duplication of effort
To implement our strategy, we have identified six strategic objectives underpinned by key service developments. Figure 3.1 details the relationship between our vision, strategy, strategic objectives, and service developments.
Due to Make Ready Depots
A&E staff are no longer
required to clean, stock and
refuel their vehicles at the
start of every shift – it is
estimated that this takes 72
minutes per shift. This has a
massive impact on UHU and
drives our cost efficiency
programme.
Page | 23 IBP2010-15_Summary_20100325
Figure 3.1 - Strategy Focus
Strategy: Our strategy is to strengthen and extend our core activities
Response time reliability Clinical effectiveness Customer satisfaction Economic efficiency Strategic Objectives Improve on the Trust‟s performance standards and reduce variation Deliver excellence in leadership and development Improve access and outcomes to match international best practice Improve satisfaction and experience for all stakeholders Be an organisation that people seek to join and are proud to be a part of Convert all available pounds / resources to maximise patient benefit Service Developments Improving IT systems Make Ready
Development of Hear & Treat
Implementation of the Front-Loaded Service Model
Page | 24 IBP2010-15_Summary_20100325
3.3. Measuring achievement of our Strategy
The concept of high performance is based on the principles of Total Quality Management, and focuses on converting the public‟s expectations into something that is tangible to manage and deliver.
High performance seeks to create a system that delivers efficiency and simultaneously enables quality to be improved. To implement high performance for our provision of A&E services, we apply the concept of Unit Hour Utilisation (UHU). This is a complex economic model that is used to calculate productivity, resource utilisation and cost, and enables us to accurately manage the resources required to deliver our services efficiently. The UHU provides an efficiency measure, calculated by considering the number of resourced hours, and the amount of activity undertaken within
the resourced hours. Based on extensive examination and monitoring of historical activity data, we are able to identify the factors that impact on the UHU, and consider how these can be best controlled and managed in order to maximise efficiency and provide value for money.
Demand for emergency services is surprisingly predictable, both temporally and geographically. We can very accurately predict the time and general area of calls, and the challenge is to
ensure the right amount of resource is on duty at the right time and in the right place to meet this. UHU informs us, for any given operational area, what the utilisation needs to be to deliver the required response times. The UHU is used to establish the resources required to match the ever changing fluctuations in demand, ensuring neither too many (money wasted) nor too few (response performance compromised) are available to respond to patients when they are required. Unit Hour Utilisation allows us to operate within defined tolerances to deliver
operational and financial performance; we have therefore set the UHU levels we plan to deliver over the next five years to ensure that we are a high performing Trust.
Implementation of high performance within the organisation will be delivered through a process of continuous improvement. This will include, but is not limited to, using IT enablers; a
comprehensive estates review, including identification of appropriate locations for response posts; evaluation of the configuration of single and double-manned vehicles.
3.4. Aim for NHS Foundation Trust status
Foundation Trust status is a mechanism that enables us to deliver the system and cultural change required to become a world class provider of emergency and urgent care. This is because the benefits that can only be realised as a Foundation Trust are key enablers to achieving our vision and strategic objectives. These are:
Greater autonomy from central control – enabling us to fast-track innovations into practice at a more rapid pace;
Ability to retain surpluses, allowing increased investment in key service developments to achieve cultural and system transformation;
Greater involvement and ownership for local communities, staff and stakeholders – a structure designed to be first and foremost responsive to the needs of local patients;
We measure efficiency in the
system by looking at unit hour
utilisation (UHU). By utilising the
hours better ie responding or
conveying for as many hours in
a shift as possible, we are able
to save money thus generating
savings without sacrificing on
quality of service
Page | 25 IBP2010-15_Summary_20100325
Long-term financial and business planning – future-proofing the organisation and our vision in an austere financial climate;
Greater flexibility to respond quickly and competitively to commercial opportunities e.g. geographic expansion or market growth;
Development of a representative membership will provide a significantly larger pool of engaged local people wanting to be involved with their local ambulance service thus increasing involvement in the development of future services. A representative
membership will also provide us with a greater insight into the varied needs of our local communities;
The creation of a Council of Governors that will ensure that the Trust is held to account for meeting the needs of local people through the delivery of our plans that members have helped to shape.
3.5. Consultation process
We undertook our consultation from 25 July to 16 October 2009 inclusive. Throughout the 12 weeks we engaged and consulted patients, members of the public, staff, community groups including seldom heard groups, NHS partner organisations, councils, Health Overview & Scrutiny Committees (HOSCs) and local authorities.
809 responses were received in total, 779 using the feedback pro forma (hardcopy, online or electronic voting) and 30 via emails / letters.
Table 3.1 details the breakdown of respondents by background. Table 3.1 - Background of respondents
Background of respondent Number of respondents from this background
% of total number of respondents
Member of the public / patient 256 32%
Representative of an NHS organisation 46 6%
Employee of SECAmb 311 38%
Volunteer of SECAmb 29 4%
HOSC / Local authority member 45 6%
LINk member 45 6%
Representative of another organisation 53 7%
Overall the response was generally positive, with the majority of respondents in favour of all the proposals put forward. Most questions received a 70-90% positive response rate, however, for the questions about the minimum age for members or governors, the positive response rate dropped to around 60%. See Appendix 4 for a more detailed breakdown of responses. Table 3.2 details the key issues identified during the consultation and the Trust‟s response.
Page | 26 IBP2010-15_Summary_20100325
Table 3.2 - Issues identified during public consultation and Trust response
Key issues identified Trust response
No minimum age for members: The majority of respondents (59%) were in favour of no minimum age for membership; however a considerable proportion (32%) felt there should be a minimum age limit.
The arguments centred on the level of contribution that younger children would be able to make, and how children and young people could be engaged. For those who believed that there should be a prescribed age limit, opinion on what the age limit should be varied, with most in favour of age 16 or 18.
There will be no minimum age for membership, but members must be 16 years of age to vote in governor elections.
Minimum age of governor should be 16: The majority of respondents (63%) were in favour of the minimum age for governors being 16, with 31% opposing this view, and suggesting it should be 18 or 21 instead. The rationale for increasing the age limit from 16 was around the experience of individuals to take on the governor role, as well as commitment from young people still in full time education.
The minimum age for a member to stand as a governor is 16 years of age.
Representation on Council of Governors: The majority of respondents (70%) were in favour of the proposals for the Council of Governors. Amongst those opposing (16%) the main concern was around the representation of appointed governors and whether one governor could adequately represent all the local authorities in the area or similarly all the PCTs or voluntary sector. There was a strong feeling that the Council needs to ensure accountability, transparency and openness.
There is no increased
representation on the Council of Governors from the proposed structure.
Membership analysis
We have set a target of recruiting 4,500 public members by 31 March 2010. This represents 0.13% of the eligible population that we serve. As at 1 March 2010, we had recruited 3,133 members.
We currently have a broadly representative membership in terms of ethnicity. However, members of Bangladeshi and Chinese ethnic groups are under-represented.
There is an over-representation of women, whilst under 18s are under-represented.
The Trust has commissioned a database to mange member information which we use on a regular basis to monitor the representativeness the Trusts membership. There is a robust action plan which details plans to address underrepresented groups.
Stakeholder analysis
The Trust employs a Stakeholder Relations Manager within the Communications and
Engagement department. Figure 3.2 shows an external stakeholder map developed using the influence / interest model (What to do when stakeholders matter: A guide to stakeholder identification and analysis techniques, John M.Bryson, 2003). This analysis informs SECAmb‟s overarching communications and engagement strategy.
Page | 27 IBP2010-15_Summary_20100325
NHS South East Coast Specialist Commissioning Group PCTs Unions HOSCs Local media CQC Audit Commission MPs
Ambulance Service Network National media
Acute trusts Police force
Local Authority CEOs Councillors
DH Leadership team
Fire & Rescue Service Social Services
Mental health trusts General public Professional bodies Seldom heard groups
Patient & public representatives Community responders
Voluntary organisations Other ambulance trusts High Low Inf lue nc e High Low Interest Figure 3.2 - Stakeholder analysis
Page | 28 IBP2010-15_Summary_20100325
4. Market Assessment
This section:
Describes the market within which the Trust operates
Recognises the influencing factors that impact on the environment in which we operate
Outlines how our strategy contributes to the overall objectives of the health economy
Provides analysis of our key competitors
Indicates the market share we hold in the markets in which we operate
The key points from this section are:
The Trust has a good understanding of the market and competitive influences that will affect it
Demand for healthcare services is causing growth in all markets; this is most significant in the unscheduled urgent care market
4.1. Description of local health economy
We provide services to the South East Coast (SEC) health economy, incorporating the counties of Kent, Surrey, Sussex and part of north east Hampshire on the Surrey County boundary. Within the region there are eight PCTs,12 acute trusts (four are FTs) and four mental health and specialist trusts (two are FTs). We are coterminous with NHS South East Coast. See section 4.3 for information about local health economy objectives.
The region breaks down into 80% rural and 20% urban (www.southeastcoast.nhs.uk, 2009.) This impacts upon where demand is generated. In planning volume and location of unit hours, rurality is considered to ensure consistent compliance with response time targets.
Within the region there are some of the busiest stretches of motorway in the country (e.g. M25) as well as major transport links (e.g. Gatwick airport, Channel Tunnel) and as such we are active members of both local and regional resilience forums – alliances consisting of category one responders (police, fire and ambulance) as well as other agencies including the Coast Guard, Highways Agency and Health Protection Agency – to ensure robust preparedness in the event of a major incident.
We serve a resident population of c4.3 million people (Office for National Statistics (ONS) mid 2008 population figures, www.ons.gov.uk, 2009)which swells during the summer months due to tourism in coastal areas; this results in an activity increase during these months (see Figure 4.1 and Figure 4.2) which we manage through deploying additional hours as with any busy period. SECAmb values diversity, equal access for patients and equality of opportunity for staff. We aim to create the best possible quality of life for those we serve by delivering a high quality service to all members of our community.
Page | 29 IBP2010-15_Summary_20100325
Figure 4.1 - Emergency calls by month for 2007-09
Source: info.secamb.nhs.uk
Figure 4.2 - Emergency responses by month for 2007-09
Source: info.secamb.nhs.uk 40,000 42,000 44,000 46,000 48,000 50,000 52,000 54,000 56,000 58,000 60,000 2007 2008 35,000 37,000 39,000 41,000 43,000 45,000 47,000 49,000 51,000 53,000 55,000 2007 2008
Page | 30 IBP2010-15_Summary_20100325
Population in the SEC health economy is increasing and this trend is set to continue as regeneration projects come on stream during the next 20 years including the construction of circa 58,000 new homes in West Sussex by 2026 and the development of the North Thames Gateway in North West Kent and Medway in the next 15 years (Healthier people, excellent care, NHS South East Coast, 2008). Population increase will directly impact upon demand for our services. Table 4.1 sets out the current population breakdown by PCT area.
Table 4.1 - Population breakdown by PCT area
PCT area All ages
(mid 2008) Children (0-15 years) Working age (16 – 64M/59F) Older people (65M/60F and over)
Brighton and Hove City 256.6 41.1 173.2 42.4
East Sussex Downs and Weald 332.3 59.0 184.4 88.8
Eastern and Coastal Kent 732.0 138.0 431.5 162.5
Hastings and Rother 177.6 31.7 98.4 47.6
Medway 253.5 51.7 159.6 42.2
Surrey 1,097.7 211.6 671.1 215.0
West Kent 674.6 134.6 407.3 132.6
West Sussex 781.5 144.0 450.3 187.2
TOTAL 4,317.8 813.2 2,584.8 919.8
Source: Mid-2008 Primary Care Organisations for England, Office of National Statistics, 1 October 2009
The SEC health economy has an above average population of older people with 21.3% of the overall population being over 65(M)/60(F), the average is 19.36% (Mid-2008 Primary Care Organisations for England, Office of National Statistics (ONS), 1 October 2009). The national trend signifies an ageing population; this will impact upon demand for our services; see Section 4.2 for more detail.
The health economy performs comparatively well in terms of key public health issues such as obesity, smoking and healthy eating. However, more than one in five adults in the region are smokers and a similar proportion of adults in some areas are binge drinkers; nearly one in five adults living in the health economy are obese (Healthier People, excellent care, NHS South East Coast, 2008). This has implications for the types of conditions that present to us in
particular for life threatening episodes linked to unhealthy lifestyles, long term cardiovascular or pulmonary diseases and for accidents and incidents related to the overconsumption of alcohol.
There is inequality across the region in terms of access to GP services. In 2008 GPs had an average patient list of 1,680, however, GPs are not evenly distributed across the region which can result in frustrated access (Healthier People, excellent care, NHS South East Coast, 2008). This presents an opportunity for us; by providing a solution to commissioners in the form of paramedic practitioners who can work alongside GPs and support them by conducting home visits freeing up GPs to conduct surgeries. This is cost effective for the health economy whilst providing a more timely service to local patients thereby improving care and experience.
Page | 31 IBP2010-15_Summary_20100325
Inequalities also exist in death rates for major killers such as stroke and heart disease. Early deaths from these conditions are higher than the national average in Medway and lower in large parts of the rest of the health economy (Healthier People, excellent care, NHS South East Coast, 2008). This means that the provision of pathways to manage early intervention following vascular compromise will be essential to reduce the death rate and also prevent significant disability following these events, which can be costly to manage and devastating for the patient and their family.
4.2. Key factors driving demand
Historically, ambulance services have not been classified as providing urgent and unscheduled care, however, trend analysis shows that this is where the increase in demand has been generated over the last decade. Emergency calls nationally have increased per annum by between 5 and 7% (see Figure 4.3), however, conveyances to hospital have not increased at the same rate signifying that the increase in 999 volume is a result of patients calling with less serious healthcare needs – typically falls (22% of SECAmb‟s overall calls in 2008/09, the largest proportion of emergency calls), exacerbations of long-term conditions (e.g. asthma, diabetes) and minor injuries and illness.
Figure 4.3 - Number of emergency ambulance calls / conveyances 1998 - 2009
Source: NHS Information Centre
The following factors inform us that this trend is set to continue in the future: Long-term conditions
There are 15.4 million people living with a long-term condition in England (www.dh.gov.uk, 2009). Numbers are expected to rise due to an ageing population and unhealthy lifestyle choices. This means more people requiring urgent and unscheduled care services.
0.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00 8.00 Cal ls / C o n ve yan ce s ('00 0) Year Calls Conveyances
Page | 32 IBP2010-15_Summary_20100325
Ageing population
Over the last 25 years the percentage of the UK population aged 65 and over has increased by one per cent which equates to 1.5 million people; this trend is set to continue (www.ons.gov.uk, 2009). The SEC health economy is the second highest health economy in the country in terms of percentage of overall population who are over 65(M) and 60(F) with 21.3%. By 2020 more than 40% of the SEC population will be over 50, over 65s will increase by circa 50% and the number of over 85s will double (Healthier people, excellent care, NHS South East Coast, 2008). Older people are the largest user group of ambulance services with many accessing our
services for conditions such as falls, breathing problems, exacerbation of a long-term condition such as diabetes (see Figure 4.4) or accessing our patient transport services. This means that the traditional pattern of ambulance response, attend and convey, will be replaced by a more differentiated response to calls, in particular, treatment provided in the home to reinforce existing care plans, referral of patients to appropriate community care and social services, and provision of minor treatments and prescribing advice. Single responders with enhanced
paramedic skills and equipped to deliver a broader range of treatment options, who understand and can guide patients to the most appropriate community service, will become the norm. Figure 4.4 - Calls by MPDS code 2007/08 and 2008/09
Source: info.secamb.nhs.uk
NB: please note that not all MPDS codes are included in this chart for display reasons 0% 5% 10% 15% 20% 25% % age o v er all ca ll v o lum e 2007/08 2008/09
Page | 33 IBP2010-15_Summary_20100325
Access to urgent and unscheduled care
Distribution of GP services across the SEC health economy is not even (Healthier people, excellent care, NHS South East Coast, 2008) which can result in patients accessing urgent and unscheduled care services via alternative routes such as 999. This is typically true out of hours since the new GMS contract that came into effect in 2003 which led to a removal of
responsibility for individual patients. This has increased demand for ambulance services for three reasons:
Patients were confused about who to contact out of hours leading many to call 999 to access healthcare;
Out of hours GP providers more risk averse as they are not familiar with local patients; as such urgent calls from GPs increased;
GP out of hours providers are not incentivised to keep patients out of hospital meaning increased calls for conveyances to secondary care services.
Other services in the Unscheduled Urgent Care market – minor injury units, walk in centres, community nursing etc – are not evenly spread across the health economy and vary depending on day of the week and hour of the day; this results in confused and frustrated access from a user perspective, which again impacts directly on our demand as a barrier-free entry point to healthcare services.
Population growth
As stated in Section 4.1, population in the SEC health economy is increasing. A larger
population who are living for longer with increasing long-term conditions all drives demand for our services.
Economic downturn
Significant research undertaken concludes there is a clear correlation between unemployment and ill health (The health consequences of unemployment: the evidence, Colin D Mathers and Deborah J Schofield, MJA 1998; 168: 178-182). As a result of the economic downturn, the unemployment rate nationally was 7.9% for the three months to August 2009, up 0.3% over the previous quarter and up 2.1% over the year (www.ons.gov.uk, 2009). In the South East Coast government region (South East Coast and South Central health economies combined) the rate of unemployment is below national average at 6.0% (Government Office of South East, 2009) however, in line with national trends of increasing unemployment, this figure is likely to increase and therefore potentially increase demand for our services.
We have developed initiatives to manage increased demand from patients with unscheduled urgent care needs, namely the paramedic practitioner programme and the Directory of Services. However, these developments are in their infancy and it is clear that significant change and further development is needed in order to manage increasing demand in the future.
The Unscheduled Urgent Care market is one where significant efficiency savings can be made and improvements to user experience and outcome can be achieved through the adoption of a more coordinated approach. This has been recognised nationally shown by the pilots for a single point of access (SPA) to urgent and unscheduled care services and as such barriers to entry for alternative providers of urgent and unscheduled care triage and treatment are significantly reducing.
In order to protect our activity and manage increased demand, SECAmb must be proactive in seizing opportunities for coordinating access to urgent and unscheduled care services. The Hear and Treat and Front Loaded Service Model service developments aim to create an
Page | 34 IBP2010-15_Summary_20100325
infrastructure that will position us as a provider of choice for urgent and unscheduled care contracts such as out of hours GP contracts, therefore expanding our market share whilst protecting our core activity.
4.3. Objectives of the local health economy
As part of Lord Darzi‟s NHS Next Stage Review, NHS South East Coast, in partnership with the local health economy, produced its 10 year vision for the region - Healthier People, Excellent Care – in June 2008. The review focussed on eight clinical care pathways ranging from maternity and newborn through to end of life care, and made recommendations and
commitments for improving care in each. SECAmb has reviewed all commitments made in the vision and identified those where the Trust‟s Strategy can and should contribute to their
achievement. These predominantly are in the acute care pathway and focus on two key areas: Better integration of community and social care to support urgent care, ensuring all patients receive the appropriate care for their need regardless of how they access the system
As a barrier free entry point to emergency and urgent care, SECAmb has a key role to play in ensuring that patients receive the most appropriate care for their condition whether this is critical or less serious. Already a coordinator of access to emergency care, the Trust is well positioned to adopt a similar role in the urgent and unscheduled care arena ensuring direct links with community services. Our strategy is therefore to improve our infrastructure to facilitate
coordination of access to urgent and unscheduled care. This includes strengthening our clinical triage function through boosting clinical capacity in our control centres to increase our ability to provide advice and treatment over the telephone – Hear and Treat service development. We also plan to increase the number of paramedic practitioners in the field who are linked into community care services and therefore able to keep patients with urgent and unscheduled care needs in the community – Front Loaded Service Model service development. The Trust is also exploring joint ventures with GP out of hours providers to further strengthen our position in the urgent and unscheduled care market whilst protecting core activity (see section 4.2 for more information).
Improved outcomes for patients suffering from critical conditions such as stroke, trauma and heart disease through ensuring patients are fast tracked to specialist care which operates 24/7
Improving outcomes for patients suffering from killer conditions is one of our six strategic objectives. As such SECAmb‟s strategy is to develop and implement care pathways for each of the above patient groups to ensure patients bypass A&E and are immediately fast tracked to the specialist care they need. This not only requires further training and development of frontline staff, but also requires service level agreements with acute partners to ensure the system supports bypass arrangements.
Supporting the overarching vision for the SEC
health economy is the South East Coast Strategic Commissioning Plan for Ambulance Services
During 2008/09 we undertook a
major transformation in the way
we manage the delivery of our
A&E Operations. In line with the
principles of High Performance,
we developed management
arrangements, reporting
processes and information
systems to allow us to effectively
flex the workforce to meet
changing patterns of demand for
every hour, of every day of the
year, in our Operational Dispatch
Areas.
Page | 35 IBP2010-15_Summary_20100325
2009 – 2014. This plan provides a framework for PCTs in the SEC health economy to use in their strategic commissioning plans, as well as providing a direction for SECAmb to respond to the needs of commissioners and their populations over the next five years.
The biggest strategic change issues facing SEC commissioners in respect of ambulance services are outlined in the plan as follows:
To minimise unnecessary calls to 999 through understanding the drivers for the increasing demand and improving access to alternative services;
Where calls come through 999, to enable telephone advice and support for patients to access more appropriate services;
To enable patients to be treated at home, with access to appropriate care, unless assessment at hospital is essential.
To ensure delivery of this strategic change, the following objectives have been agreed with commissioners and built into our plans:
Improve the speed and quality of response to life threatening (Category A) emergency calls
To meet and sustain the response time standards for the area, and subsequently to tackle the areas of greatest health inequality.
By developing new clinical skills and techniques, to manage emergencies at the scene, and transfer safely.
To develop and implement appropriate pathways through the various urgent, critical care and clinical networks – transferring to the appropriate (not necessarily nearest) provider.
To ensure best practice and national guidance regarding categorisation of calls is implemented e.g. categorising stroke as requiring a specific timely response.
Improve the speed and clinical quality of call handling to ensure patients are provided the most appropriate service
To enable all category C, and appropriate category B calls, to be triaged through a clinical assessment process by telephone
To develop a database/information centre to enable community services to be identified and the call transferred immediately where appropriate (or utilise any such system agreed across SEC)
To develop a patient based record system for patients on risk registers (e.g. COPD, End of Life) to have care plans and/or contact details lodged with the dispatch centres to support appropriate care and transfers.
To ensure integration/linkages/consistent protocols to other points of access as services and pathways are developed.
Provide a high level of clinical skill in the response to all calls to enable patients to be supported at home where appropriate
To develop paramedic practitioners with a primary care focus to assess and manage those patients where a transfer to hospital is not necessary
To increase the proportion of patients treated at home where appropriate and provide information to the patient‟s GP (and /or other professionals as agreed)
To develop systems to enable information about the range of available community services to be available to the paramedic/ paramedic practitioner at the scene, to enable transfer of care to the most appropriate service.